
ABSTRACT
As people age, their sexual activity, including sexual and relationship satisfaction, may change due to the onset of health and sexual difficulties and the activation of internalized ageist sexual stereotypes. We studied whether ageist sexual stereotypes were relevant for the importance of sex for people aged 50+ and how sexual and relationship satisfaction are interlinked with health and sexual difficulties when ageist sexual stereotypes are considered. Data for the network analysis were collected from a sample of 897 Czechs and Slovaks aged 50–96 (52% men, mean age = 62.01). Two models were analyzed – with and without the inclusion of ageist sexual stereotypes. The findings indicated that ageist sexual stereotypes play an important role in the sexuality of women and men aged 50 + .The fewer ageist sexual stereotypes people had, the less sexual difficulties they reported and the more they perceived sex as important. The inclusion of stereotypes into the models, however, weakened the negative link between sexual difficulties and the importance of sex for both women and men. These findings show that the effect of ageist sexual stereotypes are likely complex in the sexual lives of people aged 50 +.
Introduction
Sexual activity is subject to many challenges and changes after the age of 50 (DeLamater et al., Citation2019). One of them is a decrease in the frequency of sex (Gillespie, Citation2017; Lindau et al., Citation2007). This decline is mostly related to the absence of a sexual partner, the onset of sexual health difficulties, and internalized ageist sexual stereotypes that may contribute to the decrease of sexual activity (i.e., later-life sex is needless or inappropriate; DeLamater, Citation2012; Erens et al., Citation2019; Freak-Poli & Malta, Citation2020, Gore-Gorszewska, Citation2021; Ševčíková & Sedláková, Citation2020; Syme & Cohn, Citation2021; Syme et al., Citation2019). This set of changes may put a strain on sexual and partnered lives (e.g., dissatisfaction with sexual frequency and relationship dissatisfaction; Geerkens et al., Citation2020; Lodge & Umberson, Citation2012; Ševčíková et al., Citation2021). At the same time, sexual activity in later life is recognized as contributing toward better mental and physical health and it is associated with a higher reported quality of life and relationships (Štulhofer et al., Citation2019). Therefore, the focus of the present study was to examine how challenges in sexual life are related to ageist sexual stereotypes and satisfaction with sex and relationships.
Ageist Stereotypes
Ageist sexual stereotypes are beliefs based on a person’s age, in this case in relation to sexual activity, desirable behavior, or expression. These may include prejudices and negative perceptions concerning sexual expression and myths regarding the sexual life of older persons (e.g., a lack of sexual desire or physical unatractiveness; Gewirtz-Meydan et al., Citation2018; Hall et al., Citation1982; White, Citation1998). According to Levy’s stereotype embodiment theory (Citation2009), ageist stereotypes are unconsciously internalized throughout the lifespan and gain salience if they are self-relevant. For example, Syme and Cohn (Citation2021) found how internalized stereotypes become salient in the sex lives of middle-aged and older adults. Specifically, their study revealed that the acceptance of the stereotype that people lack sexual needs as they get older was associated with reduced sexual behavior, even when controlling for other factors, such as age and health. Furthermore, the activation of ageist stereotypes in older adults who face health difficulties may manifest via adherence of the belief that altering their behavior or addressing the situation in other ways is pointless (Wurm et al., Citation2013). Specifically, accepting the stereotype that later-life changes in sexual functioning are an inevitable part of the aging process discourages adults from seeking medical help or undertaking other actions to maintain their sex life (e.g., Hinchliff & Gott, Citation2004; Sinković & Towler, Citation2019; Tinetti et al., Citation2018). Although partnered sex may still be valued in a later-life relationship (Geerkens et al., Citation2020; Hinchliff et al., Citation2020; Štulhofer et al., Citation2020, internalized ageist sexual stereotypes can affect sexual activity and strategies (e.g., refraining from seeking medical help, resigning from sexual activities; Gore-Gorszewska, Citation2020; Gott & Hinchliff, Citation2003a).
Ageist Sexual Stereotypes in Relation to Coping Strategies
The later-life onset of health and sexual problems can be challenging and accompanied by frustration and stress, especially when some couples tend to consider penetrative sex as the only legitimate form of sex (Gore-Gorszewska, Citation2021; Gore-Gorszewska & Ševčíková, Citation2022; Lodge & Umberson, Citation2012; Ševčíková et al., Citation2021; Štulhofer et al., Citation2020). In addition, maintaining sexual activities and interests typical for a younger age to alleviate one’s own or one’s partner’s dissatisfaction with sexual frequency can be difficult and demanding (Choi, Citation2020). In these cases, some adults aged 50+ experience tension and emotional discomfort (Heidrich & Powwattana, Citation2004; Lapp & Spaniol, Citation2016), which results in diverse coping strategies. Some may conform to selected ageist sexual stereotypes.
For example, in the context of dealing with sexual difficulties and reduced sexual frequency, some older adults cope by reframing the meaning of sex (Connor et al., Citation2020; Freak-Poli & Malta, Citation2020). Alternative sexual expression, such as kissing, hugging, stroking, or oral sex, can replace penetrative sex when it is no longer possible (Freak-Poli & Malta, Citation2020; Gore-Gorszewska & Ševčíková, Citation2022; Lodge & Umberson, Citation2012; Tetley et al., Citation2018; Waite et al., Citation2009), contributing to the maintenance of sexual and relationship satisfaction (Connor et al., Citation2020; Gillespie, Citation2017; Rahn et al., Citation2020; Rosen et al., Citation2016; Tetley et al., Citation2018). Similarly, a study by Forbes et al. (Citation2017) suggested that, as people age, they acquire skills and knowledge (described as sexual wisdom), which can buffer the negative changes in their sex lives and help maintain the quality of their sex. Existing research highlights that preserving sexual satisfaction through the use of non-penetrative sexual activities can, to some extent, contribute to later-life relationship satisfaction (Rosen et al., Citation2016; Tetley et al., Citation2018; Wassersug et al., Citation2017).
Apart from reorientating from penetrative sex toward non-penetrative sexual activities, another way to manage sexual difficulties and the subsequent potential decreases in relationship and sexual satisfaction is to reassess the importance of sex and redefine the role of sex such that it no longer remains a mandatory aspect of a relationship at older ages (Gott & Hinchliff, Citation2003b; Lodge & Umberson, Citation2012; Ševčíková & Sedláková, Citation2020; Towler et al., Citation2021, Citation2022). For instance, treating sexual changes as a natural part of aging was found to correspond with the narratives of less distress, and even liberation, in studies on adults aged 50+ (e.g., Gott & Hinchliff, Citation2003b; Ševčíková & Sedláková, Citation2020; Sinković & Towler, Citation2019). This suggests that the activation of some internalized ageist sexual beliefs, such as the notion that “sex is no longer a component of older age,” may reduce dissatisfaction with the decreasing frequency of sexual activity. This assumption has support in prior research where the adoption of ageist stereotypes was found to emerge as a response to the heightened stress of increasing age (Wettstein et al., Citation2021), which indicates that ageist stereotypes may be activated to reduce stress. In this respect, older adults tend to disengage from stressful and emotionally challenging situations in response to diminishing bio-psycho-social resources (Carstensen et al., Citation2011; Charles, Citation2010; Reed et al., Citation2014). The activation of selected ageist stereotypes could operate as an attempt for older adults to distance themselves from strains (e.g., sexual difficulties). Alternatively, changes in sexual behavior can be understood from the perspective of transformative change (affirmative aging; Sandberg, Citation2013; Towler et al., Citation2021), which is described as accepting the changes as a natural part of life. However, there is a thin and blurred line between affirmative aging and internalized ageist sexual stereotypes.
Additionally, there are noticeable gender differences in dealing with sexual difficulties. Women and men differ in the physiological nature and subsequent treatment of sexual difficulties. Specifically, addressing some sexual difficulties may be easier for women compared to men (e.g., treatment of vaginal dryness with lubricants). In many cases, female issues do not prevent sexual intercourse (e.g., inability to reach orgasm), even though they may impair pleasure (Štulhofer et al., Citation2019; Træen et al., Citation2019). Sexual difficulties are more often recognized and discussed in older men, who tend to avoid addressing them, primarily due to shame and failure to meet the standards of heteronormativity and masculinity (e.g., being able to engage in penetrative sex; Ayalon et al., Citation2021; Fileborn et al., Citation2017; Geerkens et al., Citation2020; Hinchliff et al., Citation2020; Lodge & Umberson, Citation2012; Shen, Citation2019). Although this tendency could also be present in some women, aging women who are likely to be in a relationship with older partners, tend to prioritize maintaining the relationship over having a (satisfying) sex life (Lodge & Umberson, Citation2012; Ševčíková & Sedláková, Citation2020; Towler et al., Citation2022). These findings suggest that older heterosexual women may be more likely to tolerate their own or their partner’s sexual difficulties rather than vice versa, and this may lead to the different effects of experiencing sexual difficulties on sexual and relationship satisfaction in women and in men (Fischer et al., Citation2021; Gray et al., Citation2019; Kontula & Haavio-Mannila, Citation2009; Lindau et al., Citation2007).
Research Aim
As previously mentioned, studies have found close connections between poor health, sexual difficulties, and lower sexual frequency that may negatively affect satisfaction with the frequency of sex and the relationship in some women and men aged 50+ (Erens et al., Citation2019; Freak-Poli & Malta, Citation2020; Gillespie, Citation2017; Rahn et al., Citation2020; Rosen et al., Citation2016). Based on the existing findings, we assumed that experiencing sexual difficulties, satisfaction with sexual frequency, and relationship satisfaction are all mutually interconnected. Furthermore, women and men may differ regarding how they perceive and deal with sexual difficulties (Hinchliff et al., Citation2020; Lodge & Umberson, Citation2012). In addition, we expected that the associations among these constructs might differ when internalized ageist sexual stereotypes are considered. The expectation was that this change might be the result of older people’s responses to sexual problems, specifically by alleviating the demands on their sexual performance through the activation of internalized sexual stereotypes. In the sexual domain, satisfaction with sexual frequency was chosen because of the frequent focus of ageist sexual stereotypes on this aspect (e.g., sex is unnecessary in older age) rather than on the particular content of the sexual activities in older adults.
The aim of this study was to examine the structure of the aforementioned sex-related constructs. Our theoretical assumption about the associations among the studied constructs prompted the application of a network model (Borsboom et al., Citation2021; Schmittmann et al., Citation2013) that assumes that the variables covary not due to higher-order latent causes, but due to bidirectional causal links among each other (Cramer et al., Citation2010, Citation2012). For example, it is possible that not only does lower sexual frequency cause lower relationship satisfaction, but also lower relationship satisfaction causes lower sexual frequency. Our data were cross-sectional, so we could not test these paths directly; however, by calculating the undirected network analysis, we allow edges (links between the variables – nodes) to be estimated freely and bring some evidence of the connections. Furthermore, the network approach allowed us to estimate the role of each variable in the network – e.g., its centrality and expected influence. These indices are valuable for prediction of network processes such as information flow, clustering, or intervention guidance (Borsboom & Cramer, Citation2013; Cramer et al., Citation2010). More specifically, this approach allowed us to test which of the selected variables were in the core of the sex-related network and which were peripheral.
Assuming that ageist sexual stereotypes may be interlinked with the relationship between sexual difficulties/perceived health and satisfaction with sexual frequency/relationship, we proposed that (H1) poor health and low satisfaction with sexual frequency would be weakly connected in the presence of ageist sexual stereotypes, when controlling for ageist sexual stereotypes. Similarly, we expected that (H2) the relationship between poor health and low relationship satisfaction would be weaker in the presence of ageist sexual stereotypes, including the stereotypes in the network. We further proposed that (H3) the relationship between sexual difficulties and low satisfaction with sexual frequency would be weaker in the presence of ageist sexual stereotypes. And Similarly, we predicted that (H4) the relationship between sexual difficulties and low relationship satisfaction would be weaker in the presence of ageist sexual stereotypes. When assuming specific relationships exist in the interconnected structure, we hypothesized the existence of various positive and negative associations (see ). In several cases (marked as “?”), we had no expectations for the relationship.
Table 1. Expected valences of relationships in the network.
These hypotheses were tested using the Czech and Slovak samples. Both Czechia and Slovakia share several similarities, such as ethnic homogeneity and similar social and geopolitical histories (Manea & Rabušic, Citation2020). The countries were united as Czechoslovakia for 74 years until the end of 1992. The communist regime in Czechoslovakia initiated significant social changes, such as secularization and pro-family politics (Lišková, Citation2018). Regarding sexuality, important milestones were the decriminalization of both abortion and homosexuality at the end of the 1950s in Czechoslovakia (Lišková, Citation2018). Even during the communist era, there were educational campaigns that emphasized the quality of sexual life, recommended sexual techniques, and the destigmatization of sexuality for aging women (Bělehradová & Lišková, Citation2021). According to Czech research, sexual intercourse (i.e. penetrative sex) is still the predominant sexual activity (Steklíková, Citation2014). Masturbation is not as popular, especially among the older population, and attitudes toward it are more conservative compared to the younger population (Steklíková, Citation2014; Weiss & Zvěřina, Citation2001). A comparison of the Czech and Slovak Republics indicates greater conservatism among the Slovak population in the values of marriage, fertility, and family, probably due to the higher level of religiosity (Manea & Rabušic, Citation2020). However, further analyses of sexual behavior in Slovakia points to a reorientation to a more liberal approach among the younger population (Petrík, Citation2020).
Method
Participants and Recruitment
Respondents, aged 50+, resided in the Czech Republic and the Slovak Republic. They completed an online survey on sexual life and intimate relationships in mid- and later life that was advertised from December 2018 to March 2019. The original version of the survey was in the Czech language, then translated into Slovak. In October and December 2018, both the Czech and Slovak questionnaires were piloted via interviews with 11 people aged 50+ in order to check how respondents understood the individual questions and how sensitive the questions were. Two language experts (one Czech, one Slovak) assessed the translation and clarity, and their comments were incorporated. It should be noted that the Czech and Slovak languages are very similar. Informed consent was obtained from respondents via entry into the online questionnaire. Only those who provided informed consent online were given access to the questionnaire. The study was approved by the authors’ institutional ethics board.
The questionnaire was originally completed by 1,032 partnered Czech and Slovak respondents aged 50+ (233 from Slovakia). After applying the inclusion criteria (i.e., age 50+, being in a relationship), the final sample included 897 respondents aged 50–96. Detailed description of the sample is presented in the Results section.
Procedure
Both the Czech and Slovak questionnaires were published on the Qualtrics platform and advertised online via social media (e.g., Facebook) and two dominant Czech advertising agencies – Seznam.cz and Czech News Center (CNC) – which have internal mechanisms to target advertising to Czech internet users aged 50 and older. Seznam.cz represents a multifaceted web portal and search engine used by half of the Czech internet population. The marketing portfolio of CNC includes about 40 online newspaper and magazine products, and it reaches about 6 million internet users (the Czech Republic has about 7 million internet users aged 16 and over; CZSO, Citation2018). Both advertising companies had an internal mechanism at their disposal to promote the survey advertisement on websites popular among internet users aged 50+ (such as online tabloids – prozeny.blesk.cz; super.cz; or online news, such as novinky.cz). Participants were motivated by the chance to win a 40 Euro gift voucher for a drugstore; five vouchers were available. Respondents had a specific code for the voucher raffle. They could voluntarily choose to provide an address, which was entrusted only to the principal investigator of the project with the approval of the Research Ethics Committee of Masaryk University (EKV-2019-023). In Slovakia, an online questionnaire was distributed via various channels, such as social media (i.e., Facebook, websites targeting the older population), retirement clubs, and all 19 universities of the third age (U3A, lifelong learning for people of retirement age). No incentives were provided in Slovakia.
Measures
Ageist Sexual Stereotypes
Ageist sexual stereotypes were assessed with five items. Their development was inspired by the Aging Sexual Knowledge and Attitudes Scale (ASKAS; White, Citation1982) and other relevant studies (e.g., Minichiello et al., Citation2000; Monteiro et al., Citation2017; Syme & Cohn, Citation2021; White, Citation1982), and primarily derived from a prior qualitative study on sex in later life in the Czech Republic (Ševčíková & Sedláková, Citation2020). Respondents evaluated the degree of agreement with statements such as: “Sex is a natural part of advanced age;” “Old people should no longer have an active sex life;” and “In older age, strengthening a relationship by having sex is no longer needed.” The answers were evaluated with a Likert-type answer scale that ranged from Strongly disagree (1) to Strongly agree (5). Answers were recoded so higher scores meant greater acceptance of the ageist sexual stereotypes. The internal consistency of the measure was McDonald’s ω total = 0.77 and the fit of the unidimensional factor model, which was estimated with the mean- and variance-adjusted weighted least squares (WLSMV) estimator, was satisfactory (χ2 = 109.466, df = 5, CFI = 0.965, TLI = 0.931, RMSEA = 0.168, 95% CI [0.141, 0.196], SRMR = 0.084). We do not consider RMSEA highly relevant here due to the low degrees of freedom, which cause inflation of the RMSEA (Kenny et al., Citation2015).
Frequency of Sexual Intercourse
Frequency of sexual intercourse was assessed by a single item that indicated frequency over the preceding 12 months: “In the last 12 months, how often have you had sexual intercourse?” We decided to use only one item in line with Borsboom’s (Citation2008) arguments about similar concepts because we consider frequency of sexual intercourse to be a manifest variable (i.e., an epistemically accessible variable). The possible responses were I had no intercourse (1), Less than once a month (2), Once a month (3), Two or three times per month (4), Once a week (5), and A number of times per week or more often (6). The term pohlavní styk, which was used in the questionnaire and commonly used in Czech, refers to genital penetrative sex, mostly vaginal intercourse, and is translated as “sexual intercourse.”
Sexual Difficulties
Sexual difficulties in men were assessed with three items from the Czech version of the International Index of Erectile Function (Broul & Schraml, Citation2011; IIEF-5, Rosen et al., Citation1999). Respondents were asked to evaluate their ability to reach and maintain their erection (i.e., “When you were sexually stimulated to get an erection, how often was your erection sufficient for sexual intercourse?,” “How difficult is it for you to maintain your erection until the end of sexual intercourse?”). The assessment was on a 5-point Likert scale that ranged from very low (1) to very high (5). The erectile dysfunction items showed an exact fit (i.e., perfect fit indices) when tested for unidimensionality due to the zero degrees of freedom. However, since the Spearman correlation between the items was high (r = 0.50–0.62), we considered using the mean score in the following analyses justified. The reliability was McDonald’s ω total = 0.87. In women, we focused on assessing discomfort and pain during sexual intercourse (i.e., using one item “How often did you experience discomfort or pain during intercourse?”). This item was selected based on the findings of epidemiological studies that pain and discomfort during sex increases with age and where vaginal dryness has been identified as the main reason (National Survey of Sexual Attitudes and Lifestyles, Mitchell et al., Citation2013; German Health and Sexuality Survey; Briken et al., Citation2020; The English Longitudinal Study of Ageing; Lee et al., Citation2016; Hughes et al., Citation2015).
The Importance of Sex
This aspect was measured with one item: “With regard to the last 12 months, how important is having sex to you?” with responses on a 5-point Likert-scale that ranged from not at all (1) to very important (5). We consider the importance of sex to be an epistemically accessible variable (Borsboom, Citation2008). Therefore, we treat it as a manifest variable and do not measure it with latent structure expectations.
Satisfaction with the Frequency of Sex
This variable was assessed by a single item: “How would you rate your satisfaction with the frequency of sex, i.e., how often did you have it in the last 12 months?” The respondents evaluated their satisfaction with the frequency of sex on a 5-point Likert-type scale that ranged from Very dissatisfied (1) to Very satisfied (5). This variable was measured with only one item due to its arguably observable/manifest nature. As Borsboom (Citation2008) suggested, there is no point in measuring certain types of variables with multiple items; even though they are not literally observable, they are still epistemically accessible (e.g., age, gender, subjective health). Although the focus on satisfaction with the frequency of sex only might be reductionist, age-related decline in sexual activity is an issue that bothers some older people, therefore we refrained from elaborating on this in multiple questions (Gore-Gorszewska & Ševčíková, Citation2022; Ševčíková et al., Citation2021).
Relationship Satisfaction
Relationship satisfaction was assessed with the short, four-item version of the Couples Satisfaction Index (Funk & Rogge, Citation2007). Respondents were asked to rate four questions, such as “How satisfied are you with your relationship?”, on a 7-point Likert-type scale (i.e., from Extremely unsatisfied (1) to Extremely satisfied (7)), where higher values indicated higher satisfaction. The Couples Satisfaction Index showed very high internal consistency (McDonald’s ω total = 0.97 in our sample). For each respondent, we calculated the relationship satisfaction score as the mean of the item scores. The scale was unidimensional and overfitted in our sample due to the low degrees of freedom (χ2 = 11.746, df = 2, CFI = 1, TLI = 1, RMSEA = 0.082, 95% CI [0.041, 0.130], SRMR = 0.007). The items’ Spearman correlation ranged from 0.83 to 0.90 (i.e., each measured very similar constructs).
Subjective Health
This variable was adapted from the U.S. version used in the Survey of Health, Ageing and Retirement in Europe (SHARE, Börsch-Supan et al., Citation2013) and measured by the item “Would you say that your health is…” with response options on a 5-point Likert scale that ranged from very bad (1) to very good (5). Subjective health is commonly measured with one item and this approach has been shown to have sufficient reliability and validity (e.g., Ahmad et al., Citation2014; Ang & Eisend, Citation2018; Cunny & Perri, Citation1991).
Data Analyses
The data were analyzed with R (version 4.3.1; Team, R. D. C., Citation2011) and RStudio software (version 2023.09.1). We provide a complete analytical script in the Open Science Framework (https://osf.io/kf3zu/).
Regarding data manipulation, we first selected participants from the original dataset based on the inclusion criteria: only those currently in a relationship were included in the analysis. Missing data were imputed using the Classification and Regression Trees (CART; Burgette & Reiter, Citation2010) method for multiple imputation, which performs well on non-normal and ordinal data (Wongkamthong & Akande, Citation2023). We obtained descriptive statistics for the variables for all of the participants and then separately for women and men. Finally, we applied the non-paranormal transformation on the data to ensure the normalization of the variables’ distributions (Liu et al., Citation2009). This method is commonly used and recommended even for highly non-normally distributed data (Malgaroli et al., Citation2018; Zhao et al., Citation2012).
Before estimating the models, we applied a power analysis to ensure the validity of the findings. In the network framework, specific power analyses were not yet developed; however, we followed the procedure of Faelens et al. (Citation2019), who tested network power with the bootnet package (Epskamp & Fried, Citation2020) by simulating data.
Based on the assumption of mutual causal relationships among the sex-related constructs, we applied the network framework. In this approach, a set of nodes (i.e., observed variables) and edges (i.e., connections among the nodes) is estimated based on the covariances in the input data. We fitted a total of four freely estimated network models in a 2 × 2 fashion: Model W1 and Model M1 were calculated separately for women (nw = 431) and men (nm = 466) using the sex-related constructs without including ageist sexual stereotypes. Next, we included ageist sexual stereotypes in the modeled networks split by gender, labeling them Model W2 and Model M2.
All final network models were estimated using the bootnet package (Epskamp & Fried, Citation2020) with polychoric correlations suitable for ordinal data. We applied the regularized method of EBIC-graphical with the least absolute shrinkage and a selection operator (EBICglasso) that shrinks potentially spurious edges to zero. Additionally, we estimated the network with the unregularized stepwise model search method (Epskamp, Citation2020; Isvoranu & Epskamp, Citation2023). This approach searches for the optimal model by minimizing the extended Bayesian information criterion (EBIC; Foygel & Drton, Citation2010). We compared the estimations methods to ensure valid results. For plotting, we used the qgraph package (Epskamp et al., Citation2021) and average layouts for an easier comparison of the networks. Furthermore, we estimated centrality indices (i.e., strength, closeness, betweenness, expected influence for each node). Both the networks and the indices were tested for post hoc stability by applying nonparametric bootstrapping (n = 1,000). Finally, we compared Model W1 with M1 and Model W2 with Model M2 using the Network Comparison Test (Van Borkulo et al., Citation2022) to assess gender differences. We applied the Holm-Bonferroni correction for multiple testing and tested for which edges differed significantly in women and men.
Results
Descriptive Statistics
In , we present a demographic description of women and men in our sample. The mean age of women (M = 60.1) and men (M = 63.8) was significantly different (t(882.99) = −7.15, p < .001, Cohen d = 0.49. The difference in age between Czechs (n = 696, M = 61.7) and Slovaks (n = 181, M = 62.8) was statistically non-significant (t(313.06) = −1.90, p = .058, Cohen d = 0.15. All of the respondents were asked demographic questions about age, nationality, education level, occupational status, marital status, and sexual orientation.
Table 2. Demographic description of the sample by gender.
We also tested for differences in the study variables between Czech and Slovak respondents. These groups did not significantly differ in relationship satisfaction (t(244.46) = 0.64, p = .525), satisfaction with the frequency of sex (t(280.05) = −0.52, p = .60), or subjective health (t(217.42) = −0.57, p = .56). Czechs and Slovaks, however, differed in the mean frequency of sexual intercourse, with Czechs having a higher mean (M = 4.01) than Slovaks (M = 3.52), t(256.17) = 3.49, p < .001, Cohen d = 0.3; in the importance of sex, with Czechs having a higher mean (M = 3.37) than Slovaks (M = 2.79), t(243.28) = 6.57, p < .001, Cohen d = 0.58; and in ageist sexual stereotypes, with Czechs having a higher mean (M = 1.68) than Slovaks (M = 1.44), t(191.16) = −5.02, p < .001, Cohen d = 0.50. Even though the two groups differed in the averages of some variables, we did not expect the differences to affect the main results because, in the main analysis, we tested associations among the variables, not the mean differences.
All the variables included in the analysis are described in . All were relatively normally distributed (within −1 and 1 in skewness and kurtosis) with the exception of the frequency of sexual intercourse in women (kurt = −1.24) and satisfaction with the frequency of sex in men (kurt = −1.01). Based on the observed means, women and men did not differ in their relationship satisfaction, satisfaction with the frequency of sex, ageist sexual stereotypes, and subjective health. Some statistically significant differences were observed in the frequency of sexual intercourse (t(849.73) = −4.39, p < .001, Cohen d = 0.3) and the importance of sex (t(846.15) = −9.02, p < .001, Cohen d = 0.61. Sexual difficulties were measured differently for women and men and are, therefore, not comparable. Bivariate correlation matrices on the variables are available in the online Supplementary Material.
Table 3. Descriptive statistics of the study variables.
Network Models
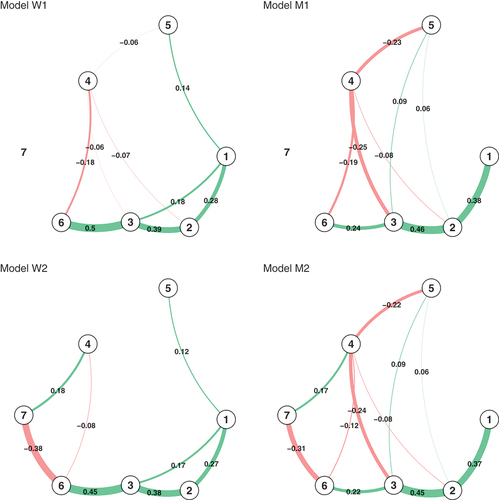
presents four network models. Models W1 and M1 (i.e., model 1 for women and men, respectively) include all sex-related variables, except for (7) ageist sexual stereotypes, while Models W2 and M2 (i.e., model 2 for women and men, respectively) were estimated with this variable. Models W1 and M1 (without ageist sexual stereotypes) both had more connections (non-zero edges in W1: 80%; M1 73%) than the models with ageist sexual stereotypes included (W2: 62%; M2: 67%). We generally considered an edge of r > 0.05 as the smallest meaningful result; therefore, we set plotting parameters to cut = 0.1 and a minimum = 0.051. Moreover, stability tests (see online Supplementary Material) showed that in models W1, M1, and W2, edges < 0.09 (in absolute value) were not significantly different from zero. In Model M2, even the edges of r < 0.08 were not significantly different from zero. Based on these results, edges smaller than 0.09 should be interpreted with great caution in all of the models.
Figure 1. Network models. Note. Models W1 (Model 1 for women) and M1 (Model 1 for men) include all sex-related variables, except for the ageist sexual stereotypes. Models W2 (Model 2 for women) and M2 (Model 2 for men) were estimated with the ageist sexual stereotypes variable. (1) relationship satisfaction; (2) satisfaction with the frequency of sex; (3) frequency of sexual intercourse; (4) sexual difficulties; (5) subjective health; (6) importance of sex; and (7) the ageist stereotypes.
Models without Ageist Sexual Stereotypes Included (W1 and M1)
In Model W1, the largest edges were (3) frequency of sexual intercourse – (6) importance of sex (r = 0.5) and (3) frequency of sexual intercourse – (2) satisfaction with frequency of sex (r = 0.39). In the men’s network (M1), the largest edges were (3) frequency of sexual intercourse – (2) satisfaction with frequency of sex (r = 0.46) and (2) satisfaction with frequency of sex – (1) relationship satisfaction (r = 0.38). The edges around (4) sexual difficulties were mostly close to zero in women, except for (4) sex difficulties – (6) importance of sex (r = −0.18). In men, (4) sex difficulties were meaningfully connected to the (6) importance of sex (r = −0.19), (3) frequency of sexual intercourse (r = −0.25), and (5) subjective health (r = −0.23).
Models with Ageist Sexual Stereotypes Included (W2 and M2)
After including (7) ageist sexual stereotypes, this variable was highly connected to (6) importance of sex (women: r = −0.38; men: r = −0.31). Overall, the inclusion of this variable changed the networks of both genders. It is important to note that by adding a variable into a model, it is likely that all of the edges weakened due to the portion of the variance being explained by the new variable. Nonetheless, in both women and men, (7) ageist sexual stereotypes seemed to weaken the connection of (4) sexual difficulties – (6) importance of sex. This change was more notable in women, where the connection differed by 0.1 in Model W2 and became non-significantly different from zero. In men, (4) sexual difficulties – (6) importance of sex remained moderately connected (r = −0.12). In women and men, both (4) sexual difficulties and (6) importance of sex formed edges with (7) ageist sexual stereotypes individually as well. Ageist sexual stereotypes did not form meaningful edges with other variables in the models.
Centrality Indices
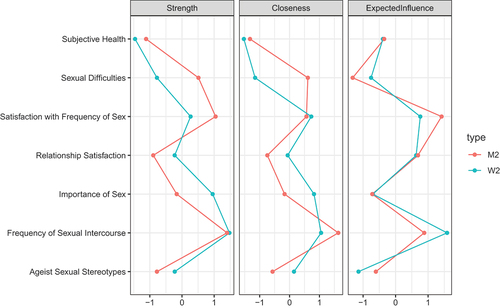
Node strength estimates the degree of direct edge connectedness of a certain node. In the case of this index, men and women differed mostly in the role of (4) sexual difficulties ( and ). In both women’s and men’s networks, (4) sexual difficulties had low strength in women (W1: z = −0.74; W2: z = −0.78) but average strength in men (M1: z = 0.19; M2: z = 0.51). Women and men also differed in the strength of the (6) importance of sex variable in both networks. Its strength was higher for women (W1: z = 0.1; W2: z = 0.95) than for men (M1: z = −0.88; M2: z = −0.16). In both genders the role of the (6) importance of sex among the variables increased when (7) ageist stereotypes were added into the model. Very similar results were obtained for the closeness centrality, which estimates the degree of indirect edge connectedness of a certain node. When analyzing closeness, women and men differed mostly in (4) sexual difficulties. Expected influence, which shows which edges have the strongest connections and thus might be most important in the network, was similar in both genders. Women and men only differed in whether (2) satisfaction with the frequency of sex (men) or (3) frequency of sexual intercourse (women) was estimated as the most important variable. We do not present betweenness centrality here in the main text due to its instability (see online Supplementary Material for all stability results). The correlation stability coefficients for strength, closeness, and expected influence were > 0.5 in all models as recommended (Epskamp et al., Citation2018).
Figure 2. Centrality indices.
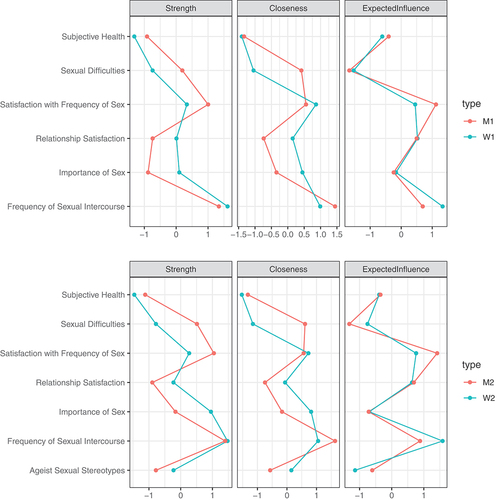
Figure 3. Centrality indices.
Model Comparisons
We tested the differences between Models W1 and M1 and found that they were not invariant (M = 0.26, p < .001). Two edges were statistically different in Models W1 and M1: (3) frequency of sexual intercourse – (4) sex difficulties (p = .022) and (3) frequency of sexual intercourse – (6) importance of sex (p = .015). In the global strength invariance test, Models W1 and M1 did not show statistically significant results (S = 0.13, p = .48). Only (4) sex difficulties had significantly different closeness and expected influence (both p = .009); other centrality indices did not differ between women and men. The centrality of (4) sex difficulties was, therefore, statistically different in women and men, whereas in men, (4) sexual difficulties was a more important variable in the model.
The network invariance test between Models W2 and M2 showed an overall significant difference (M = 0.23, p = .003). In post-hoc tests, two edges (just like in W1 v. M1) were different: (3) frequency of sexual intercourse – (4) sex difficulties (p = .021) and (3) frequency of sexual intercourse – (6) importance of sex (p = .021). The global invariance test of centrality was not statistically significant (S = 0.22, p = .31), with only (4) sex difficulties flagged and different in strength, closeness, and expected influence (all p = .007). The differences in Models W2 and M2 were similar to those between W1 and M1: (4) sex difficulties remained a more influential variable in the men’s network than in the women’s network.
Within the network analysis, the tests for comparing networks with a different number of nodes are not (yet) developed. Therefore, we could not test edge differences directly between models without (7) ageist sexual stereotypes (W1, M1) and with stereotypes included (W2, M2). Adding (7) ageist sexual stereotypes, however, explained a non-negligible portion of the variance of (4) sexual difficulties and the (6) importance of sex in both women and men. Thus, the results for gender differences and stereotype-inclusion differences are a preliminary preview of the possible disparity of the effect of ageist sexual stereotypes on intimacy in later life.
Expected Relationships in the Networks and Hypotheses
Within our hypotheses, we had general expectations about the associations among the variables in Models W2 and M2. Out of the 21 possible relationships, we stated our expectations for 12. Three of the expected relationship valences were found in all four models (see ): the positive network associations of (2) satisfaction with the frequency of sex – (1) relationship satisfaction; (3) frequency of sexual intercourse – (2) satisfaction with the frequency of sex; and (6) importance of sex – (3) frequency of sexual intercourse. Additionally, two expected associations regarding (7) ageist sexual stereotypes were also found in models W2 and M2 (positive relationship with (4) sexual difficulties and negative relationship with (6) importance of sex). Four expected associations were found only in one gender: (1) relationship satisfaction was positively associated with (3) frequency of sexual intercourse and (5) subjective health in women while in men, we found an intercorrelated structure for (3) frequency of sexual intercourse, (2) satisfaction with the frequency of sex, (4) sexual difficulties, and (5) subjective health. Finally, three hypothesized relationships were not found or were mixed: (4) sex difficulties – (1) relationship satisfaction; (5) subjective health – (2) satisfaction with the frequency of sex (the edge was not statistically different from 0); and (7) ageist sexual stereotypes – (3) frequency of sexual intercourse. When only simple bivariate correlation was used, all of these dyads were associated as expected; however, a network model takes into account all relationships at once, much like partial correlation, so these bivariate associations were explained by other variables (e.g., in case of (7) ageist sexual stereotypes – (3) frequency of sexual intercourse dyad, its covariance was eliminated by (6) importance of sex).
Table 4. Expected valences of relationships in the network (lower triangle) and obtained relationships in the networks (upper triangle).
Regarding H3, our results were also not supportive. (4) Sexual difficulties and (2) satisfaction with the frequency of sex were not meaningfully connected in women. In men, the confidence intervals around the estimated edges in M1 and M2 (both r = −0.08) did not include zero; therefore, they could be considered meaningful. The values are relatively small, so their estimate should be interpreted with caution. Finally, H4 was not supported. (4) Sexual difficulties and (1) relationship satisfaction did not form a meaningful connection in any of the networks, regardless of whether (7) ageist sexual stereotypes were included.
Discussion
In this study we used a network analysis to examine the associations between experiencing sexual difficulties, satisfaction with sexual frequency, and relationship satisfaction in women and men 50+, together with the possible effect of ageist sexual stereotypes on these associations.
The findings showed that ageist sexual stereotypes could play a relevant role in the sexual activity of people aged 50 + .Specifically, in our sample these were strongly interconnected with the importance of sex and sexual difficulties such that the fewer ageist sexual stereotypes people had, the less sexual difficulties they reported and the more they perceived sex as important. Moreover, the inclusion of stereotypes into the models seemed to weaken the negative link between sexual difficulties and the importance of sex in women and men. These results suggest that the proposed effect of ageist sexual stereotypes may not be completely rejected, albeit our hypotheses regarding sexual and relationship satisfaction were not supported. Sexual problems after the age of 50 may represent a challenge that is difficult to manage and to efficiently cope with in some cases (Rosen et al., Citation2016). To reduce uncomfortable tension, some people may adopt these ageist sexual stereotypes to attenuate the importance of sex while facing the onset of sexual difficulties (Hinchliff & Gott, Citation2004; Sinković & Towler, Citation2019) and, subsequently, start to view negative changes in sexual activity as a natural part of aging (DeLamater, Citation2012; Gore-Gorszewska & Ševčíková, Citation2022; Lodge & Umberson, Citation2012; Ševčíková & Sedláková, Citation2020). We acknowledge that future research should discern the specific conditions in which ageist sexual stereotypes may be a coping mechanism with positive outcomes and when they create a barrier to efficiently tackle sexual difficulties (e.g., individuals may struggle to sufficiently stimulate the penis through manual or oral methods to achieve a satisfactory erection or they do not incorporate using lubricants due to negative attitudes toward later-life sex). Either way, our findings expand the existing knowledge about the linkage between ageist sexual stereotypes and decreased sexual activity among adults 50+ (Estill et al., Citation2018; Skoblow et al., Citation2023; Syme et al., Citation2019). Specifically, we highlight how accepting these stereotypes may influence the perception and management of sexual difficulties among individuals in this age group, potentially leading them to reassess the importance of sex based on ageist beliefs (Gott & Hinchliff, Citation2003b; Ševčíková & Sedláková, Citation2020).
Nonetheless, it is worth mentioning that we only observed the edges between ageist sexual stereotypes, the importance of sex, and sexual difficulties. No linkages to the frequency of sexual intercourse, relationship satisfaction, satisfaction with the frequency of sex, and subjective health were identified. These findings indicate that ageist sexual stereotypes play a role when older people interpret their sexual problems and the importance of sex in their lives. If ageist sexual stereotypes exert some effect on the frequency of sexual intercourse, satisfaction with the frequency of sex, or relationship satisfaction, then this probably happens via the construct of the importance of sex. It is worth considering that the operational definition of sex as intercourse, which was employed in the measurement, may have influenced the outcomes. It cannot be ruled out that some participants reported their satisfaction with sex frequency and relationship satisfaction based on non-penetrative sexual activities that they engaged in and personally considered as “having sex” (Gore-Gorszewska, Citation2021). Future research is needed to test these potential causal links and nuances in how sex is understood by older individuals.
The network analysis showed the interconnectivity and complexity of all of the studied sex-related constructs. Specifically, ageist sexual stereotypes were interconnected via importance of sex with other sex-related constructs, such as sex frequency and satisfaction with the frequency of sex. The acceptance of sexual stereotypes becomes more likely when sexual frequency decreases and the importance of sex diminishes. The connections of sex-related constructs were similar for both genders and the frequency of sex was a central variable in the network. Our findings suggest that people aged 50+ who have sex more often find partnered sex to be important and probably crucial for sexual satisfaction and, subsequently, for relationship satisfaction. These findings about the role of sex frequency in people aged 50+ in the perception of importance of sex and sexual and relationship satisfaction differ from other studies, which found that frequent sex was, under certain conditions, not essential for relationship satisfaction and sexual satisfaction in later life (Connor et al., Citation2020; Freak-Poli & Malta, Citation2020; Gott & Hinchliff, Citation2003b). An explanation could be that our sample included middle-aged adults for whom frequent sex still may be a key element in satisfaction, similar to the findings of Fisher et al. (Citation2015). Another explanation could be that the study included people who were in a relationship with sexually active partners without sex difficulties for whom frequent sex remained accessible, constituting “the icing on the cake” of their otherwise satisfying relationship (Towler et al., Citation2022).
For women and men, satisfaction with sexual frequency was also dominant in the network. The results suggest that satisfaction with sex frequency bridges the connection between sex frequency and relationship satisfaction, supporting previous findings on the close connection between these variables in people aged 50+ (Erens et al., Citation2019; Freak-Poli & Malta, Citation2020). The importance of sexual frequency (i.e., penetrative intercourse) in a relationship probably reflects heterosexual norms present in Western cultures and particularly among Czechs (Steklíková, Citation2014). Thus, a decline in sexual frequency (e.g., due to sexual difficulties) may compromise satisfaction in diverse areas of a couple’s life (e.g., feelings of failure or insufficiency; e.g., Heiman et al., Citation2011; Lodge & Umberson, Citation2012; Rahn et al., Citation2020; Rosen et al., Citation2016). In this respect, satisfaction with sexual frequency may reflect a lack of significant sexual problems or, alternatively, the successful implementation of coping strategies (e.g., reframing the meaning of sex, affirmative aging; Towler et al., Citation2021).
In women, we did not find a direct connection between sexual difficulties and sexual frequency in the models. An explanation could be the different nature of sexual problems and different way they impact sexual activity in women and in men (Træen et al., Citation2018). In women, often-reported problems, such as vaginal dryness, can be addressed relatively easily with lubricants (Kennedy et al., Citation2022) or may not be considered a reason to cease partnered penetrative sex, in line with traditional sexual gender roles (i.e., regardless of potential discomfort or pleasure issues; Gore-Gorszewska, Citation2021; Shen, Citation2019; Træen et al., Citation2019). Thus, female sexual difficulties may not necessarily affect satisfaction with sexual frequency or sexual frequency itself. In older men, the management of frequently reported erectile difficulties, directly tied to the ability to engage in intercourse, is often complicated (i.e., not all erection difficulties may be treatable with erection-enhancing drugs), and men commonly delay seeking medical attention (Gore-Gorszewska, Citation2020; Hinchliff et al., Citation2021; Štulhofer et al., Citation2020). It is important to mention that, for older Czechs, penetrative sex is the dominant sexual activity, and the onset of erectile difficulties may facilitate sexual cessation (Ševčíková & Sedláková, Citation2020; Steklíková, Citation2014). These differences may explain why sexual difficulties in men, but not in women, had a direct negative link to sex frequency and to relationship and sex frequency satisfaction.
This study supported the hypothesis about the association between subjective health and relationship satisfaction in women. One of the possible explanations could be that women, not men, see themselves as the main caregivers in a relationship (Barken, Citation2017; Bertogg & Strauss, Citation2020; Williams et al., Citation2017). Although this assumption is stereotypical, this generation of baby boomers is accustomed to the division of gender roles (Bertogg & Strauss, Citation2020; Floridi et al., Citation2022; Langner & Furstenberg, Citation2020). If health problems arise in older women, their role and method of relationship maintenance can be shaken, leading to worsened relationship satisfaction. This could also explain why no similar association was observed in men, as their worsened health may result in their female partners attending to them to a greater extent.
Strengths and Limitations
When interpreting these findings, it is essential to consider both the study’s strengths and limitations. The strength of the study is the use of network analysis to capture the complexity of interconnections among the variables and the possibility of deepening knowledge on sexuality and aging. The study conclusions should be interpreted cautiously due to the cross-sectional design of the study, which does not allow for causal inferences or the examination of changes across time. Additionally, the convenience online sample limits the generalizability of findings to the general population, including internet non-users. The study did not address the sexuality of LGBTQ+ adults aged 50+, because the number of these respondents was insufficient (5.8%); further research on this population is needed in this respect. The sample included people in both middle and late adulthood. The possible differences between these two populations in the role of ageist sexual beliefs could not be elaborated further due to the relatively smaller number of participants in the latter developmental stage, whose level of internalization of the ageist sexual stereotypes may be higher than in the younger group. The sample size was rather small for the purpose of some components of the network analysis (i.e., several centrality indices). This study measured the frequency of sex defined as intercourse, the most common sexual practice in Czech older adults (Steklíková, Citation2014), while other relevant sexual practices (e.g., oral sex, petting, cuddling) were not assessed. However, a recent study found that non-penetrative sex did not affect the association between sexual difficulties and satisfaction with sex and relationships (Ševčíková et al., Citation2023). Lastly, to measure relationship satisfaction, we used the Couples Satisfaction Index, which has not been used and validated for the Czech context. Although the original wording of the items was easy to translate, future research should validate this measurement tool for Czech and Slovak populations.
Conclusions
The study revealed the important, yet complex, role of ageist sexual stereotypes in the sexual lives of adults aged 50+, specifically in relation to sexual difficulties and the lower perceived importance of sex. The findings showed a weakened association between sexual difficulties and the perceived importance of sex in the presence of ageist sexual stereotypes. These results suggest that stereotypes may have a function when dealing with sexual difficulties for some older adults via the decreased importance of sex. Future research should include the construct of ageist sexual stereotypes when studying changes in sexuality after the age of 50, when rates of sexual difficulties increase. The findings of this study may be relevant to clinicians who work with adults aged 50 + . They highlight the importance of assessing the context in which ageist sexual stereotypes arise and examining their potential impact on their clients’ sexual well-being. This information can help clinicians provide their patients with more tailored and effective care.
Availability of Data and Material
Data are accessible at https://osf.io/kf3zu/
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Masaryk University (EKV-2016-035).
Supplemental Material
Download Zip (121 KB)Disclosure Statement
No potential conflict of interest was reported by the author(s).
Supplementary Material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/00224499.2024.2307441.
Additional information
Funding
References
- Ahmad, F., Jhajj, A. K., Stewart, D. E., Burghardt, M., & Bierman, A. S. (2014). Single item measures of self-rated mental health: A scoping review. BMC Health Services Research, 14(1), 398. https://doi.org/10.1186/1472-6963-14-398
- Ang, L., & Eisend, M. (2018). Single versus multiple measurement of attitudes. Journal of Advertising Research, 58(2), 218 LP–227. https://doi.org/10.2501/JAR-2017-001
- Ayalon, L., Gewirtz-Meydan, A., Levkovich, I., & Karkabi, K. (2021). Older men and women reflect on changes in sexual functioning in later life. Sexual and Relationship Therapy, 36(4), 347–367. https://doi.org/10.1080/14681994.2019.1633576
- Barken, R. (2017). Reconciling tensions: Needing formal and family/friend care but feeling like a burden. Canadian Journal on Aging/La Revue canadienne du vieillissement, 36(1), 81–96. https://doi.org/10.1017/S0714980816000672
- Bělehradová, A., & Lišková, K. (2021). Aging women as sexual beings. Expertise between the 1950s and 1970s in state socialist Czechoslovakia. The History of the Family, 26(4), 562–582. https://doi.org/10.1080/1081602X.2021.1955723
- Bertogg, A., & Strauss, S. (2020). Spousal care-giving arrangements in Europe. The role of gender, socio-economic status and the welfare state. Ageing & Society, 40(4), 735–758. https://doi.org/10.1017/S0144686X18001320
- Borsboom, D. (2008). Latent variable theory. Measurement: Interdisciplinary Research & Perspectives, 6(1–2), 25–53. https://doi.org/10.1080/15366360802035497
- Borsboom, D., & Cramer, A. O. J. (2013). Network analysis: An integrative approach to the structure of psychopathology. Annual Review of Clinical Psychology, 9(1), 91–121. https://doi.org/10.1146/annurev-clinpsy-050212-185608
- Borsboom, D., Deserno, M. K., Rhemtulla, M., Epskamp, S., Fried, E. I., McNally, R. J., Robinaugh, D. J., Perugini, M., Dalege, J., & Costantini, G. (2021). Network analysis of multivariate data in psychological science. Nature Reviews Methods Primers, 1(1), 1–18. https://doi.org/10.1038/s43586-021-00055-w
- Börsch-Supan, A., Brandt, M., Hunkler, C., Kneip, T., Korbmacher, J., Malter, F., Schaan, B., Stuck, S., & Zuber, S. (2013). Data resource profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). International Journal of Epidemiology, 42(4), 992–1001. https://doi.org/10.1093/ije/dyt088
- Briken, P., Matthiesen, S., Pietras, L., Wiessner, C., Klein, V., Reed, G. M., & Dekker, A. (2020). Estimating the prevalence of sexual dysfunction using the new ICD-11 guidelines: Results of the first representative, population-based German Health and Sexuality Survey (GeSiD). Deutsches Ärzteblatt international, 117(39), 653. https://doi.org/10.3238/arztebl.2020.0653
- Broul, M., & Schraml, J. (2011). Kvalita života a hodnocení erektilní dysfunkce po robotické radikální prostatektomii. Urologie pro Praxi, 12(4), 256–259.
- Burgette, L. F., & Reiter, J. P. (2010). Multiple imputation for missing data via sequential regression trees. American Journal of Epidemiology, 172(9), 1070–1076. https://doi.org/10.1093/aje/kwq260
- Carstensen, L. L., Turan, B., Scheibe, S., Ram, N., Ersner-Hershfield, H., Samanez-Larkin, G. R., Brooks, K. P., & Nesselroade, J. R. (2011). Emotional experience improves with age: Evidence based on over 10 years of experience sampling. Psychology and Aging, 26(1), 21. https://doi.org/10.1037/a0021285
- Charles, S. T. (2010). Strength and vulnerability integration: A model of emotional well-being across adulthood. Psychological Bulletin, 136(6), 1068. https://doi.org/10.1037/a0021232
- Choi, S. (2020). The effects of social participation restriction on psychological distress among older adults with chronic illness. Journal of Gerontological Social Work, 63(8), 850–863. https://doi.org/10.1080/01634372.2020.1830217
- Connor, J. J., Girard, A., Iantaffi, A., Wiljamaa, S., & Mize, S. (2020). No expiration date: A qualitative inquiry of sexuality after 50. Sexual and Relationship Therapy, 38(2), 230–250. https://doi.org/10.1080/14681994.2020.1828575
- Cramer, A. O. J., Van Der Sluis, S., Noordhof, A., Wichers, M., Geschwind, N., Aggen, S. H., Kendler, K. S., & Borsboom, D. (2012). Dimensions of normal personality as networks in search of equilibrium: You can’t like parties if you don’t like people. European Journal of Personality, 26(4), 414–431. https://doi.org/10.1002/per.1866
- Cramer, A. O. J., Waldorp, L. J., van der Maas, H. L. J., & Borsboom, D. (2010). Comorbidity: A network perspective. Behavioral and Brain Sciences, 33(2–3), 137–150. https://doi.org/10.1017/S0140525X09991567
- Cunny, K. A., & Perri, M. (1991). Single-item vs multiple-item measures of health-related quality of life. Psychological Reports, 69(1), 127–130. https://doi.org/10.2466/pr0.1991.69.1.127
- CZSO. (2018). Informační Společnost v Číslech – [Information Society in Data 2018]. https://www.czso.cz/csu/czso/informacni-spolecnost-v-cislech
- DeLamater, J. (2012). Sexual expression in later life: A review and synthesis. The Journal of Sex Research, 49(2–3), 125–141. https://doi.org/10.1080/00224499.2011.603168
- DeLamater, J., Koepsel, E. R., & Johnson, T. (2019). Changes, changes? Women’s experience of sexuality in later life. Sexual & Relationship Therapy, 34(2), 211–227. https://doi.org/10.1080/14681994.2017.1412419
- Epskamp, S. (2020). Psychometric network models from time-series and panel data. Psychometrika, 85(1), 206–231. https://doi.org/10.1007/s11336-020-09697-3
- Epskamp, S., Costantini, G., Haslbeck, J., Isvoranu, A., Cramer, A. O., Waldorp, L. J., Schmittmann, V. D., & Borsboom, D. (2021). Package ‘Qgraph’ (1.9) [Computer Software]. https://cran.microsoft.com/snapshot/2017-08-01/web/packages/qgraph/
- Epskamp, S., & Fried, E. I. (2020). Package ‘Bootnet’(1.5) [Computer Software]. https://mran.revolutionanalytics.com/snapshot/2015-05-16/web/packages/bootnet/
- Epskamp, S., Waldorp, L. J., Mõttus, R., & Borsboom, D. (2018). The Gaussian graphical model in cross-sectional and time-series data. Multivariate Behavioral Research, 53(4), 453–480. https://doi.org/10.1080/00273171.2018.1454823
- Erens, B., Mitchell, K. R., Gibson, L., Datta, J., Lewis, R., Field, N., Wellings, K., & Tan, M. P. (2019). Health status, sexual activity and satisfaction among older people in Britain: A mixed methods study. PLoS One, 14(3), e0213835. https://doi.org/10.1371/journal.pone.0213835
- Estill, A., Mock, S. E., Schryer, E., & Eibach, R. P. (2018). The effects of subjective age and aging attitudes on mid-to late-life sexuality. The Journal of Sex Research, 55(2), 146–151. https://doi.org/10.1080/00224499.2017.1293603
- Faelens, L., Hoorelbeke, K., Fried, E., De Raedt, R., & Koster, E. H. W. (2019). Negative influences of Facebook use through the lens of network analysis. Computers in Human Behavior, 96, 13–22. https://doi.org/10.1016/j.chb.2019.02.002
- Fileborn, B., Hinchliff, S., Lyons, A., Heywood, W., Minichiello, V., Brown, G., Malta, S., Barrett, C., & Crameri, P. (2017). The importance of sex and the meaning of sex and sexual pleasure for men aged 60 and older who engage in heterosexual relationships: Findings from a qualitative interview study. Archives of Sexual Behavior, 46(7), 2097–2110. https://doi.org/10.1007/s10508-016-0918-9
- Fischer, N., Træen, B., & Hald, G. M. (2021). Predicting partnered sexual activity among older adults in four European countries: The role of attitudes, health, and relationship factors. Sexual and Relationship Therapy, 36(1), 3–21. https://doi.org/10.1080/14681994.2018.1468560
- Fisher, W. A., Donahue, K. L., Long, J. S., Heiman, J. R., Rosen, R. C., & Sand, M. S. (2015). Individual and partner correlates of sexual satisfaction and relationship happiness in midlife couples: Dyadic analysis of the international survey of relationships. Archives of Sexual Behavior, 44(6), 1609–1620. https://doi.org/10.1007/s10508-014-0426-8
- Floridi, G., Quashie, N. T., Glaser, K., & Brandt, M. (2022). Partner care arrangements and well-being in mid-and later life: The role of gender across care contexts. The Journals of Gerontology: Series B, 77(2), 435–445. https://doi.org/10.1093/geronb/gbab209
- Forbes, M. K., Eaton, N. R., & Krueger, R. F. (2017). Sexual quality of life and aging: A prospective study of a nationally representative sample. The Journal of Sex Research, 54(2), 137–148. https://doi.org/10.1080/00224499.2016.1233315
- Foygel, R., & Drton, M. (2010). Extended Bayesian information criteria for Gaussian graphical models. In J. Lafferty, C. Williams, J. Shawe-Taylor, R. Zemel, & A. Culotta (Eds.), Advances in neural information processing systems (Vol. 23., pp. 2020–2028). Curran Associates, Inc. https://proceedings.neurips.cc/paper_files/paper/2010/file/072b030ba126b2f4b2374f342be9ed44-Paper.pdf
- Freak-Poli, R., & Malta, S. (2020). An overview of sexual behaviour research in later life—Quantitative and qualitative findings. Australasian Journal on Ageing, 39(S1), 16–21. https://doi.org/10.1111/ajag.12773
- Funk, J. L., & Rogge, R. D. (2007). Testing the ruler with item response theory: Increasing precision of measurement for relationship satisfaction with the Couples Satisfaction Index. Journal of Family Psychology, 21(4), 572. https://doi.org/10.1037/0893-3200.21.4.572
- Geerkens, M. J. M., Al-Itejawi, H. H. M., Nieuwenhuijzen, J. A., Meuleman, E. J. M., Lissenberg-Witte, B. I., van Moorselaar, R. J. A., & Vis, A. N. (2020). Sexual dysfunction and bother due to erectile dysfunction in the healthy elderly male population: Prevalence from a systematic review. European Urology Focus, 6(4), 776–790. https://doi.org/10.1016/j.euf.2019.03.004
- Gewirtz-Meydan, A., Hafford-Letchfield, T., Benyamini, Y., Phelan, A., Jackson, J., & Ayalon, L. (2018). Ageism and sexuality. Contemporary Perspectives on Ageism, 149–162. https://doi.org/10.1007/978-3-319-73820-8
- Gillespie, B. J. (2017). Correlates of sex frequency and sexual satisfaction among partnered older adults. Journal of Sex and Marital Therapy, 43(5), 403–423. https://doi.org/10.1080/0092623X.2016.1176608
- Gore-Gorszewska, G. (2020). “Why not ask the doctor?” Barriers in help-seeking for sexual problems among older adults in Poland. International Journal of Public Health, 65(8), 1507–1515. https://doi.org/10.1007/s00038-020-01472-6
- Gore-Gorszewska, G. (2021). “What do you mean by sex?” a qualitative analysis of traditional versus evolved meanings of sexual activity among older women and men. Journal of Sex Research, 58(8), 1035–1049. https://doi.org/10.1080/00224499.2020.1798333
- Gore-Gorszewska, G., & Ševčíková, A. (2022). Trajectories of intimacy in later-life: A qualitative study of Czech and Polish narratives. Culture, Health & Sexuality, 25(10), 1–16. https://doi.org/10.1080/13691058.2022.2155708
- Gott, M., & Hinchliff, S. (2003a). Barriers to seeking treatment for sexual problems in primary care: A qualitative study with older people. Family Practice, 20(6), 690–695. https://doi.org/10.1093/fampra/cmg612
- Gott, M., & Hinchliff, S. (2003b). How important is sex in later life? The views of older people. Social Science & Medicine, 56(8), 1617–1628. https://doi.org/10.1016/S0277-9536(02)00180-6
- Gray, P. B., Garcia, J. R., & Gesselman, A. N. (2019). Age-related patterns in sexual behaviors and attitudes among single US adults: An evolutionary approach. Evolutionary Behavioral Sciences, 13(2), 111. https://doi.org/10.1037/ebs0000126
- Hall, A., Selby, J., & Vanclay, F. M. (1982). Sexual ageism. Australian Journal on Ageing, 1(3), 29–34. https://doi.org/10.1111/j.1741-6612.1982.tb01009.x
- Heidrich, S. M., & Powwattana, A. (2004). Self-discrepancy and mental health in older women with chronic illnesses. Journal of Adult Development, 11(4), 251–259. https://doi.org/10.1023/B:JADE.0000044528.54943.5f
- Heiman, J. R., Long, J. S., Smith, S. N., Fisher, W. A., Sand, M. S., & Rosen, R. C. (2011). Sexual satisfaction and relationship happiness in midlife and older couples in five countries. Archives of Sexual Behavior, 40(4), 741–753. https://doi.org/10.1007/s10508-010-9703-3
- Hinchliff, S., Carvalheira, A. A., Štulhofer, A., Janssen, E., Hald, G. M., & Træen, B. (2020). Seeking help for sexual difficulties: Findings from a study with older adults in four European countries. European Journal of Ageing, 17(2), 185–195. https://doi.org/10.1007/s10433-019-00536-8
- Hinchliff, S., & Gott, M. (2004). Intimacy, commitment, and adaptation: Sexual relationships within long-term marriages. Journal of Social and Personal Relationships, 21(5), 595–609. https://doi.org/10.1177/0265407504045889
- Hinchliff, S., Lewis, R., Wellings, K., Datta, J., & Mitchell, K. (2021). Pathways to help-seeking for sexual difficulties in older adults: Qualitative findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Age and Ageing, 50(2), 546–553. https://doi.org/10.1093/ageing/afaa281
- Hughes, A. K., Rostant, O. S., & Pelon, S. (2015). Sexual problems among older women by age and race. Journal of Women’s Health, 24(8), 663–669. https://doi.org/10.1089/jwh.2014.5010
- Isvoranu, A.-M., & Epskamp, S. (2023). Which estimation method to choose in network psychometrics? Deriving guidelines for applied researchers. Psychological Methods, 28(4), 925. https://doi.org/10.1037/met0000439
- Kennedy, C. E., Yeh, P. T., Li, J., Gonsalves, L., & Narasimhan, M. (2022). Lubricants for the promotion of sexual health and well-being: A systematic review. Sexual and Reproductive Health Matters, 29(3), 2044198. https://doi.org/10.1080/26410397.2022.2044198
- Kenny, D. A., Kaniskan, B., & McCoach, D. B. (2015). The performance of RMSEA in models with small degrees of freedom. Sociological Methods & Research, 44(3), 486–507. https://doi.org/10.1177/0049124114543236
- Kontula, O., & Haavio-Mannila, E. (2009). The impact of aging on human sexual activity and sexual desire. The Journal of Sex Research, 46(1), 46–56. https://doi.org/10.1080/00224490802624414
- Langner, L. A., & Furstenberg, F. F. (2020). Gender differences in spousal caregivers’ care and housework: Fact or fiction? The Journals of Gerontology: Series B, 75(1), 173–183. https://doi.org/10.1093/geronb/gby087
- Lapp, L. K., & Spaniol, J. (2016). Aging and self-discrepancy: Evidence for adaptive change across the life span. Experimental Aging Research, 42(2), 212–219. https://doi.org/10.1080/0361073X.2016.1132900
- Lee, D. M., Nazroo, J., O’Connor, D. B., Blake, M., & Pendleton, N. (2016). Sexual health and well-being among older men and women in England: Findings from the english longitudinal study of ageing. Archives of Sexual Behavior, 45(1), 133–144. https://doi.org/10.1007/s10508-014-0465-1
- Levy, B. (2009). Stereotype embodiment: A psychosocial approach to aging. Current Directions in Psychological Science, 18(6), 332–336. https://doi.org/10.1111/j.1467-8721.2009.01662.x
- Lindau, S. T., Schumm, L. P., Laumann, E. O., Levinson, W., O’Muircheartaigh, C. A., & Waite, L. J. (2007). A study of sexuality and health among older adults in the United States. New England Journal of Medicine, 357(8), 762–774. https://doi.org/10.1056/NEJMoa067423
- Lišková, K. (2018). Sexual liberation, socialist style: Communist Czechoslovakia and the science of desire, 1945–1989. Cambridge University Press. https://doi.org/10.1017/slr.2019.284
- Liu, H., Lafferty, J., & Wasserman, L. (2009). The nonparanormal: Semiparametric estimation of high dimensional undirected graphs. Journal of Machine Learning Research, 10(10).
- Lodge, A. C., & Umberson, D. (2012). All shook up: Sexuality of mid- to later life married couples. Journal of Marriage and Family, 74(3), 428–443. https://doi.org/10.1111/j.1741-3737.2012.00969.x
- Malgaroli, M., Maccallum, F., & Bonanno, G. A. (2018). Symptoms of persistent complex bereavement disorder, depression, and PTSD in a conjugally bereaved sample: A network analysis. Psychological Medicine, 48(14), 2439–2448. https://doi.org/10.1017/S0033291718001769
- Manea, B. C., & Rabušic, L. (2020). Value modernisation in central and Eastern European countries: How does Inglehart’s theory work? Sociologický Časopis/Czech Sociological Review, 56(6), 699–740.
- Minichiello, V., Plummer, D., & Loxton, D. (2000). Knowledge and beliefs of older Australians about sexuality and health. Australasian Journal on Ageing, 19(4), 190–194. https://doi.org/10.1111/j.1741-6612.2000.tb00234.x
- Mitchell, K. R., Mercer, C. H., Ploubidis, G. B., Jones, K. G., Datta, J., Field, N., Copas, A. J., Tanton, C., Erens, B., & Sonnenberg, P. (2013). Sexual function in Britain: Findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Lancet, 382(9907), 1817–1829. https://doi.org/10.1016/S0140-6736(13)62366-1
- Monteiro, A., von Humboldt, S., & Leal, I. (2017). How do formal caregivers experience the sexuality of older adults? Beliefs and attitudes towards older adults’ sexuality. Psychology, Community & Health, 6(1), 77–92. https://doi.org/10.5964/pch.v6i1.216
- Petrík, Š. (2020). Sexual behavior of men and women in Slovakia: Selected specifics. https://www.researchgate.net/profile/Stefan-Petrik-2/publication/346624101_Sexual_behavior_of_men_and_women_in_Slovakia_-_selected_specifics/links/5fc9df1c299bf188d4f15b5f/Sexual-behavior-of-men-and-women-in-Slovakia-selected-specifics.pdf
- Rahn, A., Bennett, C., Jones, T., & Lykins, A. (2020). Happily partnered older adults’ relationship-enhancing behaviours. Australasian Journal on Ageing, 39(S1), 30–39. https://doi.org/10.1111/ajag.12731
- Reed, A. E., Chan, L., & Mikels, J. A. (2014). Meta-analysis of the age-related positivity effect: Age differences in preferences for positive over negative information. Psychology and Aging, 29(1), 1–15. https://doi.org/10.1037/a0035194
- Rosen, R. C., Cappelleri, J. C., Smith, M. D., Lipsky, J., & Peña, B. M. (1999). Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. International Journal of Impotence Research, 11(6), 319–326. https://doi.org/10.1038/sj.ijir.3900472
- Rosen, R. C., Heiman, J. R., Long, J. S., Fisher, W. A., & Sand, M. S. (2016). Men with sexual problems and their partners: Findings from the international survey of relationships. Archives of Sexual Behavior, 45(1), 159–173. https://doi.org/10.1007/s10508-015-0568-3
- Sandberg, L. (2013). Affirmative old age: The ageing body and feminist theories on difference. International Journal of Ageing & Later Life, 8(1), 11–40. https://doi.org/10.3384/ijal.1652-8670.12197
- Schmittmann, V. D., Cramer, A. O. J., Waldorp, L. J., Epskamp, S., Kievit, R. A., & Borsboom, D. (2013). Deconstructing the construct: A network perspective on psychological phenomena. New Ideas in Psychology, 31(1), 43–53. https://doi.org/10.1016/j.newideapsych.2011.02.007
- Ševčíková, A., Blinka, L., Židlická, A., & Faltýnková, A. (2021). Sexual difficulties in people 50+: A content analysis of sex-related queries posted on professional counseling websites. Health Communication, 38(5), 958–966. https://doi.org/10.1080/10410236.2021.1984629
- Ševčíková, A., Gottfried, J., Gocieková, V., Gore-Gorszewska, G., Blinka, L., & Kotík, J. (2023). The role of non-penetrative partnered sex activities in the associations among erectile difficulties, sex and relationship satisfaction in men aged 50+. International Journal of Sexual Health, 35(1), 30–40. https://doi.org/10.1080/19317611.2023.2169850
- Ševčíková, A., & Sedláková, T. (2020). The role of sexual activity from the perspective of older adults: A qualitative study. Archives of Sexual Behavior, 49(3), 969–981. https://doi.org/10.1007/s10508-019-01617-6
- Shen, S. (2019). Chronic disease burden, sexual frequency, and sexual dysfunction in partnered older adults. Journal of Sex & Marital Therapy, 45(8), 706–720. https://doi.org/10.1080/0092623X.2019.1610127
- Sinković, M., & Towler, L. (2019). Sexual aging: A systematic review of qualitative research on the sexuality and sexual health of older adults. Qualitative Health Research, 29(9), 1239–1254. https://doi.org/10.1177/1049732318819834
- Skoblow, H. F., Drewelies, J., & Proulx, C. M. (2023). Sexual activity and satisfaction in older adult dyads: The role of perceptions of aging. The Gerontologist, 63(2), 251–260. https://doi.org/10.1093/geront/gnac099
- Steklíková, E. (2014). Sexualita seniorů [Sexuality of Elderly People]. [ Unpublished Master’s Thesis]. Charles University. Czech Republic.
- Štulhofer, A., Hinchliff, S., & Træen, B. (2020). Relationship intimacy, sexual distress, and help-seeking for sexual problems among older European couples: A hybrid dyadic approach. International Journal of Impotence Research, 32(5), 525–534. https://doi.org/10.1038/s41443-019-0214-z
- Štulhofer, A., Jurin, T., Graham, C., Enzlin, P., & Træen, B. (2019). Sexual well-being in older men and women: Construction and validation of a multi-dimensional measure in four European countries. Journal of Happiness Studies, 20(7), 2329–2350. https://doi.org/10.1007/s10902-018-0049-1
- Syme, M. L., & Cohn, T. J. (2021). Aging sexual stereotypes and sexual expression in mid-and later life: Examining the stereotype matching effect. Aging & Mental Health, 25(8), 1507–1514. https://doi.org/10.1080/13607863.2020.1758909
- Syme, M. L., Cohn, T. J., Stoffregen, S., Kaempfe, H., & Schippers, D. (2019). “At my age … ”: Defining sexual wellness in mid-and later life. The Journal of Sex Research, 56(7), 832–842. https://doi.org/10.1080/00224499.2018.1456510
- Team, R. D. C. (2011). R: A language and environment for statistical computing. R Foundation for Statistical Computing. http://www.r-project.org/
- Tetley, J., Lee, D. M., Nazroo, J., & Hinchliff, S. (2018). Let’s talk about sex–What do older men and women say about their sexual relations and sexual activities? A qualitative analysis of ELSA wave 6 data. Ageing & Society, 38(3), 497–521. https://doi.org/10.1017/S0144686X16001203
- Tinetti, A., Weir, N., Tangyotkajohn, U., Jacques, A., Thompson, J., & Briffa, K. (2018). Help-seeking behaviour for pelvic floor dysfunction in women over 55: Drivers and barriers. International Urogynecology Journal, 29(11), 1645–1653. https://doi.org/10.1007/s00192-018-3618-2
- Towler, L. B., Graham, C. A., Bishop, F. L., & Hinchliff, S. (2021). Older adults’ embodied experiences of aging and their perceptions of societal stigmas toward sexuality in later life. Social Science & Medicine, 287, 114355. https://doi.org/10.1016/j.socscimed.2021.114355
- Towler, L. B., Graham, C. A., Bishop, F. L., & Hinchliff, S. (2022). Sex and relationships in later life: Older adults’ experiences and perceptions of sexual changes. The Journal of Sex Research, 60(9), 1318–1331. https://doi.org/10.1080/00224499.2022.2093322
- Træen, B., Carvalheira, A. A., Hald, G. M., Lange, T., & Kvalem, I. L. (2019). Attitudes towards sexuality in older men and women across Europe: Similarities, differences, and associations with their sex lives. Sexuality & Culture, 23(1), 1–25. https://doi.org/10.1007/s12119-018-9564-9
- Træen, B., Carvalheira, A., Kvalem, I. L., & Hald, G. M. (2018). European older adults’ use of the internet and social networks for love and sex. Cyberpsychology: Journal of Psychosocial Research on Cyberspace, 12(3), i55–i66. https://doi.org/10.5817/CP2018-3-1
- Van Borkulo, C. D., van Bork, R., Boschloo, L., Kossakowski, J. J., Tio, P., Schoevers, R. A., Borsboom, D., & Waldorp, L. J. (2022). Comparing network structures on three aspects: A permutation test. Psychological Methods, 28(6), 1273–1285. https://doi.org/10.1037/met0000476
- Waite, L. J., Laumann, E. O., Das, A., & Schumm, L. P. (2009). Sexuality: Measures of partnerships, practices, attitudes, and problems in the national social life, health, and aging study. The Journals of Gerontology: Series B, 64B(suppl_1), i56–i66. https://doi.org/10.1093/geronb/gbp038
- Wassersug, R. J., Westle, A., & Dowsett, G. W. (2017). Men’s sexual and relational adaptations to erectile dysfunction after prostate cancer treatment. International Journal of Sexual Health, 29(1), 69–79. https://doi.org/10.1080/19317611.2016.1204403
- Weiss, P., & Zvěřina, J. (2001). Sexuální chování v ČR: situace a trendy. Portál.
- Wettstein, M., Wahl, H.-W., & Kornadt, A. E. (2021). Longitudinal associations between perceived stress and views on aging: Evidence for reciprocal relations. Psychology and Aging, 36(6), 752. https://doi.org/10.1037/pag0000632
- White, C. B. (1982). A scale for the assessment of attitudes and knowledge regarding sexuality in the aged. Archives of Sexual Behavior, 11(6), 491–502. https://doi.org/10.1007/BF01542474
- White, C. B. (1998). Aging sexual knowledge and attitudes scale. In C. M. Davis, W. L. Yarber, R. Bauserman, G. Schreer, & S. L. Davis (Eds.), Handbook of sexuality-related measures (1st ed., pp. 66–69). Routledge.
- Williams, L. A., Giddings, L. S., Bellamy, G., & Gott, M. (2017). ‘Because it’s the wife who has to look after the man’: A descriptive qualitative study of older women and the intersection of gender and the provision of family caregiving at the end of life. Palliative Medicine, 31(3), 223–230. https://doi.org/10.1177/0269216316653275
- Wongkamthong, C., & Akande, O. (2023). A comparative study of imputation methods for multivariate ordinal data. Journal of Survey Statistics and Methodology, 11(1), 189–212. https://doi.org/10.1093/jssam/smab028
- Wurm, S., Warner, L. M., Ziegelmann, J. P., Wolff, J. K., & Schüz, B. (2013). How do negative self-perceptions of aging become a self-fulfilling prophecy? Psychology and Aging, 28(4), 1088. https://doi.org/10.1037/a0032845
- Zhao, T., Liu, H., Roeder, K., Lafferty, J., & Wasserman, L. (2012). The huge package for high-dimensional undirected graph estimation in R. The Journal of Machine Learning Research, 13(1), 1059–1062. https://doi.org/10.48550/arxiv.2006.14781