
Abstract
Firefighters wear personal protective equipment to protect them from the thermal and chemical environment in which they operate. The self-contained breathing apparatus (SCBA) provides isolation of the airway from the hazardous fireground. National standards limit SCBA weight, however, integration of additional features could result in an SCBA exceeding the current limit. The purpose of this study was to examine the effects of increased SCBA weight on firefighters’ physiological responses, work output, dynamic stability, and comfort. Completion of simulated firefighting activities induced a strong physiological response. Peak oxygen consumption was higher with the lightest SCBA than the heaviest SCBA. Few other physiological differences were noted as SCBA weight increased. Importantly, increased SCBA weight resulted in significantly more negative perceptions by the firefighters and a trend towards significance for the duration of work time prior to reaching volitional fatigue. These results should be considered when assessing changes to existing SCBA weight limits.
PRACTITIONER SUMMARY
Increased SCBA weight above existing national standards resulted in negative perceptions by the firefighters, but not significant physiological changes after two simulated bouts of firefighting activity. SCBA weight had a nearly significant impact on the time firefighters worked before reaching volitional fatigue, with heavier SCBA trending towards decreased working time.
Introduction
Firefighting operations require firefighters to perform high levels of physically demanding work in hazardous environments. On average, 70 firefighters have been killed in the line of duty each year between 1977 and 2021 (Fahy and Petrillo Citation2022). This number does not include the 343 firefighters killed on September 11, 2001, nor does it include those who have passed away from cancer resulting from occupational exposure. Cardiovascular events have consistently been the leading cause of line-of-duty deaths in the fire service, resulting in approximately 43% of deaths, while burn injuries resulted in less than 4% of deaths. The leading cause of injuries on the fireground in 2021 was overexertion and strain (25%) followed closely by fall, jump, slip, and trip injuries (24%) (Campbell and Hall Citation2022).
Firefighters wear personal protective equipment (PPE) to protect themselves from the elevated ambient temperatures and by-products of combustion found on the fireground. The self-contained breathing apparatus (SCBA) is a critical component of firefighting PPE that provides air to the wearer, effectively isolating the firefighter from inhaling hazardous substances. The SCBA consists of a harness with straps worn over the shoulder and around the waist. A frame (typically metal or plastic) is supported by shoulder straps and holds a compressed air cylinder. A series of hoses and regulators run alongside the frame and through the shoulder straps to the wearer’s facepiece, reducing the supplied air from 5500 psi to less than 0.1 psi (other common air cylinder pressures include 4500 psi and 2216 psi). As advances in SCBA technology have occurred, several key safety features have become integrated into the SCBA and are required by national standards in the United States (National Fire Protection Association Citation2019). Specific examples of these features include an End of Service Time Indicator (EOSTI) that alarms when the remaining air in the cylinder reaches one-third of the original capacity (older editions of the standard employed a one-quarter EOSTI) and the Personal Alert Safety System (PASS), which alarms when the user is inactive for 30 seconds, indicating the need for assistance and providing an audible indicator of an inactive firefighter’s location. The Universal Emergency Breathing Safety System provides connections to allow for the sharing or transfer of air from another cylinder in the event of an emergency. There are numerous other mandatory features and design requirements for the SCBA to comply with national standards. Other safety features are available but not required (e.g. thermal imaging cameras, bail-out ropes and anchors, communication devices, tracking systems, and lighting); however, with each additional piece of technology or safety equipment, the weight of the SCBA is increased. Furthermore, the addition of high-power electronics in some safety devices drives the need for larger capacity power storage systems within the SCBA, which can further add to the total weight of the SCBA. The current SCBA weight limit within the 2019 edition of NFPA 1981: Standard on Open-Circuit Self-Contained Breathing Apparatus (SCBA) for Emergency Services is set by 42 CFR Part 84.89 (a) which states: ‘The completely assembled and fully charged apparatus shall not weigh more than 16 kg (35 pounds)’. As fire departments consider their SCBA needs, they must weigh the pros and cons of options available to help protect their firefighters while also adding additional weight to an already physically demanding occupation.
Numerous studies have quantified the physiological and biomechanical impact of firefighting and firefighting personal protective equipment on the firefighter. Past research has examined the thermal and cardiovascular response to firefighting in settings ranging from treadmill walking to real-world emergency responses (Horn et al. Citation2015; Horn et al. Citation2017) and across a range of work cycles (Horn et al. Citation2013; Hostler et al. Citation2016; Schlader, Colburn, and Hostler Citation2017; Walker et al. Citation2015). In Kesler et al. (Citation2017), firefighters conducted two bouts of simulated firefighting activity with SCBA of various sizes and weights and monitored physiological response and work output. Previous research by Bakri et al. (Citation2012) demonstrated that increasing the SCBA weight from 6.4 kg to 11.0 kg did not affect oxygen consumption.
The weight and position of the firefighter’s SCBA can introduce disturbances in the musculoskeletal system. This disturbance can have an impact on static (Hur et al. Citation2015) and dynamic (Hur et al. Citation2013; Punakallio Citation2004; Punakallio, Louhevaara, and Lusa-Moser Citation1997) balance with several studies examining both (Punakallio Citation2003; Punakallio, Lusa, and Luukkonen Citation2003, Citation2004). Hur et al. (Citation2015) reported that SCBA with larger weight, greater height, and greater magnitude of change in centre of mass had significant impacts on postural stability. Biomechanical modelling programs have been utilised to assess the maximum weight that would allow for the comfortable and safe completion of firefighting tasks and suggest that heavier SCBA result in larger lumbar lift and shoulder forces (Xu et al. Citation2021a, Citation2021b).
The purpose of this study was to further understand the impact of increasing the current weight limit for SCBA on the firefighter’s physiological and biomechanical response to simulated fireground operations. We hypothesised that the addition of 2.3 and 4.5 kg to the current maximum SCBA weight would result in increased physiological response and decreased work output, dynamic stability, and firefighters’ perceptions of comfort. Our work provides novel information related to the impact of increasing the current weight limit for SCBA on firefighters’ physiological and biomechanical responses. It also provides important data about their work output and perceptions of performing firefighting tasks with increased SCBA weight. These data are important to standard setting organisations as they consider increasing the weight limit for SCBA, and are equally important to firefighters, fire departments, equipment manufacturers, as they consider future SCBA purchasing, use, and development. This study builds on previous work that examined a range of SCBA weights below the current limit.
Methods
Study participants
Ten healthy male firefighters (Age: 31.0 ± 6.4 years, Height: 180.0 ± 8.7 cm, Weight: 85.6 ± 13.3 kg, BMI: 26.6 ± 5.2 kg/m2, Fire Fighting Experience: 8.2 ± 7.2 years) with no self-reported cardiovascular, orthopaedic, biomechanical, or digestive tract concerns participated in this study. Subjects completed a physical activity readiness questionnaire (PAR-Q) (Thomas, Reading, and Shephard Citation1992) and core temperature capsule screening prior to testing and all subjects were determined to be eligible for physical activity and core temperature capsule ingestion. All subjects were provided with the opportunity to ask questions and signed a written informed consent prior to participation. Approval for this protocol was obtained from the University of Illinois Institutional Review Board (IRB) under protocol #20927.
Study design
All participants completed four visits: one baseline visit and three simulated firefighting visits. The initial baseline visit consisted of screening, informed consent, measures of height and weight, and a maximal treadmill test. The subsequent three visits involved simulated firefighting activities and assessment of physiological response and biomechanical performance. Visits were completed on separate days at approximately the same time of day with a minimum of 24 hours between each. Previous studies have examined the impact of test environment (Horn et al. Citation2015) and varying sizes of commercially available SCBA (Kesler et al. Citation2018a; Kesler et al. Citation2018b; Kesler et al. Citation2017) utilising similar protocols. This study aimed to examine the impact of SCBA weight greater than current national standards (National Fire Protection Association Citation2019), while controlling the SCBA size and design.
Self-Contained breathing apparatus (SCBA)
A commercially available SCBA was purchased and then modified to exceed the current weight limit by 2.3 kg (5 lbs) and 4.5 kg (10 lbs) (). On average this load represented 2.7 ± 0.4% and 5.4 ± 0.8% of the participants’ total body mass. SCBA1 was used as received from the manufacturer utilising a 5500 psi, 45-minute cylinder, an integrated self-rescue belt, and quick-connect cylinder connection and weighed 16 kg. For SCBA2, five 0.45 kg (1 lb) sandbags were added at different locations: three along the lower portions of the frame and one on each arm strap over the shoulder (), increasing the total weight by 2.3 kg (5 lbs). For SCBA3, two sandbags (combined weight 0.9 kg (2 lbs)) were added at each location, increasing the total weight by 4.5 kg (10 lbs). These positions were selected as they represent locations where thermal imaging cameras, communication devices, tracking systems or other additional features or devices might typically be integrated into the SCBA, increasing the weight of the breathing apparatus.
Figure 1. SCBA utilised in study. Arrows indicate where additional weight was added for SCBA2 and SCBA3. One sandbag (0.45 kg each, 2.3 kg total) was added at each location for SCBA2 and two sandbags (0.9 kg, 4.5 kg total) were added at each location for SCBA3.
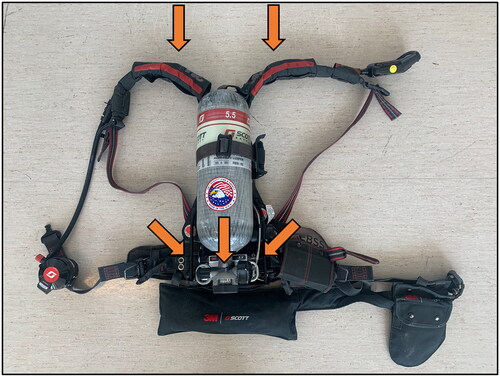
Table 1. SCBA utilised in the study included the maximum allowable weight under NFPA 1981 (16 kg), the maximal weight plus 2.3 kg (18.3 kg), and the maximal weight plus 4.5 kg (20.5 kg).
Baseline visit
Following the screening and informed consent process, eligible participants completed a health history and physical activity inventory. Research staff demonstrated the functional balance test and firefighting activities, which would be utilised in subsequent visits. Following the demonstrations, height and weight were collected. Throughout the baseline visit, participants wore typical exercise clothing (t-shirt, shorts, and running shoes).
Next, the participant was fit with a heart rate strap (Polar Electro Oy, Kempele, Finland) and portable metabolic monitoring system (K4b2, Cosmed s.r.l., Rome, Italy) and began the graded treadmill exercise test as described in NFPA 1582 (National Fire Protection Association Citation2022). The treadmill test started with two minutes of seated rest followed by three minutes of walking at 3 mph at 0% incline. After three minutes speed was increased to 4.5 mph. Alternating increases of incline (2%) and speed (0.5 mph) then occurred every one minute until volitional fatigue was reached. At each minute, the participant was asked to provide their rating of perceived exertion (RPE, (Borg Citation1970)). Baseline visits were completed at least 24 hours prior to any of the simulated firefighting visits.
Firefighting visits
Three firefighting visits were conducted utilising the various SCBA described previously (). Participants utilised only one of the prescribed SCBA conditions throughout a visit and the three SCBA conditions were presented in a counter-balanced order. That is, trial order was intentionally arranged so that on the first visit some participants utilised SCBA1, some utilised SCBA2, and some utilised SCBA3. The weights were adjusted for the second and third visits so that each firefighter utilised each weight of SCBA. This was done to minimise any learning or conditioning effects and was verified, with no statistically significant differences found as a result of trial order. Six to 12 hours prior to each visit, the participant ingested a core temperature monitoring capsule (VitalSense, Phillips Respironics, Andover, MD). Participants were coached on the importance of proper capsule ingestion timing with the goal of the capsule moving out of the stomach into the intestines but remaining in the body. On the day of each visit, the participant reported to the Illinois Fire Service Institute Research Lab for the firefighting activity visits ().
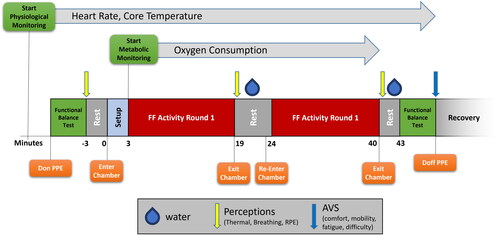
Figure 2. Schematic of firefighting test session. Heart rate and core temperature were recorded throughout the visit. Oxygen consumption was recorded throughout the firefighting activities. The Functional Balance Test was conducted pre- and post-firefighting activity. Perceptions of Thermal Sensation, Breathing Scale, and Rating of Perceived Exertion (RPE) were collected pre-, mid-, and post-firefighting activity. Visual Analog Scales (VAS) of comfort, mobility, fatigue, and subjective difficulty were collected at the end of the trial.
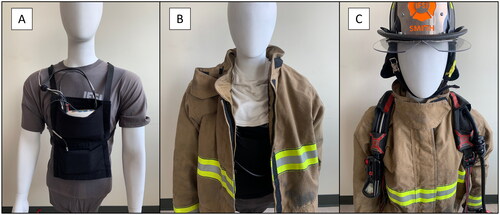
Prior to the trial initiation, research staff verified the presence of the core temperature capsule and ensured that the capsule was actively transmitting data, and the participant was fit with a physiological status monitor (EquiVital, Phillips Respironics, Andover, MD), which received data from the core temperature capsule and recorded heart rate data. The participant was also instrumented with a dedicated heart rate strap (Polar Electro Oy, Kempele, Finland) linked to the metabolic monitor. Next, the participant donned a custom harness designed to hold the portable metabolic monitor on the chest of the participant to avoid interference with the SCBA worn on the back (). The participant then donned standard firefighting personal protective equipment including a coat, pants, boots, Nomex hood (initially worn around the neck), helmet, and the prescribed SCBA ( and ). Participants were all provided the same style of PPE in their correct size. The full ensemble, without SCBA, weighed 9.4 kg. The composites in the coat and pant had a Total Heat Loss of 270.6 W/m2 and a Thermal Protective Performance rating of 36.3, as provided by the manufacturer.
Figure 3. Participants wore a custom harness to support the metabolic monitoring system under the turnout gear (A). The participant also wore standard firefighting personal protective equipment including a coat, pants, boots, nomex hood, helmet and SCBA (B and C).
After donning firefighting PPE, the participant completed the FBT, (described in detail later), followed by three minutes of seated rest. During this rest period the participant provided their baseline self-reported perceptions of Thermal Sensation (Young Citation1987), Breathing Scale (Morgan and Raven Citation1985), and their Rating of Perceived Exertion (RPE, (Borg Citation1970)). After the rest period, the participant entered the environmental chamber (47 °C, ∼30% relative humidity), guided by a member of the research team, and resumed seated rest throughout a three-minute setup period. During this time, the metabolic monitor was inserted into the front harness, the participant donned the silicone mask, pulled up the firefighting hood, and donned the helmet (). Metabolic data collection began three minutes after entering the environmental chamber.
Figure 4. Participants wore the silicone K4b2 metabolic monitor mask under the hood and helmet during firefighting activities.

At the conclusion of the first round of firefighting activities the participant was escorted out of the environmental chamber and allowed to rest while seated. This rest period represented the time it would take for the firefighter to have their air cylinder replaced between bouts of activity during a real-world response. The participant then removed their helmet, lowered their hood around their neck, removed the silicone mask, and was provided with water ad libitum. Self-reported perceptions (RPE, Breathing Scale, Thermal Sensation Scale) were collected. After four minutes and 15 seconds the participant re-entered the environmental chamber and returned to the seated rest position. In the remaining 45 seconds of the 5-minute rest period the participant donned the silicone mask, hood, and helmet. The participant then completed the second bout of firefighting activities. At the completion of activities (or volitional fatigue, whichever came first) the participant was escorted out of the chamber and metabolic data collection was terminated. The helmet was removed, the hood was lowered around the neck, the silicone mask was removed, and the participant was provided with water ad libitum. Post-test self-reported perceptions (RPE, Breathing Scale, Thermal Sensation Scale) were again collected. After three minutes of seated rest the participant completed the FBT followed by completing the Visual Analog Scale (VAS) for overall body comfort, overall body mobility, fatigue, and subjective difficulty in carrying out the activity with SCBA. Lastly, PPE was removed, physiological data collection was ended, and after a recovery period the participant was released.
Functional balance test (FBT)
Prior to, and following the completion of the firefighting activities, the participant completed the FBT (Punakallio, Louhevaara, and Lusa-Moser Citation1997). The FBT consists of two elevated platforms (122 cm by 122 cm × 15 cm high) with painted spaces (60 cm by 60 cm) connected by a narrow beam (14 cm wide by 244 cm long × 4 cm high). On a ‘GO’ cue, the participant stepped from one platform down onto the beam, moved across it to the other platform, turned around within the painted square, returned across the beam, and stopped in the original painted square. Following the initial trial, a crossbar was added at 75% of the participant’s height as an obstacle. The participant then repeated the trial while manoeuvring under the crossbar. Participants were instructed to complete the FBT as quickly as possible while avoiding errors, using a pace similar to that they would use on the fireground. Errors were scored as stepping off from the platform or beam, not turning or stopping within the defined square, or contacting the crossbar. Time to complete each trial was recorded on two hand-held stopwatches (Z-100, TYR Sport Inc, Seal Beach, CA) and averaged. To assess both completion time and error counts in a single metric, a Performance Index (PI) is utilised as in Hur et al. (Citation2013).
Firefighting activities
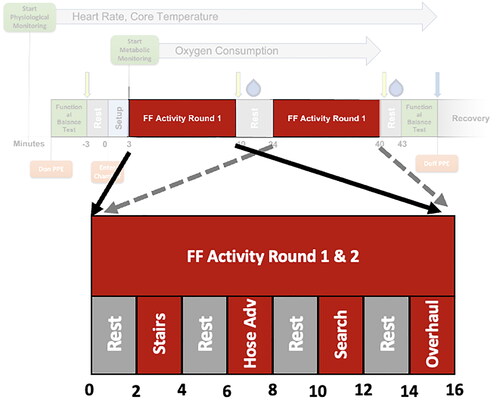
Participants completed simulated firefighting activities representative of tasks typically completed by firefighters during fire suppression operations. The simulated firefighting activities are described in detail by Horn et al. (Citation2015). Participants were encouraged to work at a pace representative of their effort on the fireground during real-world responses. Simulated activities started with two minutes of seated rest on a stool located in the environmental chamber (47 °C, ∼30% humidity). The participant then completed alternating sessions of four activities and rests (), which are representative of the intermittent work cycles on the fireground. Specifically, activities consisted of 1) a 3-step stair climb (18 cm rise, 28 cm run), 2) a hose advance where a rigid section of hose was fixed to cable running from a low pulley to a sliding carriage on a track with a constant force spring with 10 kg resistance, 3) a search in which the participant moved around the perimeter of the room in a controlled ‘secondary search’ pattern, and 4) an overhaul task where a pike pole was fixed to a cable running to a high pulley to the same constant force spring. For the stair climb activity, a single repetition was counted as traversing to the top step, touching both feet to the top, then traversing back down to the ground. For activity 2 and 4 a repetition was counted as moving the hose or the pike pole to touch a target and returning the tool to the starting position. For activity 3, a single repetition was counted as one lap around the room covering a total distance of 12.2 m.
Figure 5. Schematic of firefighting activity timeline. Activities were completed on a 2-minute work/rest cycle.
Measured variables and calculations
A number of measures were collected during the Baseline and Firefighting activity visits. During the baseline visit a health history survey was collected. During the treadmill test, O2 consumption, heart rate, and RPE were collected. O2 consumption was averaged over 15 second epochs and the highest rate (VO2,max) was recorded. The highest heart rate (HRmax) and RPE at volitional fatigue (RPEmax) were also recorded. During the firefighting visits heart rate and core temperature were collected throughout each trial. For core temperature, measures of baseline (initial) and peak (highest during activity) were recorded. Change in core temperature (ΔTco,peak) was computed as the difference between baseline and peak. Core temperature rate of rise (Tco,RoR) was computed as the change in core temperature divided by the duration between the start of the test and the time when peak core temperature was reached. This variable was only computed for six of the ten participants. In a single trial for four different participants, core temperature data loss occurred when the temperature reading was affected by ingested water between bouts of activity. To examine the effect of SCBA on core temperature before the data loss occurred, Tco,RoR during the first round (Tco,RoR, R1) was computed on all 10 participants.
O2 consumption was recorded while the participant was in the environmental chamber and was averaged over 15 second epochs and VO2,Peak reported. O2 consumption rate was also reported as a percentage of the maximal O2 consumption rate from the baseline test (VO2,Peak(%max)). Repetitions of each activity (Reps) were recorded during each of the work periods shown in , as the number of movements completed within the two-minutes for each activity. The time between when the participant entered the chamber until the participant completed the prescribed 40 minutes of activity or reached volitional fatigue was also recorded and is reported as Work Time. Participants who exited the environmental chamber without completing all the firefighting activities received a Reps score of ‘zero’ for the activities that were not attempted. Regardless of whether the participant finished all assigned activities or exited the chamber after reaching volitional fatigue, the participant moved to the next phase of the study and data collection continued.
Time to completion and errors were recorded during the FBT pre- and post-firefighting activity, then summed to create a performance index (Hur et al. Citation2013). Two members of the research team independently recorded time and errors and results were averaged. Errors were scaled according to their severity. Minor errors (scaled at 5 seconds per minor error) included the foot or hand touching the ground, the hand touching the platform, not turning around within the space, not stopping within the space, or contacting the crossbar (on trials where it was present). Major errors (scaled at 10 seconds per major error) included knocking the crossbar down during applicable trials where the crossbar was present.
Three self-reported perceptions were collected throughout the firefighting visits. Rating of perceived exertion (RPE, ranging from 6-’No Exertion’ to 20-‘Maximal Exertion’), Breathing Scale (ranging from 1-’My breathing is OK’ to 7-’I can’t breathe’), and Thermal Sensation Scale (ranging from 0-’Unbearably Cold’ to 8-’Unberably Hot’) were collected pre-, mid-, and post-firefighting activity. A visual analog scale ranging from −8 to +8 was utilised post-firefighting activity to assess overall body comfort (Uncomfortable to Comfortable), overall body mobility (Least Mobility to Highest Mobility), fatigue (perceived physical exertion, Unbearably Fatigued to Not Fatigued), and subjective difficulty in carrying out the activity with the prescribed SCBA (Restricted to Not Restricted).
Statistical analysis
All data and statistical analyses were based on the maximum number of participants with reliable data. For most variables this included all 10 participants. Tco,RoR, analysis included the six participants whose core temperature data was not impacted by water ingestion throughout both bouts of all three firefighting visits. Analysis of the visual analog scales (Comfort, Mobility, Fatigue, Difficulty) was based on nine participants as one did not complete the scale for a single visit.
Each parameter was analysed using a repeated measures ANOVA (SPSS Statistics 28 IBM; Armonk, New York) with significance set at α = 0.05. Specifically, three SCBA conditions were examined (SCBA1, SCBA2, and SCBA3). For certain variables, a second main effect was tested and a 3 × 2 repeated measures ANOVA was conducted. In these cases both main effects and their interactions were tested. For measures of HRPeak, HRPeak(%Max), and simulated firefighting repetitions, the effect of Bout (First and Second) was examined. For Perceptions (RPE, Breathing Scale, Thermal Sensation Scale), the effect of testing time (PrePost main effect) was examined. Post hoc pairwise analysis was conducted using Tukey HSD Tests.
Results
During the baseline test, 10 firefighters completed a maximal treadmill test. During the maximal test, participants obtained a maximum rate of oxygen consumption (VO2max) of 38.9 ± 5.3 ml/min/kg, a maximum heart rate (HRmax) of 183.2 ± 12.3 bpm, and reached a Rating of Perceived Exertion of 18.6 ± 1.3.
Completion of firefighting activities with different SCBA weights
Participants were instructed to complete the assigned firefighting activities or notify the research staff if they felt light-headed, dizzy, unwell, or when they reached volitional fatigue. All participants participated in the baseline visit and completed three simulated firefighting activity visits, but of the 10 participants only one was able to complete all the assigned firefighting activities during all three simulated firefighting trials. One participant completed all activities during two trials and three completed all activities for one of the trials. The other five participants did not complete all of the activities for any of the trials.
Three participants completed all the simulated firefighting activities with SCBA1, four completed all the activities with SCBA2, and only one completed the activities with SCBA3. For SCBA3, one participant ended the trial before beginning the second bout and one participant ended the trial during the first bout of activity. The other seven ended the trial during the second bout.
There was no main effect of SCBA for the number of repetitions completed in any of the activities for both bouts (). However, during the second bout participants completed significantly less work for all activities across all SCBA weights indicating a significant main effect of Bout (stairs, p = 0.014; hose advance, p = 0.004; search, p = 0.002; overhaul, p < 0.001). There were no significant interaction effects between SCBA and Bout.
Table 2. Heart rate and activity data for each bout of activity with three different SCBA weights. Heart rate data include peak heart rate across the activities (HRPeak) and peak heart rate as a percent of maximum heart rate (HRPeak % of HRmax). (‡) indicates Bout 2 is significantly different than data from Bout 1. Data are shown as mean (standard deviation).
Physiological responses to firefighting activities with different SCBA weights
A significant main effect of SCBA was detected for VO2peak (p = 0.046, ). Participants were able to obtain a significantly greater VO2peak with SCBA1 than with SCBA3 (p = 0.042). When VO2Peak was normalised as the percent of VO2Max, there were near significant differences between SCBA (p = 0.060).
Table 3. Peak values and post-firefighting assessment after completing simulated firefighting activities with three different SCBA weights for Work Time, peak rate of oxygen consumption (VO2Peak), peak rate of oxygen consumption as a percent of maximal rate of oxygen consumption (VO2peak % of VO2max), core temperature rate of rise (Tco,RoR), and visual analog scales of Comfort, Mobility, Fatigue, and Subjective Difficulty (scored -8 to +8). Superscripts (i.e. 1,2,3) indicate significant differences from SCBA noted in superscript. Data are shown as mean (standard deviation).
There were no significant main effects of SCBA in HRPeak or HRPeak(%Max) (), though there were significant main effects of Bout for HRPeak and HRPeak(%Max) (p = 0.040 and p = 0.044 respectively) with participants having higher heart rates and a higher heart rate as percentage of max in the second bout of activity. There were no significant SCBA × Bout interactions. There were no significant main effects of SCBA for Tco,RoR (n = 6) ().
Perceptions after firefighting activities with different SCBA weights
No main effect for SCBA was detected for the self-reported RPE, Breathing Scale, or Thermal Sensation Scale, though there was a significant main effect of PrePost for all measures (p < 0.001). On average participants reported ‘No Exertion’ to ‘Very Light Exertion’ levels prior to activity and increased exertion ranging from ‘Very Hard’ to ‘Maximal Exertion’ levels after firefighting (RPE, p < 0.001, ). Participants reported breathing harder and feeling hotter after activity (p < 0.001), specifically that they were breathing ‘OK’ and ‘Comfortable’ prior to firefighting activity and that they were, on average, ‘Not Getting Enough Air’ and between ‘Hot’ and ‘Unbearably Hot’ following activity. There was a significant interaction between the main effects for RPE (p = 0.035) though post-hoc analysis showed no pairwise differences.
Table 4. Perceptions pre- and post- firefighting activity by SCBA. (✢) Indicates significantly different from Pre. Data are shown as mean (standard deviation). Post hoc analysis revealed no significant differences for interaction effects.
There was a main effect of SCBA (p = 0.020) observed for Comfort (). Post hoc analysis revealed significant differences between SCBA1 and SCBA2 (p = 0.017). There was a main effect of SCBA (p = 0.005) observed for Body Mobility () with significant differences between SCBA1 and SCBA2 (p = 0.018) and between SCBA1 and SCBA3 (p = 0.021) suggesting that participants felt that they had less mobility with heavier SCBA. There was also a main effect of SCBA (p = 0.045) for Fatigue () with participants reporting feeling significantly more fatigued with SCBA2 relative to SCBA 1 (p = 0.023). There was a main effect of SCBA (p < 0.001) for Subjective Difficulty in Carrying out the Activity with SCBA (). Significant differences between SCBA1 and SCBA2 (p < 0.001) and between SCBA1 and SCBA3 (p < 0.001) were observed suggesting the participants felt more restricted with heavier SCBA.
Changes in functional balance after firefighting activities with different SCBA weights
There was no main effect of SCBA for functional balance performance index (p = 0.520, ). There was also a significant main effect of PrePost (p = 0.002) with trials after firefighting activities taking longer than trials conducted pre-firefighting activity. There were no significant interaction effects between the main effects.
Table 5. Performance Index (PI) by SCBA and PrePost without and with the crossbar present. (✢) Indicates significantly different from Pre. Data are shown as mean (standard deviation).
Discussion
The results of this study showed increases in SCBA weight of 2.3 and 4.5 kg had limited impact on the physiological response and functional balance of the firefighters when completing intermittent simulated firefighting activities, though all activities resulted in a large physiological response and decreased functional balance test performance post-activity. However, participants reported having less mobility and increased subjective difficulty with increased SCBA weight. Participants performed less work in a second bout of activity, reported higher thermal sensation and reported they were not breathing as effectively after firefighting activities compared to pre-activity. Furthermore, firefighters’ functional balance test performance was significantly worse following firefighting activities compared to pre-activity.
Participants completed activities in the environmental chamber until they reached volitional fatigue. Pairwise comparisons between SCBA1 and SCBA3 (p = 0.101) and between SCBA2 and SCBA3 (p = 0.046) show the trend towards decreased Work Time with the heaviest SCBA, though the main effect of SCBA was not significant (p = 0.052). Average Work Time was 35.9 min, 35.7 min, and 31.2 min for SCBA1, SCBA2, and SCBA3 respectively. Work Time ranged from 15 min to 40 min for SCBA3. This wide range resulted in standard deviations twice as large as for SCBA1 and SCBA2. It is likely that the large range of Work Times with SCBA3 reduced the likelihood of reaching statistical significance. The magnitude of the difference in Work Time between SCBAs could be critical to fireground operations. For example, the standard 30- and 45-min SCBA cylinders hold 1274 and 1840 litres of compressed air respectively and ventilation rates during firefighting tasks can approach 100 L/min (Kesler et al. Citation2017) suggesting that the entire capacity could be consumed in less than 20 minutes. When the end of service time indicator alerts (when 33% of the air supply remains and firefighters should be out of the structure) actual working time may have only been 12-15 minutes. A median difference in working time, reported as the time to reach volitional fatigue, of more than 4 minutes between SCBA1/2 and SCBA3 may significantly affect the amount of work able to be completed by a company during fireground operations.
In a previous study using the same exercise protocol, 11 out of 30 participants were unable to complete three separate trials with two bouts of simulated firefighting activity (Kesler et al. Citation2017). In the previous study, participants used lighter SCBA (range 9.9 kg-13.3 kg), breathed from the SCBA that they were wearing, and had higher maximal oxygen consumption levels during the baseline test. The combination of lighter SCBA, relatively cool supplied air, and increased aerobic capacity may have allowed more participants to complete all firefighting activities relative to the current study which utilised heavier SCBA and required participants to breathe ambient air in the environmental chamber (47 °C, ∼30% humidity).
Peak O2 consumption rates in this study (average 29.1 to 31.6 ml/min/kg) are slightly higher than those during similar activities in a previous study with lighter SCBA (average 14.6 to 28.7 ml/min/kg, Kesler et al. (Citation2017)). Peak O2 consumption rates in this study represent 55.1% to 97.7% of the participants’ maximal O2 consumption rate. The peak O2 consumption rate was reduced in SCBA3 when compared to SCBA1, but not when normalised as a percentage of the maximal O2 consumption rate during the treadmill test. It is possible that the reduced rate of O2 consumption contributed to the nearly significant reduction in Work Time with the heaviest SCBA. If decreased O2 consumption rates led to hypoxaemia and thus decreased oxygenation of the brain, the participant may have felt dizzy or light-headedness and been removed from the chamber. Likewise, if participants were unable to provide adequate O2 to the working muscles, the participant may have perceived increase muscle strain and elected to end the trial sooner.
Peak heart rates (and peak heart rates as a percent of maximum heart rate) were higher in the second bout of activity than in the first bout. This aligns with previous research (Horn et al. Citation2013; Hostler et al. Citation2016; Walker et al. Citation2015) and reinforces that adequate recovery time is necessary between bouts of firefighting. Schlader, Colburn, and Hostler (Citation2017) examined the effect of overnight rest on 20-minute bouts of activity and found that heart rate response was similar between bouts indicating that 24 hours rest is sufficient rest for heart rate response, though other measures (core temperature, perceived exertion, and thermal sensation) were elevated post-activity on Day 2 relative to Day 1.
It is well accepted that firefighting activity induces near max heart rates and this study corroborated that assertion. Average peak heart rate was 182 bpm (range 162-204 bpm), which is slightly lower than the average reported by Kesler et al. (Citation2017) for two bouts of activity with lighter SCBA, likely due to some participants reaching volitional fatigue before completing the both bouts of activity. Horn et al. (Citation2015) also reported higher heart rates than the current study, though only a single bout of activity was completed. In both previous studies participants had higher maximal O2 consumption rates and maximal heart rates during baseline tests, despite similar average ages. Peak heart rates in this study ranged from 81% to 110% of the maximum heart rate obtained during the maximal treadmill test which encompasses the percentages of maximal heart rates during activity in previous studies (94% to 99% in Kesler et al. (Citation2017)).
Core temperatures and rates of core temperature rise were not significantly impacted by the increased SCBA weights utilised in this study. As expected, core temperature was elevated during firefighting activity with an average rate of rise of 0.040 °C/min. Several studies that have examined core temperature rate of rise during live-fire activities have reported rates of 0.050 °C/min over 12 min of activity (Burgess et al. Citation2012), 0.037 °C/min over 18 min (Horn et al. Citation2011), 0.040 °C/min over 18 minutes (Smith et al. Citation2011), and 0.035 °C/min over 20 minutes (Colburn et al. Citation2011). In the study done by Kesler et al. (Citation2017) utilising the same firefighting protocol but lighter SCBA, rate of core temperature rise was 0.031 and 0.032 °C/min for SCBA weighing 9.9 kg and 13.3 kg respectively. Peak core temperature was significantly higher in the heaviest SCBA used by Kesler et al. (Citation2017). The current study found no statistical differences in core temperature rate of rise between the various weights of SCBA used in this study. Importantly though, the rates of increase were all higher than those reported by Kesler et al. (Citation2017) suggesting that given the same environment and tasks, substantially heavier SCBA may increase the core temperature rate of rise.
Other factors may have more clinically relevant impact on core temperature than the SCBA weight. In the present study, PPE, firefighting tasks, and the environment are all closely controlled in an attempt to limit their impact on variability. Further, the population in this study consisted of active male firefighters who are moderately fit and healthy. This study excluded female firefighters based on the representative population size in the United States fire service. Firefighters have a wide range of fitness levels and those with lower overall fitness levels are less likely to volunteer given the intensity of the work performed in this study despite the authors’ efforts to recruit firefighters with a wide range of fitness levels. Changes in these descriptive parameters, especially over a relatively short duration, may affect the core temperature more than the SCBA weight.
During the second bout of activity participants were consistently unable to match the amount of work they completed during the first bout. This was true across all SCBAs, though the specific SCBA did not impact the decrease in work completed. The number of repetitions of stairs and search distance in this study are considerably less (approximately half) than those completed in a similar protocol with lighter SCBA and participants with higher maximal oxygen consumption levels (Kesler et al. Citation2017). However, participants completed more hose advance and overhaul repetitions in this study. It is possible that the heavier SCBA utilised in this study were more limiting in the stairs and search activities than the hose advance and overhaul activities. The stair climb and search activities require physically moving the entire body while wearing the SCBA to complete the task. In the hose advance and overhaul activity the participant is primarily stationary and utilises the upper extremities to advance the tool to the target.
Participants performed worse on the FBT following firefighting activity, a result that agrees with previous studies (Hur et al. Citation2013; Kesler et al. Citation2017; Son, Muraki, and Tochihara Citation2022). Kesler et al. (Citation2018b) utilised similar firefighting activities and environmental conditions to those in the present study, but lighter SCBA, and noted average PI scores ranging from 6.8 to 7.9 when no crossbar was present. In that study SCBA weight (9.9 to 13.3 kg) did not have a significant impact on PI without the crossbar, however lighter SCBA resulted in lower PI scores when the crossbar was present. The present study’s average PI scores pre-firefighting activity without the crossbar (7.4 to 7.9) are comparable to those in Kesler et al. (Citation2018b), however post-activity PI scores without the crossbar are substantially higher in the present study (12.2 to 13.6 as opposed to 7.7 to 7.9). Despite firefighters’ similar physiological responses and FBT performance between SCBA in this study, it is possible that the higher SCBA weights used in the present study more negatively affected FBT performance than lighter SCBA used in previous studies.
Measures of perceived exertion, thermal sensation, and breathing were more negative after firefighting activity, but no differences were noted between the various SCBA. The firefighters’ rating of perceived exertion in this study is comparable to that reported in previous work for similar repeated bouts of firefighting activity, however, both thermal sensations and breathing scale appear to be more negative in this study than Kesler et al. (Citation2017). Many studies have reported a similar change to more negative perceptual responses following firefighting activity (Kesler et al. Citation2017; Schlader, Colburn, and Hostler Citation2017; Walker et al. Citation2005). The participants in this study had lower baseline maximal O2 consumption rates than those in Kesler et al. (Citation2017), which may have led to participants perceiving more difficulty in breathing.
There were significant differences between SCBA conditions for firefighters’ responses to the Visual Analog Scales that were completed at the end of each trial. Interestingly, SCBA2 was significantly different from SCBA1 and SCBA3 for perceptive measures of overall Comfort and Fatigue. There was a trend towards decreased Work Time with SCBA3 relative to SCBA2, which may have contributed to the difference in perceptions. There were significant differences in Mobility and Difficulty with SCBA1 being less negative than SCBA2 and SCBA3. The participants in this study were all firefighters and averaged 8.2 years of fire service experience. It is reasonable to expect that the participants regularly wear SCBA that weigh equal to or less than the SCBA1 utilised in this study. Thus, it is possible that the participants were able to perceive that the SCBA2 and SCBA3 were significantly heavier and thus scored them more negatively. This finding is also consistent with the results of biomechanical models which suggested that the maximum comfortable weight for an SCBA was 17.7 kg which is between SCBA1 and SCBA2 (Xu et al. Citation2021b).
While this study provides the first controlled comparison of increasing SCBA weight above current standards on firefighters’ physiological, perceptual, and functional balance measures, there are important limitations. Some data loss occurred with six out of the 10 participants having accurate core temperature data for each of the three trials. With the already limited participant numbers, this data loss further limits our ability to make statistical inferences related to core temperature. Further, participants operated in the environmental chamber breathing the ambient air (47 °C, ∼30% humidity), which is warmer and higher in humidity than the compressed air utilised in the SCBA. There is also no reduction in SCBA weight as the compressed air is consumed and exhaled throughout the firefighting activities. These limitations were anticipated, but improvements could be made to further these research efforts.
Future research efforts to understand the impact of increased SCBA weight on firefighter performance should look to expand the data presented here with additional participants. This study was limited to 10 male firefighters. Inclusion of female firefighters and a broader range of age and fitness levels would increase the sample size and representation of the fire service. An increased subject pool could also allow for analysis of how individual factors such as fitness, strength, or BMI affect physiological response and performance when SCBA weight is increased. To further support this expanded analysis, increased weight could be proportional to the firefighter’s body mass. Additional data including measures of cognitive function, decision-making ability, and agility would provide supplemental information about fireground performance.
Conclusions
The objective of this study was to examine the impact of SCBA weight on firefighter physiological response and biomechanical performance with the intent to inform decision makers on the impacts of adjusting existing limits for SCBA weight in NFPA 1981 (National Fire Protection Association Citation2019). Quantitative measures of heart rate, core temperature, and O2 consumption rate showed few statistically significant differences between SCBA with weights that are increased by 2.3 kg and 4.5 kg above current limits. However, participants felt that the heavier SCBA reduced body mobility and increased the subjective difficulty in completing the assigned tasks. There were also trends towards significance for time the participant was able to work in the environmental chamber prior to reaching volitional fatigue. Comparison between the impact of SCBA used in the current study and the effects of lighter SCBA from previous studies (Kesler et al. Citation2018b, Kesler et al. Citation2017) suggest greater core temperature rate of rise and poorer performance on a functional balance test with the heavier SCBAs.
As these data are reviewed by firefighters, fire departments, equipment manufacturers, and standard setting organisations, it is important to consider the negative impacts on working time and the more negative perceptions on mobility and difficulty in completing the task with heavier SCBA. The data reported here and similar studies using lighter SCBA and alternate weight distributions should be reviewed to cover a broad range of SCBA weights and designs. Attention should also be given to biomechanical models analysing comfortable working weight and weight distribution.
Ethics statement
All protocols used in this study were approved by the University of Illinois Institutional Review Board, under IRB #20927.
Acknowledgements
The authors thank all the firefighters who participated in the study and Spencer Romine, Whitney Anderson, Scott Kesler, Adrian Zavala, and Maddy Szamocki for their assistance in data collection.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Bakri, I., J. Y. Lee, K. Nakao, H. Wakabayashi, and Y. Tochihara. 2012. “Effects of Firefighters’ Self-Contained Breathing Apparatus’ Weight and Its Harness Design on the Physiological and Subjective Responses.” Ergonomics 55 (7): 782–791. doi:10.1080/00140139.2012.663506.
- Borg, G. 1970. “Perceived Exertion as an Indicator of Somatic Stress.” Scandinavian Journal of Rehabilitation Medicine 2 (2): 92–98.
- Burgess, J. L., M. D. Duncan, C. Hu, S. R. Littau, D. Caseman, M. Kurzius-Spencer, G. Davis-Gorman, and P. F. McDonagh. 2012. “Acute Cardiovascular Effects of Firefighting and Active Cooling during Rehabilitation.” Journal of Occupational and Environmental Medicine 54 (11): 1413–1420. doi:10.1097/JOM.0b013e3182619018.
- Campbell, R., and S. Hall. 2022. United States Firefighter Injuries in 2021. Quincy, Massachusetts, US: National Fire Protection Association.
- Colburn, D., J. Suyama, S. E. Reis, J. L. Morley, F. L. Goss, Y. F. Chen, C. G. Moore, and D. Hostler. 2011. “A Comparison of Cooling Techniques in Firefighters after a Live Burn Evolution.” Prehospital Emergency Care 15 (2): 226–232. doi:10.3109/10903127.2010.545482.
- Fahy, F. R., and J. T. Petrillo. 2022. Firefighter Fatalities in the United States in 2021. Emmitsburg, Maryland, US: US Fire Administration National Fire Data Center.
- Horn, G. P., S. Blevins, B. Fernhall, and D. L. Smith. 2013. “Core Temperature and Heart Rate Response to Repeated Bouts of Firefighting Activities.” Ergonomics 56 (9): 1465–1473. doi:10.1080/00140139.2013.818719.
- Horn, G. P., S. Gutzmer, C. A. Fahs, S. J. Petruzzello, E. Goldstein, G. C. Fahey, B. Fernhall, and D. L. Smith. 2011. “Physiological Recovery from Firefighting Activities in Rehabilitation and beyond.” Prehospital Emergency Care 15 (2): 214–225. doi:10.3109/10903127.2010.545474.
- Horn, G. P., R. M. Kesler, S. Kerber, K. W. Fent, T. J. Schroeder, W. S. Scott, P. C. Fehling, B. Fernhall, and D. L. Smith. 2017. “Thermal Response to Firefighting Activities in Residential Structure Fires: impact of Job Assignment and Suppression Tactic.” Ergonomics 61 (3): 404–419. doi:10.1080/00140139.2017.1355072.
- Horn, G. P., R. M. Kesler, R. W. Motl, E. T. Hsiao-Wecksler, R. E. Klaren, I. Ensari, M. N. Petrucci, B. Fernhall, and K. S. Rosengren. 2015. “Physiological Responses to Simulated Firefighter Exercise Protocols in Varying Environments.” Ergonomics 58 (6): 1012–1021. doi:10.1080/00140139.2014.997806.
- Hostler, D., D. Colburn, J. C. Rittenberger, and S. E. Reis. 2016. “Effect of Two Work-to-Rest Ratios on Cardiovascular, Thermal, and Perceptual Responses during Fire Suppression and Recovery.” Prehospital Emergency Care 20 (6): 681–687. doi:10.3109/10903127.2016.1168890.
- Hur, P., K. Park, K. S. Rosengren, G. P. Horn, and E. T. Hsiao-Wecksler. 2015. “Effects of Air Bottle Design on Postural Control of Firefighters.” Applied Ergonomics 48: 49–55. doi:10.1016/j.apergo.2014.11.003.
- Hur, P., K. Rosengren, G. Horn, D. Smith, and E. Hsiao-Wecksler. 2013. “Effect of Protective Clothing and Fatigue on Functional Balance of Firefighters.” Journal of Ergonomics S2 (02) doi:10.4172/2165-7556.S2-004.
- Kesler, R. M., F. F. Bradley, G. S. Deetjen, M. J. Angelini, M. N. Petrucci, K. S. Rosengren, G. P. Horn, and E. T. Hsiao-Wecksler. 2018a. “Impact of SCBA Size and Fatigue from Different Firefighting Work Cycles on Firefighter Gait.” Ergonomics 61 (9): 1208–1215. doi:10.1080/00140139.2018.1450999.
- Kesler, R. M., G. S. Deetjen, F. F. Bradley, M. J. Angelini, M. N. Petrucci, K. S. Rosengren, G. P. Horn, and E. T. Hsiao-Wecksler. 2018b. “Impact of SCBA Size and Firefighting Work Cycle on Firefighter Functional Balance.” Applied Ergonomics 69: 112–119. doi:10.1016/j.apergo.2018.01.006.
- Kesler, R. M., I. Ensari, R. E. Bollaert, R. W. Motl, E. T. Hsiao-Wecksler, K. S. Rosengren, B. Fernhall, D. L. Smith, and G. P. Horn. 2017. “Physiological Response to Firefighting Activities of Various Work Cycles Using Extended Duration and Prototype SCBA.” Ergonomics 61 (3): 390–403. doi:10.1080/00140139.2017.1360519.
- Morgan, W. P., and P. B. Raven. 1985. “Prediction of Distress for Individuals Wearing Industrial Respirators.” American Industrial Hygiene Association Journal 46 (7): 363–368. doi:10.1202/0002-8894(1985)046<0363:PODFIW>2.3.CO;2.
- National Fire Protection Association. 2019. NFPA 1981: Standard on Open-Circuit Self-Contained Breathing Apparatus (SCBA) for Emergency Services. Quincy, Massachusetts, US: National Fire Protection Association.
- National Fire Protection Association. 2022. NFPA 1582: Standard on Comprehensive Occupational Medical Program for Fire Departments. Quincy, Massachusetts, US: National Fire Protection Association.
- Punakallio, A. 2003. “Balance Abilities of Different-Aged Workers in Physically Demanding Jobs.” Journal of Occupational Rehabilitation 13 (1): 33–43. doi:10.1023/a:1021845823521.
- Punakallio, A. 2004. “Trial-to-Trial Reproducibility and Test-Retest Stability of Two Dynamic Balance Tests among Male Firefighters.” International Journal of Sports Medicine 25 (3): 163–169. doi:10.1055/s-2003-45251.
- Punakallio, A., V. A. Louhevaara, and S. Lusa-Moser. 1997. “Evaluation of a Functional Test for Assessing Dynamic Balance of Fire Fighters.” 13th Triennial Congress of the International Ergonomics Association 13th Triennial Congress of the International Ergonomics Association, Helsinki, Finland.
- Punakallio, A., S. Lusa, and R. Luukkonen. 2003. “Protective Equipment Affects Balance Abilities Differently in Younger and Older Firefighters.” Aviation, Space, and Environmental Medicine 74 (11): 1151–1156.
- Punakallio, A., S. Lusa, and R. Luukkonen. 2004. “Functional, Postural and Perceived Balance for Predicting the Work Ability of Firefighters.” International Archives of Occupational and Environmental Health 77 (7): 482–490. doi:10.1007/s00420-004-0536-z.
- Schlader, Z. J., D. Colburn, and D. Hostler. 2017. “Heat Strain is Exacerbated on the Second of Consecutive Days of Fire Suppression.” Medicine and Science in Sports and Exercise 49 (5): 999–1005. doi:10.1249/MSS.0000000000001191.
- Smith, D. L., S. J. Petruzzello, E. Goldstein, U. Ahmad, K. Tangella, G. G. Freund, and G. P. Horn. 2011. “Effect of Live-Fire Training Drills on Firefighters’ Platelet Number and Function.” Prehospital Emergency Care 15 (2): 233–239. doi:10.3109/10903127.2010.545477.
- Son, S.-Y., S. Muraki, and Y. Tochihara. 2022. “Exploring the Appropriate Test Methods to Examine the Effects of Firefighter Personal Protective Equipment on Mobility.” Fashion and Textiles 9 (1): 22. doi:10.1186/s40691-022-00295-8.
- Thomas, S., J. Reading, and R. J. Shephard. 1992. “Revision of the Physical Activity Readiness Questionnaire (PAR-Q).” Canadian Journal of Sport Sciences = Journal Canadien Des Sciences du Sport 17 (4): 338–345.
- Walker, A., C. Argus, M. Driller, and B. Rattray. 2015. “Repeat Work Bouts Increase Thermal Strain for Australian Firefighters Working in the Heat.” International Journal of Occupational and Environmental Health 21 (4): 285–293. doi:10.1179/2049396715Y.0000000006.
- Walker, P., P. Rhubart-Berg, S. McKenzie, K. Kelling, and R. S. Lawrence. 2005. “Public Health Implications of Meat Production and Consumption.” Public Health Nutrition 8 (4): 348–356. doi:10.1079/phn2005727.
- Xu, S., M. Hu, J. Powell, and Z. Zhuang. 2021a. Biomechanical Modeling and 3D Simulation of Firefighting Tasks. Cham: Springer International Publishing.
- Xu, S., M. Hu, J. Powell, and Z. Zhuang. 2021b. Comfortable SCBA Weights from Biomechanical Models for Firefighting Tasks. Cham: Springer International Publishing.
- Young, A. A. 1987. “Thermal Sensations during Simultaneous Warming and Cooling at the Forearm: A Human Psychophysical Study.” Journal of Thermal Biology 12 (4): 243–247. doi:10.1016/0306-4565(87)90023-4.