
ABSTRACT
In the U.S., sexual minority men (SMM) are disproportionately affected by HIV. Interventions are needed to increase HIV prevention and treatment behaviors, especially among syndemically exposed SMM. In recent years, researchers have created and tested combination behavioral interventions co-targeting syndemics and HIV-related health behaviors. We evaluated that literature via systematic review and meta-analysis, identifying 44 trials targeting mental health symptoms, alcohol use, and drug use, as well as sexual risk behavior, antiretroviral adherence, and healthcare engagement. For the randomized controlled trials, we computed between-group, pre-post effect sizes and tested them via random-effects models. Results supported the efficacy of combined interventions with significant, small, positive effects for improving mental health and reducing substance use (d = .20, CIs: 0.12, .29), and reducing sexual risk behavior and improving antiretroviral adherence (d = .16, CIs: .03, .30). Stratification analyses indicate that longer (9+ sessions) and individual (vs. group) interventions resulted in stronger effects on syndemic but not health behavior outcomes. Intervention developers should attend to intervention intensity and format. More evidence is needed about the importance of additional factors, such as novel intervention targets and cultural tailoring, as well as broadening the focus to multi-level interventions to address both interpersonal and structural mechanisms of change.
HIV-Related Health Behaviors
A growing body of research describes the domains of HIV-related health behaviors that serve as intervention targets for people with HIV (PWH) or those at high risk for acquiring the virus. These targets, known as the HIV treatment cascade, describe the junctures at which an individual engages with relevant health behaviors or the healthcare system (Nunn et al., Citation2017; Risher, Mayer, & Beyrer, Citation2015). The early stages include HIV testing and referral to follow-up healthcare based on HIV status (DiNenno et al., Citation2017). For HIV-negative individuals at high-risk of HIV acquisition, health education should ensure accurate understanding of the level of risk associated with their behavior (Centers for Disease Control and Prevention [CDC], Citation2015) and, for eligible individuals, pre-exposure prophylaxis (PrEP) medications can significantly reduce HIV acquisition risk by providing a pharmacologic barrier to HIV infection that is highly effective when taken as prescribed (CDC, Citation2018f). For PWH, the ensuing steps are linkage to medical care, retention in ongoing care, being prescribed antiretroviral medications (ARVs), and maintaining sufficiently high levels of ARV adherence to attain viral suppression. Achieving an undetectable viral load (VL) is crucial to optimizing the health of PWH (CDC, Citation2017b) and halting HIV transmission. In recent years, given the strength of findings that “undetectable equals untransmittable” (Cohen et al., Citation2011), reducing viral load via ARVs has been a major HIV prevention initiative of the U.S. CDC (“U = U taking off,” Citation2017).
Improving HIV-Related Health Behaviors with Behavioral Interventions
Since the early days of the epidemic, researchers and clinicians have worked to develop HIV prevention and treatment interventions. In the U.S., the most common mode of HIV transmission is through sexual behavior (CDC, Citation2018e) and, until the rise of PrEP, interventions focused on reducing sexual transmission of HIV have primarily used behavioral strategies (CDC, Citation2018a). Behavioral HIV prevention interventions include those focused on increasing HIV testing (Suthar et al., Citation2013) and, more recently, on increasing PrEP knowledge, prescriptions, and adherence of prospective PrEP-takers (Refugio et al., Citation2019) and providers (Silapaswan, Krakower, & Mayer, Citation2017). Likely the most common type of behavioral HIV prevention interventions, though, are those to increase condom use during anal or vaginal sex. Behavioral sexual risk reduction interventions have been developed both for primary prevention, targeting HIV-negative individuals (Sullivan et al., Citation2012), and secondary prevention, targeting HIV-positive individuals (Crepaz et al., Citation2014). Behavioral HIV treatment interventions include those attempting to increase engagement with care, such as through the provision of peer health navigators (Maulsby et al., Citation2015), as well as to support ARV adherence and persistence (Kanters et al., Citation2017). This latter category has been an especially prolific area of behavioral intervention research, given the high levels of medication adherence needed to maintain virologic control (>75% of prescribed doses, depending on regimen; Byrd et al., Citation2019) and the indefinite treatment duration (Günthard et al., Citation2016). Hundreds of behavioral interventions have been developed and evaluated to improve HIV-related health behaviors (Albarracin et al., Citation2005). A major open question in the field is “what works for whom?” Despite the development and success of many prevention and treatment interventions, gaining greater understanding of which HIV-related interventions might be most beneficial is critical to reducing the number of new infections.
Sexual Minority Men Remain at High Risk for HIV
Although many consider HIV to be “a plague of the past,” the virus has continued to spread – despite numerous advances in HIV prevention and treatment – and it disproportionately affects vulnerable groups, such that more than two-thirds of new infections occur among people who are economically disenfranchised or ethnic, racial, or sexual minorities (El-Sadr, Mayer, Rabkin, & Hodder, Citation2019, p. 1). Over one million people are living with HIV in the U.S. today, and there are around 40,000 new infections annually, according to U.S. surveillance data (CDC, Citation2018b). Men who have sex with men (MSM) have had the highest HIV incidence (68% of new infections) and prevalence (71% of total infections) since HIV was identified in 1981 (CDC, Citation1981; Centers for Disease Control and Prevention, Citation2018b). The vast majority of those MSM have a non-heterosexual sexual orientation, making them sexual minority men (SMM) in terms of their identities as well as their behavior. Rates of new infections have been particularly high among vulnerable subgroups of SMM, including young (CDC, Citation2018d) and Black and Latino (Hess, Hu, Lansky, Mermin, & Hall, Citation2017) SMM. Stigma, as well as social and structural determinants of health, play central roles in the burden of HIV in SMM, in addition to the high per-act transmission probability of receptive anal intercourse and strong clustering of HIV within SMM social-sexual networks (Beyrer et al., Citation2013; Earnshaw, Bogart, Dovidio, & Williams, Citation2013). As many as 80% of new infections are due to condomless sex with partners who are newly infected yet unaware of their status (Li, Purcell, Sansom, Hayes, & Hall, Citation2019). Thus, although options for reducing the spread of HIV and improving the health of PWH, even the most efficacious interventions do not work for all at-risk individuals, including SMM.
SMM HIV Disparities Driven by Psychosocial Syndemics
In addition to the factors mentioned above, there are individual-level experiences that serve as risk factors for engagement in HIV risk behaviors and disengagement from HIV care. Epidemiologic studies have demonstrated that sexual minority individuals are at increased risk for mental health problems, likely due to the added stress experienced by living in a society that is disapproving and sometimes hostile about their identities (Meyer, Citation2003; Pachankis, Cochran, & Mays, Citation2015; Plöderl & Tremblay, Citation2015). These psychosocial challenges co-occur and interact to impact SMM’s HIV-related health behaviors and have been termed syndemics in the literature – referring to the synergy created by multiple epidemics. Syndemics represent “mutually reinforcing epidemics fueled by cultural marginalization that create collectively a greater impact on a person’s or community’s health profile than any single epidemic on its own” (Halkitis, Wolitski, & Millett, Citation2013, p. 266). Singer (Citation1996) first coined the term to describe a cluster of psychosocial factors that influence health behaviors and health status. However, the first syndemic he proposed was SAVA – substance abuse, violence, and AIDS. Later, a seminal paper by Stall et al. (Citation2003) brought syndemics into the mainstream of behavioral HIV research. In this paper, the additive effect of various syndemic indicators significantly predicted HIV risk behaviors as well as HIV-positive status in a mixed serostatus sample of nearly 2,900 SMM (Stall et al., Citation2003).
Stall and colleagues expanded on the SAVA syndemic by operationalizing violence as including both childhood sexual abuse (CSA) and partner abuse, and by including mental health symptoms. Thus, these four categories of individual-level health problems – childhood sexual abuse, partner abuse, mental health symptoms, and drug and alcohol use – have been vigorously investigated in SMM, and have been shown to have strong associations with HIV risk behaviors, HIV serostatus, and higher healthcare utilization and medical costs in a variety of HIV-negative SMM subgroups (e.g., O’Cleirigh et al., Citation2018; Tsai & Burns, Citation2015). Fewer studies have focused on syndemics in HIV-positive SMM. This discrepancy is surprising since syndemic indicators remain after HIV infection, and they are no less likely to continue to exert an influence on men’s functioning, potentially impacting medication adherence or engagement with care. Indeed, in samples of HIV-positive SMM, syndemics have been associated with ARV non-adherence and medical hospitalization, among other outcomes (e.g., Pantalone, Valentine, Woodward, & O’Cleirigh, Citation2018). The importance of syndemics as an organizing principle in behavioral HIV research cannot be overstated. The data clearly implicate syndemics as a key driver of poorer HIV-related health outcomes within SMM. Thus, a comprehensive approach to ameliorating the impact of HIV on SMM must necessarily address syndemic factors.
Psychosocial Syndemics Impact Health Behavior Change Intervention Efficacy
Given that SMM have heightened risk compared to their heterosexual peers for both HIV and syndemic indicators, SMM would likely derive substantial benefit from evidence-based interventions that address both categories. The contribution of syndemic factors to HIV sexual risk among SMM may help to explain, at least in part, the variable effectiveness of behavioral HIV prevention and treatment interventions. Typically, HIV-related health behavior interventions are short and focused on improving the behavior without addressing syndemic factors that serve as barriers to behavior change, such as mental health and substance use. Following a kind of rational actor assumption (Avorn, Citation2018), many interventions aim to address the health behavior target with a minimum of additional content, based on the assumption that the participant already possesses some combination of the requisite knowledge, motivation, and skills needed to change their behavior. The goal of the intervention is to bolster whatever is lacking. This design enables scalability but may be reductive – in that it implies that a minimal intervention is all that is needed while potentially failing to provide requisite help for interrelated challenges affecting a significant portion of the population of interest.
For many SMM, especially those with syndemic exposure, successful health behavior change interventions may need to address those syndemic factors concurrently, and in the context of the health behavior change efforts. One example about the need to address syndemics to improve health behavior intervention uptake comes from the EXPLORE study, a major U.S. behavioral HIV prevention trial for HIV-negative SMM (Mimiaga et al., Citation2009). Of the 4,295 enrolled participants, two-fifths reported a history of CSA and that group was at increased risk of endorsing condomless anal sex (CAS) as well as seroconversion. Further, among participants reporting CSA, the intervention showed no effect in reducing HIV infection rates compared to modest reductions in HIV risk in the sample overall. In a follow-up to that work, O’Cleirigh et al. (Citation2019) created and tested an HIV prevention intervention for HIV-negative SMM with histories of CSA. The intervention, called THRIVE, simultaneously targets post-trauma cognitions using a standard evidence-based psychological approach alongside gold standard sexual risk reduction techniques. Results indicate significant improvements in both mental health symptoms and sexual risk behavior over and above sexual risk reduction counseling alone.
Historically, behavioral interventions to address HIV-related health behaviors and those to address mental health symptoms typically have been developed separately, by different groups of investigators, and in different settings. This siloed approach to intervention development, although understandable given the organization of the field, hinders rather than facilitates progress. Indeed, in the past decade especially, more and more scholars have highlighted the need to marry those categories of intervention targets into a single package (e.g., Carrico, Zepf, Meanley, Batchelder, & Stall, Citation2016; Mimiaga et al., Citation2015; Sikkema et al., Citation2010). Halkitis et al. (Citation2013) wrote that, “in order to be maximally effective, both HIV prevention and HIV care must be delivered holistically, such that sexual risk behaviors are addressed in relation to, and in sync with, the drug use and mental health of the individual” (p. 662). Safren, Blashill, and O’Cleirigh (Citation2011) noted that “comorbid mental health problems may compromise the impact of traditional prevention programs, overwhelming existing theory driven models” (p. 30).
To better understand the state of interventions co-targeting interrelated syndemic challenges and HIV-related health behaviors of SMM with HIV or at high risk of acquiring it, we conducted a systematic review and meta-analysis, following the procedures for systematic review and meta-analysis as described in the PRISMA guidelines (Liberati et al., Citation2009).
Method
Study Selection Criteria
Study Participants
We included studies enrolling SMM, cisgender, or transgender, including those who explicitly identified with a non-heterosexual sexual orientation and other men who have sex with men. We included studies enrolling samples of non-sexual minority (i.e., heterosexual) participants if at least 50% of the analytic sample was identified as SMM, or if there were sufficient data reported in the article on a discernable SMM subsample. Samples of all HIV statuses were included. Given the transmission dynamics and cultural mores related to sexual minority men vary widely (e.g., Beyrer et al., Citation2010), we focused our search on trials conducted in North America (Canada, U.S., Mexico) and Western Europe (Belgium, France, Ireland, Luxembourg, Netherlands, Portugal, Spain, United Kingdom) because of similarities in the epidemic in those areas.
Behavioral Interventions
For inclusion, trials must have used a controlled (RCT) or uncontrolled (pilot) study design to evaluate a behavioral intervention. Studies solely examining pharmacologic treatments were excluded. All behavioral intervention modes (e.g., individual, couple, group) and delivery formats (e.g., in person, telephone, mobile app) were eligible.
Primary and Secondary Outcomes
Studies must have tested an intervention that aimed to improve functioning on two or more targets, including at least one syndemic indicator and at least one HIV-related health behavior. Outcome assessment consisted of both objective and subjective methods of evaluation, including self-report, clinical assessment, and biological specimens. For the syndemics, although we searched for any of the four potential syndemic indicators, we only discovered interventions focused primarily on mental health and substance use, including alcohol and drug use. In terms of health behaviors, we included in our search HIV biomarkers that serve as proxy for health behaviors (i.e., undetectable viral load serves as a proxy for strong ARV adherence) when those were reported.
Search Strategy
Our search focused on articles published from 2000 through May 2019. Based on our collective linguistic capabilities, only English-language peer-reviewed articles were screened. We employed systematic search strategies consisting of three steps. First, we conducted a thorough literature review using online databases. We searched the databases we judged to have the highest likelihood of indexing relevant articles, including Academic Search Complete, CINAHL, MedLine, PsycInfo, and PubMed. We used the following Boolean search terms: (MSM OR “men who have sex with men” OR “sexual minority men” OR “homosexual” OR “bisexual” OR “gay”) AND HIV AND Intervention AND (“Condomless anal sex” OR “condomless sex” OR “unprotected anal intercourse” OR “unprotected sex” OR “sexual risk behavior” OR “Pre-exposure prophylaxis” OR “Post-Exposure Prophylaxis” OR ARV OR adherence OR “treatment cascade” OR “HIV testing” OR “healthcare engagement” OR “viral load” OR “HIV care indicator” OR “CD4 count”) AND (“mental health” OR depression OR anxiety OR PTSD OR “post-traumatic stress disorder” OR “posttraumatic stress disorder” OR “childhood sexual abuse” OR “partner abuse” OR “substance use” OR “substance abuse” OR “alcohol use” OR “alcohol abuse” OR “drug use” OR “drug abuse”). Second, we reached out to experts in the field for published articles, articles in press, and recommendations for potentially eligible articles. We sent e-mails describing our eligibility criteria to various HIV and health psychology listservs as well as intervention researchers in our own professional networks. Finally, we systematically reviewed the reference lists of the full-text articles that we assessed for eligibility and relevant review articles for additional sources.
Data Extraction
All authors, with the help of research assistants on the team, contributed to the data extraction process. Identified articles with the potential to meet inclusion criteria through abstract review were evaluated for eligibility. In this process, authors reviewed the full-text articles to make an eligibility determination using a standardized data extraction template. Extracted data comprised study design, participant demographics, recruitment procedures, trial inclusion/exclusion criteria, description of the behavioral intervention, retention data, and outcome data for both the syndemic indicators and the health behaviors. Additionally, to evaluate methodological rigor, we assessed each article’s risk of bias using the Cochrane Collaboration’s tool (Higgins & Green, Citation2011). Relevant data included random sequence generation, concealment of allocation, selective reporting, blinding, and incomplete outcome reporting.
Effect Size Calculations
Using Microsoft Excel, we calculated effect sizes as Cohen’s d, the standardized mean difference between the intervention and control groups for each outcome variable, regardless of how it was measured (Cohen, Citation1988). A positive d indicates a favorable outcome for the intervention group relative to the control group. If authors presented odds ratios, we converted them into Cohen’s d using the procedures outlined by Chinn (Citation2000), and calculated confidence intervals according to the recommendations from Hedges and Olkin (Citation2014). If authors presented effect sizes as part of their results, for consistency, we re-calculated them from the available data and compared our calculation to their reports (note that we identified no discrepancies).
Our aim was to make conservative analytic decisions to minimize the potential that we would overestimate intervention effects. Thus, we report effect sizes only for the most distal assessment point for each trial, as this represents the most valid indicator of treatment efficacy. Further, due to disagreement about the level of bias inherent in within-group, pre-post intervention comparisons (i.e., the lack of independence in scores; Cuijpers, Weitz, Cristea, & Twisk, Citation2017), we have chosen to present effect sizes for between-group comparisons only.
Meta-Analytic Methods
Determining Effect Sizes for Inclusion
In the meta-analyses, we included only studies testing the efficacy of intervention effects on mental health and health behaviors as primary aims. Thus, we removed the studies by Carrico et al. (Citation2015a; Citation2015b) because the primary intervention outcomes of those studies were feasibility/acceptability. Further, in keeping with our goal of presenting conservative efficacy estimates, we developed a number of decision-rules such that each trial contributed only one effect size per outcome variable within each of the five categories of mental health problems, alcohol use, drug use, sexual risk behavior, and ARV adherence. For example, if a study in the Mental Health category aimed to reduce both depression and anxiety symptoms, we included one effect size for the intervention’s effects on depression, despite there being multiple depression variables reported and analyzed in the paper, alongside one effect size for the intervention’s effects on anxiety, despite the potential for multiple anxiety variables measured and analyzed. These decision rules helped to decrease the potential for any individual trial to disproportionately influence the results.
Overall, if a study contributed both the full scale of a measure as well as subscales or individual items, we used the effect size associated with the full-scale measure, because it contributed more information about the variable of interest. If a study included both a self-report measure and a clinician-administered measure of the same construct, we retained the effect size associated with the clinician-administered measure (e.g., BDI vs. MADRS) because of presumed greater validity. For the syndemic indicators, if there were two measures of a given syndemic indicator, and both were self-reported scales with established psychometric properties, we retained the effect size associated with the measure that was more commonly represented within the interventions we evaluated, to enhance comparability. For the health behaviors, if there was a choice to be made between a biomarker (e.g., viral load) and a self-report measure (e.g., adherence), we retained the biomarker because of the increased validity associated with objective measures. When there were multiple formats of biomarker – continuous viral load vs. dichotomous undetectable viral load – we chose the continuous variable because it contributed more nuanced information. Similarly, we construed this rule to include the effect size associated with a more general (e.g., day-level adherence) vs. narrower (e.g., on-time dose adherence) measure. For measures of HIV sexual risk behavior, specifically, our choices were guided by a desire for maximal specificity and to capture the highest risk behaviors. Thus, we retained the effect size associated with event-level behaviors over sexual risk constructs (e.g., CAS over condom use self-efficacy), individual-level behaviors versus summaries of group behavior, serodiscordant CAS versus CAS with partners of any serostatus, and receptive CAS over insertive CAS in studies enrolling HIV-negative participants.
Conducting the Meta-analyses
We exported the effect sizes from Excel into the Comprehensive Meta-Analysis software (https://www.meta-analysis.com/). We conducted meta-analyses using random effects models to compute the pooled estimates for the trials, given the high degree of heterogeneity between studies (Viechtbauer, Citation2007). A random-effects model provides a more conservative estimate of variance and generates more accurate inferences about a population of trials beyond the set of trials included in this review (Hedges & Vevea, Citation1998). We conducted six meta-analyses, including one for each of the superordinate categories of outcomes, (1) syndemics and (2) HIV-related health behaviors, as well as one for each of the sub-categories of variables comprising those categories: the syndemics (3) mental health and (4) substance use, which is a combination of trials focused on alcohol and drug use, and the health behaviors (5) ARV adherence and (6) sexual risk. In the results of the systematic review, we report separately on interventions focusing on alcohol and drug use. However, there were too few trials for alcohol (n = 5) and drug use (n = 8) to evaluate them separately in quantitative analyses.
We selected several stratification (moderator) variables and tested them using a fully random effects analysis. We aimed to balance our selection of the number of stratification variables against the number of included trials, which limited power. The stratification variables we selected were the length of the post-intervention follow-up period; the number of intervention sessions; the format of the intervention as individual- or group-based; and whether or not the intervention was culturally tailored for the population under study. We chose the stratification variables a priori; some of the ways we operationalized the variable levels were straightforward (e.g., individual vs. group format) but others were defined post hoc based on the observed distribution informed by the results of the systematic review (e.g., 1–8 sessions vs. 9 or more).
We evaluated publication bias that would favor trials with significant findings. For each meta-analysis and each stratification analysis, we inspected the funnel plot. However, because graphical evaluation can be subjective, we also calculated Egger’s test (Egger, Smith, Schneider, & Minder, Citation1997), Duval and Tweedie (Citation2000) “Trim and Fill,” and Orwin’s (Citation1983) fail-safe N for both primary analyses – grouping together all of the syndemic outcomes and then grouping together all of the health behavior outcomes.
Results
Overview of Included Vs. Excluded Articles
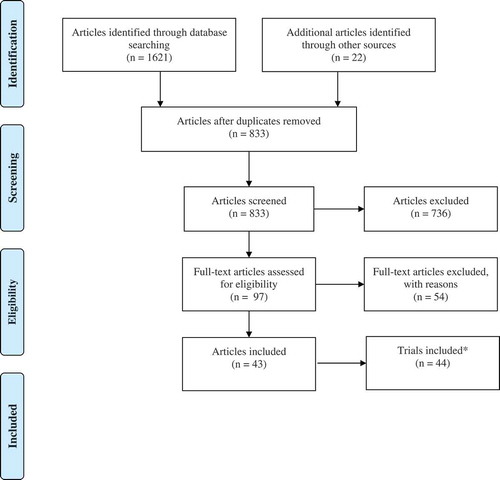
As seen in the flow diagram (), we identified 1,621 articles electronically, and 22 articles through the other methods (e.g., e-mails to listservs, review of citations in included articles). After removing duplicates, authors screened an initial group of 833 articles based on the title and abstract. Of those articles, 736 were excluded upon review of the abstract. Typically, ineligible articles did not report testing behavioral interventions; no reports of combination behavioral interventions were excluded based on geographical location alone. For the remaining 97 articles, we assessed their eligibility through a review of the full-text article. During the second round of review, one author independently reviewed each full-text article to determine the reliability of our eligibility assessment procedures (kappa = 0.89, CIs: 0.80, 0.98). We resolved discrepancies through discussion among all authors. This process resulted in the inclusion of 43 articles, which represent 44 intervention trials; the paper by Carrico et al. (Citation2014) presented two trials in a single article. The trials, which report collectively on the results of interventions with 7,156 participants, are described in .
Table 1. Intervention trials included in the systematic review (N = 44).
Figure 1. PRISMA flow diagram.
Included Trials
The 44 included trials were published between 2001–2019. Thirty-three distinct interventions (some trials presented the same or an adapted intervention with a different sample) were tested. Most of the intervention trials were based in the U.S. (n = 41, 93%). Others were conducted in Canada (n = 2, 5%) and Switzerland (n = 1, 2%). The majority of the trials were limited to SMM (n = 36, 82%), whereas the remaining one-fifth also included members of other HIV risk populations (e.g., women, heterosexual men; n = 8, 18%).
Within the included trials, interventions targeted three syndemic indicators: (1) mental health (n = 24, 55%), (2) alcohol use (n = 19, 43%), and (3) drug use (n = 24, 55%). Fifteen (34%) trials focused solely on mental health. Five (11%) trials focused solely on alcohol use. Seven (16%) trials focused solely on drug use. Eight (18%) trials addressed both drug and alcohol use. Five (11%) trials addressed drug use and mental health. One (2%) trial addressed alcohol use and mental health. Four (9%) trials addressed all three syndemic indicators.
There were three health behavior outcomes in the trials: (1) sexual behavior (n = 34, 77%), (2) ARV adherence (n = 17, 39%), and (3) missed healthcare visits (n = 1, 2%). Twenty-seven trials (61%) reported solely on sexual behavior and 10 trials (23%) reported solely on ARV adherence; six trials (14%) reported on both and one trial (2%) reported on all three.
When syndemic factors and health behaviors were paired together, the most common pairings were drug use and sexual risk behavior (n = 23, 52%), alcohol use and sexual risk behavior (n = 15, 34%), and mental health and sexual risk behavior (n = 16, 36%). Less than a quarter of the trials paired syndemic factors with ARV adherence: mental health and ARV adherence (n = 10, 23%), drug use and ARV adherence (n = 7, 16%), and alcohol use and ARV adherence (n = 5, 11%). Only one study (2%) paired drug use and missed healthcare visits and mental health and missed healthcare visits.
Excluded Trials
Of the 54 excluded publications, approximately half (n = 26, 48%) were excluded due to not reporting the proportion of the sample who were SMM. Other reasons were: reporting that <50% of the sample were SMM and not including data specifically for the SMM subsample (n = 8, 15); not reporting a health behavior outcome (n = 6, 11%); only reporting case studies and not the results of an intervention trial (n = 4, 7%); containing a description of the intervention development process and not efficacy data (n = 2, 4%); only providing qualitative data about the intervention’s effects (n = 2, 4%); only enrolling female participants (n = 1, 2%); only enrolling healthcare providers as participants but not members of our target population (n = 1, 2%); not having the results appear in a peer-reviewed article (n = 1, 2%); and providing results from a pharmacologic (not behavioral) intervention (n = 1, 2%). Of note, due to our strict inclusion criteria focusing on SMM, there are a number of interventions that co-target syndemics and HIV-related health behaviors that were not included.
A Summary of the Methodologic Status of the Literature
There were 44 intervention trials reported in the 43 reviewed papers. The average N among trials was 166, ranging from 8 to 1,686. An average of 54% across samples were people of color, with a range of 3.7% to 100%. Only one study included transgender or gender diverse participants (n = 4). All but three studies were conducted in the U.S.
Recruitment Strategies
Thirty-three studies used more than one recruitment method, with a range from two to five unique strategies employed. Among those using a single recruitment method, the most common was recruitment within a medical setting/HIV clinic or through referrals from health-care providers (n = 8). In one study, the authors did not describe the recruitment strategy used. Hanging flyers and recruitment posters were common (n = 21), as were other forms of passive recruitment, such as print (n = 10) and online advertisements (n = 16). Sixteen studies used referrals from individual providers, clinics, or substance abuse treatment clinics to identify prospective participants. Fourteen studies recruited within HIV service organizations or other community agencies, and 16 studies actively recruited using community and street outreach. Finally, a small number (n = 5) of studies recruited participants who were involved in other prior or ongoing research studies, and eight noted that participants were recruited through their peers or other forms of word of mouth.
Research Setting and Intervention Type and Delivery
Studies were conducted in various types of research settings. Intervention activities took place in research centers (n = 6), community and LGBT health centers (n = 9), and HIV clinics (n = 4). Fewer intervention settings occurred in addictions treatment centers (n = 2) or other agencies, such as public health departments (n = 2). One intervention was delivered across multiple settings, including remotely by telephone, at the participant’s home, and at public venues. Only one study was a tablet-based app, although it was delivered to participants at the clinic during an HIV testing appointment.
Twenty-one of the interventions were described as pilot trials, the majority of which (n = 13) were single-arm designs. The average number of participants in the pilot trials (all but two reported these data) was 46.9, with an average of 8.4 intervention sessions (SD = 5.5). The remainder of the trials (n = 23) were not pilot trials. Of those, one was a single-arm study, 18 were two-arm studies, three were three-arm studies and one was a four-arm study. The average number of participants across the 23 non-pilot studies was 274, with an average of 12.4 (SD = 12.3) intervention sessions. However, two studies had a large number (n = 48) of possible intervention sessions; excluding these outliers, the average number of intervention sessions was 9.0 (SD = 5.2). Most (n = 27) interventions were individually delivered, while one-quarter (n = 11) were delivered in a group format. We identified only one couple-based intervention. All but two studies, one delivered through a Facebook chat and the other using a tablet-based app, were delivered in-person. Three of the in-person interventions also had an additional telephone delivery component for some intervention content.
Among the studies whose design included a control condition (n = 33), seven used attention-matched controls and seven were treatment-as-usual or enhanced treatment-as-usual arm. Three control conditions consisted of a smaller set of the larger activities in the intervention arm. For instance, Antoni et al. (Citation2006) provided ARV adherence training plus cognitive behavioral stress management as the intervention arm, and ARV adherence training alone as the control condition. Four studies used a wait-list control condition. Two studies made referrals to services as their control condition (Kahler et al., Citation2018; Velasquez et al., Citation2009) and one provided HIV testing only as the control (Santos et al., Citation2014). Five other interventions reported control conditions that varied in type and intensity.
The included articles varied in terms of how they described primary and secondary outcomes. Half of the studies (n = 22) described both the health behavior and one or more syndemic indicators as co-primary outcomes. Fourteen studies described the health behavior as the primary outcome, and a syndemic indicator as a secondary outcome. Only four studies noted a syndemic indicator as the primary outcome and the health behavior as a secondary outcome. The remaining studies reported both health behaviors and syndemic indicators factors as secondary outcomes.
In 17 interventions, authors described the content as culturally tailored for SMM in a number of ways, primarily through developing psychoeducational content, strategies, and examples that specifically referenced and reflected the experiences of SMM. In addition, SMM-tailored interventions were grounded in SMM-specific theories or models, adapted from a prior SMM-focused intervention, and developed using formative research with SMM (e.g., focus groups). However, there were numerous interventions that did not explicitly state that they were tailored to SMM in these ways, but were individually tailored to the unique circumstances of participants' (many or all of whom were SMM) lives and, therefore, were substantively but not systematically tailored to SMM. Thus, depending on whether tailoring only includes explicit mention of being tailored to SMM or also may include tailoring to an individual without explicit mention of being tailored to SMM, the proportion of tailored interventions ranges from 34% to 68%.
One-quarter (n = 11) of interventions did not report providing incentives for completing assessments or attending sessions. The majority of interventions (57%; n = 25) reported incentivizing completion of assessments and 13 incentivized session attendance. Three interventions provided incentives, although it was not clear when those incentives were delivered and three trials were primarily contingency management.
There was substantial variation in whether, and the degree to which, the number of planned sessions were completed by participants. Sixteen studies reported an average of 75.1% completion of planned sessions by participants in the treatment arm. Only 10 interventions reported planned sessions completed in both the experimental (average sessions completed = 72.8%) and control (average sessions completed = 76.7% for these 10) arms of the study. Four studies reported the percentage of participants completing all sessions (47.5%).
The average number of weeks of follow-up assessments across all interventions was 33.5 (range = 6–64 weeks). The average percent retention at the final follow-up assessment was 81.2%, with a range of 58% to 100%.
A Summary of Intervention Results by Syndemic and Health Behavior Combination
Next, we present the outcomes of the combined syndemic and HIV-related health behavior intervention studies we reviewed. We present the interventions that targeted (a) mental health, (b) alcohol use, and (c) drug use, respectively. For studies that targeted mental health alone, we listed them in the Mental Health section. For studies that targeted mental health and alcohol or drug use, we listed them in the Alcohol or Drug Use section, respectively. For studies that targeted both alcohol and drug use, we listed them in the Drug Use section.
Interventions Targeting Mental Health (N = 15)
Mental Health and Sexual Risk Behavior (N = 7/15)
Of the 15 trials that solely targeted mental health (i.e., not in combination with substance abuse reduction), seven (47%) co-targeted sexual risk behavior. Five (71%) of these trials were RCTs. The remaining two (29%) were open pilots (Hart et al., Citation2016; Reisner et al., Citation2011). Six (86%) of these trials exclusively included SMM. All seven (100%) assessed in-person interventions. Five (71%) were group-based interventions (Hart et al., Citation2016; Reisner et al., Citation2011; Williams et al., Citation2013, Citation2008).
Mental health symptoms targeted included depression (n = 5, 71%), anxiety and stress (n = 5, 71%), traumatic stress and PTSD (n = 3, 43%), loneliness (n = 2, 29%), self-efficacy (n = 1, 14%) (Carrico et al., Citation2009; Hart et al., Citation2016), and sexual compulsivity (n = 1, 14%; Hart et al., Citation2016). Cognitive behavioral therapy (CBT) techniques were used in all trials to address mental health (n = 7, 100%). A few trials noted explicitly using psychoeducation (n = 4, 57%), motivational interviewing (MI; n = 4, 57%), or problem solving (n = 3, 43%) techniques as well.
Five (71%) trials reported on within-group changes across time in mental health for the intervention condition. Of the five, three (75%) reported significant, favorable changes in depressive symptoms, two (50%) reported significant, favorable changes in loneliness, and one (25%) reported significant, favorable changes in anxiety. All five RCTs provided enough information to calculate effect sizes for the mental health outcomes. Among those three trials, there were no observed statistically significant between-group differences in either depression (d range = −0.15 to 0.06) or anxiety (d range = −0.06 to 0.06) symptoms. One trial reported a significant difference in stress (d = −0.13, 95% CI: −0.26, 0.00; Carrico et al., Citation2009).
To address sexual risk behavior, all of the trials (n = 7, 100%) reported using CBT techniques. Additional techniques specifically noted to address sexual risk behavior included MI (n = 3, 43%), problem solving (n = 3, 43%), and psychoeducation (n = 1, 20%). Six out of seven (86%) trials reported within-group changes in sexual risk behavior over time. Of those six, five (83%) reported significant, favorable changes in sexual risk behaviors for the intervention condition. Four of the five RCTs provided enough information to calculate effect sizes for the sexual risk behavior outcomes. For the remaining RCT, although the authors did not report enough information to calculate effect sizes, they did report a significant difference between the intervention and control conditions for sexual behavior outcomes.
Mental Health and ARV Adherence (N = 8/13)
Of the 13 studies that solely targeted mental health, eight (62%) co-targeted ARV adherence. Five (63%) of these trials were RCTs. Two (25%) trials were pilot RCTs. The remaining trial (12%) was a one-arm feasibility study (Kennard et al., Citation2014). Only three trials (38%) exclusively included SMM. All eight (100%) trials assessed in-person interventions. Six (75%) trials were individual interventions and two (25%) trials were group-based interventions.
Mental health symptoms that were targeted in these trials included depression (n = 8, 100%), anxiety (n = 2, 25%), global functioning (n = 2, 25%), and body image disturbance (n = 1, 13%). All of the interventions utilized CBT techniques (n = 8, 100%) to address mental health. Psychoeducation (n = 3, 38%), relaxation (n = 3, 38%), MI (n = 2, 25%), problem solving (n = 2, 25%), and supportive therapy (n = 1, 13%) techniques were also explicitly noted as intervention components for some trials.
Seven (88%) trials reported on within-group changes in mental health. Of those, six (86%) reported beneficial changes in depressive symptoms, one (14%) reported beneficial changes in anxiety, one (14%) reported beneficial changes in global functioning, and one (14%) reported beneficial changes in body image disturbance for participants assigned to the intervention condition. Four of the RCTs provided enough information to calculate effect sizes for mental health measures. Of those four, two (50%) reported significant group differences in depression (d range = −0.75 to −0.45) and global functioning (d range = −0.83 to −0.53) (Safren et al., Citation2016, Citation2009). Only one (50%) of the pilot RCTs provided enough information to calculate effect sizes. That trial reported a non-significant trend for depressive symptoms (d = −0.54, 95% CI: −1.18, 0.10) and a significant effect on body image disturbance (d = −1.08, 95% CI: −1.75, −0.40).
To address ARV adherence, all of the trials (n = 8, 100%) reported using CBT techniques. Additional techniques specifically noted to address ARV adherence included problem solving (n = 3, 38%), psychoeducation (n = 2, 25%), and MI (n = 1, 13%). Seven (88%) trials reported within group changes in ARV adherence over time. Of those seven, three (43%) reported significant beneficial changes over time in ARV adherence in the intervention group. Four of the RCTs provided enough information to calculate effect sizes for ARV adherence measures. Of those, one (25%) reported significant group differences in ARV adherence (d = 1.36, 95% CI: 0.71, 2.01). One of the pilot RCTs also provided enough information to calculate effect sizes (Blashill et al., Citation2017). That trial did not find significant group differences on ARV adherence measures, but results trended in a positive direction (d range = 0.38 to 0.57).
Interventions Targeting Alcohol use (N = 5)
Five trials had the main objective to reduce alcohol use, without a focus on other types of substance use. Three (60%) of these studies were RCTs to assess efficacy, one was a pilot study, and the fifth study appeared to be, although not explicitly stated as, a pilot trial as well. Four (80%) of the five studies exclusively recruited SMM and one identified SMM as just over half (53.1%) of the sample. The percentage of persons of color across the four trials ranged from 94% to 30% (with the authors separately reporting that four participants were Latinx). Four interventions were delivered in-person and were either exclusively individually delivered or had both an individual and a peer group education/support component. One intervention was a tablet-based app that was delivered in the clinic during an HIV testing visit (Wray, Kahler, Simpanen, & Operario, Citation2019).
Alcohol use and HIV Clinical Outcomes (N = 2/5)
Two (40%) studies assessed the effects of alcohol use on HIV clinical outcomes, including VL, CD4 cell count, or self-reported ARV adherence. Using a motivational interviewing approach (MI), the 8-session Project PLUS intervention (Parsons, Golub, Rosof, & Holder, Citation2007), compared to a time- and content-matched control, showed a significant improvement at the six-month assessment for log VL (d = 0.20, 95% CI: −0.17, 0.57) and CD4 cell counts (d = 0.20, 95% CI: −0.17, 0.57). In the same study, there were also significant improvements in the intervention condition compared to the control condition for the percentage of self-reported doses taken (divided by the number of prescribed doses) in the previous 14 days (6-month assessment d = 0.20, 95% CI: −0.17, 0.57) and the percentage days of perfect ARV adherence in the previous 14 days at the three-month assessment (6-month assessment d = 0.29, 95% CI: −0.08, 0.66). In addition to these between-group differences, participants in both conditions reported significant increases in these ARV adherence factors at the three-month assessment visit. In contrast, no improvements in HIV clinical care outcomes (VL, CD4 cell count) were found in the study by Kahler et al. (Citation2018).
No group differences in alcohol use were found in the trial by Parsons et al. (Citation2007). However, both groups reported significant decreases in the number of standard drinks consumed in the previous 14 days, and in the number of drinks consumed during drinking days in the previous 14 days, at both the 3- and 6-month assessments (see below for effects on alcohol use in the trial by Kahler et al., Citation2018).
Alcohol use and Sexual Risk Behavior (N = 3/5)
Three (60%) studies used an MI approach, or a combination of MI and the transtheoretical model of change, to address the ways that alcohol use may impact sexual behavior. Kahler et al. (Citation2018) reported significant decreases in the number of days having sex under the influences of alcohol or drugs at the 3-month assessment, but not at the 6- or 12-month assessment visits, for the treatment condition compared to the control condition. However, when restricted to SMM who reported sexual risk behavior at baseline, the authors identified significant improvements in the treatment group compared to the control group in the number of days reporting condomless sex with non-primary partners (d = 0.37, 95% CI: 0.06, 0.68), and the number of days reporting sex under the influence of alcohol and drugs (d = 0.14, 95% CI: −0.17, 0.45), at the 3- and 12-month assessment visits. Similarly, the trial by Velasquez et al. (Citation2009) showed no between-group intervention effects on sexual risk behavior in an intent-to-treat analysis, but did find significant improvements in the reduction of sexual risk behavior for the intervention group when the sample was restricted to those men who reported heavy-drinking and unprotected-sex days at baseline (d = 0.59, 95% CI: 0.31, 0.86), i.e., the men who were most in need of the intervention. In the same study, men in both conditions showed decreases in the number of drinks, drinking days, and heavy drinking days over the study period. In contrast, Wray et al. (Citation2019) found that men who were randomized to receive the in-clinic tablet-based app plus standard HIV testing were more likely to report fewer new anal sex partners at the 2- and 3-month follow-up assessments compared to men who received standard HIV testing alone. No between group differences were detected for CAS or CAS with new or casual partners or partners with an unknown HIV status.
All studies reported significant improvements in alcohol use outcomes in the treatment group compared to the control group. The treatment group reported fewer drinks per week in the Kahler et al. study (Citation2018) compared to the control condition (d = − 0.33, 95% CI: −0.64, −0.02). Likewise, compared to the control group, the treatment group reported fewer drinks in the previous 30 days in the Velasquez et al. (Citation2009) study (d = .18, 95% CI: −0.09, .45). Both of these studies showed that treatment condition participants reported fewer heavy-drinking days in the previous 30 days (d for Kahler et al. = −0.40, 95% CI: −0.71, −0.09; d for Velasquez et al. = .22, 95% CI: −0.05, .49). The results of the study by Wray et al. (Citation2019) showed that those in the treatment condition reported fewer total drinking days and fewer alcohol-related problems over the three-month follow-up period compared to those in the control condition.
Alcohol use, Mental Health, and Sexual Risk Reduction (N = 1/5)
One (20%) study assessed the effects of a CBT-based intervention to address alcohol use, mental health (depression, anxiety), and other minority stress factors (e.g., rejection, internalized homophobia, concealment, emotion regulation, and social support) to reduce condomless sex among SMM (Pachankis, Hatzenbuehler, Rendina, Safren, & Parsons, Citation2015). In a trial of 67 SMM, the ESTEEM (Effective Skills to Empower Effective Men) intervention was individually delivered over 10 sessions. Compared to a waitlist control, SMM randomized to the ESTEEM condition reported significant improvements in alcohol use problems (d = 1.03, 95% CI: 0.50, 1.56) and depressive symptoms (d = 0.55, 95% CI: 0.05, 1.05). There were non-significant trends for improvement in the number of days of heavy drinking in the previous 90 days (d = 0.32, 95% CI: −0.18, 0.82) and anxiety (d = 0.47, 95% CI: −0.03, 0.97). Significant group effects were found on a variety of condom use outcomes, including condomless acts with casual partners in the past 90 days (d = 0.59, 95% CI: 0.09, 1.09), condom use self-efficacy (d = 0.93, 95% CI: 0.41, 1.45), and sexual compulsivity (d = 0.76, 95% CI: 0.25, 1.27). When results from the intervention and waitlist groups were pooled, significant within-group effects were found in each of these factors, with the exception of the number of days of heavy drinking in the previous 90 days, which showed non-significant improvement (p < .10).
Interventions Targeting Drug use (N = 24)
The majority of trials (24 studies described in 23 papers) targeted drug use. Seven of these focused on drug use only (29%), eight studies (7 published papers) on drug and alcohol use (33%), four on drug and alcohol use as well as mental health (17%), and five on drug use and mental health (20%).
Drug use Only (N = 7/24)
Of the seven trials that targeted drug use, four (57%) co-targeted sexual risk and three (43%) co-targeted both sexual risk and ARV adherence.
Drug use and Sexual Risk Behavior (N = 4)
Of the four studies that co-targeted drug use and sexual risk behavior, two (50%) were fully powered RCTs and two (50%) were uncontrolled pilot studies. All four (100%) studies only included SMM and assessed in-person interventions. Two (50%) were individual interventions, one (25%) was a couples intervention, and one (25%) intervention involved four randomization assignments, comparing (1) group-based CBT to (2) SMM-specific CBT, (3) contingency management, and (4) CBT plus contingency management.
Two (50%) of the trials tested interventions of MI techniques and one (25%) compared general versus SMM-specific CBT focused approaches. Wu et al. (Citation2011) aimed to address knowledge and technical skills related to drug use and sexual risk reduction, in addition to expectancies of methamphetamine use. Both fully powered RCTs reported significant between-group differences, indicating that the interventions had performed favorably. Specifically, Morgenstern et al. (Citation2009) found that participants in the intervention group reported lower club drug use at the 12-month follow-up visit compared to the control group (d = 0.61, 95% CI: 0.11–1.11). Further, Shoptaw et al. (Citation2005) reported similar findings across their four-arm trial: those who received general CBT produced fewer metabolite-free urine samples compared to participants randomized to any of the other three conditions (i.e., SMM-specific CBT, contingency management, CBT plus contingency management). However, Shoptaw et al. (Citation2005) did not provide enough information to compute effect sizes.
To decrease sexual risk behavior, two (50%) of the trials reported using MI techniques. Shoptaw et al. (Citation2005) used SMM-specific CBT strategies to address sexual risk behaviors in the context of drug use. Wu et al. (Citation2011) described providing psychoeducation and technical skills related to HIV and other STI transmission and condom use. Investigators found no significant differences at the final assessment visits for either of the two fully powered RCTs. One (25%) trial identified a significant reduction in unprotected receptive anal sex in the first four weeks of treatment in the SMM-specific CBT group (Shoptaw et al., Citation2005); however, at the six- and twelve-month follow-up visits, there were no significant differences across groups. In both uncontrolled pilots, authors identified within-group improvements from pre- to post-intervention for sexual risk behavior. Neither of the RCTs reported sufficient data to calculate effect sizes in relation to sexual risk behavior.
Drug use, Sexual Risk, and ARV Adherence (N = 3)
Of the three studies that triply targeted drug use, sexual behavior, and ARV adherence, two (67%) were RCTs and one (33%) was an uncontrolled pilot feasibility study. All three included SMM and were conducted in-person. The uncontrolled pilot and one of the RCTs were contingency management interventions that involved providing vouchers to participants in exchange for drug-free urine samples. The second RCT was an individually delivered weekly intervention involving motivational interviewing and CBT focused on reducing methamphetamine use.
Although the uncontrolled pilot study did not have a comparison condition, the authors observed a significant pre- to post-intervention decrease in number of days of methamphetamine use reported from baseline to the three-month assessment. In a subsequent RCT of the same intervention, participants in the contingency management group submitted significantly more drug-free urine samples than participants in the control group. Despite the group difference not reaching statistical significance in the RCT, at the six-month follow-up visit, participants in the CM group continued to submit more drug-free urine samples than control group participants (d = 0.36, 95% CI: 0.03, 0.70; Landovitz, Fletcher, Shoptaw, & Reback, Citation2015). Although Parsons, John, Millar, and Starks (Citation2018) did not provide overall means by condition, men in both conditions reported significant reductions in days of methamphetamine use at the three-month follow-up visit, and days of methamphetamine use did not differ between groups (d = 0.07, 95% CI: −0.20, 0.34.
To address sexual behavior and ARV adherence in these three trials, two (67%) of the studies provided participants with post-exposure prophylaxis (PEP) for use after any reported episode of high-risk sex. In the third study, therapists used MI and CBT strategies to increase ARV adherence and reduce condomless anal sex. From baseline to the three-month follow-up visit, the uncontrolled pilot reported significant decreases in the number of sexual partners over the past 30 days, as well as decreases in the number of instances of unprotected anal intercourse. Both RCTs provided sufficient information for calculating effect sizes involving sexual risk outcomes; however, none were significant.
Both Drug and Alcohol use (N = 8/24)
There were eight trials (seven published papers) focused on interventions to reduce both drug and alcohol use concurrently. Of those eight trials, for the health behavior target, six (75%) focused on sexual behavior, one (13%) focused on both sexual behavior and ARV adherence, and one (13%) on ARV adherence alone.
Drug and Alcohol use and Sexual Behavior (N = 6)
Of the six trials that targeted drug and alcohol use together, as well as sexual risk behavior, five (83%) were RCTs and one (17%) was an uncontrolled trial. All trials enrolled SMM exclusively. Three (50%) trials assessed group-based interventions, two (33%) assessed individually delivered interventions, and one (17%) assessed a combined individual and group intervention.
The intervention content related to drug and alcohol use involved MI or CBT skills for drug use reduction (e.g., identifying triggers, craving management, and relapse analysis). Additionally, some interventions described emphasizing the connections between depression, drug use, and experiences of stigma and discrimination.
Two (33%) of the trials did not find significant intervention-related differences in drug and alcohol use. One (17%) study found reductions in the odds of drug use in the MI condition versus the control condition, which was psychoeducation only. Santos et al. (Citation2014) found that a greater proportion of those who engaged in Personalized Cognitive Counseling (PCC) discussions reported abstinence from alcohol, marijuana, and phosphodiesterase-5 (PDE-5) inhibitor use during the follow-up period. Finally, although Shoptaw et al. (Citation2008) did not find a significant difference in number of positive drug screens for stimulants between groups, they did observe differences in patterns of drug use between-groups, with those in the “gay-specific” CBT condition (an intervention that was culturally tailored to SMM) averaging significantly higher percentages of negative screens for drug metabolites compared to the gay-specific social support category. Further, longitudinal modeling showed that over the 16-week follow-up period, the gay-specific CBT condition produced significantly fewer days of methamphetamine use compared to the gay-specific social support category. Three (50%) studies provided enough detail to calculate effect sizes related to changes in drug and alcohol use, none of which were significant.
To address sexual risk behavior, the majority of trials reported using psychoeducation as an intervention tool to reduce sexual risk, including provision of content regarding the linkages between sexual risk and alcohol or drug use. Additionally, one (17%) trial used MI to improve motivation to reduce condomless anal sex, and that trial was the only one to report a significant intervention effect on sexual risk behavior. Three (50%) trials reported sufficient information to calculate effect sizes, only one (17%) of which was significant: change in unprotected receptive anal sex at 12-month follow-up in the Mansergh et al. (Citation2010) trial (d = 0.13, 95% CI: 0.01–0.25). All other effect sizes assessing change in sexual behavior were non-significant, including three measures from the Mansergh et al. (Citation2010) trial (ds ranged from 0.03 to 0.13), four from the Kurtz, Stall, Buttram, Surratt, and Chen (Citation2013) trial (ds ranged from 0.04 to 0.1), and one from the Parsons, Lelutiu-Weinberger, Botsko, and Golub (Citation2014) trial (d = −0.15, 95% CI: −0.52, 0.22).
Drug and Alcohol use and ARV Adherence (N = 1)
One uncontrolled pilot study targeted drug and alcohol use as well as ARV adherence (Carrico et al., Citation2014). In this study, authors recruited MSM with HIV for weekly individual in-person sessions. Therapists in this open pilot took a harm reduction approach to skills teaching, for example, transitioning to less potent modes of methamphetamine administration, promoting self-care strategies while using methamphetamine, and delivering education about safer injection practices. Results indicated that participants reported significant reductions in stimulant use, but increases in marijuana use, over the 12-month follow-up period. Additionally, more HIV-positive participants also reported undetectable viral load from baseline to the 12-month follow-up visit. As this was an uncontrolled study, we could not calculate a between-group effect size.
Drug and Alcohol use, Sexual Behavior, and ARV Adherence (N = 1)
The trial that targeted drug and alcohol use as well as sexual behavior and ARV adherence was an uncontrolled open pilot involving mostly SMM with HIV. In this study, Carrico et al. (Citation2014) leveraged evidence-based intervention components to behavior change, while maintaining a harm reduction focus. Although the aim of the pilot study was to establish feasibility and acceptability, the investigators did observe reductions in drug use as well as in sexual risk-taking while under the influence of methamphetamines. Specifically, there were reductions in self-reported methamphetamine use, PDE-5 inhibitor use in combination with other drugs, and in sexual risk-taking while using methamphetamines – although there were increases in marijuana use. As this was an uncontrolled study, a between-group effect size could not be calculated.
Drug and Alcohol use and Mental Health (N = 4/24)
Of the four trials that targeted both alcohol and drug as well as mental health, three (75%) co-targeted sexual risk and one (25%) co-targeted both sexual risk and ARV adherence. Authors did not provide sufficient data to calculate between-group effect sizes.
Drug and Alcohol use, Mental Health, and Sexual Risk Behavior (N = 3)
Three trials targeted the combination of drug and alcohol use, mental health, and sexual behavior. One (33%) was an RCT and two (67%) were uncontrolled pilots. All three (100%) involved SMM, with two (67%) focused on HIV-positive participants and (33%) one that included only HIV-negative participants and those with an unknown HIV status. One (33%) of the interventions was an individual intervention delivered online, one (33%) was an individual intervention delivered in person, and the third (33%) was a group-based intervention delivered in person.
In addition to targeting drug and alcohol use, the interventions in these three studies also targeted mental health. All three (100%) targeted depressive symptoms, two (67%) targeted anxiety symptoms, two (67%) targeted sexual-orientation related stigma, and one (33%) additionally targeted several other mental health-related outcomes (e.g., loneliness, self-esteem, and need for acceptance).
The RCT by Safren, O’Cleirigh, Skeer, Elsesser, and Mayer (Citation2013) demonstrated that men who screened positive for depression at baseline, and who were assigned to the intervention group showed significant reductions in depression at the 12-month follow-up; however, they found no intervention effect on drug or alcohol use. Both pilot trials reported reductions in drug use. Additionally, in relation to mental health, Smith et al. (Citation2017) found changes in internalized homonegativity, loneliness, and self-esteem from pre-post. None of these three trials provided sufficient information for calculating effect sizes related to drug and alcohol use or mental health.
In terms of reducing sexual risk behavior, all three (100%) studies described providing psychoeducation related to reducing HIV sexual risk. One (33%) trial specified using MI and CBT strategies; one (33%) described modules addressing triggers for high-risk sex, links between stress and sex, as well as HIV status disclosure and relationship satisfaction; and the third (33%) trial described role-playing sexual communication skills. The RCT did not find a group by time effect, although both pilot trials found pre-post within-group changes in sexual behavior, with one reporting decreased HIV-related risk behavior and the other reporting a decreased number of sexual partners. The RCT provided sufficient data for calculating an effect size related to transmission risk behavior, albeit small (Cohen’s d = 0.08, 95% CI: −0.20, 0.36; Safren et al., Citation2013).
Drug and Alcohol use, Mental Health, Sexual Risk Behavior, and ARV Adherence (N = 1)
One trial targeted drug and alcohol use, mental health, and two health behaviors (sexual behavior, ARV adherence; Esposito-Smythers et al., Citation2014). This study was an uncontrolled pilot involving HIV-positive young people ages 16–24, most of whom were SMM. This individual-level intervention integrated CBT with contingency management and aimed to reduce alcohol and marijuana use and sexual risk behavior, as well as to improve mental health symptoms and ARV adherence. Although the pilot study was designed to establish feasibility and acceptability, the investigators did observe reductions in drug use and mental health symptoms, but not improvements in the health behaviors. They also found that participants reported reductions in alcohol use, withdrawal symptoms, dependence symptoms, and drug-related problems, as well as co-occurring depressive symptoms. Since this was an uncontrolled pilot trial, we could not calculate a between-group effect size.
Drug use and Mental Health (N = 5/24)
Five trials targeted two syndemic conditions (drug use, mental health) and sexual risk behavior. Of these five, one (20%) additionally aimed to improve ARV adherence and maintain engagement in care by reducing missed medical visits.
Drug use, Mental Health, and Sexual Risk Behavior (N = 4)
Of the four trials in this category, two (50%) were pilot RCTs and two (50%) were uncontrolled pilot trials. All four (100%) trials enrolled SMM exclusively and provided individual, in-person interventions. In addition to drug use, the mental health targets included traumatic stress, depressive symptoms, positive and negative affect and emotion regulation, anxiety, and obsessive-compulsive symptoms. The interventions to address drug use and mental health each involved multicomponent strategies including, but not limited to, CBT focused on minority stress experiences, expressive writing, behavioral activation, and a multi-component intervention that combined contingency management, positive affect enhancement, content to optimize affect regulation, and skills for engaging in the recovery process.
Although between-group effect sizes could not be calculated from the information provided for the two (50%) uncontrolled pilots, effect sizes could be calculated for the two (50%) pilot RCTs. Of the two uncontrolled pilots, one (50%) reported decreases in depression symptom severity, and one (50%) reported decreases in depression and anxiety symptoms. Of the four interventions, two (50%) reported decreases in stimulant use. However, the effect size calculated based on Carrico et al.’s (2015b) estimated difference in stimulant use between groups at 3-month follow-up was not significant (d = −0.22, 95% CI: −1.06, 0.62). Carrico et al. (Citation2015b) did find significant effect sizes in HIV-related trauma at 3-month follow-up (d = 1.19, 95% CI: 0.28, 2.10) but not in either total number of risky partners at 3-month follow-up (d = 0.00, 95% CI: −0.84, 0.84) or number of partners using methamphetamine at 3-month follow-up (d = 0.47, 95% CI: −0.38, 1.32). Carrico et al. (Citation2015a) also did not find significant effect sizes when comparing methamphetamine use in the past 30 days at 6-month follow-up between groups (d = 0.85, 95% CI: −0.05, 1.75) or number of risky anal sex partners at the 6-month follow-up visits (d = 0.00, 95% CI: −0.86, 0.86).
Drug use, Mental Health, Sexual Risk Behavior, ARV Adherence, and Missed Healthcare Visits (N = 1)
One trial targeted two syndemic conditions (drug use, mental health) and three health behaviors (sexual behavior, ARV adherence, missed health-care visits; Rotheram-Borus et al., Citation2004). This was a three-arm RCT that involved an individual-level intervention delivered (1) by telephone or (2) in-person, with (3) a delayed-intervention control. It included young people with HIV (16–29 years old), with most participants identifying as SMM. This trial aimed to reduce drug use, emotional distress, and missed medical appointments, and to increase ARV adherence and the proportion of condom use in sexual encounters. Although authors provided insufficient data to calculate an effect size, they reported a significant between-group effect: the in-person intervention resulted in a higher proportion of sexual acts protected by condoms than the other intervention groups. Specifically, youth in the in-person arm showed increases in the percent of protected sex acts across all sex partners (increasing from 45% at baseline to 58% at follow-up) compared to the delayed-intervention condition (decreasing from 30% to 22%). Additionally, youth in the telephone arm showed a significant decrease in the percentage of protected sex acts with HIV-negative partners (decreasing from 75% to 65%) compared to the in-person arm (increasing from 53% to 73%). There were no significant differences in ARV adherence scores between conditions and no significant differences in emotional distress between baseline and 15-month follow-up across groups.
Summary of Methodologic Rigor and Risk of Bias of Included Studies
We used the Cochrane Risk of Bias Tool for RCTs (Higgins & Green, Citation2011) to assess the methodologic rigor and risk of bias of the 30 RCTs (7 pilot RCTs) included in this review. This tool highlights seven areas of bias within each trial, each of which is rated as low, high, or unclear risk of bias. The areas include random sequence generation (selection bias); allocation concealment (selection bias); selective reporting (reporting bias); blinding of participants and personnel (performance bias); blinding of outcome assessors (detection bias); incomplete outcome data (attrition bias); or any other area of bias introduced by the study procedures.
The majority of RCTs were categorized as low risk of selection bias due to using adequate methods to generate a randomized sequence (n = 27, 90%) and concealment of allocations prior to assignment (n = 17, 57%). However, most trials failed to provide sufficient information to determine if there was selective outcome reporting (n = 17, 57%) or any other possible biases that should be accounted for (n = 19, 63%). The majority (n = 25, 83%) were evaluated as having a high risk of performance bias due to inadequate methods for blinding the participants or study staff to intervention allocation. Most trials were at high or unclear risk of detection bias, either due to the outcome assessors not being blinded to study condition (n = 12, 44%) or a lack of information about outcome assessor blinding (n = 12, 40%). Finally, although a good proportion of the trials appeared to be at low risk of attrition bias (n = 14, 47%) due to the amount, nature, or handling of incomplete outcome data, over half of the trials (n = 14, 52%) did not provide enough information to determine their risk of attrition bias.
Meta-Analytic Results
Core Analyses
A total of 44 intervention trials met our inclusion criteria. The trials are different along with a variety of dimensions, including outcomes, intervention approach, length, delivery setting, specific population of interest, and more. A description of the primary features of each trial is listed in and we present forest plots of the effect sizes of the RCT effects on syndemic () and health behavior outcomes () from the RCTs. Forest plots for the additional outcome categories are available as online supplementary materials (Figures 4–7).
Figure 2. Forest plot of RCT syndemic outcomes.
Figure 3. Forest plot of RCT health behavior outcomes.

Based on the data reported by the authors of the RCTs, we calculated between-group, pre-post effect sizes for 29 syndemics outcomes and 19 health behavior outcomes and tested them via meta-analysis (see ). The included RCTs significantly improved syndemics outcomes with an effect size of .20 (CIs: 0.12, .29), and significantly improved health behavior outcomes with an effect size of .16 (CIs: .03, .30), which correspond to small effects per Cohen (Citation1988). The heterogeneity statistics indicated significant heterogeneity in these effects, both for syndemics outcomes (Q = 73.47, p < .001) and health behavior outcomes (Q = 58.17, p < .001). We conducted individual analyses examining RCT effects on mental health, substance use (combining alcohol and drug use because of small ns of each), and sexual risk behaviors, each of which showed significant improvements in the .17 to .23 range of ds. The meta-analysis for ARV adherence yielded a non-significant d.
Table 2. Effect sizes and sensitivity analyses for syndemics and health behavior outcomes.
Sensitivity Analyses
Funnel plots appeared asymmetrical, confirmed quantitatively by Eggers’ tests, p < .001 for syndemics outcomes and p = .017 for health behavior outcomes. “Trim and fill” procedures reflected a smaller yet still positive and significant effect of the RCTs on syndemics outcomes (d = .09, CIs: .0036, .18), and a smaller, positive, non-significant effect of the RCTs on health behavior outcomes (d = .033, CIs: −0.12, .18). The fail-safe n, which represents the numbers of unpublished studies with null findings that would theoretically be required to bring these effects to non-significance, were 361 for syndemics outcomes and 52 for health behavior outcomes.
Stratified Analyses
We conducted stratified analyses to further examine the identified heterogeneity in RCT outcomes. No stratification variables were significant for the effects of the interventions on health behavior outcomes. However, we observed stronger effects of the intervention on syndemics outcomes for individual (vs. group) interventions (Qb = 5.431, p = .02) and interventions providing nine or more (vs. eight or fewer) sessions (Qb = 9.771, p = .002). RCTs with a follow-up period of six months or less (vs. more) showed stronger effects (Qb = 5.381, p = .02), reflecting attenuation of the intervention’s effects over time (potentially to be expected without booster sessions). Sexual minority-specific cultural tailoring was non-significant as a stratification variable for syndemics outcomes although many studies did not report on that element of their intervention development efforts.
Discussion
Overview of Findings
We identified 44 behavioral intervention trials published between 2001–2019 that co-targeted syndemic indicators and health behaviors among SMM. Findings from meta-analytic evaluation of the RCTs indicated small, positive, significant intervention effects on both syndemic (d = .20, CIs: 0.12, .29) and health behavior (d = .16, CIs: .03, .30) outcomes. Effect sizes for meta-analyses examining RCT effects on mental health, substance use (alcohol and drug use), and sexual risk behaviors also showed small, positive, significant improvements in the .17 to .23 range of ds. The meta-analysis for ARV adherence yielded a non-significant effect size estimate, indicating that the health behavior meta-analysis is primarily driven by successful outcomes on sexual risk behavior reduction. Overall, these results reflect promising support for this growing line of research. The syndemics framework is based on the premise that multiple, co-occurring psychosocial epidemics are inextricably intertwined and, as such, are thought to interact synergistically to increase the burden of disease among vulnerable populations (Singer, Citation1996). There are some commonly identified limitations to the ways that a syndemic framework has been operationalized, one of which is that the typical analytic approach involves weighing equally each of the syndemic indicators and then investigating their associations with health behaviors or health status additively and not multiplicatively, as would follow from their theoretical interrelations (see Tsai & Burns, Citation2015).
The intervention development strategy reviewed here, of combining intervention techniques for syndemics and health behaviors, is novel and, we believe, has great potential to improve the health of SMM. Many mental health providers do not focus on working to change health behaviors, and many health-care providers focused on physical health do not focus on working to improve mental health symptoms. This is a false dichotomy, of course, and points to the need for a more holistic approach to health-care provider training that conceptualizes the two arenas as interrelated and not separate. In the behavioral interventions we identified, drug use was the most commonly targeted syndemic indicator, and sexual risk behavior was the most commonly targeted health behavior. There were a number of interventions that targeted mental health symptoms and alcohol and/or drug use and those studies provided mixed support for targeting multiple syndemics and/or multiple health behaviors concurrently, i.e.,, depending on the intervention, some of the intervention targets improved while others showed no changes. Many of the published trials were uncontrolled pilot studies and so, as those interventions are tested in RCTs, there is the potential for their efficacy to be evaluated favorably in the future.
Across the RCTs we examined, we observed modest effect sizes that indicated favorable intervention effects, with substantial heterogeneity across studies and outcome categories. In aggregate, the range of effect sizes suggests that combination prevention efforts must be strengthened to substantially impact the HIV epidemic among SMM. Combination behavioral interventions may be critical for reducing the HIV disease burden among SMM, yet this review indicates that their full potential has yet to be realized.
Interventions Targeting Mental Health
The most favorable intervention findings were those related to reducing mental health symptoms (d = .23, CIs: .12, .34). Most behavioral intervention trials solely targeting mental health (without a focus on substance use) were in-person interventions using CBT techniques to target both mental health and health behaviors. These interventions were primarily group-based and enrolled SMM exclusively. The majority of these trials reported within-group improvements in mental health symptoms and sexual risk behaviors, but few found significant between-group differences. Given this pattern of results, it could be the case that group-based interventions for SMM that co-target mental health and sexual risk behaviors may produce favorable change over time within individuals, but that they are not necessarily more effective than a standard health-focused group, which was the most common control group in the reviewed trials.
A different pattern emerged for the trials targeting mental health and ARV adherence. These trials primarily tested individual, in-person interventions utilizing CBT techniques and enrolled both SMM and other populations. Most of these trials reported significant within- and between-group improvements in mental health symptoms. Regrettably, most of these trials failed to find significant within- or between-group differences in ARV adherence. Indeed, the meta-analytic results speak to the efficacy of individual CBT interventions to decrease mental health symptoms within a variety of populations, including SMM. Unfortunately, this pattern of findings also highlights the difficulty in improving ARV adherence, especially in individuals with mental health symptoms. There are well-described challenges to conducting behavioral interventions for ARV adherence, including measurement difficulties and ceiling effects, that likely impacted the ability of the reviewed trials to effectively improve (or, perhaps, document improvements) in ARV adherence. CDC (Citation2018a) maintains a website of efficacious HIV-related behavioral interventions with the session content freely available. Future research is needed to improve the science of ARV adherence interventions, as well as to be able to more successfully improve ARV adherence in syndemically exposed SMM.
Interventions Targeting Alcohol use
Given the small number of effect sizes contributing to alcohol reduction outcomes, in our analyses, we combined interventions targeting alcohol use and those targeting drug use. The results of that substance use meta-analysis was a small, positive, significant intervention effect (d = .17, CIs: .05, .30), suggesting that the substance use component of the combination interventions is promising and, yet, could be bolstered to be more efficacious in the future.
Five studies focused primarily on reducing alcohol use (rather than drug use or a combined focus on alcohol and drug use). Across these studies, interventions aimed additionally to address mental health symptoms from the syndemic category, and HIV care outcomes and sexual risk behavior from the health behavior category. Although it is difficult to draw inferences from the results of this small group of trials, there was only one intervention focused on improving ARV adherence that was successful at changing that behavior as well as the associated clinical indicators of HIV viral load – although that study did not observe between-group differences in reducing alcohol use in comparison to the control condition. Interventions that aimed to reduce sexual risk behavior were found to be effective largely when restricted to participants reporting sexual risk behavior or heavy alcohol use at baseline. This finding highlights an important methodologic consideration in RCT design: selecting participants with high baseline values of the behavior that the intervention is designed to change is preferable at the stage of efficacy testing, as participants with low baseline values have little opportunity for improvement. Only one study had as a goal to address mental health alongside alcohol use. The findings on intervention effects for reducing alcohol use were shown across studies, which is encouraging. Four intervention trials showed greater improvement on one or more alcohol use measures for the intervention group compared to the control group; the fifth intervention showed improvement in alcohol use measures in both study arms.
Overall, the results of interventions that focus on reducing alcohol only are promising. More research is needed on how best to address problematic alcohol use among SMM to fully understand whether alcohol-focused interventions should be stand-alone programs or whether they are most effective when combined with content that also addresses other forms of drug use.
Interventions Targeting Drug use
Of the 44 trials included in this review, 24 targeted drug use (many in addition to other syndemic indicators). All but one of those 24 trials co-targeted sexual risk behavior. Five of the 24 trials also targeted ARV adherence, one of which co-targeted ARV adherence as well as missed health-care appointments. Eleven of the 24 trials were uncontrolled pilot studies and two were controlled pilot studies, with the aim to determine feasibility and acceptability of the intervention procedures. Within the 11 RCTs, the intervention efficacy varied in relation to changes in drug and alcohol use, mental health, and health behaviors. Although the results of some RCTs were non-significant between-group differences in drug use, the results of other trials did include significantly greater reductions in drug use in the intervention group compared to the control group. Five of the 11 RCTs reported some between-group differences in drug use; however, it is challenging to draw general conclusions from this group of studies because of the heterogeneity of the intervention content presented to participants. For example, the intervention conducted by Landovitz et al. (Citation2015) involved contingency management, which is a very specific type of behavioral intervention component not used in any of the other trials reviewed and challenging to implement in many clinical contexts. The studies aiming to address substance use, both alone and in conjunction with other syndemic indicators, were diverse, making generalizations challenging; however, it is clear that additional work is needed to reduce substance use among SMM.
Only two of the RCTs identified between-group reductions in sexual risk behavior. In the trial conducted by Parsons et al. (Citation2014), they reported a significant difference in the likelihood of reporting condomless sex on any day of follow-up relative to the odds of those in the education condition. In the trial by Shoptaw et al. (Citation2005), they reported a significant difference in reports of condomless receptive anal intercourse after the first four weeks of treatment, although that difference attenuated over the follow-up period. Overall, the interventions that aimed to address drug use in conjunction with health behaviors overwhelmingly focused on reducing sexual risk behaviors. Although some of these RCTs demonstrated success in reducing drug use, with some showing benefits for reducing mental health symptoms as well, the majority did not significantly and consistently reduce HIV sexual risk behavior. Future intervention development efforts are sorely needed to better mitigate sexual risk in the context of drug use, a combination of factors that has proven intractable to change.
Stratification Analysis Results
Stratification analyses helped us to disentangle some of the observed between-study variance in intervention effects, and may help to provide guidance to the field in terms of future directions. Surprisingly, no stratification variables were significant for the effects of the interventions on health behavior outcomes, although this finding is limited by a relatively small number (19) of effect sizes from RCTs that contributed to the analysis. A different pattern emerged from the stratification analyses on intervention outcomes related to syndemics – potentially facilitated by greater statistical power because there were 29 effect sizes included.
We observed significant study variance between individual (versus group) interventions and those that provided nine or more sessions, pointing toward the importance of greater intervention intensity in terms of mode and duration of treatment.
Excluding outliers, the average number of intervention sessions for pilot trials and non-pilot (primarily efficacy) trials was approximately eight and nine, respectively. Considerations for providing successful interventions to target populations include both determining efficacious content and balancing the population’s multiple needs against the feasibility of intervention implementation in “real world” settings. Although brief interventions have demonstrated efficacy across a number of behaviors (e.g., Dunn, Deroo, & Rivara, Citation2001), including reducing HIV risk behavior of people with HIV (Crepaz et al., Citation2014), the results of our review showed that most interventions targeting combined syndemic and HIV prevention and care outcomes are necessarily more intensive in comparison and, yet, may need to be even more intensive to further improve intervention outcomes. Despite the length of interventions being longer than typical public health interventions, it appears to be the case that co-targeting syndemic- and HIV-related risk requires an even greater intensity or duration of intervention, based on the modest effect sizes, especially for syndemically exposed SMM with complex psychosocial histories and individual, social, structural, and cultural barriers to reduce HIV-related risk.
SMM have unique syndemic and HIV-related health behavior patterns and needs that may not be addressed sufficiently in interventions developed and tested for heterosexual individuals with, or at high risk for acquiring, HIV. However, contrary to our expectation, sexual minority-specific cultural tailoring was non-significant as a stratification variable for syndemics outcomes – although many studies failed to report on that element of their intervention. We encourage intervention developers in this area, as part of future reports of behavioral intervention trials, to report more detail about the cultural tailoring process that they engaged in, or to note specifically that they did not use cultural tailoring. Approximately one-third of studies in our review reported explicitly having tailored intervention content to apply to SMM; an additional one-third of studies provided intervention content that was tailored to the individual and, therefore, may have been tailored to their SMM participants although not in a standardized (or measurable) way. Culturally tailoring intervention content and other factors (e.g., using similar peers for intervention delivery) appears to be associated with higher perceived intervention acceptability and more effective interventions among SMM (e.g., Horvath & Bauermeister, Citation2017).
We know of several interventions being developed that address the unique cultural context of SMM (e.g., Pachankis, Citation2014) as well as the intersecting identities of SMM (e.g., being both SMM and Black; Bogart et al., Citation2017, Citation2018), and that are working to incorporate content that acknowledges overlapping stigmas (e.g., sexual minority identity and drug abuser) in a meaningful way (Batchelder et al., Citation2019). Interventions addressing intersectionality of identities and stigmas may draw on emerging theories that recognize multi-faceted influences on syndemic and HIV-related behaviors such as resilience (Woodward, Banks, Marks, & Pantalone, Citation2017), and may find that addressing the affective correlates of internalized stigma may be advantageous in reducing HIV risk and improving self-care behaviors (e.g., Batchelder, Carrico, Acree, Hecht, & Moskowitz, Citation2018). We look forward to seeing more data about the process of, and outcomes of trials that use, SMM-specific cultural tailoring.
Risk of Bias in Reviewed Interventions
The methodologic rigor and introduction of bias observed were highly variable in the subset of trials that used an RCT design. Although most of the RCTs used and described strong methods to reduce the risk of selection bias (i.e., well-described randomization procedures), other potential sources of bias were either not described at all or poorly described (e.g., procedures to blind outcome assessors from intervention allocation; methods for handling missing outcome data), or the reported procedures indicated a strong possibility for bias to be introduced (e.g., procedures for blinding researchers and participants from intervention allocation). This pattern of results is unlikely unique to interventions that met our inclusion criteria. Instead, our findings in this category likely reflect the difficulties in sustaining methodologic rigor in behavioral RCTs generally. Specifically, it is straightforward to/generate a proper randomization sequence and enact procedures to blind to allocation all parties prior to group assignment, but it is considerably more challenging to keep participants from knowing which arm of a behavioral trial they are assigned to, especially if one arm includes more sessions or a different format than the others. Moving forward, it will be important for investigators to more rigorously report on their trials’ outcome blinding procedures and methods for handling missing outcome data; indeed, using the Cochrane instrument (Higgins & Green, Citation2011) would be helpful in planning trials, and using relevant publishing guidelines, like CONSORT for randomized trials (Schulz, Altman, & Moher, Citation2010), would be helpful in standardizing the reporting of all pertinent methodologic details. Further, to help decrease the risk of participant unblinding to allocation, resource-permitting, future interventions could consider control arms that are time-, location-, and format matched.
Additional Findings
Nearly all of the trials we reviewed were conducted in the U.S., despite our search strategy attempting to identify similar trials throughout North America and Western Europe where sex between men is the primary mode of HIV transmission (UNAIDS, Citation2017). We encountered no interventions conducted outside of North America or Western Europe that otherwise met our inclusion criteria. It will be important for this work, especially if it is found to be more successful, to be conducted cross-culturally to truly establish the efficacy of co-targeted interventions to address syndemics and HIV-related health behaviors.
Across intervention trials reviewed, just over one half (54%) of the participants identified as a person of color. In the U.S., Black and Latino SMM, especially youth, are at the highest risk for acquiring HIV and, after an HIV diagnosis, have poorer HIV care outcomes than their White peers (CDC, Citation2017a, Citation2018e, Citation2018d). New HIV diagnoses among Black SMM increased 4% and among Hispanic/Latino SMM increased 14% from 2011 to 2015; in contrast, new HIV diagnoses decreased by 10% among white SMM in the same time period (Centers for Disease Control and Prevention, Citation2018e). It will be critical for current and future syndemic and HIV intervention trials not only to enroll SMM successfully, but also to enroll Black and Latino SMM specifically – in order to change the course of the epidemic and meet the unmet health needs of these multiply stigmatized individuals. The focus on reaching those individuals at highest risk for HIV infection will require robust recruitment and retention plans to engage SMM of color that consider the often difficult challenges these men face and the potential mistrust of the medical and research establishment based on a history of unethical behavior, such as the Tuskegee syphilis experiment (Bogart, Wagner, Galvan, & Banks, Citation2010).
Current estimates hold that one-quarter of transgender women live with HIV, and over half of Black transgender women have been diagnosed with HIV (CDC, Citation2018c). Despite these alarming HIV rates among transgender populations, only one study in this review reported enrolling gender diverse participants (n = 4) in their intervention trial (Velasquez et al., Citation2009). In many cases, it was not clear whether the other intervention trials excluded transgender and gender diverse participants, or whether they were included but their participation was not reported clearly. For example, historically, it has been standard to assess only two options for gender (or sex, depending on the context), male and female, which likely fails to capture the gender identities of transgender, non-binary, and other gender diverse individuals. It is essential for contemporary intervention studies to assess and report gender in more nuanced ways (Williams Institute, Citation2014). Further, given the empirical research on syndemic indicators among transgender individuals – for example, the high rates of substance use – behavioral intervention developers should focus on tailoring programs to the unique needs and experiences of this group, efforts which could reduce significantly the burden of disease in these especially vulnerable, marginalized communities (Horvath, Iantaffi, Swinburne-Romine, & Bockting, Citation2014).
The intervention trials we reviewed included only two interventions conducted online, despite numerous recently completed and ongoing technology-based interventions addressing substance use and mental health to improve individuals’ HIV prevention and care outcomes (Muessig, LeGrand, Horvath, Bauermeister, & Hightow-Weidman, Citation2017; Tso, Tang, Li, Yan, & Tucker, Citation2016). In contrast, about one-third of the reviewed trials reported online recruitment of SMM, which we see as recognizing that many SMM use social media and other electronic venues for connecting with dating and sex partners (Grov, Rendina, & Parsons, Citation2014; Prescott et al., Citation2016). The growing use of eHealth and mHealth interventions could shift dramatically how we address syndemics and HIV-related health behaviors. However, with some notable successes (Mustanski et al., Citation2018), the effectiveness and eventual implementation of technology-based studies have not been fully determined. As more eHealth and mHealth interventions are tested for efficacy, future reviews like this one may provide clearer answers to open questions related to the efficacy of behavioral interventions using less conventional delivery formats.
Strengths and Limitations
Strengths of the present paper include an in-depth focus on combination interventions that summarize and compare studies both qualitatively and quantitatively in terms of design features, intervention components, and outcomes. We report on interventions in a highly granular manner, separating findings by sets of intervention targets to maximize accuracy. Pilot trials as well as fully powered RCTs are included, to give information about interventions at all stages of the development pipeline. We followed the PRISMA guidelines closely and made the most conservative methodologic decisions in an effort to reflect the state of the field as accurately as possible without overstating successes.
In a systematic review and meta-analysis of intervention trials, there exist two categories of limitations, (a) one of the review methodology, implementation, and analysis, and the other (b) in terms of the boundaries inherent in the conducted trials. First, despite our commitment to a thorough examination of the extant literature – and our team-based approach to each step in the review process to ensure validity – we may not have uncovered all relevant trials. Our explicit focus was on behavioral interventions that co-target syndemic indicators and HIV-related health behaviors for SMM because of that group’s heightened HIV risk. However, our strict inclusion criteria (>50% SMM in the sample if data were not reported specifically for the SMM subsample) resulted in some important trials not being included because their samples fell short of that bar. Similarly, we included trials that focused on North American or Western European SMM and, although we did not come across trials from other geographic regions, we did not specifically search for them and so might have missed an opportunity to review a greater number of interventions. Our focus was on interventions delivered to SMM directly; another important source of intervention-focused data might be interventions aimed at changing health-care provider behavior or structural factors. Further, most of the reviewed trials were conducted with urban SMM samples, reducing our ability to understand how this type of intervention might work with rural SMM. Given historical and logistical barriers to research participation, the reviewed trials may not have reached the SMM who are most in need of intervention. Finally, sensitivity analyses indicated significant heterogeneity in the effect sizes of the trials under study, leading us to be concerned about the reliability of the point estimates we have identified. The conduct and publishing of future studies, and a replication of these methods with additional data, will increase our confidence in the results.
Implications and Future Directions
A critical component for improving the health of SMM, including those who have HIV and those at high risk of acquiring it, is to increase our ability to support SMM to address the syndemic exposure that impedes their successful engagement in healthful and protective behaviors, as well as inhibits their full engagement in HIV-related health behavior interventions. Earlier on, the prevailing strategy was to develop piecemeal interventions to address mental health or substance use issues and, separately, to address HIV-related health behaviors. It is important to highlight that few interventions have aimed to address the other syndemic indicators, CSA or partner abuse. For the past 20 years, behavioral interventions have increasingly attempted to address combinations of mental health, substance use, and HIV risk behaviors. The results of those efforts are chronicled here and, overall, suggest that more work is needed to fully realize the potential of combination prevention interventions. However, there are interventions that demonstrate effectiveness and some intervention targets appear to be relatively moveable. Based on our review, we discovered a large number of trials focused on substance use that appear to have delivered consistent treatment gains. Nevertheless, when we examine the effect sizes in aggregate, it is clear that more work is needed.
The results of this review suggest that HIV intervention developers should consider modifications to intervention targets, intensity/duration, and cultural tailoring, as well as broadening the focus of intervention mechanisms from interpersonal alone to include modifying structural factors as well. First, given the interrelated nature of syndemics, combination behavioral interventions may benefit from focusing on improving multiple syndemic indicators within the same protocol, as some have begun to do. SMM often present clinically with many, multifaceted psychosocial needs that require therapists to focus on specific mental health targets when working with narrow intervention protocols; however, combination behavioral interventions allow clinicians to address the most pressing, potentially interrelated, psychosocial stressors. Co-targeting of syndemic indicators could look like a greater focus on generalizability of coping skills and strategies for more than one type of problem within a syndemic or across syndemic indicators – for example, addressing depression and anxiety both, or addressing substance use as well as reducing sexual risk behaviors, as some studies have done. For example, the ESTEEM intervention by Pachankis, Hatzenbuehler, Rendina, Safren, and Parsons (Citation2015) used a version of standard CBT techniques culturally tailored for SMM and found strong effects for depression, alcohol use, and condomless sex, among other variables. An alternative way to advance the science might be to begin a focus on the common psychological mechanisms across syndemic indicators, such as working to improve distress tolerance or emotion regulation skills, as suggested by Hatzenbuehler, Nolen-Hoeksema, and Dovidio (Citation2009). Improving SMM’s general capabilities to manage negative emotions and asserting greater control over their behavior, including leveraging strategies such as motivational interviewing, might be a promising way of approaching efficiently the multiple and interrelated psychosocial needs of this population, as well as skills that may be later generalized to manage problematic substance use and HIV risk behaviors.
Irrespective of whether the field’s intervention development efforts move in the direction of addressing multiple syndemic indicators concurrently, there are several additional intervention design features worthy of consideration. First, efficacy trials should consider carefully inclusion criteria to focus on those at highest risk for poor syndemic and HIV-related outcomes, in order to have enough variability to show effects at post-intervention assessments. Further, given the relatively small effect size estimates, existing interventions may lack sufficient intensity to change syndemic factors or health behaviors in the life contexts of SMM. Shorter and more focused interventions do work for some people but not for everyone, especially the segment of the population dealing with a significant mental health burden. We found stronger intervention effects for individual versus group intervention formats, lending support to the notion that more intensive interventions are needed for syndemic-exposed SMM. There is a dynamic tension between the session format and the number of required sessions to maintain high levels of participant engagement and retention, on the one hand, and optimizing intervention effects, on the other. Further, investigators must balance the need to address multiple mental and physical health needs of high-risk SMM with the preferences of funding agency grant reviewers, who may prioritize efficiency of resources (staff time, number of sessions) over thoroughness.
We share the hope that behavioral interventions can bring about substantial changes in relatively few sessions, although the data do not support this position. Indeed, our findings indicate that the effect size for intervention outcomes related to mental health doubled (.11 vs. .23) for participants receiving nine or more sessions, compared to those receiving eight or fewer. These results suggest that more intensive intervention is likely needed to significantly improve the lives of our research participants. Future intervention trials should be informed by clinical practice, in which clinicians would not expect substantial changes to multiple psychological and behavioral targets in complex, multi-problem clients via brief intervention alone. One way of meeting the diverse needs of syndemically exposed SMM engaging in health risk behaviors could be to use SMART intervention approaches to maximize the tailoring of intervention intensity to participants’ diverse needs (e.g., Lei, Nahum-Shani, Lynch, Oslin, & Murphy, Citation2012).
Relatively few of the trials we reviewed identified their intervention content as uniquely culturally tailored to SMM, and even fewer explicated the process for how they conducted the tailoring. Quantitatively, we observed non-significant stratification effects for SMM cultural tailoring. However, there were relatively few studies contributing to that analysis (13 not tailored, 6 tailored), although a large proportion of the published articles did not report on this variable. There are multiple ways that intervention content could be tailored and more data are needed about the types of tailoring that might make a difference in terms of intervention acceptability, participant retention, and outcomes (Lau, Citation2006). For example, one basic form of tailoring might be omitting or revising heteronormative language on measures or in the intervention content to reduce the chances of systemic invalidation or microaggression. However, it is not clear whether omitting harmful content is enough to make a difference in the participant’s experiences, or whether inclusion of affirming content in terms of SMM identities would motivate greater behavioral change. One noted limitation to the syndemics framework is the lack of attention to identity elements, such as those described in the sexual minority stress model (Meyer, Citation2003), that may be highly salient in the lives of SMM (Pantalone, Puckett, & Gunn, Citation2016) – as well as a limitation of the sexual minority stress model that it lacks sufficient attention to the clusters of psychosocial stressors that are associated with identity-based stress (Rendina et al., Citation2017). We recommend that future trials focused on mental health and health behaviors of SMM should include a tailored focus on the important identity characteristics of the men in terms of sexual orientation and HIV status. An empirical test of this hypothesis might look like a three-arm comparison, i.e., one arm that tests an identity tailored version of the intervention, another that tests a non-tailored version, and then an appropriate control for the stage of intervention development. Further, cultural tailoring for SMM must necessarily take into account the men’s intersectional identities, including attention in intervention content to age cohort diversity and racial/ethnic diversity, among other characteristics (Bogart et al., Citation2017).
An important gap in the reviewed studies is the lack of attention on multi-level predictors of HIV risk. Although it is important to address individual-level predictors of mental health, substance use, and HIV risk behaviors, there is ample evidence that institutional and structural factors strongly impact the health of stigmatized populations, such as SMM. Therefore, we suggest that future intervention efforts with this population include multi-level strategies to address both individual-level barriers and structural barriers, such as housing and the availability of culturally appropriate services, to have greater impact on syndemic factors and HIV risk behaviors (Adimora & Auerbach, Citation2010).
Several efficacious trials tested intervention delivery in the context of primary care, which could be a fruitful way to increase retention and bring evidence-based approaches into the health-care settings where many SMM already are. There is a significant movement toward incorporating mental health service delivery into primary care settings. Our findings point to the potential utility of adding substance use treatment services to that integration as well.
Conclusions
In sum, combination behavioral interventions for SMM that co-target syndemic factors and health behaviors have the potential to effect significant change in the HIV-related health disparities facing this population. Existing interventions in this area show positive effects on mental health and sexual risk behavior outcomes, although we hope that future iterations of the interventions are able to exert a stronger influence on symptom reduction and behavior change. More work is needed to improve the efficacy of ARV adherence interventions, given the null findings we observed in that domain, and there was a disappointing (but perhaps not surprising given the time lag from intervention development to testing to publication) lack of published trials on PrEP adherence interventions – as well as interventions focused on addressing the traumatic sequelae of victimization experiences like CSA and partner abuse tailored to SMM.
One set of findings that seems especially worthy of future attention are the results of the stratification analyses, showing significantly improved efficacy for mental health treatments for SMM were delivered individually, as well as those with a duration of nine or more sessions. These findings confirm what many intervention developers have long known, but what haunts grant reviewers and public health program directors: for some populations and some clusters of intervention targets, it takes careful, individualized attention from a trained therapist over multiple sessions to bring about clinically significant changes. Thus, brief or group-based interventions, which are obviously preferable given the realities of resource scarcity, unfortunately cannot be the only ammunition in our arsenal. Complex patient populations who struggle to address intertwined physical and mental health challenges, while existing in a context of societal marginalization, simply need more time and attention for change to occur.
Our ability to weigh in on SMM-specific cultural tailoring was limited by the lack of details provided by most manuscript authors. We hope that future articles describing interventions specifically developed for SMM will include greater detail on what we know anecdotally: many of the intervention developers have given a lot of attention to cultural tailoring it the design and implementation of the interventions, a fact that was not reflected in many papers we reviewed.
Finally, it will be important to continue to assess these findings over time, in light of trends in society toward greater engagement with technology – as reflected in the development of few, but increasingly, technology-mediated intervention platforms. Intervention technology will continue to change, and so will we. Using fewer human resources and having more automation are laudable goals. However, there may continue to be limits to their effectiveness for some populations or clinical issues of significant complexity.
We commend our colleagues who have been working hard on this line of research and encourage them to continue to do so – we hope, with bolstered confidence about the need for innovation and some ideas for how to move forward in the future.
Supplemental Material
Download Zip (971.2 KB)Acknowledgments
The authors would like to thank other members of the research team who helped with early tasks, such as literature searches and data extraction, and later tasks, such as reference management and help with all elements of the revision process. These individuals include Alison Goldblatt, Elliot Marrow, and Erin Pereida.
Supplementary material
Supplemental data for this article can be accessed on the publisher’s website.
References
- Adimora, A. A., & Auerbach, J. D. (2010). Structural interventions for HIV prevention in the U.S. Journal of Acquired Immune Deficiency Syndromes, 55, S132–S135. doi:10.1097/QAI.0b013e3181fbcb38
- Albarracin, D., Gillette, J., Earl, A., Glasman, L., Durantini, M., & Ho, M. (2005). A test of major assumptions about behavior change: A comprehensive look at the effects of passive and active HIV-prevention interventions since the beginning of the epidemic. Psychological Bulletin, 131, 856–897. doi:10.1037/0033-2909.131.6.856
- Antoni, M. H., Carrico, A. W., Duran, R. E., Spitzer, S., Penedo, F., Ironson, G., … Scheiderman, N. (2006). Randomized clinical trial of cognitive behavioral stress management on human immunodeficiency virus viral load in gay men treated with highly active antiretroviral therapy. Psychosomatic Medicine, 68, 143–151. doi:10.1097/01.psy.0000195749.60049.63
- Avorn, J. (2018). The psychology of clinical decision making—Implications for medication use. New England Journal of Medicine, 378, 689–691. doi:10.1056/NEJMp1714987
- Batchelder, A. W., Carrico, A. W., Acree, M., Hecht, F. M., & Moskowitz, J. T. (2018). Positive and negative self-conscious emotion and transmission risk following HIV diagnosis. AIDS & Behavior, 22, 1496–1502. doi:10.1007/s10461-017-1943-y
- Batchelder, A. W., Moskowitz, J. T., Jain, J., Cohn, M., Earle, M., & Carrico, A. (2019). A novel technology-enhanced internalized stigma and shame intervention for HIV-positive persons with substance use disorders. Cognitive and Behavioral Practice. epub ahead of print. doi:10.1016/j.cbpra.2019.03.001
- Berger, S., Schad, T., von Wyl, V., & Ehlert, U. (2008). Effects of cognitive behavioral stress management on HIV-1 RNA, CD4 cell counts and psychosocial parameters of HIV-infected persons. AIDS, 22, 767–775. doi: 10.1097/QAD.0b013e3282f511dc
- Beyrer, C., Baral, S. D., Walker, D., Wirtz, A. L., Johns, B., & Sifakis, F. (2010). The expanding epidemics of HIV Type 1 among men who have sex with men in low- and middle-income countries: Diversity and consistency. Epidemiologic Reviews, 32, 137–151. doi:10.1093/epirev/mxq011
- Beyrer, C., Sullivan, P., Sanchez, J., Baral, S. D., Collins, C., Wirtz, A. L., … Mayer, K. (2013). The increase in global HIV epidemics in MSM. AIDS, 27, 2665–2678. doi:10.1097/01.aids.0000432449.30239.fe
- Blashill, A. J., Safren, S. A., Wilhelm, S., Jampel, J., Taylor, S. W., O'Cleirigh, C., & Mayer, K. H. (2017). Cognitive behavioral therapy for body image and self-care (CBT-BISC) in sexual minority men living with HIV: A randomized controlled trial. Health Psychology, 36(10), 937–946. doi: 10.1037/hea0000505
- Bogart, L. M., Dale, S. K., Christian, J., Patel, K., Daffin, G. K., Mayer, K. H., & Pantalone, D. W. (2017). Coping with discrimination among HIV-positive Black men who have sex with men. Culture, Health, and Sexuality, 19, 723–737. doi:10.1080/13691058.2016.1258492
- Bogart, L. M., Dale, S. K., Daffin, G. K., Patel, K. N., Klein, D. J., Mayer, K. H., & Pantalone, D. W. (2018). Pilot intervention for discrimination-related coping among HIV-positive Black sexual minority men. Cultural Diversity and Ethnic Minority Psychology, 24, 541–551. doi:10.1037/cdp0000205
- Bogart, L. M., Wagner, G., Galvan, F. H., & Banks, D. (2010). Conspiracy beliefs about HIV are related to antiretroviral treatment nonadherence among African American men with HIV. Journal of Acquired Immune Deficiency Syndromes, 53, 648–655. doi:10.1097/QAI.0b013e3181c57dbc
- Brown, J. K., Vanable, P. A., Bostwick, R. A., & Carey, M. P. (2019). A pilot intervention trial to promote sexual health and stress management among HIV-infected men who have sex with men. AIDS & Behavior, 23(48–59). doi:10.1007/s10461-018-2234-y
- Brown, L. K., Houck, C., Donenberg, G., Emerson, E., Donahue, K., & Misbin, J. (2013). Affect management for HIV prevention with adolescents in therapeutic schools: The immediate impact of Project Balance. AIDS & Behavior, 17, 2773–2780. doi:10.1007/s10461-013-0599-5
- Byrd, K. K., Hou, J. G., Hazen, R., Kirkham, H., Suzuki, S., & Clay, P. G.; for the Patient-centered HIV Care Model Team. (2019). Antiretroviral adherence level necessary for HIV viral suppression using real-world data. Journal of Acquired Immune Deficiency Syndromes, 82, 245–251. epub ahead of print. doi:10.1097/QAI.0000000000002142
- Carrico, A. W., Antoni, M. H., Duran, R. E., Ironson, G., Penedo, F., Fletcher, M. A., … Scheiderman, N. (2006). Reductions in depressed mood and denial coping during cognitive behavioral stress management with HIV-positive gay men treated with HAART. Annals of Behavioral Medicine, 31, 155–164. doi:10.1207/s15324796abm3102_7
- Carrico, A. W., Chesney, M. A., Johnson, M. O., Morin, S. F., Neilands, T. B., & Remien, R.; for the NIMH Health Living Project Team. (2009). Randomized control trial of a cognitive-behavioral intervention for HIV-positive persons. AIDS & Behavior, 13, 555–563. doi:10.1007/s10461-008-9429-6
- Carrico, A. W., Flentje, A., Gruber, V. A., Woods, W. J., Discepola, M. V., Dilworth, S. E., … Siever, M. D. (2014). Community-based harm reduction substance abuse treatment with methamphetamine-using men who have sex with men. Journal of Urban Health, 91, 555–567. doi:10.1007/s11524-014-9870-y
- Carrico, A. W., Gómez, W., Siever, M. D., Discepola, M. V., Dilworth, S. E., & Moskowitz, J. T. (2015a). Pilot randomized controlled trial of an integrative intervention with methamphetamine-using men who have sex with men. Archives of Sexual Behavior, 44, 1861–1867. doi:10.1007/s10508-015-0505-5
- Carrico, A. W., Nation, A., Gomez, W., Sundberg, J., Dilworth, S. E., Johnson, M. O., ..., Dawson Rose, C. (2015b). Pilot trial of an expressive writing intervention with HIV-positive methamphetamine-using men who have sex with men. Psychology of Addictive Behaviors, 29, 277–282. doi: 10.1037/adb0000031
- Carrico, A. W., Zepf, R., Meanley, S., Batchelder, A., & Stall, R. (2016). Critical review. Journal of Acquired Immune Deficiency Syndromes, 73, 299. doi:10.1097/QAI.0000000000001102
- Centers for Disease Control and Prevention. (1981). Pneumocystis. Pneumonia—Los Angeles. Retrieved from https://www.cdc.gov/mmwr/preview/mmwrhtml/june_5.htm
- Centers for Disease Control and Prevention. (2015). HIV infection: Detection, counseling and referral. Retrieved from https://www.cdc.gov/std/tg2015/hiv.htm
- Centers for Disease Control and Prevention. (2017a). Monitoring Selected National HIV Prevention and Care Objectives by Using HIV Surveillance Data—U.S. and 6 Dependent Areas, 2015. Retrieved from http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html
- Centers for Disease Control and Prevention. (2017b). Recommendations for HIV prevention with adults and adolescents with HIV. Retrieved from https://www.cdc.gov/hiv/guidelines/recommendations/personswithhiv.html
- Centers for Disease Control and Prevention. (2018a). Effective interventions: HIV prevention that works. Retrieved from https://effectiveinterventions.cdc.gov/
- Centers for Disease Control and Prevention. (2018b). Estimated HIV Incidence and Prevalence in the U.S., 2010–2015: HIV Surveillance Supplemental Report 2018. Retrieved from http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html
- Centers for Disease Control and Prevention. (2018c). HIV among transgender people. Retrieved from https://www.cdc.gov/hiv/group/gender/transgender/index.html
- Centers for Disease Control and Prevention. (2018d). HIV among youth. Retrieved from https://www.cdc.gov/hiv/group/age/youth/index.html
- Centers for Disease Control and Prevention. (2018e). HIV in the U.S.: At a glance. Retrieved from https://www.cdc.gov/hiv/statistics/overview/ataglance.html
- Centers for Disease Control and Prevention. (2018f). U.S. Public Health Service: Pre-exposure prophylaxis for the prevention of HIV infection in the U.S.—2017 update: A clinical practice guideline. Retrieved from https://www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2017.pdf
- Chinn, S. (2000). A simple method for converting an odds ratio to effect size for use in meta-analysis. Statistics in Medicine, 19, 3127–3131. doi:10.1002/1097-0258(20001130)19:22<3127::AID-SIM784>3.0.CO;2-M
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Earlbaum Associates.
- Cohen, M. S., Chen, Y. Q., McCauley, M., Gamble, T., Hosseinipour, M. C., Kumarasamy, N., … Godbole, S. V. (2011). Prevention of HIV-1 infection with early antiretroviral therapy. New England Journal of Medicine, 365, 493–505. doi:10.1056/NEJMoa1105243
- Crepaz, N., Tungol-Ashmon, M. V., Higa, D. H., Vosburgh, W., Mullins, M. M., Barham, T., … Lyles, C. M. (2014). A systematic review of interventions for reducing HIV risk behaviors among people living with HIV in the U.S., 1988-2012. AIDS, 28, 633–656. doi:10.1097/qad.0000000000000108
- Cuijpers, P., Weitz, E., Cristea, I. A., & Twisk, J. (2017). Pre-post effect sizes should be avoided in meta-analyses. Epidemiology and Psychiatric Sciences, 26, 364–368. doi:10.1017/S2045796016000809
- DiNenno, E. A., Prejean, J., Irwin, K., Delaney, K. P., Bowles, K., Martin, T., … Lansky, A. (2017). Recommendations for HIV screening of gay, bisexual, and other men who have sex with men—U.S., 2017. MMWR. Morbidity and Mortality Weekly Report, 66, 830. doi:10.15585/mmwr.mm6631a3
- Dunn, C., Deroo, L., & Rivara, F. P. (2001). The use of brief interventions adapted from motivational interviewing across behavioral domains: A systematic review. Addiction, 96, 1725–1742. doi:10.1080/09652140120089481
- Duval, S., & Tweedie, R. (2000). Trim and fill: A simple funnel plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics, 56, 455–463. doi:10.1111/j.0006-341X.2000.00455.x
- Earnshaw, V. A., Bogart, L. M., Dovidio, J. F., & Williams, D. R. (2013). Stigma and racial/ethnic HIV disparities: Moving toward resilience. American Psychologist, 68, 225–236. doi:10.1037/a0032705
- Egger, M., Smith, G. D., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. The BMJ, 315, 629–634. doi:10.1136/bmj.315.7109.629
- El-Sadr, W. M., Mayer, K. H., Rabkin, M., & Hodder, S. L. (2019). AIDS in America—Back in the headlines at long last. New England Journal of Medicine, 380, 1985–1987. doi:10.1056/NEJMp1904113
- Esposito-Smythers, C., Brown, L. K., Wolff, J., Xu, J., Thornton, S., & Tidey, J. (2014). Substance abuse treatment for HIV infected young people: An open pilot trial. Journal of Substance Abuse Treatment, 46, 244–250. doi:10.1016/j.jsat.2013.07.008
- Grov, C., Rendina, H. J., & Parsons, J. T. (2014). Comparing three cohorts of MSM sampled via sex parties, bars/ clubs, and Craigslist.org: Implications for researchers and providers. AIDS Education and Prevention, 26, 362–382. doi:10.1521/aeap.2014.26.4.362
- Günthard, H. F., Saag, M. S., Benson, C. A., Del Rio, C., Eron, J. J., Gallant, J. E., … Gandhi, R. T. (2016). Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2016 recommendations of the international antiviral society–USA panel. Journal of the American Medical Association, 316, 191–210. doi:10.1001/jama.2016.8900
- Halkitis, P. N., Wolitski, R. J., & Millett, G. A. (2013). A holistic approach to addressing HIV infection disparities in gay, bisexual, and other men who have sex with men. American Psychologist, 68, 261–273. doi:10.1037/a0032746
- Hart, T. A., Stratton, N., Coleman, T. A., Wilson, H. A., Simpson, S. H., Julien, R. E., … Adam, B. D. (2016). A pilot trial of a sexual health counseling intervention for HIV-positive gay and bisexual men who report anal sex without condoms. PLoS ONE, 11, e0152762. doi: 10.1371/journal.pone.0152762
- Hatzenbuehler, M. L., Nolen-Hoeksema, S., & Dovidio, J. (2009). How does stigma “get under the skin”?: The mediating role of emotion regulation. Psychological Science, 20, 1282–1289. doi:10.1111/j.1467-9280.2009.02441.x
- Hedges, L. V., & Olkin, I. (2014). Statistical methods for meta-analysis. Orlando, FL: Academic Press.
- Hedges, L. V., & Vevea, J. L. (1998). Fixed-and random-effects models in meta-analysis. Psychological Methods, 3, 486–504. doi:10.1037/1082-989X.3.4.486
- Hess, K. L., Hu, X., Lansky, A., Mermin, J., & Hall, H. I. (2017). Lifetime risk of a diagnosis of HIV infection in the U.S. Annals of Epidemiology, 27, 238–243. doi:10.1016/j.annepidem.2017.02.003
- Higgins, J. P., & Green, S. (2011). Cochrane handbook for systematic reviews of interventions (Vol. 4). Chichester, UK: John Wiley & Sons.
- Horvath, K. J., & Bauermeister, J. A. (2017). eHealth literacy and intervention tailoring impacts the acceptability of a HIV/STI testing intervention and sexual decision making among young gay and bisexual men. AIDS Education and Prevention, 29, 14–23. doi:10.1521/aeap.2017.29.1.14
- Horvath, K. J., Iantaffi, A., Swinburne-Romine, R., & Bockting, W. (2014). A comparison of mental health, substance use, and sexual risk behaviors between rural and non-rural transgender persons. Journal of Homosexuality, 61, 1117–1130. doi:10.1080/00918369.2014.872502
- Joint United Nations Programme on HIV/AIDS (UNAIDS). (2017). Ending AIDS: Progress towards the 90- 90-90targets. Global AIDS Update. Retrieved from https://www.unaids.org/sites/default/files/media_asset/Global_AIDS_update_2017_en.pdf
- Kahler, C. W., Pantalone, D. W., Mastroleo, N. R., Liu, T., Bove, G., Ramratnam, B., … Mayer, K. H. (2018). Motivational interviewing with personalized feedback to reduce alcohol use in HIV-infected men who have sex with men: A randomized trial. Journal of Consulting and Clinical Psychology, 86, 645–656. doi:10.1037/ccp0000322
- Kanters, S., Park, J. J., Chan, K., Socias, M. E., Ford, N., Forrest, J. I., … Mills, E. J. (2017). Interventions to improve adherence to antiretroviral therapy: A systematic review and network meta-analysis. The Lancet HIV, 4, e31–e40. doi:10.1016/S2352-3018(16)30206-5
- Kennard, B., Brown, L. K., Hawkins, L., Risi, A., Radcliffe, J., Emslie, G., … Thornton, S. (2014). Development and implementation of health and wellness CBT for individuals with depression and HIV. Cognitive Behavioral Practice, 21, 237–246. doi:10.1016/j.cbpra.2013.07.003
- Kurtz, S. P., Stall, R. D., Buttram, M. E., Surratt, H. L., & Chen, M. (2013). A randomized trial of a behavioral intervention for high risk substance using MSM. AIDS & Behavior, 17, 2914–2926. doi:10.1007/s10461-013-0531-z
- Landovitz, R. J., Fletcher, J. B., Inzhakova, G., Lake, J. E., Shoptaw, S., & Reback, C. J. (2012). A novel combination HIV prevention strategy: Post-exposure prophylaxis with contingency management for substance abuse treatment among methamphetamine-using men who have sex with men. AIDS Patient Care and STDs, 26, 320–328. doi:10.1089/apc.2011.0432
- Landovitz, R. J., Fletcher, J. B., Shoptaw, S., & Reback, C. J. (2015). Contingency management facilitates the use of postexposure prophylaxis among stimulant-using men who have sex with men. Open Forum Infectious Diseases, 2(ofu114). doi:10.1093/ofid/ofu114
- Lau, A. S. (2006). Making the case for selective and directed cultural adaptations of evidence‐based treatments: Examples from parent training. Clinical Psychology: Science and Practice, 13, 295–310. doi:10.1111/j.1468-2850.2006.00042.x
- Lei, H., Nahum-Shani, I., Lynch, K., Oslin, D., & Murphy, S. A. (2012). A “SMART” design for building individualized treatment sequences. Annual Review of Clinical Psychology, 8, 21–48. doi:10.1146/annurev–clinpsy–032511–143152
- Lelutiu-Weinberger, C., Pachankis, J. E., Gamarel, K. E., Surace, A., Golub, S. A., & Parsons, J. T. (2015). Feasibility, acceptability, and preliminary efficacy of a live-chat social media intervention to reduce HIV risk among young men who have sex with men. AIDS & Behavior, 19, 1214–1227. doi:10.1007/s10461-014-0911-z
- Li, Z., Purcell, D. W., Sansom, S. L., Hayes, D., & Hall, H. I. (2019). Vital signs: HIV transmission along the continuum of care—U.S., 2016. Morbidity and Mortality Weekly Report, 68, 267–272. doi:10.15585/mmwr.mm6811e1
- Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Loannidis, J. P. A., … Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLOS Medicine, 6, e1000100. doi:10.1371/journal.pmed.1000100
- Mansergh, G., Koblin, B. A., McKirnan, D. J., Hudson, S. M., Flores, S. A., Wiegand, R. E., … Colfax, G. N. (2010). An intervention to reduce HIV risk behavior of substance-using men who have sex with men: A two-group randomized trial with a nonrandomized third group. PLoS Medicine, e1000329. doi:10.1371/journal.pmed.1000329
- Maulsby, C., Charles, V., Kinsky, S., Riordan, M., Jain, K., & Holtgrave, D. (2015). Positive charge: Filling the gaps in the U.S. HIV continuum of care. AIDS & Behavior, 19, 2097–2107. doi:10.1007/s10461-015-1015-0
- Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129, 674–697. doi:10.1037/0033-2909.129.5.674
- Mimiaga, M. J., Noonan, E., Donnell, D., Safren, S. A., Koenen, K. C., Gortmaker, S., … Mayer, K. H. (2009). Childhood sexual abuse is highly associated with HIV risk-taking behavior and infection among MSM in the EXPLORE Study. Journal of Acquired Immune Deficiency Syndromes, 51, 340–348. doi:10.1097/QAI.0b013e3181a24b38
- Mimiaga, M. J., O’Cleirigh, C., Biello, K. B., Robertson, A. M., Safren, S. A., Coates, T. J., … Mayer, K. H. (2015). The effect of psychosocial syndemic production on 4-year HIV incidence and risk behavior in a large cohort of sexually active men who have sex with men. Journal of Acquired Immune Deficiency Syndromes, 68, 329–336. doi:10.1097/QAI.0000000000000475
- Mimiaga, M. J., Reisner, S. L., Pantalone, D. W., O’Cleirigh, C., Mayer, K. H., & Safren, S. A. (2012). A pilot trial of integrated behavioral activation and sexual risk reduction counseling for HIV uninfected men who have sex with men abusing crystal methamphetamine. AIDS Patient Care and STDs, 26, 681–693. doi:10.1089/apc.2012.0216
- Morgenstern, J., Bux, D. A., Jr., Parsons, J. T., Hagman, B. T., Wainberg, M. L., & Irwin, T. W. (2009). Randomized trial to reduce club drug use and HIV risk behaviors among men who have sex with men. Journal of Consulting and Clinical Psychology, 77, 645–656. doi:10.1037/a0015588
- Muessig, K. E., LeGrand, S., Horvath, K. J., Bauermeister, J. A., & Hightow-Weidman, L. B. (2017). Recent mobile health interventions to support medication adherence among HIV-positive MSM. Current Opinion in HIV and AIDS, 12, 432–441. doi:10.1097/coh.0000000000000401
- Mustanski, B., Parsons, J. T., Sullivan, P. S., Madkins, K., Rosenberg, E., & Swann, G. (2018). Biomedical and behavioral outcomes of Keep It Up!: An eHealth HIV prevention program RCT. American Journal of Preventive Medicine, 55, 151–158. doi:10.1016/j.amepre.2018.04.026
- Nunn, A. S., Brinkley-Rubinstein, L., Oldenburg, C. E., Mayer, K. H., Mimiaga, M., Patel, R., & Chan, P. A. (2017). Defining the HIV pre-exposure prophylaxis care continuum. AIDS, 31, 731–734. doi:10.1097/QAD.0000000000001385
- O’Cleirigh, C. M., Pantalone, D. W., Batchelder, A. W., Hatzenbuehler, M. L., Marquez, S., Grasso, C., … Mayer, K. H. (2018). Co-occurring psychosocial problems predict increased health care costs and utilization among gay and bisexual men. Journal of Behavioral Medicine, 41, 450–457. doi:10.1007/s10865-018-9913-z
- O’Cleirigh, C. M., Safren, S. A., Taylor, S. W., Goshe, B. M., Bedoya, C. A., Marquez, S. M., … Shipherd, J. C. (2019). Cognitive behavioral therapy for trauma and self‑care (CBT‑TSC) in men who have sex with men with a history of childhood sexual abuse: A randomized controlled trial. AIDS & Behavior. epub ahead of print. doi:10.1007/s10461-019-02482-z
- Orwin, R. (1983). A fail-safe N for effect size in meta-analysis. Journal of Educational Statistics, 8, 157–159. doi:10.2307/1164923
- Pachankis, J. E. (2014). Uncovering clinical principles and techniques to address minority stress, mental health, and related health risks among gay and bisexual men. Clinical Psychology: Science and Practice, 21, 313–330. doi:10.1111/cpsp.12078
- Pachankis, J. E., Cochran, S. D., & Mays, V. M. (2015). The mental health of sexual minority adults in and out of the closet: A population-based study. Journal of Consulting and Clinical Psychology, 83, 890–901. doi:10.1037/ccp0000047
- Pachankis, J. E., Hatzenbuehler, M. L., Rendina, H. J., Safren, S. A., & Parsons, J. T. (2015). LGB-affirmative cognitive-behavioral therapy for young adult gay and bisexual men: A randomized controlled trial of a transdiagnostic minority stress approach. Journal of Consulting and Clinical Psychology, 83, 875–889. doi:10.1037/ccp0000037
- Pantalone, D. W., Puckett, J. A., & Gunn, H. A. (2016). Psychosocial factors and HIV prevention for gay, bisexual, and other men who have sex with men. Social and Personality Psychology Compass, 2, 109–122. doi:10.1111/spc3.12234
- Pantalone, D. W., Valentine, S. E., Woodward, E. N., & O’Cleirigh, C. M. (2018). Syndemic indicators predict poor medication adherence and increased health care utilization for urban HIV-positive sexual minority men. Journal of Gay and Lesbian Mental Health, 22, 71–87. doi:10.1080/19359705.2017.1389794
- Parsons, J. T., Golub, S. A., Rosof, E., & Holder, C. (2007). Motivational interviewing and cognitive-behavioral intervention to improve HIV medication adherence among hazardous drinkers: A randomized controlled trial. Journal of Acquired Immune Deficiency Syndromes, 46, 443–450. doi:10.1097/QAI.0b013e318158a461
- Parsons, J. T., John, S. A., Millar, B. M., & Starks, T. J. (2018). Testing the efficacy of combined motivational interviewing and cognitive behavioral skills training to reduce methamphetamine use and improve HIV medication adherence among HIV-positive gay and bisexual men. AIDS & Behavior, 22, 2674–2686. doi:10.1007/s10461-018-2086-5
- Parsons, J. T., Lelutiu-Weinberger, C., Botsko, M., & Golub, S. A. (2014). A randomized controlled trial utilizing motivational interviewing to reduce HIV risk and drug use in young gay and bisexual men. Journal of Consulting and Clinical Psychology, 82, 9–18. doi:10.1037/a0035311
- Parsons, J. T., Rendina, H. J., Moody, R. L., Gurung, S., Starks, T. J., & Pachankis, J. E. (2017). Feasibility of an emotion regulation intervention to improve mental health and reduce HIV transmission risk behaviors for HIV-positive gay and bisexual men with sexual compulsivity. AIDS & Behavior, 21, 1540–1549. doi:10.1007/s10461-016-1533-4
- Plöderl, M., & Tremblay, P. (2015). Mental health of sexual minorities: A systematic review. International Review of Psychiatry, 27, 367–385. doi:10.3109/09540261.2015.1083949
- Prescott, T. L., Phillips, G., II, DuBois, L. Z., Bull, S. S., Mustanski, B., & Ybarra, M. L. (2016). Reaching adolescent gay, bisexual, and queer men online: Development and refinement of a national recruitment strategy. Journal of Medical Internet Research, 18, e200. doi:10.2196/jmir.5602
- Reback, C. J., & Fletcher, J. B. (2017). Outcomes from a homegrown HIV prevention program for extremely high-risk, substance-using men who have sex with men with multiple health disparities. Journal of Gay and Lesbian Social Services, 29, 167–181. doi:10.1080/10538720.2017.1296394
- Refugio, O. N., Kimble, M. M., Silva, C. L., Lykens, J. E., Bannister, C., & Klausner, J. D. (2019). Brief report: PrEPTECH: A telehealth-based initiation program for HIV pre-exposure prophylaxis in young men of color who have sex with men: A pilot study of feasibility. Journal of Acquired Immune Deficiency Syndromes, 80, 40–45. doi:10.1097/QAI.0000000000001873
- Reisner, S. L., O’Cleirigh, C., Hendriksen, E. S., McLain, J., Ebin, J., Lew, K., … Mimiaga, M. J. (2011). “40 & forward”: Preliminary evaluation of a group intervention to improve mental health outcomes and address HIV sexual risk behaviors among older gay and bisexual men. Journal of Gay & Lesbian Social Services, 23, 523–545. doi:10.1080/10538720.2011.611113
- Rendina, H. J., Gamarel, K. E., Pachankis, J. E., Ventuneac, A., Grov, C., & Parsons, J. T. (2017). Extending the minority stress model to incorporate HIV-positive gay and bisexual men’s experiences: A longitudinal examination of mental health and sexual risk behavior. Annals of Behavioral Medicine, 51, 147–158. doi:10.1007/s12160-016-9822-8
- Risher, K., Mayer, K., & Beyrer, C. (2015). The HIV treatment cascade in men who have sex with men, people who inject drugs and sex workers. Current Opinion in HIV and AIDS, 10, 420–429. doi:10.1097/COH.0000000000000200
- Rotheram-Borus, M. J., Swendeman, D., Comulada, W. S., Weiss, R. E., Lee, M., & Lightfoot, M. (2004). Prevention for substance-using HIV-positive young people: Telephone and in-person delivery. Journal of Acquired Immune Deficiency Syndromes, 37, S68–S77. doi:10.1097/01.qai.0000140604.57478.67
- Safren, S. A., Bedoya, C. A., O’Cleirigh, C., Biello, K. B., Pinkston, M. M., Stein, M. D., … Mayer, K. H. (2016). Cognitive behavioural therapy for adherence and depression in patients with HIV: A three-arm randomised controlled trial. The Lancet HIV, 3, e529–e538. doi:10.1016/s2352-3018(16)30053-4
- Safren, S. A., Blashill, A. J., & O’Cleirigh, C. M. (2011). Promoting the sexual health of MSM in the context of comorbid mental health problems. AIDS and Behavior, 15(1), 30–34. doi:10.1007/s10461-011-9898-x
- Safren, S. A., O’Cleirigh, C., Tan, J. Y., Raminani, S. R., Reilly, L. C., Otto, M. W., & Mayer, K. H. (2009). A randomized controlled trial of cognitive behavioral therapy for adherence and depression (CBT-AD) in HIV-infected individuals. Health Psychology, 28, 1–10. doi:10.1037/a0012715
- Safren, S. A., O’Cleirigh, C. M., Skeer, M., Elsesser, S. A., & Mayer, K. H. (2013). Project ENHANCE: A randomized controlled trial of an individualized HIV prevention intervention for HIV-infected men who have sex with men conducted in a primary care setting. Health Psychology, 32, 171–179. doi:10.1037/a0028581
- Safren, S. A., Otto, M. W., Worth, J. L., Salomon, E., Johnson, W., Mayer, K., & Boswell, S. (2001). Two strategies to increase adherence to HIV antiretroviral medication: Life-Steps and medication monitoring. Behaviour Research and Therapy, 39, 1151–1162. doi:10.1016/S0005-7967(00)00091-7
- Santos, G. M., Coffin, P. O., Vittinghoff, E., DeMicco, E., Das, M., Matheson, T., … Dilley, J. W. (2014). Substance use and drinking outcomes in personalized cognitive counseling randomized trial for episodic substance-using men who have sex with men. Drug and Alcohol and Dependence, 138, 234–239. doi:10.1016/j.drugalcdep.2014.02.015
- Schulz, K. F., Altman, D. G., & Moher, D. (2010). CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMC Medicine, 8, 18. doi:10.1186/1741-7015-8-18
- Shoptaw, S., Reback, C. J., Larkins, S., Wang, P. C., Rotheram-Fuller, E., Dang, J., & Yang, X. (2008). Outcomes using two tailored behavioral treatments for substance abuse in urban gay and bisexual men. Journal of Substance Abuse Treatment, 35, 285–293. doi:10.1016/j.jsat.2007.11.004
- Shoptaw, S., Reback, C. J., Peck, J. A., Yang, X., Rotheram-Fuller, E., Larkins, S., … Hucks-Ortiz, C. (2005). Behavioral treatment approaches for methamphetamine dependence and HIV-related sexual risk behaviors among urban gay and bisexual men. Drug and Alcohol Dependence, 78, 125–134. doi:10.1016/j.drugalcdep.2004.10.004
- Sikkema, K. J., Watt, M. H., Drabkin, A. S., Meade, C. S., Hansen, N. B., & Pence, B. W. (2010). Mental health treatment to reduce HIV transmission risk behavior: A positive prevention model. AIDS & Behavior, 14, 252–262. doi:10.1007/s10461-009-9650-y
- Silapaswan, A., Krakower, D., & Mayer, K. H. (2017). Pre-exposure prophylaxis: A narrative review of provider behavior and interventions to increase PrEP implementation in primary care. Journal of General Internal Medicine, 32, 192–198. doi:10.1007/s11606-016-3899-4
- Singer, M. (1996). A dose of drugs, a touch of violence, a case of AIDS: Conceptualizing the SAVA syndemic. Free Inquiry in Creative Sociology, 24, 99–110.
- Smith, N. G., Hart, T. A., Kidwai, A., Vernon, J. R. G., Blais, M., & Adam, B. (2017). Results of a pilot study to ameliorate psychological and behavioral outcomes of minority stress among young gay and bisexual men. Behavior Therapy, 48, 664–677. doi:10.1016/j.beth.2017.03.005
- Stall, R., Mills, T. C., Williamson, J., Hart, T., Greenwood, G., Paul, J., … Catania, J. A. (2003). Association of co-occurring psychosocial health problems and increased vulnerability to HIV/AIDS among urban men who have sex with men. American Journal of Public Health, 93, 939–942. doi:10.2105/AJPH.93.6.939
- Sullivan, P. S., Carballo-Diéguez, A., Coates, T., Goodreau, S. M., McGowan, I., Sanders, E. J., … Sanchez, J. (2012). Successes and challenges of HIV prevention in men who have sex with men. The Lancet, 380, 388–399. doi:10.1016/S0140-6736(12)60955-6
- Suthar, A. B., Ford, N., Bachanas, P. J., Wong, V. J., Rajan, J. S., Saltzman, A. K., … Baggaley, R. C. (2013). Towards universal voluntary HIV testing and counselling: A systematic review and meta-analysis of community-based approaches. PLoS Medicine, 10, e1001496. doi:10.1371/journal.pmed.1001496
- Tsai, A. C., & Burns, B. F. (2015). Syndemics of psychosocial problems and HIV risk: A systematic review of empirical tests of the disease interaction concept. Social Science & Medicine, 139, 26–35. doi:10.1016/j.socscimed.2015.06.024
- Tso, L. S., Tang, W., Li, H., Yan, H. Y., & Tucker, J. D. (2016). Social media interventions to prevent HIV: A review of interventions and methodological considerations. Current Opinions in Psychology, 9, 6–10. doi:10.1016/j.copsyc.2015.09.019
- U=U taking off in 2017. (2017, November 01). The Lancet HIV, 4, e475. doi:10.1016/S2352-3018(17)30183-2
- Velasquez, M. M., von Sternberg, K., Johnson, D. H., Green, C., Carbonari, J. P., & Parsons, J. T. (2009). Reducing sexual risk behaviors and alcohol use among HIV-positive men who have sex with men: A randomized clinical trial. Journal of Consulting and Clinical Psychology, 77, 657–667. doi:10.1037/a0015519
- Viechtbauer, W. (2007). Confidence intervals for the amount of heterogeneity in meta-analysis. Statistics in Medicine, 26(1), 37–52. doi:10.1002/(ISSN)1097-0258
- Williams Institute. (2014). Best practices for asking questions to identify transgender and other gender minority respondents on population-based surveys: From the GenIUSS Group. Retrieved from https://williamsinstitute.law.ucla.edu/research/census-lgbt-demographics-studies/geniuss-report-sept-2014/.
- Williams, J. K., Glover, D. A., Wyatt, G. E., Kisler, K., Liu, H., & Zhang, M. (2013). A sexual risk and stress reduction intervention designed for HIV-positive bisexual African American men with childhood sexual abuse histories. American Journal of Public Health, 103, 1476–1484. doi:10.2105/ajph.2012.301121
- Williams, J. K., Wyatt, G. E., Rivkin, I., Ramamurthi, H. C., Li, X., & Liu, H. (2008). Risk reduction for HIV-positive African American and Latino men with histories of childhood sexual abuse. Archives of Sexual Behavior, 37, 763–772. doi:10.1007/s10508-008-9366-5
- Woodward, E. N., Banks, R. J., Marks, A. K., & Pantalone, D. W. (2017). Identifying resilience resources for HIV prevention among sexual minority men: A systematic review. AIDS & Behavior, 21, 2860–2873. doi:10.1007/s10461-016-1608-2
- Wray, T. B., Kahler, C. W., Simpanen, E. M., & Operario, D. (2019). A preliminary randomized controlled trial of Game Plan, a web application to help men who have sex with men reduce their HIV risk and alcohol use. AIDS & Behavior, 23, 1668–1679. doi:10.1007/s10461-019-02396-w
- Wu, E., El-Bassel, N., McVinney, L. D., Hess, L., Remien, R. H., Charania, M., & Mansergh, G. (2011). Feasibility and promiseof a couple-based HIV/STI preventive intervention for methamphetamine-using, Black men who have sex with men. AIDS & Behavior, 15, 1745–1754. doi:10.1007/s10461-011-9997-8
- Zule, W. A., Poulton, W. E., Coomes, C. M., Mansergh, G., Charania, M., Wechsberg, W. M., & Jones, H. E. (2012). Results of a pilot study to reduce methamphetamine use and sexual risk behaviors among methamphetamine-using men who have sex with men (MSM) not currently in treatment. Journal of Psychoactive Drugs, 44, 351–358. doi:10.1080/02791072.2012.736794