
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
This study investigates the effect of quick coherence technique (QCT) on commercial pilots’ resilience to the unprecedented impact of a pandemic. Eighteen commercial pilots voluntarily participated in a 2-day training course on QCT followed by 2 months of self-regulated QCT practicing during controlled rest in the flight deck and day-to day life. There are subjective and objective assessments to evaluate the effects of QCT on commercial pilots’ psychophysiological resilience. Results demonstrated that QCT training can significantly increase pilots’ psychophysiological resilience thereby improving their mental/physical health, cognitive functions, emotional stability and wellness on both subjective (PSS & AWSA) and objective measures (coherence scores). Moreover, pilots who continued practicing self-regulated QCT gained the maximum benefits. Current research has identified great potential to enhance pilots’ mental/physical health via QCT training. Operators can develop peer support programs for pilots to increase resilience and maintain mental and physical health using the QCT technique.
Practitioner summary: QCT breathing has been proven to increase commercial pilots’ resilience by moderating psychophysiological coherence, strengthening mental/physical capacity and sustaining positive emotions to deal with the challenges both on the flight deck and in everyday life.
Pilots have suffered from the impact of the Covid-19 pandemic across many factors including social, economic, mental, physical, emotional, and operational issues
Biofeedback training can increase commercial pilots’ resilience by moderating psychophysiological coherence, strengthening mental and physical capacity
Self-regulated practicing QCT to form a habitual behaviour is required to sustain the maximum benefits either in the flight or day-to-day life
QCT is an effective intervention for aviation authorities and airline operators to develop peer support programs to increase pilots’ fatigue resilience
HIGHLIGHTS
1. Introduction
The outbreak of the COVID-19 pandemic induced an unprecedented impact on the aviation industry with the grounding of aircraft, cancellation of flights, strict travel bans and closure of international borders. According to the International Air Transport Association (IATA Citation2021), there were over 18,000 aircraft parked up, representing 66% of the world’s commercial transport fleet; the number of airport pairs in March 2021 was only 50% of the connections of pre-pandemic. The International Civil Aviation Organisation (ICAO Citation2022) noted that COVID-19 has caused an overall reduction of 60% passengers and around a 372-billion-dollar loss of airline revenue compared to pre-pandemic levels in 2019. The rapid reduction of scheduled flights caused by the pandemic led to thousands of commercial pilots not flying, and many were furloughed or laid-off by airlines. Commercial pilots were threatened with redundancy, unwelcome changes to their employment contracts such as lower pay, and the prospect that some may never fly for a living again. It further resulted in a lack of stability with many also suffering financial pressure, which could undermine their mental/physical heath, cognitive functions, and wellness (Alaminos-Torres et al. Citation2022). Airline pilots’ mental health and psychological states have been brought to the forefront and have been the focus of increasing attention in aviation since the Germanwings Flight 9525 crash in 2015. ICAO (Citation2016) issued a working paper to convene a task force to analyse recent aviation accidents in which a mental health condition was cited as a ‘causal factor’. Furthermore, the Federal Aviation Administration (FAA Citation2021) has included the consideration of psychological condition and mental health in the medical certification of commercial pilots. The European Union Aviation Safety Agency (EASA Citation2016) also introduced new rulemaking related to the management of pilots’ mental health issues. More recently, the aviation industry and pilot unions are addressing the promotion of positive wellbeing and the practice of healthy behaviours for aviation professionals (Cullen, Cahill, and Gaynor Citation2021; Flight Safety Foundation Citation2020). Effective mitigations for these negative impacts are required to improve pilot’s stress resilience and cognitive functions in order to maintain aviation safety.
2. Related works
The quick coherence technique (QCT) is a mental and emotional self-regulation technique that has been shown to increase one’s level of heart-rate variability (HRV) coherence. Learning the breathing technique was facilitated using HeartMath Inner Balance technology. Breathing technique has been proven to be effective in improving psychological resilience and to contribute to coping with stress, anxiety, control emotions, and decision-making (Kloudova, Kozlova, and Stehlik Citation2019). Breathing techniques have been used by military pilots for preventing loss of consciousness when facing prolonged hypoxia and hyperventilation conditions for decades (FAA Citation2016). In the context of the COVID-19 pandemic, there are increasing risks that pilots may experience burnout due to overload stress and serious mental health issues above the normal baseline stressors, which can negatively influence their wellbeing and job motivation (Demerouti et al. Citation2019). Currently, there are thousands of pilots worldwide suffering from redundancy, unpleasant changes to their contracts, increased duty hours with lower pay rates which may have potential on developing mental/physical health issues and may jeopardise aviation safety (Vuorio and Bor Citation2020). And this impact will persist and translate into further consequences with health and safety threats to pilots and airlines even after the pandemic crisis has passed.
2.1. Pilots’ psychological states affected aviation safety
The commencement of the COVID-19 pandemic in late 2019 caused an abrupt cancellation of flight operations which not only limited pilots’ proficiency in performing routine tasks, but also increased pilots’ stress levels and operational risk due to new procedures related to COVID-19 safety and health regulations (Olaganathan and Amihan Citation2021). The requirements to wear Personal Protective Equipment (PPE) including face masks, gloves and goggles may have had negative effects on pilots’ operational performance, as the PPE may reduce pilots’ performance by diminishing their perception on sight, hearing, touch, and communication during flight operations. This can then increase crews’ mental and physical workload, reduce handling abilities and crew resource management skills (IFALPA Citation2020; CAA Citation2020). Pilots’ psychological issues persist as an insidious threat to aviation safety due to the impairment of the pilot’s cognitive functions and task performance (Marin et al. Citation2011). According to the causes review of aviation accidents from the database of the National Transportation Safety Board (NTSB) and National Aviation Safety Data Analysis Centre (NASDAC), 13.3% of the accidents are associated with the mental or physical conditions of the pilots (Shappell et al. Citation2007). Furthermore, a survey based on thousands of active pilots showed that 12.6% airline pilots met the depression threshold and 4.1% pilots reported having suicidal thoughts (Wu et al. Citation2016). Although commercial airlines have focussed on pilot’s mental health by the management of crew fatigue and alertness (Cahill et al. Citation2021), stress-related psychological issues and wellbeing detriments are not properly addressed within existing airlines safety management systems due to crew’s concern on loss of their medical certification and job (Vuorio and Bor Citation2020).
Social isolation, mental stress, and anxiety at the time of the severe acute respiratory syndrome (SARS) epidemic resulted in an extremely high rate of suicide deaths (Yip et al. Citation2010). The risk of suicide is increased due to economic deterioration and social isolation particularly affecting aviation professionals, even worse, pilots were conscious that they were exposed to potentially high risk of infection with COVID-19. Pilot aircraft-assisted suicide such as Germanwings Flight 9525 in commercial aviation is an unusual event. However, research proposed that pilot aircraft-assisted suicide is 0.33% (with 95% CI, 0.21–0.49) in general aviation in United States (Vuorio et al. Citation2014). It is recognised that the pandemic may increase suicide rates just as during the SARS crisis of 2003. However, the association between pilot suicides and social change such as unpaid leave, furlough, financial risks and quarantine isolation have not been studied yet. A study of 442 commercial pilots demonstrated that mental health was found to be associated with occupational dispute, fatigue, insufficient flying time and flying patterns, together with an inability to relax and a lack of social support (Cooper and Sloan Citation1985). To effectively manage the negative impact of pilot’s psychological issues, mental health professionals work closely with aeromedical professionals for pilot selection, assessment, and monitoring of pilots’ mental health (Bor, Field, and Scragg Citation2002). Relevant policies and strategies aim to improve screening, evaluation, and management of pilots’ mental health have been taken by aviation authorities and airline operators. FAA (Citation2016) made a commitment to combat the dangers of mental health issues in aviation by removing the stigma surrounding psychological problems in the aviation industry, so that pilots are more likely to self-report, get treatment, and return to work. EASA (Citation2018) required aviation medical examiners to focus on pilot mental health and well-being in their annual pilot assessment after the Germanwings accident. The quick coherence breathing technique has been demonstrated as an effective method to increase air traffic controllers’ fatigue resilience and operational risk management (Li, Zhang, and Kearney Citation2022). Based on the above literature, there is an alternative hypothesis to be tested as follows ‘H1: there is a significant interaction on pilots’ coherence between practicing QCT and flight duty’.
2.2. Biofeedback technique improved mental health
Individual resilience is the ability to cope with a crisis and return to pre-crisis status quickly using mental processes and behaviours in promoting personal assets and protecting self from the potential negative effects of stressors (Robertson et al. Citation2015). Self-regulated QCT can provide individuals with a greater awareness as to how they can regulate their own psychological and cognitive functioning using physiological signals. Empowered with a breathing technique its possible for one to shift one’s own physiology into a more coherent state. QCT can effectively enhance individual resilience which is associated with improved psychophysiological coherence, cognitive functions, and general health (Edwards, Edwards, and Honeycutt Citation2022; McCraty and Tomasino Citation2006). Research has demonstrated that breathing conciliation is able to facilitate individuals’ Autonomic Nervous System (ANS) functions by monitoring physiological responses to stress (Carroll and Winslow Citation2017). QCT has been proved as an effective intervention to improve air traffic controllers fatigue resilience and mitigate the negative impact of accumulated workload (Li, Zhang, and Kearney Citation2022). QCT is a self-regulation technique based on a breathing pacer which provides real-time response to the trainee’s current state (HeartMath Citation2022). Psychophysical coherence is associated with the alignment of physical and mental functions which can facilitate a well-established relationship between cognitive information processing and task performance (Bradley et al. Citation2010).
Increased coherence reflects the abilities of self-regulated emotions more consistent with intuitive, intelligent, and stable inner reference which is correlated with improved mental health, wellness, and cognitive functioning (McCraty Citation2011; Ireland Citation2010). The social, economic, and personal challenges of COVID-19 threaten a pilot’s mental health and well-being in several ways. There is a pressing need to develop psychological support in order to address pilots’ stress, distress and the potential for increased pilot suicides as a direct impact of the pandemic. Previous research demonstrated that practicing an 8-week intervention programme of breathing technique can significantly reduce stress and mental health issues, as well as increasing psychological and physical functions (Ehsan et al. Citation2019). Psychophysiological coherence can boost the ability of individuals to resist and recover from negative experiences such as stress and fatigue (Rutter Citation2007). The breathing is a simple technique which requires individuals to breathe deeply and slowly at a fixed rate around 6 to 10 times per minute to achieve the maximum benefits. Paced breathing can lead to a better psychological state through modulation of ANS which has been proven to have positive effects in the reduction of feelings of stress and anxiety (Ma et al. Citation2017; Aristizabal et al. Citation2020). Therefore, two alternative hypotheses are raised in this research as follows, ‘H2: there is a significant improvement on pilots’ wellness score based on QCT training’; and ‘H3: there is a significant decrease on pilots’ perceived stress based on QCT training’.
2.3. Self-regulation strengthened wellness
Self-regulation has been defined as recurring efforts to optimise one’s cognitive, motivational, and behavioural processes leading to goal fulfilment (Winne and Jamieson-Noel Citation2002). It has been suggested that the quantity and quality of one’s self-regulation capacity is significantly associated with developing expert levels of competence and task-specific cognitive performance (Ericsson Citation1997; Singer Citation2000). Specific skill acquisition can be achieved progressively with regular practice that learners self-regulate in three sequential phases: forethought, performance, and self-reflection (Zimmerman and Kitsantas Citation1997; Derossis et al. Citation1998). Previous research has demonstrated that breathing technique can provide clear awareness of psychophysiological coherence state and improve self-regulation in practicing engagement (Field et al. Citation2018). Furthermore, the long-term practice of psychological interventions can significantly improve cognitive information processing and task performance in workplace (Thomas and Fogarty Citation1997; Slimani et al. Citation2016). Regular practice of breathing techniques have been proved to have positive effects on individual’s ANS functions by facilitating heart rate response, and thus improve both physical and psychological health (Joshi, Joshi, and Gokhale Citation1992; Mourya et al. Citation2009). The long-standing practice of mindfulness can significantly increase wellness and stress management skills (Kingston et al. Citation2007; Roeser et al. Citation2012). Similarly, the long-term practice of breathing technique has been proven to have effective moderation effects on perceived stress, and improvement in cognitive functions, and mental health (Szulczewski Citation2019).
To maintain mental health and wellness requires regular practice of intervention techniques over a prolonged period of time (Erikssen et al. Citation1998; Gardner and Rebar Citation2019). Regular practice over a long term is associated with better training outcomes and skill acquisitions compared to short-term massed practice (Spruit, Band, and Hamming Citation2015). Long-term practice has multiple effects on task performance and automatic behaviours, including increasing the response speed and accuracy of goal-directed action selection, reducing the demand of cognitive workload and stress required to perform the task, as well as rendering the practiced behaviour habitual (Haith and Krakauer Citation2018). Habit has been proposed to represent a form of self-control and autonomy, protecting regular practice in the longer-term against shorter-term motivation losses (Galla and Duckworth Citation2015). Therefore, the formation of a positive habit of practicing QCT regularly can optimise pilots’ coherence and task performance. Consistent practice breathing technique can effectively improve psychophysical coherence and emotion-regulation ability (Reyes Citation2014), and reduce health care costs (Bedell and Kaszkin-Bettag Citation2010). Therefore, the current study applies psychophysiological coherence as the hallmark indicator of pilot’s perceived stress and resilience in the cockpit and everyday life. Based on the above literature, there are two alternative hypotheses to be tested as follows, ‘H4: there is a significant correlation between frequency of practicing QCT and pilots’ stress level’; and ‘H5: there is a significant correlation between frequency of practicing QCT and pilots’ wellness score’.
2.4. Motivations and hypotheses
COVID-19 significantly reduced the volume of flights by up to 70% in 2020 compared with 2019, which caused the majority of pilots to be furloughed and mental and physical issues. Furthermore, new regulations on wearing PPE induced additional procedures, risk of infection, long and irregular working hours, isolation during quarantine and potential loss of employment are stressors which can lead to psychological strains and physiological issues (IATA Citation2020). There is a pressing need to improve aviation safety by providing coherence training to increase pilots’ resilience to manage the impacts of a pandemic. This research is to evaluate the effectiveness of the QCT training on moderating pilots’ psychophysiological coherence, perceived stress, and wellness during the impacts of the COVID-19 pandemic.
3. Method
3.1. Participants
Eighteen commercial pilots who are working for an international airline volunteered to participate in this research. The participants’ ages ranged from 30 to 58 years old (M = 45.1, SD = 7.5) with different aircraft type ratings and flight hours (M = 11,597.2, SD = 5496.8). Participants’ service years are between 3 years and 26 years (M = 14.7, SD = 7.8). The research ethical approval was granted in advance of the research taking place. All participants were informed that this research is evaluating the effectiveness of quick coherence technique (QCT) on stress and fatigue risk management in flight operations as related to the impacts of the Covid 19 pandemic. Participants were guaranteed their right to withdraw from this research at any stage and provided their signed consent form. All collected data is managed in accordance with the United Kingdom Ethical Code and the General Data Protection Regulation (GDPR).
3.2. Apparatus and materials
3.2.1. Inner balance
The Inner Balance Bluetooth sensor and Inner Balance App are developed by HeartMath (). It is a mobile Bluetooth device to measure psychophysiological coherence which indicates how physical and mental states are affected by the automatic nervous system (ANS) including both the sympathetic and para-sympathetic systems. It can be easily connected with personal mobile devices (using android or iOS) for training purposes. Furthermore, it provides additional information on start and end times of practice, average coherence and cumulative achievement scores are also available on the HeartCloud apps (right-hand side on ). Visual feedback on coherence states comprises of red (low), blue (medium) and green (high) coloured bars with percentage indicators summed up to 100%. This study uses high percentage (green) as the coherence indicator for data analysis. A coherent heart rhythm is a stable regular repeating rhythm resembling a sine wave at a single frequency between 0.04 and 0.24 hz. The scoring algorithm updates the coherence score and achievement score at five second intervals. The achievement score is the sum of all individual low, medium and high coherence scores (HeartMath Citation2014).
Figure 1. The Inner Balance device is a state of the art, ultra-low Bluetooth device with 125 hz sample rate measuring HRV parameters to optimise accurate HRV and QCT training.

3.2.2. Perceived stress scale (PSS)
Perceived Stress Scale (PSS) is a self-reported subjective questionnaire which was developed to measure the degree that ten scenarios in an individual’s life are considered as stressful (Cohen, Kamarck, and Mermelstein Citation1983). The PSS has become one of the most widely used psychological instruments for measuring perceived stress. It has been used in studies assessing the stressfulness of situations and the effectiveness of stress-reducing interventions (Lee Citation2012; Oró et al. Citation2021). The PSS consisted of ten items evaluating the degree to which individuals believe their life has been unpredictable, uncontrollable, and overloaded during the previous month. The PSS-10 also includes a number of direct queries about current levels of experienced stress. The assessed items are general in nature rather than focussing on specific events or experiences. Therefore, it can be used to assess both long-term and short-term situations in one’s life which are considered stressful (Bastianon et al. Citation2020).
3.2.3. Ardell wellness self-assessment
Ardell Wellness Self-Assessment (AWSA) is often applied to diagnose participants’ state of wellness and stress index using a seven-point Likert scale (from +3 to −3) that measures individual wellbeing. Ardell Wellness test consists of 25 questions incorporating physical, mental, emotional, and social aspects of health which offer a balanced assessment of varied stress sources. Where the higher the total score, the higher the happiness of that participant, and vice versa (Ardell Citation1983). The AWST scale is used to collect data on the subjective well-being of pilots during the furlough related to covid-19.
3.3. Training syllabus
QCT training took 2 days, and the training syllabus consisted of introducing the theoretical framework of psychophysiological coherence and resilience, practicing the QCT breathing technique, demonstration and exercising of breathing techniques, and Automatic Nervous System, Energy depletion and renewal exercise, and applying QCT to optimise effective communication and interpersonal relationships based on the HeartMath QCT training syllabus. Two licenced Resilience Instructors and Coherence Advantage Instructors from HeartMath UK delivered the training. The application of Inner Balance together with QCT is aimed to boost participants’ psychophysiological state via simple and effective breathing techniques. There are two steps to QCT including step-1 heart-focussed breathing and step-2 activation of a positive feeling which can integrate with the freeze frame. The Inner Balance device facilitates participants’ practicing QCT by providing visual signs reflecting heart rhythms and recharging energy based on moment-to-moment changes in heart rate via a personal mobile device.
3.4. Research procedures
Participants voluntarily attended this 2-day psychophysiological coherence training program following notification of the study on the airline’s internal notification system. There was neither an incentive nor a financial allowance for individuals participating in this research. All participants went through the same procedures as follows, (1) briefing the research objectives and 2-day training syllabus; (2) participants provide their signed consent form with agreed data management plan; (3) participants conduct pre-training subjective assessments on AWSA and PSS; (4) participants provide pre-training HRV as baseline for 5 min using Inner Balance connected to his/her personal device (Android or iOS); (5) participants attend 2-day coherence training on practicing QCT and stress management; (6) participants performed their post-training assessments using AWSA, PSS and Inner Balance for psychophysiological coherence once training is completed. Furthermore, participants were encouraged to practice QCT for 5-min sessions as often as they could either off-duty or on-duty in the flight deck. While pilots are in the flight deck, they must comply with the airline’s controlled rest policies at all times while using inner balance to collect baseline data, then practice QCT for 5 min. If this is not possible or is interrupted by an emergency event this, the safety of the flight takes priority; (7) Debriefing and response to participants’ comments; (8) participants were informed that the subjective assessments on both AWSA and PSS will be forwarded to them 2 months later to trace the QCT training effects. All participants were advised to forward their experiences and comments on practicing QCT to the principal researcher on a weekly basis. All participants’ coherence data was stored on the HeartCloud which can only be accessed by the project leader using encrypted username and passwords to follow GDPR requirements.
4. Results
4.1. Sample characteristics
One-way repeated measure ANOVA is applied to investigate QCT training effects on pilots’ AWSA and PSS levels among pre-training, post-training and after 2-months of practicing. The correlations between pilots practicing QCT sessions with AWSA and PSS were analysed by Pearson’s correlation coefficient. There was no outlier observed by boxplots. The assumption of normality is verified by Q-Q plots and the homogeneity of covariance assumption was verified by Mauchly’s test (p > .05). The post-hoc pairwise comparisons were accomplished by Bonferroni, and effect sizes of samples were quantified by partial eta square (). The descriptive statistics are shown as . Furthermore, two-way ANOVA is applied to examine pilots’ psychophysiological coherence between QCT training effects (baseline vs practicing QCT) and flight duty (on-duty vs off-duty) for QCT training effects in flight operations. The descriptive statistics are shown as .
Table 1. Means and standard deviations of pilot’s AWSA and PSS scores among three stages of QCT training.
Table 2. Means and standard deviations of recorded sessions (N) of all participated pilots’ psychophysiological state between baseline and practicing QCT while off-duty (daily life) and on-duty (flight operations) for 2-months practice.
4.2. Qct training moderating pilots’ psychophysiological resilience
The two-way ANOVA results indicated a significant interaction on pilots’ psychophysiological state between frequencies on practicing QCT and flight duty, F (1, 3285) = 6.46, p = .011, = 0.002 (). Therefore, ‘H1: there is a significant interaction on pilots’ psychophysiological state between practicing QCT and flight duty’ is supported. Furthermore, simple main effect analysis on pilots ‘practicing QCT’ within each group on ‘flight duty’ showed that the psychophysiological state on practicing QCT is significantly higher than baseline on both off-duty and on-duty (p < .001). Another simple main effect analysis on pilots’ ‘flight duty’ within each group on ‘practicing QCT’ revealed that pilots’ baseline psychophysiological state while off-duty is significantly lower than on-duty (p < .001). Moreover, a significant main effect was found on the factor ‘practicing QCT’, F (1, 3285) = 673.62, p < .001,
= 0.170. There is also a significant main effect on ‘flight duty’ on pilots’ psychophysiological state, F (1, 3285) = 6.22, p = .013,
= 0.002. The details of two-way ANOVA are shown as ( and ).
Figure 2. The differences of AWSA and PSS scores among three different stages on QCT pre-training, post-training and 2-month self-regulated practicing.
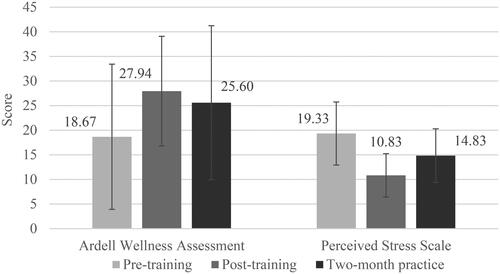
Figure 3. The interaction effect of self-regulated practicing QCT and flight duty on pilots’ psychophysiological coherence.
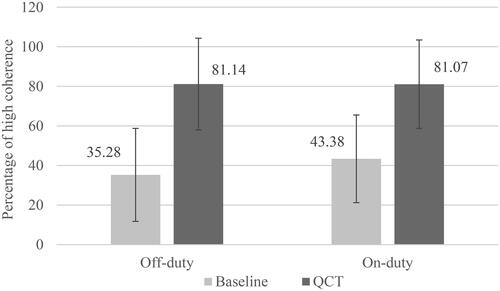
Table 3. Two-way ANOVA interactions, simple main effects, and main effects on pilots’ psychophysiological coherence between practicing QCT and flight duty.
4.3. QCT training effects
The results of one-way repeated measures ANOVA indicated that there is a significant improvement on pilots’ wellness scores among three stages on QCT training, F (2, 34) = 5.12, p = .011, = 0.23. Furthermore, post-hoc pairwise Bonferroni comparison revealed that the post-training wellness score is significantly higher than pre-training (p = .007) and 2-month practice ( and ). Therefore, ‘H2: there is a significant improvement on pilots’ wellness score based on QCT training’ is supported. Also, there is a significant decline on pilots perceived stress levels among three stages on QCT training, F (2, 34) = 23.07, p < .001,
= 0.58. Furthermore, post-hoc pairwise Bonferroni comparison revealed that pilots’ stress level is the lowest on post-training, followed by 2-month practice and pre-training is the highest (p = .021) ( and ). Therefore, ‘H3: there is a significant decrease on pilots’ perceived stress based on QCT training’ is supported.
4.4. Correlation on practicing QCT sessions and resilience
Pilots’ self-regulation of practicing QCT for 2 months varied from 19 to 376 sessions (M = 192.1, SD = 114.0). Pearson’s correlation analysis is applied to examine the association between the frequencies of practicing QCT with PSS and AWSA scores. The frequencies of practicing QCT shown negatively correlated with the PSS score after 2-month trials, r = −.48, p = .045. Therefore, ‘H4: there is a significant correlation between frequency of practicing QCT and stress level’ is supported. Pilots who conducted more sessions of practicing QCT are associated with lower stress levels. However, there is no significant correlation between practicing QCT sessions and pilots’ AWSA scores (r = .13, p = .622). Therefore, ‘H5: there is a significant correlation between frequency on practicing QCT with wellness’ is not supported. The frequencies of practicing QCT have no association with pilots’ wellness for 2-month trials.
5. Discussion
Pilots have suffered from the impact of the Covid-19 pandemic in many ways (Olaganathan and Amihan Citation2021). This unprecedented challenge and disruption led to a range of negative stressors for pilots including uncertainty of employment and high risk of infection. The forecasts for air transportation recovery also increased pilots’ stress as global flight restrictions were foreseen to run through the post-pandemic (Miani et al. Citation2021). Suffering from prolonged furlough, pilots appreciated the opportunity to return to the flight deck again. However, the lack of recency in practicing operational procedures and operating automation systems resulted in pilots suffering from skill fade which induced high stress level and associated with incidents (EASA Citation2021). The effectiveness of QCT in the flight deck (on-duty) and day-to-day life (off-duty) were evaluated and discussed in relation to the hypotheses in current research.
5.1. Qct biofeedback training increasing pilots’ resilience
The research finding confirms H1: ‘there is a significant interaction on pilots’ psychophysiological state between practicing QCT and flight duty’ is supported. The main effects of ‘practicing QCT’ showed that pilots’ coherence significantly increased from 35.86% to 81.38% after practicing QCT. The simple main effect of ‘flight duty’ demonstrated that pilots’ coherence between off-duty and on-duty are different, however practicing QCT increased pilots’ coherence to an equal level (81.14% off-duty vs 81.07% on-duty) without statistical significance (p = .974), which indicated the effectiveness of QCT in improving pilots’ coherence on both day-to-day life and in the flight deck (). This finding is consistent with previous research which proposed QCT training significantly improved air traffic controllers’ fatigue resilience and perceived workload related to rotating shift works (Li, Zhang, and Kearney Citation2022). In this study, pilots practiced QCT sessions during the controlled rest in flight deck, which is an effective strategy of taking breaks at work to help pilots re-charge their mental and physical resources during long-haul flights (Caldwell Citation2005), such as 12 h from London to Hong Kong. The results also support H2: ‘there is a significant improvement on pilots’ wellness score based on QCT training’ which may reflect the effectiveness on QCT training integrated with positive psychology and HRV biofeedback breathing techniques. The pandemic lockdown caused social isolation, economic stresses and more complicated protection procedures during flight operations which may induce negative impacts on pilots’ mental and physical health. QCT can increase pilots’ coherence which is able to improve pilots’ wellness and mitigate pilots’ stress levels related to day-to-day life and flight duty.
The COVID-19 pandemic imposed restrictions on flight operations and created additional stressors that may reduce pilots’ capacity and proficiency to perform their tasks as effectively as would be usual in the flight deck (CAA Citation2020). The benefits of practicing QCT are reported from pilots based on their experiences both on-duty and off-duty within 2 months of QCT trials. In the same vein, H3: ‘there is a significant decrease on pilots’ perceived stress based on QCT training’ is supported. Practicing QCT can lead to increased individual emotional calmness and wellness and reduce perceived stress (). Pilots were impressed that the simple biofeedback could have such astonishing power with positive impact on their performance in the flight deck and day-to-day life. QCT were reported by pilots in relation to increased resilience to stress situations (annual licence revalidation) and significant improvement on task performance (simulator check and flight operations) and physical functions (COVID-19 jabs recovery and blood pressure back to normal) (detailed information see ). Pilots also mentioned that the QCT biofeedback could effectively promote fatigue recovery and stress management during the controlled rest in the flight deck. The objective data analysis and pilots’ subjective feedback support the contention that practicing QCT biofeedback can significantly improve mental resilience and enhance ‘good mood’ while on duty in the flight deck and in everyday life ().
Table 4. Summaries on pilots’ experiences shared while practicing QCT both on controlled reset in the flight deck and day-to-day life.
5.2. Practicing more QCT sessions associated with better resilience
According to results on Pearson correlation analysis, H4: ‘there is a significant correlation between frequency on practicing QCT and pilots’ stress level’ is confirmed. Pilots who self-regulated by practicing more QCT sessions are associated with lower level of perceived stress after the 2-month trials, which is associated with the research by Field et al. (Citation2018) indicating that the biofeedback intervention can benefit both psychophysiological coherence and self-regulation by improving the awareness of practice effects. This finding also supports that pilots’ habit behaviours are critical to strengthening their learning from the 2-day training. The effective QCT biofeedback training must be regularly practiced achieving effective stress management in both everyday life and flight duty. In the process of habitual behaviour formation, the effectiveness and strength of habitual behaviours have strong positive correlations with higher frequency and longer duration of self-regulated practice (Gardner, de Bruijn, and Lally Citation2011; Rebar et al. Citation2016). Pilots also shared their experience of practicing QCT with the following benefits ‘lower blood pressure on annual medical check, relief of headache after COVID-19 jab, calmness, good sleep, simple technique with science backing’. The phenomenon of self-regulated QCT practice allows pilots to moderate their physiological and psychological wellness, which positively influenced on cognitive processes, emotional stability and stress resilience to improve the quality and accuracy of in-flight decision-making and critical operational manoeuvres in emergency scenarios (Winne and Jamieson-Noel Citation2002). Increasing coherence will also assist pilots in adapting to stress scenarios and maintaining mental and physical equilibrium while facing challenging situations and adversity. Previous research also indicated that the self-regulation on continuous practicing a task leads to improved skill level and reduced cognitive workload while performing complex tasks (Haith and Krakauer Citation2018; Slimani et al. Citation2016).
The results on Pearson correlation analysis did not support H5: ‘there is a significant correlation between frequency on practicing QCT and pilots’ wellness score’, although abundance of practice is necessary to generate proficiency and automaticity of specific actions (Fisk and Schneider Citation1983; Dolan and Dayan Citation2013). This finding is inconsistent with previous research on practicing more biofeedback technique associated with better psychological wellness (Kruskal et al. Citation2019). There are several factors which may have influenced this finding including the small sample size, individual difference of motivation, and the inherent differences in the psychophysical characteristics between perceived stress level (H4) and wellness (H5). Wellness is a holistic perspective integrating a standard of both psychological and physical characteristics including five key elements: self-responsibility, nutritional awareness, physical fitness, stress awareness and management, and environmental sensitivity (Ardell Citation1983). Comparing with PSS, AWSA contains border range of concepts of physical, emotional, and spiritual well-being. The moderation of perceived stress tends to be associated with the stress management and emotion regulation skills, while facilitating wellness involved incorporating all five dimensions which are more challenging to validate. Therefore, the promotion of wellness is more complicated and more vulnerable to individual differences, which led to the difficulty of getting significant association between practice QCT sessions and wellness on the small-size samples of 18 commercial pilots.
It is important to note that the regular practicing of a biofeedback technique learned from the training syllabus is to strengthen behaviour by automatic enacted support and is insusceptible to context changes (Nilsen et al. Citation2012). With some behaviours, one practice is sufficient to gain desired health outcomes, such as a single vaccination may yield immunity to virus; but practicing one mindfulness session will not achieve the same health benefits as regular activity over a prolonged period of practice (Gardner and Rebar Citation2019). Therefore, the self-regulated practice on QCT at a regular frequency and over a prolonged period will gradually form a habitual behaviour that can facilitate pilots’ performance to respond rapidly and appropriately with less cognitive workload and mental stress. Therefore, long-term QCT practice can effectively moderate pilots’ perceived stress and negative emotions during events such as the COVID-19 pandemic, promoting psychological coherence and mental/physical health. Pilots’ mental and physical issues have significant capacity to impact aviation safety which may have deteriorated after the Covid-19 pandemic (Marin et al. Citation2011; CAA Citation2020). Therefore, encouraging pilots to practice self-regulated QCT regularly will not only improve their coherence and mental/physical health, but also enhance their performance and aviation safety for long-standing effect.
5.3. Limitations and future works
This empirical study demonstrated a biofeedback QCT intervention can increase commercial pilots’ coherence and stress resilience. However, there are a few constraints and more potential applications identified with this research. Firstly, only 18 pilots’ subjective data has been collected among QCT pre-training, post-training and 2-month later post-training on both AWSA and PSS levels. Such a small sample size may decrease statistical power and skew the results. It will be better when further data has been collected with future research. Secondly, there are only 225 QCT datasets collected while pilots were on-duty in the flight deck compared with 3064 QCT data collected while pilots were off-duty. Nevertheless those 225 sessions of QCT data are extremely valuable for empirical research and very difficult to collect due to the limitations on the environment of flight operations and airline safety regulations. There are some invalidated data due to emergency situations on the flight deck which pilots interrupted the QCT sessions for operational safety reasons. The authors would like to conduct further research to accumulate more validated data in the flight deck in the future. Thirdly, there are individual differences on self-regulation which may be a confounding variable to the psychophysiological coherence. Finally, the collection of pilots’ coherence data in the flight deck was only available on long-haul flights which had a ‘controlled-rest’ policy allowing pilots to practice QCT while discharged from flight duty. On the other hand, the subjective data on pilots’ AWSA and PSS were able to collect from both long-haul and short-haul flights. The differences on the operational characteristics between long-haul and short-haul flights may be associated with different stress levels and mental and physical demands which will have to be investigated in a future study.
6. Conclusions
The COVID-19 pandemic induced medical risks to commercial pilots including mental and physical health issues. Furthermore, the social, economic, employment, emotional and personal relationship challenges are presented as threats affecting pilots’ emotional stability and wellbeing. This research applies QCT biofeedback as an intervention to increase pilots’ resilience and mitigate COVID-19 negative impacts during flight operations. Empirical data collected on both pilots’ everyday life (off-duty) and in the flight deck (on-duty) demonstrated that biofeedback training can effectively improve pilots’ psychophysiological coherence and reduce stress levels if pilots maintain a regular practice of QCT. Self-regulation of practicing QCT biofeedback was found to be significantly associated with higher coherence and lower perceived stress level for commercial pilots following 2 months practice which can strengthen training effects. In summary, a short session of practicing QCT for five minutes during controlled rest breaks in the flight deck can significantly increase pilots’ psychophysiological coherence by improving cognitive function and stress resilience. Furthermore, regular practice of QCT has long-standing benefits in boosting pilot’s resilience and stress management capacity during flight operations or off-duty. QCT biofeedback can be an effective intervention for aviation authorities and airline operators to develop peer support programs for pilots to increase resilience and maintain mental and physical health.
Acknowledgement
Authors would like to express special thanks to Captain Ben Whitworth and all pilots who are voluntarily participating this research and for their substantial contributions to this research. Their support and the enthusiasm on providing their knowledge and experiences were invaluable in facilitating the authors’ research efforts.
Disclosure statement
The authors declared that they have no commercial or associative interest that represents a conflict of interest in connection with the work submitted to Ergonomics.
Additional information
Funding
References
- Alaminos-Torres, A., M. Martinez-Lorca, I. Sifre De Sola, N. López-Ejeda, and M. Dolores Marrodán. 2022. “Psychological Distress in Spanish Airline Pilots During the Aviation Crisis Caused by the COVID-19 Pandemic and Psychometric Analysis of the 12-Item General Health Questionnaire.” Ergonomics 65 (5): 741–752. doi:10.1080/00140139.2021.1984587.
- Ardell, D. B. 1983. “A Wellness Model for National Health Insurance.” Journal of Health and Human Resources Administration 5 (3): 321–333. https://www.jstor.org/stable/25780120.
- Aristizabal, J. P., R. Navegantes, E. Melo, and A. Pereira. 2020. “Use of Heart Rate Variability Biofeedback to Reduce the Psychological Burden of Frontline Healthcare Professionals Against COVID-19.” Frontiers in Psychology 11: 572191–572194. doi:10.3389/fpsyg.2020.572191.
- Bastianon, C. D., E. M. Klein, A. N. Tibubos, E. Brähler, M. E. Beutel, and K. Petrowski. 2020. “Perceived Stress Scale (PSS-10) Psychometric Properties in Migrants and Native Germans.” BMC Psychiatry 20 (1): 1–9. doi:10.1186/s12888-020-02851-2.
- Bedell, W., and M. Kaszkin-Bettag. 2010. “Coherence and Health Care Cost–RCA Actuarial Study: A Cost-Effectiveness Cohort Study.” Alternative Therapies in Health and Medicine 16 (4): 26–31. https://www.heartmathbenelux.com/doc/blog/24_Coherence%20and%20Health%20Care%20Cost_RCA%20Actuarial%20Study%20A%20Cost%20Effectiveness%20….pdf
- Bor, R., G. Field, and P. Scragg. 2002. “The Mental Health of Pilots: An Overview.” Counselling Psychology Quarterly 15 (3): 239–256. doi:10.1080/09515070210143471.
- Bradley, R. T., R. McCraty, M. Atkinson, D. Tomasino, A. Daugherty, and L. Arguelles. 2010. “Emotion Self-Regulation, Psychophysiological Coherence, and Test Anxiety: Results from an Experiment Using Electrophysiological Measures.” Applied Psychophysiology and Biofeedback 35 (4): 261–283. doi:10.1007/s10484-010-9134-x.
- CAA. 2020. The Effect on Aviation Mental Health From the Covid-19 Pandemic and Return to Re-defined ‘Normal’ Flight Operations (Safety Notice No. SN–2020/014). London, UK: Civil Aviation Authority. https://publicapps.caa.co.uk/docs/33/SN%20-%20The%20Effect%20on%20Mental%20Health%20From%20Return%20To%20Work%20Due%20to%20Covid%2019.pdf
- Cahill, J., P. Cullen, S. Anwer, S. Wilson, and K. Gaynor. 2021. “Pilot Work Related Stress (WRS), Effects on Wellbeing and Mental Health, and Coping Methods.” The International Journal of Aerospace Psychology 31 (2): 87–109. doi:10.1080/24721840.2020.1858714.
- Caldwell, J. A. 2005. “Fatigue in Aviation.” Travel Medicine and Infectious Disease 3 (2): 85–96. doi:10.1016/j.tmaid.2004.07.008.
- Carroll, M, and B. Winslow. 2017. “Examination of the Impact of Condensed Biofeedback Training on Acute Stress Responses.” Journal of Behavioral and Brain Science 07 (07): 287–303. doi:10.4236/jbbs.2017.77021.
- Cohen, S., T. Kamarck, and R. Mermelstein. 1983. “A Global Measure of Perceived Stress.” Journal of Health and Social Behavior 24 (4): 385–396. doi:10.2307/2136404.
- Cooper, C. L, and S. Sloan. 1985. “Occupational and Psychosocial Stress among Commercial Aviation Pilots.” Journal of Occupational Medicine: Official Publication of the Industrial Medical Association 27 (8): 570–576. doi:https://www.jstor.org/stable/45006150.
- Cullen, P., J. Cahill, and K. Gaynor. 2021. “A Qualitative Study Exploring Well-Being and the Potential Impact of Work-Related Stress Among Commercial Airline Pilots.” Aviation Psychology and Applied Human Factors 11 (1): 1–12. doi:10.1027/2192-0923/a000199.
- Demerouti, E., W. Veldhuis, C. Coombes, and R. Hunter. 2019. “Burnout Among Pilots: psychosocial Factors Related to Happiness and Performance at Simulator Training.” Ergonomics 62 (2): 233–245. doi:10.1080/00140139.2018.1464667.
- Derossis, A. M., J. Bothwell, H. H. Sigman, and G. M. Fried. 1998. “The Effect of Practice on Performance in a Laparoscopic Simulator.” Surgical Endoscopy 12 (9): 1117–1120. doi:10.1007/s004649900796.
- Dolan, R. J., and P. Dayan. 2013. “Goals and Habits in the Brain.” Neuron 80 (2): 312–325. doi:10.1016/j.neuron.2013.09.007.
- EASA. 2016. Aircrew Medical Fitness: Implementation of the Recommendations Made by the EASA-Led Germanwings Task Force on the Accident of the Germanwings Flight 9525 (Changes to Regulation (EU) No 965/2012). Opinion No.14/2016. Cologne, Germany: European Union Aviation Safety Agency. https://www.easa.europa.eu/downloads/21686/en.
- EASA 2018. Commission Regulation (EU) 2018/1042. Cologne, Germany: European Union Aviation Safety Agency. https://eur-lex.europa.eu/legal-content/EN/TXT/HTML/?uri=CELEX%3A32018R1042&from=EN
- EASA 2021. COVID-19 SR Portfolio Safety Issue Report – Skills and Knowledge Degradation Due to Lack of Recent Practice (SI-5003). Cologne, Germany: European Union Aviation Safety Agency. https://www.easa.europa.eu/community/system/files/2021-08/Safety%20Issue%20Report%20-%20%20Skills%20and%20Knowledge%20Degradation_REV2%20Clean_0.pdf
- Edwards, S. D., D. J. Edwards, and R. Honeycutt. 2022. “HeartMath as an Integrative, Personal, Social, and Global Healthcare System.” Healthcare 10 (2): 376–310. doi:10.3390/healthcare10020376.
- Ehsan, H. B., S. Vahedi, M. Amjadian, R. Rostami, and K. Saboni. 2019. “Comparison of the Effects of Islamic Spiritual Educations and Breathing Techniques with Heart Rate Variability Feedback Therapies on Heart Rate Variability, Psychophysiological Coordination and Stress in Patients Undergoing Coronary Artery Bypass Graft Surgery.” Shiraz E Medical Journal 20 (8): 1–6. doi:10.5812/semj.83485.
- Ericsson, K. A. 1997. “Deliberate Practice and the Acquisition of Expert Performance: An Overview.” In Does Practice Make Perfect?, edited by H. Jorgensen and A. C. Lehmann, 9–51. Stockholm: NIH Publikasjoner.
- Erikssen, G., K. Liestøl, J. Bjørnholt, E. Thaulow, L. Sandvik, and J. Erikssen. 1998. “Changes in Physical Fitness and Changes in Mortality.” The Lancet 352 (9130): 759–762. doi:10.1016/S0140-6736(98)02268-5.
- FAA 2021. Guide for Aviation Medical Examiners: Decision Considerations - Aerospace Medical Dispositions. Washington, DC: Federal Aviation Administration (FAA). https://www.faa.gov/about/office_org/headquarters_offices/avs/offices/aam/ame/guide/app_process/exam_tech/item48/amd/gd/
- FAA 2016. Pilot’s Handbook of Aeronautical Knowledge. Chapter 17: Aeromedical Factors. Washington, DC: Federal Aviation Administration (FAA). https://www.faa.gov/regulations_policies/handbooks_manuals/aviation/phak/media/19_phak_ch17.pdf
- Field, L., S. Edwards, D. Edwards, and S. E. Dean. 2018. “Influence of HeartMath Training Programme on Physiological and Psychological Variables.” Global Journal of Health Science 10 (2): 126–133. doi:10.5539/gjhs.v10n2p126.
- Fisk, A. D, and W. Schneider. 1983. “Category and Word Search: Generalizing Search Principles to Complex Processing.” Journal of Experimental Psychology. Learning, Memory, and Cognition 9 (2): 177–195. doi:10.1037/0278-7393.9.2.177.
- Flight Safety Foundation 2020. An Aviation Professional’s Guide to Wellbeing. Alexandria, VA: Flight Safety Foundation.
- Galla, B. M, and A. L. Duckworth. 2015. “More Than Resisting Temptation: Beneficial Habits Mediate the Relationship Between Self-Control and Positive Life Outcomes.” Journal of Personality and Social Psychology 109 (3): 508–525. doi:10.1037/pspp0000026.
- Gardner, B., G.-J. de Bruijn, and P. Lally. 2011. “A Systematic Review and Meta-Analysis of Applications of the Self-Report Habit Index to Nutrition and Physical Activity Behaviors.” Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine 42 (2): 174–187. doi:10.1007/s12160-011-9282-0.
- Gardner, B, and A. L. Rebar. 2019. “Habit Formation and Behavior Change." Oxford Research Encyclopedia of Psychology 1–26. doi:10.1093/acrefore/9780190236557.013.129
- Haith, A. M, and J. W. Krakauer. 2018. “The Multiple Effects of Practice: Skill, Habit and Reduced Cognitive Load.” Current Opinion in Behavioral Sciences 20: 196–201. doi:10.1016/j.cobeha.2018.01.015.
- HeartMath. 2014. “Inner Banlance User Manual.” https://cdn.heartmath.com/manuals/InnerBalanceManual_v3_1_for_iOS6.pdf
- HeartMath. 2022. “The Science of HeartMath.” https://www.heartmath.com/science/
- IATA. 2020. Guidance for Flight Operations During and Post Pandemic. Montreal, Canada: International Air Transport Association (IATA). https://www.icao.int/MID/Documents/RPTF/iata-guidance-flight-operations-during-post-pandemic.pdf
- IATA. 2021. World Air Transport Statistics 2021. Montreal, Canada: International Air Transport Association (IATA). https://www.iata.org/en/publications/store/world-air-transport-statistics/
- ICAO. 2022. Effects of Novel Coronavirus (COVID-19) on Civil Aviation: Economic Impact Analysis. Montréal, Canada: International Civil Aviation Organization (ICAO). https://www.icao.int/sustainability/Documents/COVID-19/ICAO_Coronavirus_Econ_Impact.pdf
- ICAO. 2016. Aviation Medicine, Psychiatric and Psychological Aspects (A39-WP/106). Montréal, Canada: Technical Commission, International Civil Aviation Organization (ICAO). https://www.icao.int/Meetings/a39/Documents/WP/wp_106_en.pdf
- IFALPA. 2020. Safely Navigating the Industry Recovery Bulletin 5: Occupational Health and Safety in the Context of COVID. Montreal, Canada: The International Federation of Air Line Pilots’ Associations. https://ifalpa.org/media/3625/21sab06-occupational-health-and-safety-in-the-context-of-covid-jp.pdf
- Ireland, R. R. 2010. “Is Electrophysiological Coherence-Based Wellness Coherent?” Alternative Therapies in Health and Medicine 16 (4): 68–69.
- Joshi, L. N., V. D. Joshi, and L. V. Gokhale. 1992. “Effect of Short Term “Pranayam” Practice on Breathing Rate and Ventilatory Functions of Lung.” Indian Journal of Physiology and Pharmacology 36 (2): 105–108.
- Kingston, J., P. Chadwick, D. Meron, and T. C. Skinner. 2007. “A Pilot Randomized Control Trial Investigating the Effect of Mindfulness Practice on Pain Tolerance, Psychological Well-Being, and Physiological Activity.” Journal of Psychosomatic Research 62 (3): 297–300. doi:10.1016/j.jpsychores.2006.10.007.
- Kloudova, G., S. Kozlova, and M. Stehlik. 2019. “The Use of Biofeedback to Increase Resilience and Mental Health of Supersonic Pilots.” International Journal of Science and Engineering Investigations 8 (91): 85–93. http://www.ijsei.com/papers/ijsei-89119-11.pdf.
- Kruskal, J. B., T. Shanafelt, P. Eby, C. C. Meltzer, J. Rawson, L. N. Essex, C. Canon, D. West, and C. Bender. 2019. “A Road Map to Foster Wellness and Engagement in Our Workplace—a Report of the 2018 Summer Intersociety Meeting.” Journal of the American College of Radiology : JACR 16 (6): 869–877. doi:10.1016/j.jacr.2018.10.025.
- Lee, E. H. 2012. “Review of the Psychometric Evidence of the Perceived Stress Scale.” Asian Nursing Research 6 (4): 121–127. doi:10.1016/j.anr.2012.08.004.
- Li, W-C., J. Zhang, and P. Kearney. 2022. “Psychophysiological Coherence Training to Moderate Air Traffic Controllers’ Fatigue on Rotating Roster.” Risk Analysis 2022: 1–14. doi:10.1111/risa.13899.
- Ma, X., Z. Q. Yue, Z. Q. Gong, H. Zhang, N. Y. Duan, Y. T. Shi, G. X. Wei, and Y. F. Li. 2017. “The Effect of Diaphragmatic Breathing on Attention, Negative Affect and Stress in Healthy Adults.” Frontiers in Psychology 8: 874–812. doi:10.3389/fpsyg.2017.00874.
- Marin, M. F., C. Lord, J. Andrews, R. P. Juster, S. Sindi, G. Arsenault-Lapierre, A. J. Fiocco, and S. J. Lupien. 2011. “Chronic Stress, Cognitive Functioning and Mental Health.” Neurobiology of Learning and Memory 96 (4): 583–595. doi:10.1016/j.nlm.2011.02.016.
- McCraty, R. 2011. “Coherence: Bridging Personal, Social and Global Health.” Activitas Nervosa Superior Rediviva 53 (3): 85–102.
- McCraty, R., and D. Tomasino. 2006. “Emotional Stress, Positive Emotions, and Psychophysiological Coherence.” In Stress in Health and Disease, edited by B. B. Arnetz and R. Ekman, 342–365. Weinheim: Wiley-VCH. doi:10.1002/3527609156.ch21.
- Miani, P., T. Kille, S. Y. Lee, Y. Zhang, and P. R. Bates. 2021. “The Impact of the COVID-19 Pandemic on Current Tertiary Aviation Education and Future Careers: Students’ Perspective.” Journal of Air Transport Management 94: 102081–102088. doi:10.1016/j.jairtraman.2021.102081.
- Mourya, M., A. S. Mahajan, N. P. Singh, and A. K. Jain. 2009. “Effect of Slow-and Fast-Breathing Exercises on Autonomic Functions in Patients With Essential Hypertension.” Journal of Alternative and Complementary Medicine (New York, N.Y.) 15 (7): 711–717.
- Nilsen, P., K. Roback, A. Broström, and P. E. Ellström. 2012. “Creatures of Habit: Accounting for the Role of Habit in Implementation Research on Clinical Behaviour Change.” Implementation Science: IS 7 (1): 53–56. doi:10.1186/1748-5908-7-53.
- Olaganathan, R., and R. A. H. Amihan. 2021. “Impact of Covid-19 on Pilot Proficiency–a Risk Analysis.” Global Journal of Engineering and Technology Advances 6 (03): 1–13. doi:10.30574/gjeta.2021.6.3.0023.
- Oró, P., M. Esquerda, B. Mas, J. Viñas, O. Yuguero, and J. Pifarré. 2021. “Effectiveness of a Mindfulness-Based Programme on Perceived Stress, Psychopathological Symptomatology and Burnout in Medical Students.” Mindfulness 12 (5): 1138–1147. doi:10.1007/s12671-020-01582-5.
- Rebar, A. L., J. A. Dimmock, B. Jackson, R. E. Rhodes, A. Kates, J. Starling, and C. Vandelanotte. 2016. “A Systematic Review of the Effects of Non-Conscious Regulatory Processes in Physical Activity.” Health Psychology Review 10 (4): 395–407. doi:http://doi.org/10.1080/17437199.2016.1183505.
- Reyes, F. J. 2014. “Implementing Heart Rate Variability Biofeedback Groups for Veterans with Posttraumatic Stress Disorder.” Biofeedback 42 (4): 137–142. doi:10.5298/1081-5937-42.4.02.
- Robertson, I. T., C. L. Cooper, M. Sarkar, and T. Curran. 2015. “Resilience Training in the Workplace from 2003 to 2014: A Systematic Review.” Journal of Occupational and Organizational Psychology 88 (3): 533–562. doi:10.1111/joop.12120.
- Roeser, R. W., E. Skinner, J. Beers, and P. A. Jennings. 2012. “Mindfulness Training and Teachers’ Professional Development: An Emerging Area of Research and Practice.” Child Development Perspectives 6 (2): 167–173. doi:10.1111/j.1750-8606.2012.00238.x.
- Rutter, M. 2007. “Resilience, Competence, and Coping.” Child Abuse & Neglect 31 (3): 205–209. doi:10.1016/j.chiabu.2007.02.001.
- Shappell, S., C. Detwiler, K. Holcomb, C. Hackworth, A. Boquet, and D. A. Wiegmann. 2007. “Human Error and Commercial Aviation Accidents: An Analysis Using the Human Factors Analysis and Classification System.” Human Factors 49 (2): 227–242.
- Singer, R. N. 2000. “Performance and Human Factors: Considerations About Cognition and Attention for Self-Paced and Externally-Paced Events.” Ergonomics 43 (10): 1661–1680. doi:10.1080/001401300750004078.
- Slimani, M., N. L. Bragazzi, D. Tod, A. Dellal, O. Hue, F. Cheour, L. Taylor, and K. Chamari. 2016. “Do Cognitive Training Strategies Improve Motor and Positive Psychological Skills Development in Soccer Players? Insights from a Systematic Review.” Journal of Sports Sciences 34 (24): 2338–2349. doi:10.1080/02640414.2016.1254809.
- Spruit, E. N., G. P. H. Band, and J. F. Hamming. 2015. “Increasing Efficiency of Surgical Training: effects of Spacing Practice on Skill Acquisition and Retention in Laparoscopy Training.” Surgical Endoscopy 29 (8): 2235–2243. doi:10.1007/s00464-014-3931-x.
- Szulczewski, M. T. 2019. “Training of Paced Breathing at 0.1 Hz Improves CO2 Homeostasis and Relaxation During a Paced Breathing Task.” Plos ONE 14 (6): e0218550. doi:10.1371/journal.pone.0218550.
- Thomas, P. R, and G. J. Fogarty. 1997. “Psychological Skills Training in Golf: The Role of Individual Differences in Cognitive Preferences.” The Sport Psychologist 11 (1): 86–106. doi:10.1123/tsp.11.1.86.
- Vuorio, A, and R. Bor. 2020. “Black Swan Pandemic and the Risk of Pilot Suicide.” Frontiers in Public Health 8: 573006–573003. doi:10.3389/fpubh.2020.573006.
- Vuorio, A., T. Laukkala, P. Navathe, B. Budowle, A. Eyre, and A. Sajantila. 2014. “Aircraft-Assisted Pilot Suicides: Lessons to Be Learned.” Aviation, Space, and Environmental Medicine 85 (8): 841–846. doi:10.3357/ASEM.4000.2014.
- Winne, P. H, and D. Jamieson-Noel. 2002. “Exploring Students’ Calibration of Self Reports about Study Tactics and Achievement.” Contemporary Educational Psychology 27 (4): 551–572. doi:10.1016/S0361-476X(02)00006-1.
- Wu, A. C., D. Donnelly-McLay, M. G. Weisskopf, E. McNeely, T. S. Betancourt, and J. G. Allen. 2016. “Airplane Pilot Mental Health and Suicidal Thoughts: A Cross-Sectional Descriptive Study via Anonymous Web-Based Survey.” Environmental Health 15 (1): 1–12. doi:10.1186/s12940-016-0200-6.
- Yip, P. S., Y. T. Cheung, P. H. Chau, and Y. W. Law. 2010. “The Impact of Epidemic Outbreak.” Crisis 31 (2): 86–92. doi:10.1027/0227-5910/a000015.
- Zimmerman, B. J., and A. Kitsantas. 1997. “Developmental Phases in Self-Regulation: Shifting from Process Goals to Outcome Goals.” Journal of Educational Psychology 89 (1): 29–36. doi:10.1037/0022-0663.89.1.29.
