
Abstract
Analysis of thirty-one hours of video-data documenting 36 experienced drivers highlighted the prevalence of face-touching, with 819 contacts identified (mean frequency: 26.4 face touches/hour (FT/h); mean duration: 3.9-seconds). Fewer face-touches occurred in high primary workload conditions (where additional physical/cognitive demands were placed on drivers), compared to low workload (4.4 and 26.1 FT/h, respectively). In 42.5% of touches (or 11.2 FT/h), mucous membrane contact was made, with fingertips (33.1%) and thumbs (35.6%) most commonly employed. Individual behaviours differed (ranging from 5.1 to 90.7 FT/h), but there were no significant differences identified between genders, age-groups or hand used. Results are of relevance from an epidemiological/hygiene perspective within the context of the COVID-19 pandemic (and can therefore inform the design of practical solutions and encourage behavioural change to reduce the risk of self-inoculation while driving), but they also help to elucidate how habitual human behaviours are imbricated with the routine accomplishment of tasks.
Practitioner summary: The study highlights the propensity of face touching whilst driving through the analysis of on-road video datasets. Results have implications for the design of technological interventions (such as touchless interfaces and driver monitoring systems) and can inform awareness campaigns to reduce the risk of self-inoculation and infection transmission while driving.
Introduction
Driving is a complex, visuospatial task requiring the physical touch and manipulation of various devices and artefacts to control and interact with the vehicle and environment in a safe and efficient manner (Michon Citation1985). For example, the driver must turn the steering wheel to manoeuvre and guide the vehicle, actuate stick controls to engage direction signals and windscreen wipers etc., and depress or twist various knobs, dials and buttons (or touch a touchscreen) to change cabin temperature, interact with infotainment systems etc. There is a plethora of research looking at the organisation and integration of these physical, ‘touch’ tasks—largely from the perspective of form, function and performance (e.g. Burnett and Irune Citation2009). Studies have also explored touch in the context of design, for example, investigating how to differentiate between two or more controls using the sense of touch. This has resulted in many influential and highly-cited human factors guidelines regarding control coding (e.g. Jenkins Citation1947; Bradley Citation1967; Chapanis and Kinkade Citation1972; Boff and Lincoln Citation1988), that have been subsequently employed in the design of traditional physical controls within vehicles (e.g. Burnett and Porter Citation2001). Moreover, research studies have highlighted that drivers are particularly sensitive to the touch characteristics of controls in vehicles when making judgements concerning the overall quality of a design (Burnett and Irune Citation2009).
However, driving studies typically fail to acknowledge or recognise intrinsic and habitual human touch behaviours, such as interactions with oneself, and to consider how these may impact on the specific task or activity under evaluation. For example, if a driver pauses to scratch their nose or rub their eye while they are driving, they may inadvertently delay activation of the windscreen wipers or interrupt a lane change manoeuvre. This can elevate primary task risk factors. For example, the driver’s vision may be temporarily obscured resulting in them missing an approaching hazard, or the available space/headway may have significantly reduced such that it is now too short to consider safely changing lanes.
A related, additional concern is that such ‘face-touching’ behaviours, by their very nature, present a health or hygiene risk to driver. For example, by scratching their nose or rubbing their eye, the driver may inadvertently transfer a foreign substance (acquired from a contaminated vehicle control/surface while driving or prior to entering the vehicle) to their face. The current COVID-19 pandemic has brought such concerns to the stark attention of the populace. Indeed, face-touching has already been recognised as a mechanism for the transmission of disease and infection, and therefore presents an indisputable risk to public health in the context of COVID-19. Consequently, quantifying and characterising face-touching behaviours in different contexts is important. Although various environments have been scrutinised, driving is notably absent. Using the COVID-19 global public health crisis as a backdrop to frame the research, the paper presents a study investigating the propensity of face touching whilst driving through the analysis of existing on-road driving datasets. The primary aim of the study was to identify drivers’ propensity to face-touch during routine driving and to quantify and characterise this behaviour, for example, by considering the impact of primary and secondary task factors, such as workload. The findings provide new understanding about the potential risks faced by drivers during the everyday, private and occupational activity of driving and present a new and novel perspective on analysing human behaviour.
Face touching and COVID-19
In December 2019, the first case of COVID-19 (a highly infectious, novel coronavirus: SARS-COV-2, originating in Wuhan, China) was reported to World Health Organisation, (WHO Citation2020). Since then, the virus has spread rapidly throughout the World. Current figures (at time of writing) show 247,129,785 confirmed cases worldwide, with 5,008,683 deaths (Johns Hopkins Coronavirus Resource Center Citation2021). The COVID-19 pandemic presents an unparalleled threat to public health and the global economy (Ali et al. Citation2020; Ozili and Arun Citation2020).
The COVID-19 virus can be transmitted by self-inoculation. Self-inoculation is a type of contact transmission whereby a person’s contaminated hands make subsequent contact with another area of their body and thereby introduces contaminated material to those sites. For diseases carried in the nasal mucosa, self-inoculation may occur via face-touching if contact is made with the mucous membranes of the eyes, mouth and nose, which together comprise the ‘T-zone’ ( Elder et al. Citation2014). Self-inoculation through face-touching has been shown to be a highly efficient transmission mechanism for coronaviruses, including COVID-19 (Kampf Citation2020), though it is noted that self-inoculation does not necessarily constitute the main infection vector for COVID-19.
Face-touching is defined as touching any part of one’s hair, face, neck or shoulders (HFNS), with one’s hand (Zhang et al. Citation2020), and is a habitual behaviour, often occurring with little or no conscious awareness (Harrigan et al. Citation1987). Ekman and Friesen (Citation1969) postulated that self-touching acts are an effort to manage unpleasant emotions, that is, they signify ‘emotional leakage’ which represent the person’s arousal state. Furthermore, there is evidence to suggest that facial self-touch has associations with attentional focussing (Barroso, Freedman, and Grand Citation1980) and is common in stressful, or high workload, situations (Grunwald et al. Citation2014). For example, Mueller, Martin, and Grunwald (Citation2019) found that self-touch was triggered in participants whilst undertaking delayed memory tasks, suggesting the potential influence of variation in cognitive demand and workload.
Data on face-touching behaviours have been used to assess the likelihood of pathogen transfer to the body, with frequency of touch used to calculate health risk based on exposure modelling (Beamer et al. Citation2015). These data can also help understand and mitigate the potential ramifications of inadequate handwashing after handling any potentially dangerous substance, which may lead to dermatological issues, poisoning or ocular irritation or infection. Although the current, published data are limited, a number of common activity settings have been explored. Dimond and Harries (Citation1984) early study involved 20-min observations of university students. On average, students touched their face 13.33 times. Most self-touch was directed towards the mouth, chin and nose. Interestingly, left hand face-touching predominated, suspected to be because the non-dominant, left hand is typically employed for auxiliary (non-skill-based) functions (Kousaka et al. Citation2013). Hatta and Dimond (Citation1984) and Zhang et al. (Citation2020) also reported higher prevalence of non-dominant hand use during face-touching, as well as the occurrence of ‘private’ functions, such as nose-picking and eye-rubbing. Kwok, Gralton, and McLaws (Citation2015) observational study of medical students in a lecture hall found that, on average, students touched their faces 26 times per hour—demonstrating the prevalence of the behaviour even amongst those who have been educated in hand hygiene and infection control.
Face-touching presents a particular problem if hand hygiene practices are poor, especially following contact with contaminated surfaces, or fomites, or any potentially hazardous material (see: Aiello and Larson Citation2002; Lau et al. Citation2012; Larson et al. Citation2003). Inadequate or ineffectual hand washing is often cited as the most significant contributory factor (Curtis and Cairncross Citation2003), with studies showing that any and all areas of the hand may be missed or inadequately cleaned (see: Taylor Citation1978; Szilágyi et al. Citation2013; Vanyolos et al. Citation2015). In addition, the required length of time for effective contamination removal (i.e. 15–30 s) (Fuls et al. Citation2008; Luby et al. Citation2007) is seldom met during ‘normal’ handwashing conditions. For example, Edwards et al. (Citation2002) reported that only 10% of a population of 313 university students handwashed for longer than 15 seconds, and in Drankiewicz and Dundes (Citation2003) study, only 2% of participants washed their hands for ten seconds or longer. Moreover, these findings involved direct observation, which may have actually increased the likelihood and duration of handwashing (Edwards et al. Citation2002)—handwashing practices in ‘everyday’ settings may be even shorter.
In order to minimise the airborne transmission of the COVID-19 virus, the wearing of personal protective equipment (PPE), notably face masks or coverings, became mandatory in enclosed public settings, such as public transport, shopping centres and during driving lessons in the UK on 24 July 2020 (GOV.UK. Citation2020). However, this also prompted concern amongst some that wearing masks may inadvertently increase transmission rates (European Centre for Disease Prevention and Control Citation2020). Amongst the reasons cited was that putting on a face mask naturally places (potentially contaminated) hands in close proximity to the face, thereby increasing the potential for self-inoculation through face-touching, and that people may make frequent adjustments while wearing their mask particularly if the mask is tight-fitting or uncomfortable. Nevertheless, Lucas, Mustain, and Goldsby (Citation2020) did not report an increased incidence of face-touching in their investigation involving participants both with and without a mask. In practice, face-touching actually decreased with mask wearing (5.4 face touches per hour when wearing a mask compared to 20 per hour without a mask), though it is noted that the study was conducted amongst health professionals, specifically paediatric haematology and oncology staff, who would be expected to be more attuned to the potential risks in situations when face masks are required. In contrast, Chen et al. (Citation2020) explored mask-wearing and face-touching behaviour in general populations. Videographic data captured from public spaces before and during the COVID-19 pandemic in China, South Korea, Japan and Western Europe (England, France, Germany, Italy and Spain) were analysed. This also confirmed that an increase in mask-wearing correlated with a decrease in face-touching, especially associated with the T-zone—although it is noted that concurrent education campaigns on the risk of transmission by face-touching may also account for some of this reduction.
Driving
Driving is commonly classified as an essential daily activity worldwide (Cobb and Coughlin Citation1998), and was specifically identified as a necessity during recent national COVID-19 lockdowns, for example, for food shopping and essential work. There has also been a notable decline in the use of public transport since the outbreak of COVID-19 in the UK, accompanied by a corresponding increase in private car usage (Department for Transport Citation2020). This mirrors the effects seen during the SARS epidemic, which severely reduced public transportation usage due to health and safety concerns (Wang Citation2014).
Concerns have already been raised regarding the potential airborne transmission of pathogens through ventilation systems operating within the confined interior of a car (Knibbs, Morawska, and Bell Citation2012, Sattar et al. Citation2016). In the context of COVID-19, Jayaweera et al. (Citation2020) postulate that with the air conditioning on and windows closed, the recirculation of cooled air could result in an infected backseat passenger exposing all passengers in the car if they cough, for example. Indeed, two early cases were reported in Sri Lanka—one in which the driver became infected with COVID-19 after travelling for less than an hour with an infected passenger sitting in the backseat (Jayaweera et al. Citation2020).
A further concern is that while the exterior of the car is often considered as a projection of public self, the interior is considered a private space (Squires Citation2010). As such, ‘private’ face-touching behaviours, such as nose-picking and ear cleaning, may be more prevalent amongst drivers in their own cars, and when travelling alone. Indeed, although not conducted in the automotive domain, Hendley, Wenzel, and Gwaltney (Citation1973) research reported differences in touch habits based on public visibility. For example, higher frequencies of touching or picking of their nose were recorded by participants when seated in an open amphitheatre compared to participants seated in an intimate conference seating plan. Wilson et al. (Citation2020) conducted similar observations in ten separate indoor locations and reported significant differences in touch frequencies between locations, that were suspected to be privacy-related.
Aims of the study
The everyday, private and occupational activity of driving is an important and under-evaluated area in the context of face-touching yet presents a genuine risk of self-inoculation in the current COVID-19 pandemic. Using archival video data collected from two on-road user studies undertaken prior to the COVID-19 pandemic, this study aims to identify the intrinsic and habitual face-touching behaviour undertaken by drivers during routine driving. To quantify and characterise this behaviour, the study aims to highlight the frequency, duration and distribution of face-touches. A further aim is to expose any associations between individual differences (gender, age, dominant hand used), and begin to explore the effect of primary and secondary task workload on face-touching behaviour.
Methodology
Video data
Archival video data taken from two on-road driving studies were analysed—Pampel et al. (Citation2019) and Morris et al. (Citation2015). Both of these studies occurred prior to the COVID-19 pandemic and at the time of data collection, neither study purported to be concerned with face-touching. Informed consent was obtained from each participant during the original studies for subsequent, additional analyses. The current study involving the re-analysis of these data was approved by the University of Nottingham Faculty of Engineering ethics committee. shows relevant details from the original studies.
Figure 1. Screenshot showing camera views used during Study One (Pampel et al. Citation2019).

Figure 2. Screenshot showing camera views used during Study Two (Morris et al. Citation2015).

Table 1. Details of study data, showing Pampel et al. (Citation2019) (L) and Morris et al. (Citation2015) (R).
Participants
Thirty-six drivers were observed across the two datasets. All participants had normal or corrected vision and no known health issues. All drivers were aged over 21 and drove at least 3000 miles per annum. The complete sample for the analysis (i.e. from both studies), consisted of 23 male and 13 female drivers. The mean age was 37.9 for male participants (SD = 11.2) and 39.9 for female participants (SD = 10.5).
Face touching coding scheme
Videos were coded for face touching area and the hand segment used with Behavioural Observation Research Interactive Software (BORIS) (Friard and Gamba Citation2016) (inter-rater reliability, α = .89). Face touching behaviour was categorised using Zhang et al. (Citation2020) taxonomy, in which the face is split into six segments: hair, neck, shoulders, face (middle), face (left) and face (right), each with clearly defined sub-surface areas ( and ). Contact measurement was only declared when a hand and face were in direct contact with each other, and in accordance with Zhang et al. (Citation2020) taxonomy. Face contact with other parts of the body (e.g. the driver’s forearm) were not included. Roaming face region contacts were counted as separate contacts when the point of hand contact changed definitive face region (Morita et al. Citation2019). For example, if the driver touched their nose (N1) and then their lips (FM3), two contacts were recorded.
Figure 3. Classification of touch action on hair, face, neck and shoulders, with mucous membranes are shown in red (L), and sub-surface listed codes (R) (Zhang et al. Citation2020).
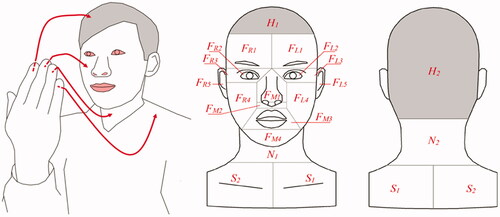
Table 2. Classification and code allocation of face-touching areas (Zhang et al. Citation2020).
Hand segments were coded using regions identified by Taylor (Citation1978) and Szilágyi et al. (Citation2013), which focus on areas of the hand that are frequently missed or inadequately cleaned during handwashing. Hand mappings were devised with the palmar and dorsal surfaces of the hand each segmented into five sections (, ). In situations where multiple sub-surfaces of the hand were used during the touch action, all areas were recorded. For example, if a driver touched their hand on their lips in a closed fist, palmar fingers (PFT), palmar palm (PP) and palmar thumb (PT) may be involved and subsequently all three areas were recorded. When the means of contact changed significantly, a new face-touching contact and hand area were recorded.
Figure 4. Palmar (A) and dorsal (B) sides of the hand coding segments.
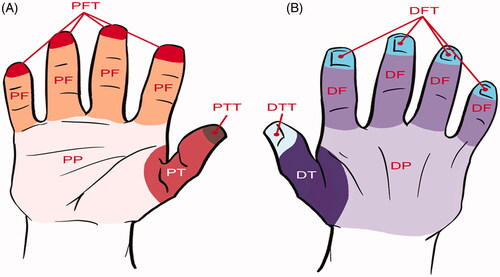
Table 3. Hand segment classification and code allocation.
Driver workload coding scheme
In order to explore any relationship between workload and face-touching behaviour, the following assumptions and coding schemes were adopted. Firstly, for study one (Pampel et al. Citation2019), all testing took place on a motorway and primary task (driving) workload was therefore consistent (as far as practicable) between tasks and participants, i.e. there were no junctions or sudden changes to the road layout, and data collection only took place at times when traffic density was expected to be low (in any situation to the contrary, either data collection was delayed, or the study was aborted). Pampel et al. (Citation2019) explored drivers’ interactions with an in-vehicle touchscreen, positioned in the centre console in two different locations—firstly, at the top of the centre console, aligned with the top of the dashboard and drivers’ line of sight, and then in a lower position, 10 cm below this. Thus, secondary task workload differed between conditions (nominally, ‘high’ and ‘low’), with the upper position designated ‘low’ workload, and the lower position. ‘high’ workload.
For study two (Morris et al. Citation2015), participants drove along a more diverse route, including a variety of different junctions and route decision points, and were also required to interact with other road users. Thus, primary task (physical and cognitive) workload differed along the route and between participants. To differentiate primary task workload, the presence of known elevators of workload were coded for each face-touching event. These events included: lane changing, rapid deceleration, turn preparation (Kim et al. Citation2014), and left and right turn manoeuvres (Hancock et al. Citation1990), i.e. situations that placed additional demands on vehicle handling and/or information processing (Jahn et al. Citation2005). If any such event occurred during the four seconds immediately preceding a face-touch (thereby allowing time for the workload to develop—in line with Verwey (Citation2000)), the primary task workload was deemed to be ‘high’. For face-touching acts occurring on straight roads without other vehicles, primary task workload was coded as ‘low’.
In summary, secondary task workload was coded for face-touching events occurring in Pampel et al. Citation2019 across each condition, whereas primary task workload was coded in Morris et al. Citation2015 for each face-touching event. Workload data from each study were therefore evaluated independently. In both situations, workload was nominally ‘high’ or ‘low’.
Analysis approach and statistical testing
Descriptive statistics are provided for overall touch frequency and duration, and the distribution of face-touches. To explore any associations between individual differences (gender, age, hand used) and workload on face-touching behaviour, inferential analyses are performed. These data are tested for normality using the Shapiro-Wilk test of normality. In situations where this is violated, appropriate non-parametric tests are employed. Thus, the Mann-Whitney U-test was employed to evaluate gender, Kruskal–Wallis H-test for age and Wilcoxon signed-rank for hand used and hand surface (palmar or dorsal). For data that were normally distributed, parametric analyses were employed, such as a paired samples t-test to evaluate the effect of primary and secondary task workload on face-touching.
Results and analysis
Touch frequency and duration
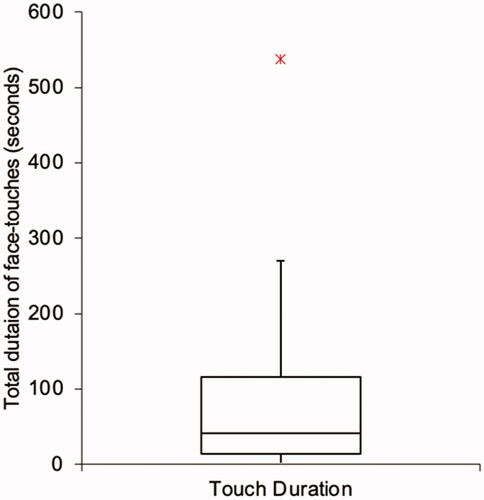
In total, 819 contacts with the HFNS were recorded during 31:01:34.1 (hh:mm:ss) analysed. As an illustration, this equates to a mean touch frequency of 26.4 times per hour—in other words, a new HFNS touch was made every 2.3 min, and each touch lasted 3.9 s, on average. Most (over 97%, or 35 out of 36), but not all, drivers displayed face-touching behaviours. Amongst these, touch frequency ranged from 5.1 to 90.7 per hour (), demonstrating that while some drivers seldom touched their face (i.e. once every 12 min, or so), others were doing so frequently (approximately every 40 s). Duration of contact varied considerably, indicating that for some drivers, touches were quick whereas others displayed more sustained face-touching behaviours ().
Figure 5. Box-plot showing touch frequency (face touches per hour) observed for all participants.
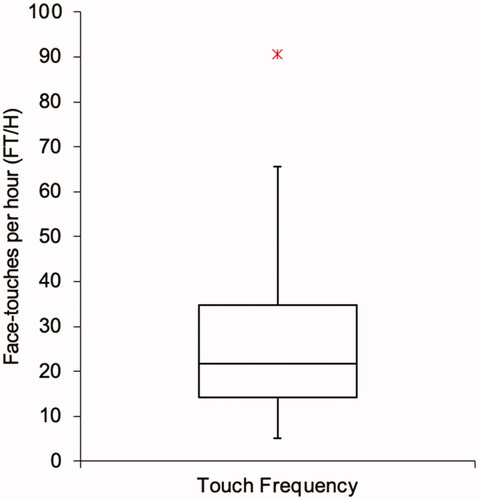
Figure 6. Box-plot showing total duration of face touches (in seconds) observed for all participants.
The face itself was touched most (79.6%), followed by the hair (10.0%), neck (8.6%) and shoulders (1.7%). Thus, on average, drivers touched their face 21 times, their hair 2.6, their neck 2.3 and their shoulder 0.5 times every hour. Results revealed the prominence of self-touch in the T-zone (). All segment frequencies in this zone (nose, nostril, lips and chin) were higher individually than all other segments. Contact with the lips was more than double that of any other facial segment and was responsible for 25.8% of total touches. Self-touch with the nostrils was the second most frequent contact point with the face (12.1%), followed by the chin (9.8%) and the nose (8.1%). Importantly, the high frequency of touches to the lips and nostrils show the recurrence of touch on mucous membranes. Overall, contact with mucous membranes (mouth, nostrils and eyes) occurred in 42.5% of actions, or 11.2 touches per hour. Individual frequencies (touches per hour) for each mucous membrane were 6.8 for lips, 3.2 for nostrils and 1.2 for eyes. Detailed data for each facial segment touch frequency are presented in and .
Figure 7. Frequency map of HFNS self-touch contacts.
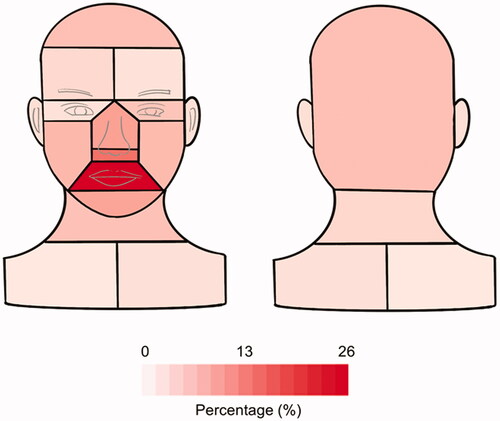
Figure 8. Self-touch frequency (mean values with standard error bars).
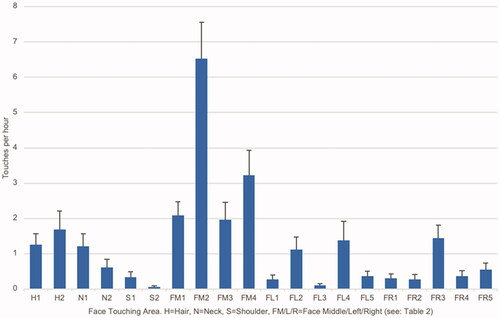
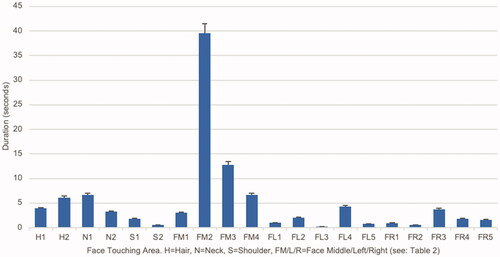
Figure 9. Self-touch duration (mean values and standard error bars).
Individual differences
Inferential analyses were performed to explore any associations between individual differences (gender, age, hand used) on face-touching behaviour.
Gender
For touch frequency, parametric assumptions were not met (as determined by Shapiro-Wilk test of normality, where p = .001). A Mann–Whitney U-test was thus performed to determine if differences existed between males and females. Frequency scores for males (mean rank = 17.35) and females (mean rank = 20.54) were not statistically different (U = 123, z = −.973, p = .397) but suggested that female participants (n = 13) touched their face 8.4 more times per hour, on average, than male participants (n = 23) (Hedges’ g = 0.50 indicating a medium to large effect). For touch duration, parametric assumptions were also not met (Shapiro-Wilk, p < .005). A Mann-Whitney U-test was executed to determine if there were differences in duration between males and females. Duration scores for males (mean rank = 17.52) and females (mean rank = 17.75) were not statistically different (U = 127, z = −.741, p = .474), but suggested that female participants touched their face for 30s longer, on average, than male participants (Hedges’ g = 0.27 indicating a small to medium effect).
Age
For touch frequency, parametric assumptions were not met (Shapiro-Wilk, p < .005). A Kruskal-Wallis H-test was therefore conducted to determine if differences in face-touching frequencies existed between age groups: 20–29 (n = 10), 30–39 (n = 9), 40–49 (n = 10) and 50–59 (n = 7). Distributions of touch frequency were similar for all groups. Median scores for each age group were 20–29 (33.5), 30–39 (16.9), 40–49 (17.8) and 50–59 (23.7). Although differences were not statistically significant (X2(3) = 3.314, p = .346), the data indicated that, on average, face-touching amongst participants aged 30–39 was least frequent (mean = 17.5), with participants aged 20–29 touching their face 11.2 more times per hour, those aged 40–49, 12.2 times more per hour, and those aged 50–59, 23.6 times more per hour.
Hand used
For hand used, normality assumptions were not met due to outliers in the data and a skewed distribution (Shapiro-Wilk, p < .005). A Wilcoxon signed-rank test was conducted to determine any difference between left and right-hand face-touching. There was a median difference per hour in left-hand (12.3) and right-hand (9.7) contact, suggesting that on average, participants used their left hand on 6.2 occasions more than their right hand (Cohen’s d = 0.49 indicating a medium effect) but this difference was not statistically significant (z = −1.705, p = .088).
Hand segments and hand surface
Touch data was also differentiated based on the hand segment. The mean frequency of hand segments engaged in self-touch was 47.9 per hour, indicating that multiple hand segments were potentially used during each face-touch (recall, overall mean frequency was 26.4 FT/h). The palmar surface of the hand was predominantly used and contributed 81.6% of self-touch behaviour. Palmer fingertips (33.1%), palmar thumb (16.8%) and palmar thumb tip (14.8%) were the most utilised segments in self-touch behaviour ( and ). Inferential analysis was conducted to establish any significant differences between palmar or dorsal surface on face-touching. Because normality assumptions were not met (Shapiro-Wilk, p < .005), a Wilcoxon signed-rank test was conducted. There was a statistically significant difference between contact with the palmar surface (Mdn = 28.2) and dorsal surface (Mdn = 3.65) (z = −4.693, p <.0001), with data indicating that, on average, the palmar surface was employed in 31.1 more face-touches than the dorsal side (Cohen’s d = 1.04 indicating a large effect).
Figure 10. Frequency map of hand segments used in face-touching.
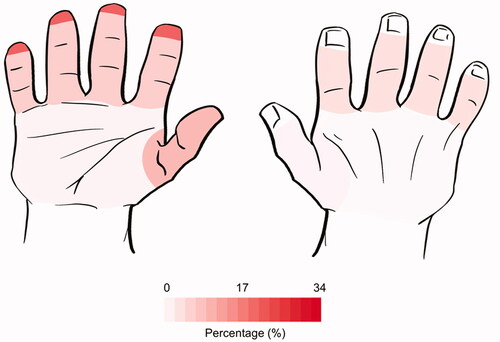
Table 4. Touch frequency of hand segments.
Workload
For secondary task workload (explored in study one, Pampel et al. Citation2019), there was an apparent higher frequency of face-touches in the low workload condition (touchscreen positioned at the top of the centre console in drivers’ direct line of sight) (), although these data also suggest that the duration of face-touches were shorter when secondary task workload was low. Nevertheless, examination of the data using a paired T-test (assumptions were not violated, Shapiro-Wilk, p = .111) indicated that there was no statistically significant difference in self-touch frequency between high and low secondary task workload conditions (t(16) = .533, ns). On average, 0.2 fewer face-touches occurred in high secondary workload conditions compared to low workload (Cohen’s d = .15 indicating a small effect). A paired T-test was also used to determine if there was a statistically significant mean difference between face-touching duration and secondary task workload (Shapiro-Wilk, p = .168). However, the data also show no statistically significant differences in self-touch duration (t(16) = 1.056, ns), although, on average, face-touches lasted 2.5 s longer in low secondary workload conditions compared to high workload (Cohen’s d = .36 indicating a small to medium effect).
Table 5. Face touching events during high and low secondary workload conditions in Pampel et al. (Citation2019) (mean and standard deviation).
For primary task workload (explored in Morris et al. Citation2015), there was an apparent higher frequency of face-touches in the lower workload condition (i.e. episodes of the journey that were absent of known elevators of primary workload) (). A paired-samples T-test confirmed that the differences were indeed significant (t(16)=4.59, p < .005), with drivers making more frequent face-touches during episodes of low primary task workload. On average, 21.7 additional face-touches were made when primary workload was low compared to situations of high primary task workload (Cohen’s d = 1.5, indicating a large effect).
Table 6. Frequency of face touching events (FT/h) during high and low primary task workload conditions in Morris et al. (Citation2015) (mean and standard deviation).
Discussion
The primary aim of the study was to identify drivers’ propensity to face-touch during driving and to quantify and characterise these behaviours, for example, regarding the impact of primary and secondary task workload and individual differences. Face-touching has been highlighted as a potential source of viral transmission through self-inoculation and is therefore particularly relevant during the current COVID-19 pandemic, although contextual data on face-touching is also relevant to any situation in which inadequate handwashing may present a risk, for example, after handling a potentially dangerous substance. Such behaviours are also likely to impact on primary task execution which require the use of one’s hand/s. Based on existing literature exploring face-touching in a variety of settings, notably absent of driving, the phenomenon was also expected to be prevalent amongst drivers, particularly given that the car interior is often considered as a private space, thereby enabling more personal touch habits (Squires Citation2010). Utilising a human factors approach, existing datasets captured during two on-road studies were examined and evaluated. It is important to recognise at the outset that both of these studies occurred prior to the COVID-19 pandemic: awareness of self-inoculation through face-touching may now be more prevalent within the public domain and so behaviours may have changed as a result. Moreover, although neither of the original studies purported to be concerned with face-touching behaviour at the time of data collection, drivers were indeed under observation, and this may have influenced the prevalence and nature of these behaviours in a number of (potentially contradicting) ways. For example, the fact that there was a passenger present (in both cases, the researcher) and that the driver was being video-recorded, may have inhibited some face-touching behaviours, particularly so-called, private behaviours, such as nose-picking and eye-rubbing (Hatta and Dimond Citation1984). Conversely, the fact that drivers were taking part in a research study may have elevated their stress levels, thereby increasing the prevalence of face touching (as predicted by Grunwald et al. Citation2014).
Face touching behaviour and workload
Taking all data into account, drivers were observed, on average, touching their face (i.e. their hair, face, neck or shoulders, HFNS) 26.4 times per hour and for an average of 3.9 seconds during each touch. These results tend to fall broadly within a similar range reported in the literature for other contexts. For example, Kwok, Gralton, and McLaws (Citation2015) identified 23.0 face-touches per hour (FT/h) amongst students engaged in a lecture theatre, although it is interesting to note that in contexts where students were seated in an empty room with no specific task to complete, the frequency of face-touching was purportedly higher. Dimond and Harries (Citation1984) observed 40 FT/h amongst students in this scenario. This suggests a possible influence of workload, in effect, lower workload afforded the students more opportunity to engage in face-touching.
There was also evidence of the influence of workload in the current study. Here, primary task workload (i.e. that associated with the primary, driving task) had a direct impact on the frequency of face-touching. When primary task workload was high (i.e. drivers were required to negotiate situations that placed additional physical and/or cognitive demands on vehicle handling and/or information processing, such as preparing to or making a lane change or turn manoeuvre (Jahn et al. Citation2005)), they made significantly fewer face-touches (4.4 FT/h compared to 26.1 FT/h in non-demanding conditions). Naturally, this difference may have been influenced by the availability of the driver’s hands (in other words, it would be difficult to touch one’s face if both hands were already actively engaged in vehicle handling activities, for example). However, the determination of primary task workload included both physical (vehicle handling) and cognitive (information processing) elements, as would be experienced in driving. Needless to say, further studies should seek to isolate these effects.
In contrast, variability in secondary task workload (i.e. any additional, non-driving demands placed on the driver, for example, when interacting with a touchscreen in the car, as explored in Pampel et al. Citation2019), appeared to have no significant effect on the number of face-touches per hour. That said, the secondary tasks explored in Pampel et al. (Citation2019) were fairly rudimentary (i.e. single button presses), and their impact on driver workload may have been negligible. Again, further studies should seek to explore these effects in more detail.
Overall, the middle of the face was the most frequently touched area, with the highest frequencies recorded on the lips and nostrils, both notably mucous membranes. Indeed, in 42.5% of hand to face actions, a mucous membrane was touched. Moreover, these occurred, on average, at a rate of 11.2 touches per hour—in other words, drivers were touching their mucous membrane approximately every 5 min, with the lips receiving the highest contact frequency (6.8 FT/h), followed by nostrils (3.2) and eyes (1.2). The findings are comparable with those reported by Nicas and Best (Citation2008): lips 8.0; nostrils 5.3; eyes 2.5. Zhang et al. (Citation2020) work also support the findings, although their observed rates were generally higher (eyes 2.8; nostrils 14.9; lips 17.1).
Hand-Related factors
Analysis of the areas and surfaces of the hand used in face-touching while driving revealed that, on average, 47.9 hand segments were used per hour, suggesting that multiple hand segments were used during each face-touch. Moreover, the palmar surface of the hand was used for the vast majority of touches, accounting for over 80% of touches, with the fingertips, thumb and thumb tip most commonly employed. Although neither of the studies assessed the quality of participants’ handwashing, Taylor’s (Citation1978) research found that the fingertips, thumb and thumb tips are commonly missed or inadequately cleaned during handwashing. The findings of more recent studies conducted by Pan et al. (Citation2014), Szilágyi et al. (Citation2013) and Vanyolos et al. (Citation2015) are consistent with those of Taylor (Citation1978), and highlight that much of the dorsal surface of the hand is also frequently missed. An interesting finding from this study was that the dorsal surface of the hand was rarely used for face-touching in a driving context. Future education on handwashing practices before entering the car could nevertheless reinforce the necessity of fingertip, thumb and thumb tip washing.
It is interesting to note that there was no statistically significant difference between the primary hand used for face-touching. Elsewhere, evidence suggests that one’s dominant hand is typically used for skill-based behaviour (Scharoun and Bryden Citation2014), suggesting that their non-dominant hand would then be available for non-skill-based activities, such as face-touching. Indeed, in the context of driving, the driver’s dominant hand might be expected to be more heavily involved in the driving task. However, it is noted that the nature of driving on the left side of the road in the UK (i.e. driver is located on the right in the vehicle) means that many of the manual driving-related tasks (changing gear, manipulating infotainment system etc.) are already undertaken using the driver’s typically non-dominant, left hand (data suggests that only 9.3% of the world population is left-handed (Papadatou-Pastou et al. Citation2020)). This may account for the contradictions or confusion observed here. Nevertheless, it remains an important consideration, as different hands may play a different role in self-inoculation. Fierer et al. (Citation2008) microbiome analysis, for example, showed that the dominant hand makes a significantly larger number of contacts with environmental surfaces, compared to the non-dominant hand. Zhang et al. (Citation2020) observations are also consistent with this finding. Subsequently, there may be an elevated risk of self-inoculation when drivers’ dominant hand is used for face-touching. Again, this could be investigated in further work.
Individual differences
Data indicated a lack of differences between genders and different age profiles. This arguably highlights the prevalence of the behaviour across the entire user population, suggesting that all drivers are potentially at risk of self-inoculation and contamination through face-touching while driving. It is also noted, however, that there was considerable variability in face-touching behaviour between participants—with mean touches per hour ranging from nil (one participant made no face-touches) to over 90, and with some drivers making short, fleeting touches and others, more sustained contact. This range of behaviours suggests there may be different underlying motivations and intentions associated with face-touching in the context of driving, including personality factors, for example, which were not explored as part of the current analyses. It is therefore recommended that further work should seek to understand these intrinsic, individual differences in more detail.
Practical implications
The paper presents new data on face-touching while driving, which is of value in and of itself. However, there are also practical implications for these data—not least, in the context of infection transmission and COVID-19. Taking the view that face-touching in the context of a global pandemic is an unintended action, or ‘human error’, and could potentially result in self-inoculation or the transfer of hazardous substances following inadequate or ineffectual handwashing, exploring ways to reduce the likelihood of such actions occurring and/or removing the risks or consequences should they occur is important. This can be achieved through design, but also by encouraging behavioural change.
For example, health awareness campaigns, similar to those already deployed during the current COVID-19 pandemic, may help to improve drivers’ awareness of the potential risks associated with face-touching and encourage them to avoid doing so. These could also reinforce handwashing practices before entering the car, encourage drivers to sanitise their hands when they get in the car, or even place an emphasis on encouraging specific hand roles during daily activities (though it is noted that there were no differences in hand used during the current study). It is also noted that health-care professionals, such as doctors, community nurses and social workers, for whom car travel may form part of their normal working day, already follow established procedures to prevent infection transmission and self-inoculation whilst driving, including good handwashing. Privately-owned car-drivers could be encouraged to follow similar practices. Moreover, reminders and notifications could be located within vehicles in the driver’s normal field of view or incorporated within human-machine interfaces (HMIs) to encourage the adoption and maintenance of these new behaviours (Verplanken and Wood Citation2006).
In addition, technological solutions, such as driver monitoring systems (DMS)—which can already detect fatigue and distraction by tracking eye blink rate and head nodding, among other physical indicators (Sigari et al. Citation2014), may be developed and deployed to detect or predict inadvertent face-touching. As such, the driver could be alerted if the system detects unusual behaviour indicative of face-touching, or be provided with a pre-emptive warning, for example, during periods of low driving workload (when results from this study indicate that face-touching may be higher)—although it is recognised that such warnings could become annoying.
Furthermore, given that surfaces within a car may become contaminated, particularly if that vehicle is shared or occupied by multiple parties, there is also a potential risk of self-inoculation through face-touching following contact with a contamination surface, or fomite. As such, the driver and passenger experience could be re-imagined to reduce transmission risk by reducing or eliminating unnecessary physical contact with in-vehicle surface and devices. Indeed, Jaguar Land Rover, for example, has developed a so-called ‘touchless touchscreen’ that purportedly reduces pathogen transmission (Jaguar Land Rover Citation2020), and emerging interaction companies, such as Ultraleap (https://www.ultraleap.com), are already heavily invested in developing completely touchless in-vehicle interaction solutions, for example using focussed ultrasound and gestures to interact with the car’s infotainment and comfort features (Large et al. Citation2019; Brown et al. Citation2020).
As a final note, the paper situates face touching behaviour firmly within the contemporaneous context of the COVID-19 pandemic, and thus focusses on epidemiological concerns of self-inoculation and infection control. Nevertheless, these data are also relevant to any situation in which a driver may inadvertently transfer a foreign substance to their face, for example, due to inadequate handwashing after handling any potentially hazardous substance. Moreover, understanding how habitual human behaviours (i.e. interactions with oneself) are intertwined with routine task accomplishment (i.e. interaction with things) in a specific context (here, driving), is a fundamental aim and founding principle of Human Factors as a discipline. Even so, analysis of ‘personal’ behaviours such as face-touching seldom feature within Human Factors studies and literature. Thus, the findings also present a new and novel perspective on human behaviour. Indeed, driving as a task already has a multitude of physical touch points and requires the manual manipulations of various control devices. Understanding how these are punctuated by intrinsic human behaviours (such as face touching), and the potential impact these have on human factors, such as health and hygiene, and task-related factors, such as function and performance, is clearly important.
Conclusion
The study presents a new and novel perspective on understanding how habitual human behaviours, such as face-touching, are imbricated with driving using the COVID-19 global public health crisis as a backdrop to frame the research. Scrutinising over 31 h of archival driving footage obtained from previous on-road driving research, the study has shown that, on average, drivers touched their face 26.4 times per hour while driving, with each touch lasting 3.9 s, although individual behaviours varied considerably amongst the participant cohort. Driving complexity and ensuing workload had a significant effect on the frequency of face-touches, with drivers apparently more inclined to touch their face during episodes of low workload. In general, contact with mucous membranes was made 11.2 times per hour (or approximately every 5 min), highlighting the potential viral transmission risk of the behaviour in the context of the COVID-19 pandemic. Analysis of hand segments used in the face-touching actions identified that the palmar fingertips and thumb tip were predominantly used—areas of the hands that are frequently missed in handwashing. It is acknowledged that the original data were collected in 2011 and 2018, pre-COVID-19 pandemic, and that current behaviours may be different. Subsequently, caution should be applied when generalising from the results. Nevertheless, the study provides firm evidence of the potential for self-inoculation through face-touching during routine driving, as well as the potential transmission of other hazardous substances, and this has implications for private and occupational drivers alike. Attention to the in-car environment to discourage face-touching behaviour could be achieved using simple and cost-effective solutions, such as prominent warnings to increase awareness. In addition, more complex technological solutions, such as driver monitoring systems and novel ‘touchless’ interfaces could reduce risks further.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Aiello, A. E., and E. L. Larson. 2002. “What is the Evidence for a Causal Link Between Hygiene and Infections?” The Lancet Infectious Diseases 2 (2): 103–110. doi:https://doi.org/10.1016/S1473-3099(02)00184-6.
- Ali, S. A., M. Baloch, N. Ahmed, A. A. Ali, and A. Iqbal. 2020. “The Outbreak of Coronavirus Disease 2019 (COVID-19)-An Emerging Global Health Threat.” Journal of Infection and Public Health 13 (4): 644–646. doi:https://doi.org/10.1016/j.jiph.2020.02.033.
- Barroso, F., N. Freedman, and S. Grand. 1980. “Self-Touching, Performance, and Attentional Processes.” Perceptual and Motor Skills 50 (3_suppl): 1083–1089. doi:https://doi.org/10.2466/pms.1980.50.3c.1083.
- Beamer, P. I., K. R. Plotkin, C. P. Gerba, L. Y. Sifuentes, D. W. Koenig, and K. A. Reynolds. 2015. “Modeling of Human Viruses on Hands and Risk of Infection in an Office Workplace Using Micro-Activity Data.” Journal of Occupational and Environmental Hygiene 12 (4): 266–275. doi:https://doi.org/10.1080/15459624.2014.974808.
- Boff, K. R., and J. E. Lincoln (Eds.). 1988. “Engineering Data Compendium: Human Perception and Performance, Wright-Patterson Air Force Base”, OH: Armstrong Aerospace Medical Research Laboratory.
- Bradley, J. V. 1967. “Tactual Coding of Cylindrical Knobs.” Human Factors 9 (5): 483–496. doi:https://doi.org/10.1177/001872086700900513.
- Brown, E., D. R. Large, H. Limerick, and G. Burnett. 2020. “Ultrahapticons: “Haptifying” Drivers’ Mental Models to Transform Automotive Mid-Air Haptic Gesture Infotainment Interfaces.” AutomotiveUI '20: 12th International Conference on Automotive User Interfaces and Interactive Vehicular Applications, September 2020, 54–57. doi:https://doi.org/10.1145/3409251.3411722.
- Burnett, G., and A. Irune. 2009. “Drivers’ Quality Ratings for Switches in Cars: Assessing the Role of the Vision, Hearing and Touch Senses.” In Proceedings of ACM Conference on Automotive User Interfaces and Interactive Vehicular Applications, 107–114. New York: ACM.
- Burnett, G. E., and J. M. Porter. 2001. “Ubiquitous Computing Within Cars: Designing Controls for Non-Visual Use.” International Journal of Human-Computer Studies 55 (4): 521–531. doi:https://doi.org/10.1006/ijhc.2001.0482.
- Chapanis, A., and R. Kinkade. 1972. “Design of Controls.” In Human Engineering Guide to Equipment Design, edited by H. P. Van Cott & R. Kinkade. Washington DC: Government Printing Office.
- Chen, Y. J., G. Qin, J. Chen, J. L. Xu, D. Y. Feng, X. Y. Wu, and X. Li. 2020. “Comparison of Face-Touching Behaviors Before and During the Coronavirus Disease 2019 Pandemic.” JAMA Network Open 3 (7): e2016924. doi:https://doi.org/10.1001/jamanetworkopen.2020.16924.
- Cobb, R. W., and J. F. Coughlin. 1998. “Are Elderly Drivers a Road Hazard? Problem Definition and Political Impact.” Journal of Aging Studies 12 (4): 411–427. doi:https://doi.org/10.1016/S0890-4065(98)90027-5.
- Curtis, V., and S. Cairncross. 2003. “Effect of Washing Hands with Soap on Diarrhoea Risk in the Community: A Systematic Review.” The Lancet Infectious Diseases 3 (5): 275–281. doi:https://doi.org/10.1016/S1473-3099(03)00606-6.
- Department for Transport 2020. Transport Use by Mode: Great Britain, since 1 March 2020. London: Department for Transport.
- Dimond, S., and R. Harries. 1984. “Face Touching in Monkeys, Apes and Man Evolutionary Origins and Cerebral Asymmetry.” Neuropsychologia 22 (2): 227–233.
- Drankiewicz, D., and L. Dundes. 2003. “Handwashing among Female College Students.” American Journal of Infection Control 31 (2): 67–71.
- Edwards, D., E. Monk-Turner, S. Poorman, M. Rushing, S. Warren, and J. Willie. 2002. “Predictors of Hand-Washing Behavior.” Social Behavior and Personality: An International Journal 30 (8): 751–756. doi:https://doi.org/10.2224/sbp.2002.30.8.751.
- Ekman, P., and W. V. Friesen. 1969. “The Repertoire of Nonverbal Behavior: Categories, Origins, Usage, and Coding.” Semiotica 1 (1): 49–98. doi:https://doi.org/10.1515/semi.1969.1.1.49.
- Elder, N. C., W. Sawyer, H. Pallerla, S. Khaja, and M. Blacker. 2014. “Hand Hygiene and Face Touching in Family Medicine Offices: A Cincinnati Area Research and Improvement Group (CARInG) Network Study.” Journal of the American Board of Family Medicine 27 (3): 339–346.
- European Centre for Disease Prevention and Control. 2020. Using Face Masks in the Community: Reducing COVID-19 Transmission from Potentially Asymptomatic or Pre-Symptomatic People Through the Use of Face Masks. Stockholm, Sweden: ECDC.
- Fierer, N., M. Hamady, C. L. Lauber, and R. Knight. 2008. “The Influence of Sex, Handedness, and Washing on the Diversity of Hand Surface Bacteria.” Proceedings of the National Academy of Sciences 105 (46): 17994–17999. doi:https://doi.org/10.1073/pnas.0807920105.
- Friard, O., and M. Gamba. 2016. “BORIS: A Free, Versatile Open‐Source Event‐Logging Software for Video/Audio Coding and Live Observations.” Methods in Ecology and Evolution 7 (11): 1325–1330. doi:https://doi.org/10.1111/2041-210X.12584.
- Fuls, J. L., N. D. Rodgers, G. E. Fischler, J. M. Howard, M. Patel, P. L. Weidner, and M. H. Duran. 2008. “Alternative Hand Contamination Technique to Compare the Activities of Antimicrobial and Nonantimicrobial Soaps Under Different Test Conditions.” Applied and Environmental Microbiology 74 (12): 3739–3744. doi:https://doi.org/10.1128/AEM.02405-07.
- GOV.UK. 2020. “Face coverings to be mandatory in shops and supermarkets from 24 July.” Accessed 14 July 2020. www.gov.uk/government/speeches/face-coverings-to-be-mandatory-in-shops-and-supermarkets-from-24-july
- Grunwald, Martin, Thomas Weiss, Stephanie Mueller, and Lysann Rall. 2014. “EEG Changes Caused by Spontaneous Facial Self-Touch May Represent Emotion Regulating Processes and Working Memory Maintenance.” Brain Research 1557: 111–126.
- Hancock, P. A., G. Wulf, D. Thom, and P. Fassnacht. 1990. “Driver Workload During Differing Driving Maneuvers.” Accident; Analysis and Prevention 22 (3): 281–290. doi:https://doi.org/10.1016/0001-4575(90)90019-h.
- Harrigan, J. A., J. R. Kues, J. J. Steffen, and R. Rosenthal. 1987. “Self-Touching and Impression of Others.” Personality and Social Psychology Bulletin 13 (4): 497–512. doi:https://doi.org/10.1177/0146167287134007.
- Hatta, T., and S. J. Dimond. 1984. “Differences in Face Touching by Japanese and British People.” Neuropsychologia 22 (4): 531–534.
- Hendley, J. O., R. P. Wenzel, and J. M. Gwaltney Jr. 1973. “Transmission of Rhinovirus Colds by Self-Inoculation.” New England Journal of Medicine 288 (26): 1361–1364. doi:https://doi.org/10.1056/NEJM197306282882601.
- Jaguar Land Rover 2020. “Jaguar Land Rover develops contactless touchscreen to help fight bacteria and viruses.” Accessed 23 July 2020. https://media.jaguarlandrover.com/news/2020/07/jaguar-land-rover-develops-contactless-touchscreen-help-fight-bacteria-and-viruses
- Jahn, G., A. Oehme, J. F. Krems, and C. Gelau. 2005. “Peripheral Detection as a Workload Measure in Driving: Effects of Traffic Complexity and Route Guidance System Use in a Driving Study.” Transportation Research Part F: Traffic Psychology and Behaviour 8 (3): 255–275.
- Jayaweera, M., H. Perera, B. Gunawardana, and J. Manatunge. 2020. “Transmission of COVID-19 Virus by Droplets and Aerosols: A Critical Review on the Unresolved Dichotomy.” Environmental Research 188: 109819.
- Jenkins, W. O. 1947. “The Tactual Discrimination of Shapes for Coding Aircraft Controls.” In Psychological Research on Equipment Design, Research Report 19, edited by P. Fitts. US Army Air Force, Aviation Psychology Program. Washington, DC: US Government Printing Office.
- Johns Hopkins Coronavirus Resource Center 2021. “Global cases.” Accessed 02 November 2020. https://coronavirus.jhu.edu/
- Kampf, G. 2020. “Potential Role of Inanimate Surfaces for the Spread of Coronaviruses and Their Inactivation with Disinfectant Agents.” Infection Prevention in Practice 2 (2): 100044. doi:https://doi.org/10.1016/j.infpip.2020.100044.
- Kim, H. S., Y. Hwang, D. Yoon, W. Choi, and C. H. Park. 2014. “Driver Workload Characteristics Analysis Using EEG Data from an Urban Road.” IEEE Transactions on Intelligent Transportation Systems 15 (4): 1844–1849. doi:https://doi.org/10.1109/TITS.2014.2333750.
- Knibbs, L.D., L. Morawska, and S.C. Bell. 2012. “The Risk of Airborne Influenza Transmission in Passenger Cars.” Epidemiology and Infection 140 (3): 474–478. doi:https://doi.org/10.1017/S0950268811000835.
- Kousaka, H., H. Mizoguchi, M. Yoshikawa, H. Tanaka, and Y. Matsumoto. 2013. “Role Analysis of Dominant and Non-Dominant Hand in Daily Life.” In 2013 IEEE International Conference on Systems, Man, and Cybernetics, Manchester, UK, 13–16 October, 3972–3977
- Kwok, Y. L. A., J. Gralton, and M. L. McLaws. 2015. “Face Touching: A Frequent Habit That Has Implications for Hand Hygiene.” American Journal of Infection Control 43 (2): 112–114.
- Large, D. R., K. Harrington, G. Burnett, and O. Georgiou. 2019. “Feel the Noise: Mid-Air Ultrasound Haptics as a Novel Human-Vehicle Interaction Paradigm.” Applied Ergonomics 81: 102909. doi:https://doi.org/10.1016/j.apergo.2019.102909.
- Larson, E. L., C. Gomez-Duarte, L. V. Lee, P. Della-Latta, D. J. Kain, and B. H. Keswick. 2003. “Microbial Flora of Hands of Homemakers.” American Journal of Infection Control 31 (2): 72–79.
- Lau, C. H., E. E. Springston, M. W. Sohn, I. Mason, E. Gadola, M. Damitz, and R. S. Gupta. 2012. “Hand Hygiene Instruction Decreases Illness-Related Absenteeism in Elementary Schools: A Prospective Cohort Study.” BMC Pediatrics 12 (1): 52. doi:https://doi.org/10.1186/1471-2431-12-52.
- Luby, S. P., M. Agboatwalla, W. Billhimer, and R. M. Hoekstra. 2007. “Field Trial of a Low Cost Method to Evaluate Hand cleanliness.” Tropical Medicine & International Health : TM & IH 12 (6): 765–771. doi:https://doi.org/10.1111/j.1365-3156.2007.01847.x.
- Lucas, T. L., R. Mustain, and R. E. Goldsby. 2020. “Frequency of Face Touching with and without a Mask in Pediatric Hematology/Oncology Health Care Professionals.” Pediatric Blood & Cancer 67: e28593.
- Michon, J.A. 1985. “A Critical View of Driver Behavior Models: What Do We Know, What Should we Do?” In Human Behavior and Traffic Safety, 485–524. Springer, Boston, MA.
- Morita, K., K. Hashimoto, M. Ogata, H. Tsutsumi, S. I. Tanabe, and S. Hori. 2019. “Measurement of Face-Touching Frequency in a Simulated Train.” E3S Web of Conferences 111: 02027. doi:https://doi.org/10.1051/e3sconf/201911102027.
- Morris, A., R. Welsh, S. Reed, L. Brown, and SA. Birrell. 2015. “The Distraction Effects of Navigation and Green-Driving Systems – Results from Field Operational Tests (FOTs) in the UK.” European Transport Research Review 7 (3): 0717–1867. doi:https://doi.org/10.1007/s12544-015-0175-3.
- Mueller, S. M., S. Martin, and M. Grunwald. 2019. “Self-Touch: Contact Durations and Point of Touch of Spontaneous Facial Self-Touches Differ Depending on Cognitive and Emotional Load.” PLOS One 14 (3): e0213677. doi:https://doi.org/10.1371/journal.pone.0213677.
- Nicas, M., and D. Best. 2008. “A Study Quantifying the Hand-to-Face Contact Rate and Its Potential Application to Predicting Respiratory Tract Infection.” Journal of Occupational and Environmental Hygiene 5 (6): 347–352.
- Ozili, P. K., and T. Arun. 2020. Spillover of COVID-19: Impact on the global economy. Available at SSRN 3562570.
- Pampel, S. M., G. Burnett, C. Hare, H. Singh, A. Shabani, L. Skrypchuk, and A. Mouzakitis. 2019. “Fitts Goes Autobahn: Assessing the Visual Demand of Finger-Touch Pointing Tasks in an on-Road Study.” In Proceedings of the 11th International Conference on Automotive User Interfaces and Interactive Vehicular Applications, 254–261. New York, NY: ACM.
- Pan, S. C., E. Chen, K. L. Tien, I. C. Hung, W. H. Sheng, Y. C. Chen, and S. C. Chang. 2014. “Assessing the Thoroughness of Hand Hygiene: “Seeing is Believing”.” American Journal of Infection Control 42 (7): 799–801. doi:https://doi.org/10.1016/j.ajic.2014.03.003.
- Papadatou-Pastou, M., E. Ntolka, J. Schmitz, M. Martin, M. R. Munafò, S. Ocklenburg, and S. Paracchini. 2020. “Human Handedness: A Meta-Analysis.” Psychological Bulletin 146 (6): 481–524.
- Sattar, S. A., K. E. Wright, B. Zargar, J. R. Rubino, and M. K. Ijaz. 2016. “Airborne Infectious Agents and Other Pollutants in Automobiles for Domestic Use: Potential Health Impacts and Approaches to Risk Mitigation.” Journal of Environmental and Public Health 2016: 1548326. doi:https://doi.org/10.1155/2016/1548326.
- Scharoun, S. M., and P. J. Bryden. 2014. “Hand Preference, Performance Abilities, and Hand Selection in Children.” Frontiers in Psychology 5: 82.
- Sigari, M. H., M. R. Pourshahabi, M. Soryani, and M. Fathy. 2014. “A Review on Driver Face Monitoring Systems for Fatigue and Distraction Detection.” International Journal of Advanced Science and Technology 64: 73–100. doi:https://doi.org/10.14257/ijast.2014.64.07.
- Squires, S. 2010. “Meaning of the Car: Identity vs. Private Space.” TDM Review 17 (1): 16–17.
- Szilágyi, L., T. Haidegger, A. Lehotsky, M. Nagy, E. A. Csonka, X. Sun, K. L. Ooi, and D. Fisher. 2013. “A Large-Scale Assessment of Hand Hygiene Quality and the Effectiveness of the ‘WHO 6-Steps.” BMC Infectious Diseases 13 (1): 249. doi:https://doi.org/10.1186/1471-2334-13-249.
- Taylor, L. J. 1978. “An Evaluation of Handwashing Techniques 1.” Nursing Times 74 (2): 54–55.
- Vanyolos, E., K. Peto, A. Viszlai, I. Miko, I. Furka, N. Nemeth, and P. Orosi. 2015. “Usage of Ultraviolet Test Method for Monitoring the Efficacy of Surgical Hand Rub Technique among Medical Students.” Journal of Surgical Education 72 (3): 530–535.
- Verplanken, B., and W. Wood. 2006. “Interventions to Break and Create Consumer Habits.” Journal of Public Policy & Marketing 25 (1): 90–103. doi:https://doi.org/10.1509/jppm.25.1.90.
- Verwey, W. B. 2000. “ On-line driver workload estimation. Effects of road situation and age on secondary task measures.” Ergonomics 43 (2): 187–209. doi:https://doi.org/10.1080/001401300184558.
- Wang, K. Y. 2014. “How Change of Public Transportation Usage Reveals Fear of the SARS Virus in a City.” PLOS One 9 (3): e89405. doi:https://doi.org/10.1371/journal.pone.0089405.
- Wilson, A. M., M. P. Verhougstraete, P. I. Beamer, M. F. King, K. A. Reynolds, and C. P. Gerba. 2020. “Frequency of Hand-to-Head, -Mouth, -Eyes, and -Nose Contacts for Adults and Children during Eating and Non-Eating Macro-Activities.” Journal of Exposure Science & Environmental Epidemiology 31 (1): 34–44.
- World Health Organization (WHO). 2020. Coronavirus Disease (COVID-19): Situation Report, 173. Geneva: WHO.
- Zhang, N., W. Jia, P. Wang, M. F. King, P. T. Chan, and Y. Li. 2020. “Most Self-Touches Are With the Nondominant Hand.” Scientific Reports 10 (1): 1–1.