
Abstract
The COVID-19 pandemic focused the world’s attention on the gross relative health risks, inequities and injustices experienced by first responders, of whom front-line, hospital-based nurses may be the most vulnerable. A series of research syntheses prior to the pandemic estimated that such front-line nurses were at approximately two-fold greater risk of experiencing mental health challenges such as increased symptoms (and diagnoses) of anxiety, depression and PTSD than were nursing administrators or otherwise similar, people in the general population. Aiming to clarify how the pandemic impacted such mental health risks, we conducted a rapid review and meta-analysis of observational studies from the worldwide published and gray research literature. Twelve longitudinal studies that covered the pandemic’s pre-vaccination phase were included. The overall pooled increased relative risk of mental health challenges among frontline, hospital-based nurses from pre-pandemic to the pre-vaccination phase of the COVID-19 pandemic was 2.62 (95% CI 2.10, 3.27). But sensitivity and moderator analyses accounting for research design limitations better estimated two-fold increased risks (relative risks ranged from 1.69 to 2.00). Already at elevated risk of experiencing symptoms of anxiety, depression and PTSD and so, such increased symptoms and diagnoses among front-line, hospital-based nurses probably doubled during the early, pre-vaccination phase of the pandemic, perhaps quadrupling among women. Implications for nursing practice, health care policy, future pandemic preparedness as well as future research are discussed.
Introduction
Since declaring the coronavirus disease-19 (COVID-19) a worldwide pandemic on March 11, 2020, the World Health Organization (WHO) reported more than 775 million confirmed cases of the novel respiratory disease and more than seven million resultant deaths by the spring of 2024, the time of this writing (World Health Organization [WHO], 2020, 2023); of these, 765 million confirmed cases and 6.9 million deaths had been reported by the time the WHO declared COVID-19 to no longer be a public health emergency in May 2023 (United Nations [UN], Citation2023). In addition to such clear physical health consequences, there seem dire mental health consequences as well. Again, the WHO (Citation2022) estimated that the global prevalence of anxiety and depression increased by 25% during the first year of the pandemic. Surely certain groups of people experienced much greater risks. In fact, prior to the pandemic, frontline hospital-based nurses, who most predominately worked in acute and critical care areas such as emergency departments and intensive care units, already had prevalent symptoms or diagnoses of anxiety, depression or posttraumatic stress disorder (PTSD) that were 25% greater than those observed among otherwise similar people in the general population or among frontline physicians or non-frontline administrative nursing staff (Robinson et al., Citation2022; Trudgill et al., Citation2020).
We are unaware of any previous research synthesis on the impacts of the COVID-19 pandemic on frontline, hospital-based nurses’ mental health. This review aims to expeditiously fill this knowledge gap. In addition to their clear vulnerability prior to the COVID-19 pandemic, such nurses will be this study’s focus for the following reasons. First, nurses’ mental health has been demonstrated to have been significantly and negatively impacted by previous, less severe and more localized viral outbreaks such as severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS; Brooks et al., Citation2018; Lee et al., Citation2018; Magnavita et al., Citation2021). Second, COVID-19 not only increased the comorbid complexity of the patients nurses cared for, but also greatly increased nurses’ own risks of serious illness and death. The WHO (Citation2021) estimated that more than 100,000 health care workers, the majority of whom were nurses, died during the early, pre-vaccination phase of the pandemic. The pre-vaccination phase was a period of maximum vulnerability; we had the least amount of information about COVID-19, and there were no available proven treatments. Third, the population of at-risk, nurses providing, for example, critical care in transformed medical wards tripled during the pandemic as their workloads as well as the care demands of their patients concomitantly increased substantially (Hoogendoorn et al., Citation2021; Keene et al., Citation2021). Fourth and finally, such mental health conditions are well known to be associated with impaired social and occupational functioning (American Psychiatric Association, Citation2022). Such illness among nurses was very likely associated with lower health care quality, prior to and during the COVID-19 pandemic (Havaei et al., Citation2022). This rapid review and meta-analysis, therefore, poses the following research question: How has the COVID-19 pandemic impacted the mental health of frontline hospital-based nurses compared to their pre-pandemic self-reported mental health?
Review of previous, tangentially relevant, reviews
As we began our systematic searches of the relevant research literature, we surprisingly found five previous reviews; four systematic reviews, three of which had meta-analytic components, and one umbrella review of previous systematic reviews (Al Maqbali et al., Citation2021; Chirico et al., Citation2021; Ślusarska et al., Citation2022; Varghese et al., Citation2021; Xu et al., Citation2021). In reviewing more than 100 primary studies these research syntheses, in aggregate, estimated symptoms of mental illness and or diagnoses such as anxiety disorders, depression or PTSD to have been experienced by approximately one third of all frontline nurses during the pandemic. Moreover, one of the meta-analyses tested the potential moderating influence of gender and found that the risks of experiencing such profound mental health challenges were significantly greater among female than male nurses (Varghese et al., Citation2021). Regrettably, all but one of the previous reviews confounded the experiences of nurses with those of other health care workers, and all of the more than 100 primary studies reviewed were cross-sectional. As such, though they confidently estimated the magnitude of the problem at one point in time (i.e., mental illness among frontline nurses), they could not possibly have assessed the pandemic-specific effects or impacts as their exclusively cross-sectional designs could not have observed changes in the mental health of nurses during the pandemic; longitudinal studies would be needed for such assessments. This research synthesis, therefore, will systematically replicate this field’s previous reviews and meta-analyses with a sample of longitudinal studies.
Hypotheses
We first hypothesized that the mental health of frontline, hospital-based nurses will have diminished significantly during the COVID-19 pandemic. Secondly, we explored the following moderator hypothesis: Mental health challenges such as having experienced increased symptoms of anxiety or depression occurred more commonly among such female than male nurses during the COVID-19 pandemic.
Methods
As a meta-analysis, our study did not directly involve human subjects and therefore did not require ethics approval from an institutional review board (IRB; Sullivan, Citation2011). All data included in this meta-analysis were publicly available, and were from primary studies that had previously received approval from their researchers’ respective IRBs.
Study selection
Under temporal, fiscal and logistic constraints, aiming to synthesize knowledge expeditiously and efficiently for decision makers, publics and future researchers, we performed a rapid review and pooled meta-analysis of observational longitudinal primary studies (Deeks et al., Citation2021; Ganann et al., Citation2010; Stroup et al., Citation2000; Tricco et al., Citation2015). The following research literature databases were searched in the spring of 2022 for longitudinal studies that were initiated prior to the COVID-19 pandemic and included a longitudinal follow-up measurement during or immediately after the pre-vaccination phase of the pandemic, all published in their final form in 2020, 2021 or 2022: Cumulative Index of Nursing and Allied Health Literature Complete, Google Scholar, medRxvi, ProQuest Coronavirus Research Database, ProQuest Dissertations & Theses Global, PubMed/Medline, PsycINFO, and the WHO Covid-19 Database. In addition to peer-reviewed, published literature, so-called grey, unreviewed unpublished literature such as government documents, community or professional conference-based reports, and dissertations were searched to guard against publication bias (de Smidt & Gorey, Citation1997; Grenier & Gorey, Citation1998).
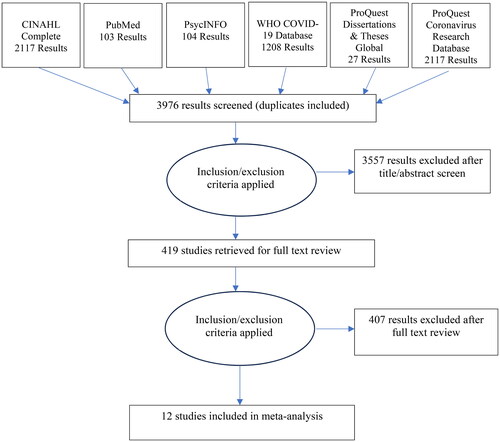
Research literature databases were searched with exhaustive iterations of this broad keyword search scheme that were then systematically replicated with subject terms specific to each database: (COVID-19 or SARS-CoV-2 or coronavirus [anywhere]) and (anxiety or depress* or posttraumatic stress* or suicid* or alcohol, drug or substance dependence, misuse or abuse [title/abstract]) and (nurs* [title/abstract]). Eligible studies also had to meet the following inclusion criteria: (1) 50% or more of participants were hospital-based, frontline nurses, or nursing subsample findings were reported separately; (2) used a longitudinal design with a baseline prior to 2020, or a pseudo-longitudinal design such as a cross-sectional survey design with an external comparison group that was assessed prior to 2020, or analogously included comparative places where COVID-19 had not yet prevalently intruded, or used a retrospective measure to assess pre-pandemic mental health; (3) findings were reported in enough detail to allow for calculation of practical effect size metrics as well as for the assessment of their statistical significance and precision; and (4) report was written in English. Most studies were excluded for multiple reasons, but the central, most restricting reason for exclusion for nearly all was that they were prevalence surveys, incapable of assessing incidence, change or impacts due to the COVID-19 pandemic. The primary study selection process is outlined with a PRISMA diagram (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) in (Kelly et al., Citation2016; Moher et al., Citation2009). First, 3976 conceptually relevant studies were screened for their potential empirical relevance by one reviewer based upon their titles and abstracts. The initial screening resulted in 419 studies being selected for full-text review, which was completed by two independent reviewers. Then empirically and methodologically relevant studies were selected; the two reviewers’ initial agreement was 80.0%. After the few disagreements were resolved through discussion and cross-validated with an experienced meta-analytic research assistant, 12 studies were finally selected for meta-analysis. They are indicated with an asterisk in the reference list.
Figure 1. PRISMA diagram of literature search results.
Meta-analysis of observational studies
The unit of analysis for this synthesis was the unique hypothesis test, that is, if a study provided two hypothesis tests (e.g., on both anxiety and depressive outcomes), both were included in this analysis. Pre-during pandemic comparisons were observed on mental health challenges, primarily self-reported symptoms of anxiety, PTSD and or depression. These were treated as independent hypotheses. A total of 18 independent findings from 12 studies were included in this synthesis, with 6 of the studies contributing a pooled estimate. Each study contributed once to the overall mental health hypothesis test; if a primary study provided multiple relevant outcomes, they were pooled so that the study would contribute one data point for the hypothesis test. Prevalence ratios (PR), odds ratios (OR), rate ratios (RR), or similar measures of association estimated primary study relative risks (RR). Natural logarithms of study RRs were weighted by their inverse variances so that larger studies carried more weight. Sample-weighted, random effects were then pooled using meta-regression models (Cooper, Citation2017; Fleiss et al., Citation2003; Greenland, Citation1987). Pooled RRs within 95% CIs were calculated from regression statistics, as were tests of heterogeneity and between-group meta-analytic comparisons, distributed as I2 and χ2 statistics. Statistical decisions were made at the α criterion of 0.05 and RRs greater than 1.00 indicated increased mental health challenges. As for interpreting associations, an exemplary RR of 2.00 would mean that frontline, hospital-based nurses were twice as likely to experience symptoms of anxiety, PTSD and or depression during the pandemic as they themselves or otherwise similar nurses were prior to the pandemic. Finally, after reliable extraction of descriptive characteristics of the primary study reports, participants and designs that are displayed in the first three columns of (89.6% initial agreement between two reviewers that reached consensus with discussion) outcome effect size calculations and this synthesis were accomplished with version 3 of Comprehensive Meta-Analysis (Borenstein et al., Citation2013) by two cooperating analysts.
Table 1. Descriptive characteristics and 18 mental health outcomes of the 12 studies included in the meta-analysis.
Results
Sample description
Descriptive characteristics and outcomes of the 12 studies included in the meta-analysis are displayed in . Thanks probably to editorial expedition of such research during the COVID-19 pandemic, all 11 articles and a dissertation were published in either 2021or 2022. About half longitudinally followed the pandemic’s first three to six months, the others up to its first year. They all essentially followed frontline, hospital-based nurses before vaccines were available. The earliest three studies were accomplished in China, while one each was accomplished in nine other countries: USA, Canada, Spain, South Africa, Japan, Turkey, Saudi Arabia, Jordan and Iran. As expected, primary study participants were largely young to middle aged women; their median age was 32 among the six studies that provided such estimates, and the percentage of women in each primary study sample ranged from 60% to 90%, most typically 83%. As for nurse versus other health care worker representations, eight of the primary studies sampled only nurses, while the other five studies ranged in nurse representations from 63% to 86% (Mdn = 78%). Weighting by sample sizes, the aggregated meta-analytic sample was comprised mostly of nurses (94%).
Eight of the primary studies were successive cross-sections; seven of these trend studies, one a panel study. The other four studies were surveys, augmented with external, pre-pandemic comparison groups or with retrospective measures. Eight of the studies were accomplished online and all but one of the 12 primary studies used convenience sampling methods from accessible populations. Furthermore, the primary study designs varied greatly, so some of them may be limited in other important ways. For example, participant outcome sample sizes ranged widely from only 51 to more than 2,000, typically seeming to be adequately powered (median n = 374). Half of the studies provided some measure of control for potential confounds such as age, gender and others through sample restriction or regression modeling, while half provided no such control. Additionally, most of the studies used established, standardized measures, while two developed and used original, single-item measures. Only one study reported response rates, suggesting marginally adequate responding pre-pandemic (66%) with a significantly lower response rate (48%) during the pandemic. Clearly, synthetic interpretations will need to account for such research methodological variability. Finally, all 18 of the mental health outcomes reported by the 12 primary studies included in this research synthesis as well as the pooled outcomes for studies that reported multiple relevant mental health outcomes are displayed in the far-right column of the table. As after accounting for other study characteristics (see below) the pandemic-mental health associations were similar across the represented conceptual outcomes of anxiety, depression, PTSD, cigarette consumption (addictions) and simply general mental health, they will be meta-analyzed together as a single mental health/illness construct.
Meta-analytic findings
The 12 associations of frontline, hospital-based nurses during the COVID-19 pandemic and mental health ranged from risk ratio point estimates of 1.08 to 36.35, the median being 2.40. In consistent support of our main hypothesis, the 12 point-estimates were all in the hypothesized direction and all but one was statistically significant. Centrally, the overall pooled relative risk of mental health challenges among frontline, hospital-based nurses during the COVID-19 pandemic was 2.62 (95% CI 2.10, 3.27). Next, a sensitivity analysis found that the exclusion of each single study produced a distribution of RRs that ranged from 2.05 to 2.93 (all p < 0.001). A final sensitivity analysis found that even the removal of the two most outlying studies resulted in a pooled association indicating that frontline, hospital-based nurses were substantially impacted during the COVID-19 pandemic (RR = 2.00, 95% CI 1.64, 2.44). Already at elevated risk of experiencing symptoms and probable diagnoses of anxiety, depression or PTSD, the risks among them probably doubled again during the pre-vaccination phase of the pandemic.
Next, that distribution was observed to be significantly heterogeneous, nearly all of its variability potentially being explained by systematic factors like characteristics of the primary study participants, contexts or research designs; χ2 (11) = 909.00, p < 0.05, I2 = 98.8%. We next aimed to test our hypothesis of moderation by gender. As alluded to above, we lacked sufficient meta-analytic power to directly test this hypothesis. Furthermore, none of the primary studies included in this meta-analysis directly tested any potential mental health differences between female and male nurses. However, one study observed the risk of COVID-19 mental health impacts to be more than two and a half times greater among nurses, who were predominantly women, as among other hospital staff, the majority of whom were physicians and predominantly men (OR = 2.60 [95% CI 2.03, 3.34], Katsuta et al., Citation2021).
Finally, other potential moderators were explored. First, the risks of mental health challenges among frontline, hospital-based nurses during the COVID-19 pandemic were observed to be particularly elevated in China (RR = 5.45, 95% CI 2.81, 10.57; χ2 [1] = 8.68, p = 0.003), the USA (RR = 4.46, 95% CI 3.12, 6.38; χ2 (1) = 7.25, p = 0.007) and Saudi Arabia (RR = 13.60, 95% CI 2.84, 65.12; χ2 [1] = 4.31, p < 0.05), but relatively depressed in Japan (RR = 1.08, 95% CI 0.99, 1.18; χ2 [1] = 57.84, p < 0.001). Second, the pooled association among the six studies that provided some measure of control for covariates that might be confounding was significantly lower (RR = 1.69, 95% CI 1.30, 2.18) than that observed among the six, relatively uncontrolled studies (RR = 4.59, 95% CI 2.68, 7.86; χ2 (1) = 10.83, p = 0.001). We think the better controlled estimate to be a closer approximation of the truth. Third, the single grey literature or dissertation report’s association (RR = 4.46, 95% CI 3.12, 6.38) was significantly larger than the pooled association among the 11 published articles (RR = 2.49, 95% CI 1.99, 3.18; χ2 [1] = 7.25, p = 0.007), a finding distinctly counter to any suggestion of publication bias. Lastly, none of the other study participant, contextual or research design characteristics (Greenland, Citation1998) displayed in was observed to be significantly moderating.
Discussion
This rapid meta-analytic review of 12 longitudinal studies identified important novel findings related to changes in frontline, hospital-based nurses’ mental health symptomatology and probable diagnoses as a result of the COVID-19 pandemic. This field’s best controlled longitudinal studies allowed for the following pooled inference in strong support of our central hypothesis. Specifically, symptoms and or diagnoses of anxiety, depression, and PTSD essentially doubled from the pre-COVID to the early-pre-vaccination-COVID time periods. This sharp increase in the relatively short span of time of only three months to a year is not surprising given the often-drastic reactive changes to nursing work environments that the pandemic necessitated. These included the prevalent transfer of non-critical care nurses to substantially expanded ICUs where increasingly sick and contagious patients were cared for by less relevantly experienced nurses with significantly larger and more burdensome workloads (Hoogendoorn et al., Citation2021; Keene et al., Citation2021; Perraud et al., Citation2022; Tang et al., Citation2021; Vera San Juan et al., Citation2022). Next, we asked: What about gender? Without sufficient meta-analytic power to directly test our moderator hypothesis—that such risks were greater among female than male nurses—we did uncover some relevant indirect evidence. One study observed that such mental health risks were significantly and substantially (more than two-fold) greater among female than male health care workers, but its gender comparison was confounded by its mix of nurse and physician participants (Katsuta et al., Citation2021). This inference of greater risks among female nurses specifically, however, is consistent with and so strengthened by the findings of two previous systematic reviews (Trudgill et al., Citation2020; Varghese et al., Citation2021). Finally, recall that it was well known that nurses exhibited mental health challenges at about twice the rate of their general population counterparts before the COVID-19 pandemic. So, the ultimate effect of the probable doubling of mental health symptoms among frontline, hospital-based nurses during the early, pre-vaccination phase of the pandemic, is that the magnitude of their mental health challenges may have grown to magnitudes four-fold greater than those of general, non-nursing populations.
We additionally found that the risks of mental health challenges were particularly elevated in China, the USA, and Saudi Arabia. These elevated risks, perhaps not surprisingly, given that the novel and deadly outbreak began in China, were consistent with the findings of a recent umbrella review (Chirico et al., Citation2021). Although the relatively greater impacts in places like the USA and Saudi Arabia seem not yet well understood, we think that explanations probably lie withing the inequities and injustices of their health care structures and perhaps even their societies at large. Furthermore, perhaps the mere 10% elevation in nurses mental health symptoms, a non-significant trend, observed in Japan can be similarly explained. Such may belie its relative racialized homogeneity and health care system equity. Advancement of better between-country understandings remain for future research examination.
Implications for health care and future pandemic preparedness
The COVID-19 pandemic will undoubtedly have a lasting impact on health care workers and health care. Clearly it exposed gross racialized, gender and other inequities, not only among patients, but among and between health care providers. This study focused on a particularly vulnerable group, frontline hospital-based nurses, having indeed found their mental health to have suffered appreciably during the COVID-19 pandemic. Gratefully, their stories are beginning to be told through quantitative and qualitative study, and through exposing their unmet needs they have provided key suggestions relevant to future pandemic preparedness. Not surprisingly, as so many more patients required ICU care during the initial through early, pre-vaccine phases of the pandemic, many of the non-critical care nurses who willingly filled critical care nursing roles in much expanded ICUs felt ill-prepared and frightened (Hoogendoorn et al., Citation2021; Keene et al., Citation2021; Xu et al., Citation2021). Such newly recruited ICU nurses prevalently expressed the following themes that were robustly replicated with primary and quantitative research synthesis: they felt profoundly “stressed out,” lived in constant fear of cross-contamination and of infecting others, including their own family members, and they seemingly voiced their need for more specific training and greater support in the field (Perraud et al., Citation2022; Tang et al., Citation2021; Vera San Juan et al., Citation2022). Nursing schools and hospitals ought to proactively incorporate more such critical care training into the routine education and training of all professional nurses. Earlier experiences with the SARS outbreak clearly showed that where such additional training existed, deleterious mental health impacts were minimized among health care workers (Brooks et al., Citation2018).
As prevalently expressed by nurses themselves, more direct support is also needed in the field. By proactively providing excellent mental health supports we may at once prevent the prevalent development of mental disorders among nurses practicing in future pandemics and provide timely access to and effective treatment of those nurses who may be beginning to develop early symptoms of mental health disorders. We wonder if the profession of social work may not have something quite valuable to share with the nursing profession in this regard, that is, our seemingly much more entrenched commitment to self-care in practice (Ashley-Binge & Cousins, Citation2020; Collins, Citation2021; Elizabeth & Rassman, Citation2021; Sewell, Citation2018). For example, nursing decision makers might consider incorporating routine supportive supervision into their critical and acute care nursing programs, much like social work does especially in fields of practice where the risks of vicarious trauma are great. Numerous other well-developed supervisory techniques to support self-care and peer support might also be shared between the professions (McFadden et al., Citation2019; O’Donoghue & Tsui, Citation2015; Russ et al., Citation2020). Such we think would go a long way toward retaining a highly trained, skilled and healthy nursing workforce, capable of providing the highest quality health care, not only day to day, but also during future pandemics.
Limitations and future research needs
Primary studies needed to be longitudinal to be included in this meta-analysis. But, in fact, most of the 12 included studies used the most limited longitudinal designs. Seven were successive surveys that used different participant samples at baseline and follow-up, while four were surveys that used external comparison groups. None were prospective cohorts, the most confidence-inspiring longitudinal design. The retrospective, pseudo-longitudinal studies that seemed to have predominated this field, thus far, are indeed efficient designs that can be quite easy to employ, but they also are essentially correlational designs that can leave myriad potential confounds uncontrolled. Recall though that our central outcome of a two-fold increase in mental health symptoms among frontline, hospital-based nurses, was based upon the six strongest of the included studies. They all provided some measure of control for between two and five potential confounds through sample restriction and or regression modeling. We were, therefore, quite confident in their aggregate conclusion.
This rapid review has its own limitations in addition to those of the included primary studies. First, for its rapidity and practical, public health significance we admittedly focused upon the early, pre-vaccine phase of the COVID-19 pandemic, essentially its first year. We are comforted by the fact that longer cohorts are in process, but we would defend our decision to focus on this phase of the pandemic as we believe its knowledge advancement most relevant to future pandemic preparations. Second, as with all rapid reviews, this one was subject to certain fiscal, temporal and human constraints. Consequently, we could not follow every single Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendation (Kelly et al., Citation2016; Tricco et al., Citation2015). For our lack of library science, software and human resources, we were not blind to the primary studies’ findings, nor could we produce an unduplicated PRISMA diagram. However, each step of the review process, selection of studies, data extraction and meta-analysis was reliably cross-validated by at least two reviewers. Also, as our search strategies ultimately found very consistent support of the central hypothesis (11 of 12 primary studies) and none refuted it, in a quantitative sense we are confident that ‘theme saturation’ was reached. Therefore, we believe that despite its rapid nature, our review findings could be systematically replicated by a well-endowed, full systematic review. In fact, as suggested above, we believe that it should be.
Conclusion
Millions suffered and died during the COVID-19 pandemic, especially during its early pre-vaccination phase for our seeming profound lack of preparation. On the frontline, hospital-based nurses seemed at gravest risk. Tens of thousands died while providing critical care, while surviving nurses experienced large risks of developing anxiety, depression or PTSD. In retrospect, it seems that much of that suffering and many of those deaths could have been prevented. Necessary pandemic preparations are clear. We ought to work with our nursing and allied mental health colleagues, health care advocates and legislative decision-makers to make all of the necessary preparations to provide the highest quality health care, critical care if needed, immediately upon learning of any novel disease outbreak.
Acknowledgment
The authors are grateful for the research assistance of Nancy L. Richter, a research associate in the School of Social Work, University of Windsor.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Al Maqbali, M., Al Sinani, M., & Al-Lenjawi, B. (2021). Prevalence of stress, depression, anxiety and sleep disturbance among nurses during the COVID-19 pandemic: A systematic review and meta-analysis. Journal of Psychosomatic Research, 141, 110343. https://doi.org/10.1016/j.jpsychores.2020.110343
- American Psychiatric Association (APA). (2022). Diagnostic and statistical manual of mental disorders (5th ed., text revision). APA. https://doi.org/10.1176/appi.books.9780890425787
- Ashley-Binge, S., & Cousins, C. (2020). Individual and organisational practices addressing social workers’ experiences of vicarious trauma. Practice, 32(3), 191–207. https://doi.org/10.1080/09503153.2019.1620201
- Borenstein, M., Hedges, L., Higgins, J., & Rothstein, H. (2013). Comprehensive meta-analysis, version 3 [Computer software]. Biostat.
- Brooks, S. K., Dunn, R., Amlôt, R., Rubin, G. J., & Greenberg, N. (2018). A systematic, thematic review of social and occupational factors associated with psychological outcomes in healthcare employees during an infectious disease outbreak. Journal of Occupational and Environmental Medicine, 60(3), 248–257. https://doi.org/10.1097/JOM.0000000000001235
- Chirico, F., Ferrari, G., Nucera, G., Szaroak, L., Crescenzo, P., & Ilesanmi, O. (2021). Prevalence of anxiety, depression, burnout syndrome, and mental health disorders among healthcare workers during the COVID-19 pandemic: A rapid umbrella review of systematic reviews. Journal of Health and Social Sciences, 6(2), 209–220.
- Collins, S. (2021). Social workers and self-care: A promoted yet unexamined concept? Practice, 33(2), 87–102. https://doi.org/10.1080/09503153.2019.1709635
- Cooper, H. M. (2017). Research synthesis and meta-analysis: A step-by-step approach (5th ed.). Sage.
- Deeks, J. J., Higgins, J. P. T., & Altman, D. G. (2021). Analysing data and undertaking meta-analyses. In J. P. T. Higgins, J. Thomas, J. Chandler, M. Cumpston, T. Li, M. J. Page, & V. A. Welch (Eds.), Cochrane handbook for systematic reviews of interventions, version 6.2 (Chapter 10). The Cochrane Collaboration. https://www.training.cochrane.org/handbook.
- de Smidt, G. A., & Gorey, K. M. (1997). Unpublished social work research: Systematic replication of a recent meta-analysis of published intervention effectiveness research. Social Work Research, 21(1), 58–62. https://doi.org/10.1093/swr/21.1.58
- *Duru, H. (2022). The continuing effect of COVID-19 pandemic on physical well-being and mental health of ICU healthcare workers in Turkey: A single-centre cross-sectional later-phase study. Journal of Intensive Care Medicine, 37(9), 1206–1214. https://doi.org/10.1177/08850666211070740
- Elizabeth, W. R., & Rassman, A. (2021). cAIR: Implementation of peer response support for frontline health care workers facing the COVID-19 pandemic. Social Work in Health Care, 60(2), 177–186. https://doi.org/10.1080/00981389.2021.1904321
- Fleiss, J. L., Levin, B., & Paik, M. C. (2003). Statistical methods for rates and proportions (3rd ed.). Wiley.
- Ganann, R., Ciliska, D., & Thomas, H. (2010). Expediting systematic reviews: Methods and implications of rapid reviews. Implementation Science, 5(1), 56. https://doi.org/10.1186/1748-5908-5-56
- Greenland, S. (1987). Quantitative methods in the review of epidemiologic literature. Epidemiologic Reviews, 9(1), 1–30. https://doi.org/10.1093/oxfordjournals.epirev.a036298
- Greenland, S. (1998). Meta-analysis. In K. J. Rothman & S. Greenland (Eds.), Modern epidemiology (2nd ed., pp. 643–673). Lippincott-Raven.
- Grenier, A. M., & Gorey, K. M. (1998). Effectiveness of social work with older people and their families: A meta-analysis of conference proceedings. Social Work Research, 22(1), 60–64. https://doi.org/10.1093/swr/22.1.60
- *Harry, S. (2021). Predictors of burnout for frontline nurses in the COVID-19 pandemic: Well-being, satisfaction with life, social support, fear, work setting factors, psychological impacts, and self-efficacy for nursing tasks (Publication No. 28498893) [Doctoral dissertation]. Columbia University. ProQuest Dissertations & Theses Global.
- *Havaei, F., Smith, P., Oudyk, J., & Potter, G. G. (2021). The impact of the COVID-19 pandemic on mental health of nurses in British Columbia, Canada using trends analysis across three time points. Annals of Epidemiology, 62, 7–12. https://doi.org/10.1016/j.annepidem.2021.05.004
- Havaei, F., Tang, X., Smith, P., Boamah, S. A., & Frankfurter, C. (2022). The association between mental health symptoms and quality and safety of patient care before and during COVID-19 among Canadian nurses. Healthcare (Basel, Switzerland), 10(2), 314. https://doi.org/10.3390/healthcare10020314
- Hoogendoorn, M. E., Brinkman, S., Bosman, R. J., Haringman, J., de Keizer, N. F., & Spijkstra, J. J. (2021). The impact of COVID-19 on nursing workload and planning of nursing staff on the intensive care: A prospective descriptive multicenter study. International Journal of Nursing Studies, 121, 104005. https://doi.org/10.1016/j.ijnurstu.2021.104005
- *Katsuta, N., Ito, K., Fukuda, H., Seyama, K., Hori, S., Shida, Y., Nagura, R., Nojiri, S., & Sato, H. (2021). Elevated depressive symptoms among newer and younger healthcare workers in Japan during the COVID-19 pandemic. Neuropsychopharmacology Reports, 41(4), 544–547. https://doi.org/10.1002/npr2.12217
- Keene, A. B., Shiloh, A. L., Eisen, L., Berger, J., Karwa, M., Fein, D., Orsi, D., & Gong, M. (2021). Critical care surge during the COVID-19 pandemic: Implementation and feedback from frontline providers. Journal of Intensive Care Medicine, 36(2), 233–240. https://doi.org/10.1177/0885066620973175
- Kelly, S. E., Moher, D., & Clifford, T. J. (2016). Quality of conduct and reporting in rapid reviews: An exploration of compliance with PRISMA and AMSTAR guidelines. Systematic Reviews, 5(1), 79. https://doi.org/10.1186/s13643-016-0258-9
- Lee, S. M., Kang, W. S., Cho, A. R., Kim, T., & Park, J. K. (2018). Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Comprehensive Psychiatry, 87, 123–127. https://doi.org/10.1016/j.comppsych.2018.10.003
- *Li, J., Su, Q., Li, X., Peng, Y., & Liu, Y. (2021a). COVID-19 negatively impacts on psychological and somatic status in frontline nurses. Journal of Affective Disorders, 294, 279–285. https://doi.org/10.1016/j.jad.2021.07.031
- *Li, X., Zhou, Y., & Xu, X. (2021b). Factors associated with the psychological well-being among front-line nurses exposed to COVID-2019 in China: A predictive study. Journal of Nursing Management, 29(2), 240–249. https://doi.org/10.1111/jonm.13146
- Magnavita, N., Chirico, F., Garbarino, S., Bragazzi, N. L., Santacroce, E., & Zaffina, S. (2021). SARS/MERS/SARS-CoV-2 outbreaks and burnout syndrome among healthcare workers. An umbrella systematic review. International Journal of Environmental Research and Public Health, 18(8), 4361. https://doi.org/10.3390/ijerph18084361
- McFadden, P., Campbell, A., & Taylor, B. (2019). Resilience and burnout in child protection social work: Individual and organisational themes from a systematic literature review. British Journal of Social Work, 45(5), 1546–1563. https://doi.org/10.1093/bjsw/bct210
- Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. British Medical Journal, 339, b2535.
- *Obeidat, N. A., Dodin, Y. I., Hawari, F. I., Albtoosh, A. S., Manasrah, R. M., & Mansour, A. H. (2022). Mitigating psychological distress in healthcare workers as COVID-19 waves ensue: A repeated cross-sectional study from Jordan. Human Resources for Health, 20(1), 32. https://doi.org/10.1186/s12960-022-00728-x
- O’Donoghue, K., & Tsui, M. (2015). Social work supervision research (1970–2010): The way we were and the way ahead. British Journal of Social Work, 45(2), 616–633. https://doi.org/10.1093/bjsw/bct115
- *Oosthuizen, S., Bergh, A.-M., Silver, A., Malatji, R., Mfolo, V., & Botha, T. (2022). Maternity healthcare providers’ self-perceptions of well-being during COVID-19: A survey in Tshwane Health District, South Africa. African Journal of Primary Health Care & Family Medicine, 14(1), e1–e10. https://doi.org/10.4102/phcfm.v14i1.3034
- Perraud, F., Ecarnot, F., Loiseau, M., Laurent, A., Fournier, A., Lheureux, F., Binquet, C., Rigaud, J.-P., Meunier-Beillard, N., & Quenot, J.-P. (2022). A qualitative study of reinforcement workers’ perceptions and experiences of working in intensive care during the COVID-19 pandemic: A PsyCOVID-ICU substudy. PloS One, 17(3), e0264287. https://doi.org/10.1371/journal.pone.0264287
- *Ren, H., Luo, X., Wang, Y., Guo, X., Hou, H., Zhang, Y., Yang, P., Zhu, F., Hu, C., Wang, R., Sun, Y., Du, Y., Yin, Q., Xu, G., Zuo, H., Hu, Q., & Wang, Y. (2021). Psychological responses among nurses caring for patients with COVID-19: A comparative study in China. Translational Psychiatry, 11(1), 273. https://doi.org/10.1038/s41398-020-00993-1
- *Reverté-Villarroya, S., Ortega, L., Lavedán, A., Masot, O., Burjalés-Martí, M. D., Ballester-Ferrando, D., Fuentes-Pumarola, C., & Botigué, T. (2021). The influence of COVID-19 on the mental health of final-year nursing students: Comparing the situation before and during the pandemic. International Journal of Mental Health Nursing, 30(3), 694–702. https://doi.org/10.1111/inm.12827
- Robinson, E., Sutin, A. R., Daly, M., & Jones, A. (2022). A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID- 19 pandemic in 2020. Journal of Affective Disorders, 296, 567–576. https://doi.org/10.1016/j.jad.2021.09.098
- Russ, E., Lonne, B., & Lynch, D. (2020). Increasing child protection workforce retention through promoting a relational-reflective framework for resilience. Child Abuse & Neglect, 110(Pt 3), 104245. https://doi.org/10.1016/j.chiabu.2019.104245
- Sewell, K. M. (2018). Social work supervision of staff: A primer and scoping review (2013–2017). Clinical Social Work Journal, 46(4), 252–265. https://doi.org/10.1007/s10615-018-0679-0
- Ślusarska, B., Nowicki, G. J., Niedorys-Karczmarczyk, B., & Chrzan-Rodak, A. (2022). Prevalence of depression and anxiety in nurses during the first eleven months of the COVID-19 pandemic: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health, 19(3), 1154. https://doi.org/10.3390/ijerph19031154
- Stroup, D. F., Berlin, J. A., Morton, S. C., Olkin, I., Williamson, G. D., Rennie, D., Moher, D., Becker, B. J., Sipe, T. A., & Thacker, S. B. (2000). Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. Journal of the American Medical Association, 283(15), 2008–2012.
- Sullivan, G. M. (2011). IRB 101. Journal of Graduate Medical Education, 3(1), 5–6. https://doi.org/10.4300/JGME-D-11-00005.1
- Tang, C. J., Lin, Y. P., & Chan, E.-Y. (2021). ‘From expert to novice’, perceptions of general ward nurses on deployment to outbreak intensive care units during the COVID-19 pandemic: A qualitative descriptive study. Journal of Clinical Nursing, 00, 1–13. https://doi.org/10.1111/jocn.16029
- *Temsah, M. H., Al Huzaimi, A., Alrabiaah, A., Alamro, N., Al-Sohime, F., Al-Eyadhy, A., Alhasan, K., Kari, J. A., Alhaboob, A., Alsalmi, A., AlMuhanna, W., Almaghlouth, I., Aljamaan, F., Halwani, R., Saddik, B., Barry, M., Al-Zamil, F., AlHadi, A. N., Al-Subaie, S., Jamal, A., & Somily, A. M. (2021). Changes in healthcare workers’ knowledge, attitudes, practices, and stress during the COVID-19 pandemic. Medicine, 100(18), e25825. https://doi.org/10.1097/MD.0000000000025825
- Tricco, A. C., Antony, J., Zarin, W., Strifler, L., Ghassemi, M., Ivory, J., Perrier, L., Hutton, B., Moher, D., & Straus, S. E. (2015). A scoping review of rapid review methods. BMC Medicine, 13(1), 224. https://doi.org/10.1186/s12916-015-0465-6
- Trudgill, D. I. N., Gorey, K. M., & Donnelly, E. A. (2020). Prevalent posttraumatic stress disorder among emergency department personnel: Rapid systematic review. Humanities & Social Sciences Communications, 7, 89.
- United Nations (UN). (2023, May 5). WHO chief declares end to COVID-19 as a global health emergency. UN News. https://news.un.org/en/story/2023/05/1136367
- Varghese, A., George, G., Kondaguli, S. V., Naser, A. Y., Khakha, D. C., & Chatterji, R. (2021). Decline in the mental health of nurses across the globe during COVID-19: A systematic review and meta-analysis. Journal of Global Health, 11, 05009. https://doi.org/10.7189/jogh.11.05009
- Vera San Juan, N., Clark, S. E., Camilleri, M., Jeans, J. P., Monkhouse, A., Chisnall, G., & Vindrola-Padros, C. (2022). Training and redeployment of healthcare workers to intensive care units (ICUs) during the COVID-19 pandemic: A systematic review. BMJ Open, 12(1), e050038. https://doi.org/10.1136/bmjopen-2021-050038
- World Health Organization (WHO). (2020). WHO Director-General’s opening remarks at the media briefing on COVID-19. https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19–-11-march-2020
- World Health Organization (WHO). (2021). Health and care worker deaths during COVID-19. https://www.who.int/news/item/20-10-2021-health-and-care-worker-deaths-during-covid-19
- World Health Organization (WHO). (2022). COVID-19 pandemic triggers 25% increase in prevalence of anxiety and depression worldwide. https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide
- World Health Organization (WHO). (2023). WHO coronavirus (COVID-19) dashboard. Retrieved May 2, 2024, from https://covid19.who.int
- Xu, H., Stjernswärd, S., & Glasdam, S. (2021). Psychological experiences of frontline nurses working in hospital-based settings during the COVID-19 pandemic – a qualitative systematic review. International Journal of Nursing Studies Advances, 3, 100037. https://doi.org/10.1016/j.ijnsa.2021.100037
- *Zakeri, M. A., Rahiminezhad, E., Salehi, F., Ganjeh, H., & Dehghan, M. (2021). Burnout, anxiety, stress, and depression among Iranian nurses: Before and during the first wave of the COVID-19 pandemic. Frontiers in Psychology, 12, 789737. https://doi.org/10.3389/fpsyg.2021.789737
