
Abstract
Demographic research has paid much attention to the impact of childhood conditions on adult mortality. We focus on one of the key aspects of early life conditions, sibling group size, and examine the causal effect of growing up in a large family on mortality. While previous studies have focused on low- or middle-income countries, we examine whether growing up in a large family is a disadvantage in Sweden, a context where most parents have adequate resources, which are complemented by a generous welfare state. We used Swedish register data and frailty models, examining all-cause and cause-specific mortality between the ages of 40 and 74 for the 1938–72 cohorts, and also a quasi-experimental approach that exploited multiple births as a source of exogenous variation in the number of siblings. Overall our results do not indicate that growing up in a large family has a detrimental effect on longevity in Sweden.
Introduction
Recent years have seen researchers across the social sciences directing their attention towards the long-term consequences of early life conditions, especially in terms of the quality and duration of life (Galobardes et al. Citation2004; Bengtsson and Mineau Citation2009; Myrskylä Citation2010). There is a growing body of literature examining the relationship between socio-economic status (SES), family structure, and health in early childhood in relation to adult mortality (Bengtsson and Lindström Citation2000; Gluckman et al. Citation2008; Bengtsson and Broström Citation2009; Gagnon and Mazan Citation2009; Huang and Elo Citation2009; Van den Berg et al. Citation2009; Barclay and Kolk Citation2015). However, there have been very few studies examining the relationship between number of siblings and longevity (Hart and Smith Citation2003; Smith et al. Citation2009; Donrovich et al. Citation2014). The study reported in this paper aimed to examine whether the necessity of dividing parental resources among a large number of children has a long-lasting effect on the duration of those individuals’ lives. First, we examined the impact of family size on both all-cause and cause-specific mortality using Swedish administrative register data and event history analysis. Second, we used a quasi-experimental design to estimate the isolated effect on mortality of an additional sibling, through an exogenous increase in the size of the sibling group due to a twin birth.
Many previous studies that examine the way in which number of siblings is related to health or mortality have focused on outcomes that can be observed among infants and small children (Glick et al. Citation2007; Baez Citation2008; Henderson et al. Citation2008; Rosenzweig and Zhang Citation2009; Millimet and Wang Citation2011), and therefore do not provide evidence on the long-term effects of growing up in a large family. Moreover, previous studies have almost exclusively used data from low- or middle-income countries, or historical populations (Hart and Smith Citation2003; Smith et al. Citation2009; Hatton and Martin Citation2010; Gagnon and Bohnert Citation2012). While this body of research has provided a number of interesting insights, the results of these studies must be interpreted in the light of their contexts of harsh economic conditions and limited access to state support. There is very little evidence of how family size may affect adult mortality in developed, higher-income countries. Understanding whether the impact of the number of siblings is conditional on the context is crucial from a policy perspective. Some pathways by which number of siblings would affect mortality have been successfully removed through policy measures and governmental health spending (such as on early child health) in higher-income societies, while others such as parental time investment are likely to still be of relevance.
The aim of the study reported in this paper was to examine the impact of family size on adult mortality in Sweden, a developed country with a welfare state system that provides generous support for families with children. Infant mortality in Sweden had already seen a profound decline in the nineteenth century (Perrenoud Citation1984). During the twentieth century, Sweden’s Social Democratic governments developed extensive welfare programmes aimed at reducing poverty and decreasing inequalities (Sundin and Willner Citation2007). In response to growing concerns about declining population in the 1930s (Myrdal and Myrdal Citation1934), the government began implementing programmes with the goal of making it possible to combine work and family. This resulted in very stable cohort fertility patterns for the rest of the twentieth century. One such reform was the introduction of child allowances in 1948, which gave benefits for each additional child in a family (Hoem and Hoem Citation1996). These programmes were complemented by major programmes focused on child and infant health, resulting in some of the world’s lowest infant and child mortality rates (Sundin and Willner Citation2007). The period after the Second World War also saw continuous expansion of pre-school childcare. Given the favourable economic and institutional contexts of Sweden, we can expect any mortality disadvantage for children raised in larger families to be less profound than in the contexts studied in previous research on the long-term health consequences of family size.
Theory and empirical research
Theory
The relationship between number of children and their survival is a classical demographic question that is fundamental for theories of demographic change as well as central to evolutionary theories on parental investment and optimal number of offspring. Researchers have predicted that an increase in fertility will decrease the probability of survival for each child (Kaplan Citation1996). Classical theories on the demographic transition see a reduction in mortality in infancy and early adulthood as the main explanation for the demographic transition and eventual reduction of average family size (Taylor et al. Citation1976; Preston Citation1978; Scrimshaw Citation1978; Cleland Citation2001). Much of this theory is concerned with mortality early in life, but it seems plausible that with increasing societal longevity, parents would also be increasingly concerned about whether their children will survive into late adulthood. The idea that parents make a trade-off between the number of children and the investment in each child is still of relevance in both contemporary developed and less developed populations, though increased affluence has likely reduced the link between resources and fertility (Scrimshaw Citation1978; Yamada Citation1984; Aksan Citation2014).
Several theories have been proposed in the sociological, economic, and demographic literature to account for why children reared in large sibling groups should experience poorer later-life outcomes in contemporary developed populations, independent of confounding factors such as the SES of the parents. These include the resource dilution hypothesis (Blake Citation1981) and the model of trade-off between child quality and quantity (Becker and Lewis Citation1973; Becker and Tomes Citation1976). Both theories suggest that parents face trade-offs between the investment in each child and the total number of children. If parental investment is associated with health, including in later life, we would expect to observe a relationship between number of siblings and mortality.
According to the resource dilution model (Blake Citation1981), developed in the sociological and demographic literature, a child’s development is heavily influenced by the degree of parental resource investment. These resources include not only financial means, but also the amount of time and attention paid to each child, which may in turn translate into the child having better educational outcomes, a lower propensity to engage in risky behaviours, and an increase in the likelihood of the child adopting a healthy lifestyle (Mercy and Steelman Citation1982; Evans Citation2006). It should be noted that parental time is constrained even in affluent societies, and this might be particularly so in contexts with high labour force participation among women such as in Sweden. A relative lack of parental investment in childhood might be related to worse adult socio-economic outcomes, which are known to be associated with poor mortality outcomes. The resource dilution model is also applicable to household space: the negative effect of family size on the physical and mental health of the child may be exacerbated through household overcrowding (Burström et al. Citation1999; Solari and Mare Citation2012). Living in a home environment that provides insufficient space and privacy for the inhabitants has been shown to raise levels of stress, impede interpersonal relations within the family, and to have detrimental consequences for academic performance and health (Evans Citation2006; Jaine et al. Citation2011). Moreover, research shows that household overcrowding is a risk factor in the transmission of serious diseases, even in developed nations (Baker et al. Citation2008), as exposure to aggressive pathogens early in life may have a detrimental effect on long-term health (Mucci et al. Citation2004; Bengtsson and Broström Citation2009).
Given that parental material and non-material resources are constrained, each additional child decreases the per child investments made by parents (Hertwig et al. Citation2002). However, the resource dilution hypothesis may operate through birth order as well as family size (Rodgers Citation2001). The size of the sibling group is not fixed at birth, unless you happen to be the last-born child, and a first-born in a five-child sibling group is likely to spend the majority of his or her childhood without four other siblings. Previous research indicates that there is an independent effect of birth order on adult mortality (Barclay and Kolk Citation2015), and this may mediate the importance of the size of the sibling group, suggesting increased disadvantage at high birth orders in large families.
The predictions of a negative impact of family size on child health can also be found in the economic literature. According to theoretical models proposed by Becker and Lewis (Citation1973) as well as Becker and Tomes (Citation1976), parents face trade-offs between investing in the quantity and quality of children when making decisions regarding the size of their family. Early life health is a key dimension of investment in offspring ‘quality’. A favourable home environment, regular access to health care, and parents taking care to shape a healthy lifestyle for their children may have important long-term consequences for the health and longevity of offspring in adulthood (Currie and Madrian Citation1999; Yeung et al. Citation2002; Case and Paxson Citation2010). Hence, an exogenous increase in sibship size, such as a multiple birth, may lead to poorer health outcomes and higher mortality rates among offspring. Although most interpretations of the resource dilution hypothesis, as well as the quality–quantity trade-off model, focus on childhood experiences, it is also possible to extend the application of these theories over the whole life course. This is particularly clear when considering how any potential inheritance from the parents may be divided among the adult siblings.
The health of children may also be influenced by the health of their parents. Being raised in a large family necessarily means that the parents have raised a large number of children, and the number of children born and raised has been shown to be associated with mortality risk for both mothers and fathers (Doblhammer Citation2000; Grundy and Kravdal Citation2007; Engelman et al. Citation2010; Hank Citation2010). Several explanations have been proposed for the relationship between parity and mortality, but those that could also potentially impact the health of the children include the fact that parenthood implies stress related to childrearing responsibilities, pressure to combine labour market participation with childrearing, and lower opportunities for the accumulation of savings (Aassve et al. Citation2006; Schultz Citation2007). Moreover, due to intergenerational transmission of fertility (Kolk Citation2014), higher fertility in the offspring generation may lead to higher fertility in subsequent generations, which might in turn be related to worse health outcomes.
The impact of family size on the life chances of children may also be moderated by the sex composition of the sibling group (for a detailed overview, see Steelman et al. Citation2002). The sex composition of siblings may affect the normative climate within a household (Powell and Steelman Citation1989, Citation1990). For example, girls tend to achieve more highly and adopt healthier lifestyles than boys, and this may have an influence on their brothers. As a result, daughters may contribute towards generating a family environment with higher expectations for children in comparison to families that only have sons, which in the long term may lead to better health outcomes and lower mortality for individuals who grew up in families with more women. As a consequence, the presence of sisters may positively affect long-term life chances. Moreover, in societies in which parents have a strong preference for sons or expect relatively lower benefits from human capital investments in daughters, brothers will be stronger competitors for parental resources than sisters (Parish and Willis Citation1993; Garg and Morduch Citation1998; Morduch Citation2000). Hence, the number of brothers may have a stronger negative impact on a child’s life chances than the number of sisters.
While the literature overall provides many arguments for family size having a negative impact on the life chances of the child, it is also possible that having a large number of siblings might be beneficial in adulthood. Sibling relations vary in terms of frequency of contacts, and may be either a source of support or of conflict. Siblings typically share a common background and history, and hence sibling ties commonly extend across the life course (Knipscheer and Van Tilburg Citation2013). This matters for long-term health outcomes, because social support from kin is related to health in adulthood (Seeman Citation2000; Rostila et al. Citation2012). Furthermore, children may benefit from interactions with their siblings during childhood in order to learn and practice interpersonal skills, self-control, or conflict resolution techniques, which may be helpful later on in life in developing their relationships with peers (Whiteman et al. Citation2011; Downey et al. Citation2015). Social ties in turn have a strong positive long-term impact on health and longevity (Berkman Citation1984; Berkman and Glass Citation2000; Eng et al. Citation2002; Cohen Citation2004; Gagnon and Mazan Citation2009). All in all, it can be presumed that having a greater number of siblings increases the possibility of being able to seek social and financial support in adulthood, if and when that support might be needed, which may improve both the quality and duration of human life.
Review of empirical research
Previous research on the relationship between family size and health has mainly used contemporary data from low- or middle-income countries such as Romania, Colombia, China, and Indonesia (Glick et al. Citation2007; Baez Citation2008; Henderson et al. Citation2008; Rosenzweig and Zhang Citation2009; Millimet and Wang Citation2011). This body of work has typically focused on the health outcomes of very young children. The results of these studies generally show that an additional child in the household has a negative effect on children’s nutrition (Glick et al. Citation2007; Henderson et al. Citation2008), weight (Rosenzweig and Zhang Citation2009), and height (Hatton and Martin Citation2010; Millimet and Wang Citation2011). In less developed countries, growing up in a large family increases the likelihood of sharing a room and reduces the chance of having access to clean water and sanitary sewerage facilities (Baez Citation2008). Studies using historical data have also found that an additional sibling in the household is negatively associated with longevity (Hart and Smith Citation2003; Gagnon and Mazan Citation2009; Smith et al. Citation2009; Hatton and Martin Citation2010; Gagnon and Bohnert Citation2012; Donrovich et al. Citation2014).
While these studies do demonstrate a negative effect of family size on child health, the context of much of this previous work has been harsh economic conditions and little or no access to state support. There is limited evidence on how family size may affect health in higher-income developed countries, and the few available studies show rather mixed results. Larger family size was not found to be related to mortality from coronary heart disease among Finns in a study carried out by Eriksson et al. (Citation1999). In the Swedish context, according to findings reported by Weitoft et al. (Citation2003), the death rate in childhood among children living in larger families is lower than among their peers living in small families. One Swedish study has found that growing up in a family with more than five children, compared with growing up in a smaller family, was associated with poorer health and higher mortality in late adulthood during a three-year follow-up period after age 80 (Lundberg Citation1993).
Poor conditions for health in childhood may result in profound long-term consequences and decrease the quality and duration of life among adults (Case and Paxson Citation2010). However, given ambiguous conclusions from previous studies that describe associations between the number of siblings and child health in less developed countries, it is very difficult to predict the long-term impact of family size on health outcomes in adult life in more developed nations. It is therefore unclear whether or not growing up in a large family would be expected to have a negative effect on child well-being when parents have adequate resources and access to support from a welfare state system.
Data, study design, and methods
Data
We used data from the Swedish administrative registers, which cover the full population, focusing on cohorts born between 1938 and 1972. We examined mortality from age 40 onwards and followed our study population until 2012, when the earliest cohort had reached age 74. We right censored individuals at first emigration. The Swedish multigenerational registers allowed us to link offspring to their parents, and therefore also to their siblings. The digitized Swedish register data are based on the 1960 census, so our population of index individuals and siblings is conditioned on survival to 1960. The analysis population consisted of individuals born in Sweden whose personal identity number could be linked to the personal identity numbers of both their mother and father, which therefore also allowed us to link them to their full biological siblings. The advantage of this register dataset is that even though we looked at a society with fertility levels typical for developed countries, we could still capture the impact of having large numbers of siblings, because of the exceptionally large sample that covered the whole population. The size of the registers was also required to apply our quasi-experimental approach that exploits multiple births as a source of exogenous variation in the number of siblings, as multiple births are very uncommon in most other data sources.
The registers contain information on year and month of birth, which made it possible both to identify children born as part of a multiple birth and to establish the birth order of siblings. We based all our family size variables on groups of siblings that all shared their biological mother and father. We also excluded all individuals with half-siblings, thereby restricting our population to sibling groups where neither parent had any children with a different partner. In total our analysis population consisted of 1,354,253 men and 1,284,645 women born in cohorts from 1938 to 1972. The earliest birth cohorts who could be linked to the mother and father were those born in 1932, and the latest point for which we had data was 2012. Therefore, our calculations of number of siblings were based on siblings born between 1932 and 2012. It is likely that we have underestimated the number of siblings in the earliest birth cohorts to a small extent, as we cannot link siblings who were born before 1932.
In the analysis of mortality using data on twins, we used a subsequent twin birth in the family as a risk factor for their siblings. Among men we found 4,888 first-born index persons who experienced a twin birth at their mother’s parity two, 4,569 first- and second-born index persons who experienced a twin birth at parity three, 2,500 first-, second-, and third-born index persons who experienced a twin birth at parity four, and 1,279 first-, second-, third-, and fourth-born index persons who experienced a twin birth at parity five. The mortality analysis for women included 4,630 first-born index persons who experienced a twin birth at parity two, 4,237 first- and second-born index persons who experienced a twin birth at parity three, 2,330 first-, second-, and third-born index persons who experienced a twin at parity four, and 1,217 first-, second-, third-, and fourth-born index persons who experienced a twin birth at parity five. Triplets and larger multiple births in the data were excluded from the analysis.
Using these data, we carried out analyses using a hazard model framework. We estimated frailty models as well as hazard models using twins data, which are described in more detail in the next two sections. We analysed both all-cause and cause-specific mortality. The reason for the latter analyses is that if the number of siblings was found to be particularly related to certain causes of death then that would allow us to gain an insight into the pathways by which family size is related to mortality in adulthood. For example, mortality due to cancer may be a consequence of social contagion of risky behaviours among siblings (e.g., smoking). On the other hand, mortality from external causes, often related to violence, suicide, or substance abuse, is more commonly associated with social disadvantage in mid-adulthood. Our main analyses focused on all-cause mortality, but we also present results for the most common causes of death, examining mortality attributable to neoplasms (cancers), diseases of the circulatory system, external causes, and then all other remaining causes grouped together. All statistical analyses were carried out using the ‘st’ suite of commands for event history analysis available in Stata 13 (StataCorp Citation2013).
Frailty models
Our main analyses consisted of Gompertz proportional hazard models with shared frailty that is assumed to follow a Gamma distribution (Vaupel and Missov Citation2014). Shared frailty is used in order to account for unobserved shared factors at the family level that may be related to mortality. Previous research has shown that in the Swedish context, family-level factors may explain a substantial proportion of the variance in mortality (Hemminki et al. Citation2001; Edvinsson et al. Citation2005). The hazard for individual i (i = 1, … , n) in family cluster j (j = 1, … , n) in our model took the following form:where t denotes age,
is a vector of observable covariates, β is a vector of unknown regression coefficients describing the effect of the covariates,
is the Gompertz baseline hazard function, and
is an unobserved (random) effect or frailty following a gamma distribution. The Gompertz baseline hazard assumes an exponential increase in the baseline hazard with time, therefore, we checked that assumption and found that it was met. We also used chi-square tests to examine whether the estimates are proportional over time in the fully adjusted models for men and women. The results of these tests confirmed that our key explanatory variable did not violate the proportional hazards assumption. The only variable that did consistently violate the proportional hazards assumption was the cohort indicator, and the separate analyses by cohort revealed that the estimates for the relationship between the size of the sibling group and mortality were very similar for different cohort groups.
presents descriptive information for men and women, including number of deaths, and baseline mortality rates for different covariates. In addition to covariates on sibling group size and cohort, we included covariates on age of the mother at the time of birth, and birth order in the sibling group, as well as parental SES. Our SES measure consisted of the Erikson, Goldthorpe, and Portocarero social class scheme (EGP) (Erikson et al. Citation1979) applied at the household level and measured between ages 30 and 40 using information on occupation from the Swedish censuses of 1960, 1970, 1980, and 1990. The EGP variable used in this study was divided into the following categories: upper service class, including self-employed professionals (EGP = I); lower service class (EGP = II); routine non-manual (EGP = III); self-employed non-professionals, farmers, and fishermen (EGP = IV); skilled and unskilled workers (EGP = V–VII); and unknown/other.
Table 1 Descriptive statistics for analysis population of Swedish men and women born 1938–72
In we present the distributions of men and women across sibling group sizes and periods of time. This analysis shows that across time family sizes were converging towards a pattern with two or three children, with decreasing proportions of children raised with no siblings or with a large number of siblings. also shows that infant mortality rates decreased substantially across these cohorts, from 2,196 deaths down to 728 deaths per 100,000 births among boys and from 1,582 deaths down to 504 deaths per 100,000 births among girls.
Table 2 Distribution of men and women in Sweden across sibling group sizes by cohort (per cent) and infant mortality (number of deaths per 100,000 births)
Hazard models using twins data
The number of children is not randomly distributed across families and may differ according to factors which cannot be directly observed. Indeed, one of the key insights from the quality–quantity trade-off model is that parents take the well-being of their offspring into account when they decide whether or not to have another child (Becker and Lewis Citation1973; Becker and Tomes Citation1976), which implies endogeneity of sibship size with respect to health and longevity. Furthermore, lower-than-intended fertility in the parental generation likely correlates with increased mortality in the progeny if low fertility is due to health problems that may be inherited.
The frailty models described in the previous section do not solve problems of selection, because they assume independence between unobserved factors and covariates. In order to look beyond the association between number of siblings and mortality, and to understand the causal relationship between an additional exogenous sibling and mortality, we used the econometric approach proposed by Rosenzweig and Wolpin (Citation1980). This approach uses information on multiple births in order to examine the impact on mortality of an exogenous increase in the number of children. Multiple births are, to most extents and purposes, an outcome of a random process and not the result of a deliberate parental decision driven by a calculus considering future child welfare. Thus, information on twin births can be applied to reveal the causal effect of the number of siblings on outcomes such as mortality. The approach proposed by Rosenzweig and Wolpin (Citation1980) can be regarded as comparable to a natural experiment and has opened up new opportunities for research on the outcomes of different family sizes (Moffitt Citation2005; Schultz Citation2007).
Another instrumental variable used in the literature about the impact of the number of siblings on child well-being is the sex composition of siblings. This alternative has three disadvantages. First, the strong impact on the number of children in a family can be observed only in some specific countries with strong preferences for a specific composition of sex among siblings. Second, the analysis that uses such an instrumental variable needs to exclude families with fewer than three children. Finally, there are studies which show that sex structure of siblings is correlated with children’s outcomes (see, e.g., Conley Citation2000). Hence, both relevance and validity of this instrument are potentially problematic and, therefore, we decided not to use sex composition as a variable in the instrumental variable models.
Our analyses were based on what is often referred to as the reduced form relationship between an instrumental variable and the outcome, in this case a twin birth and mortality. Thus, in a strict sense we identified the causal relationship and effect size of a subsequent twin birth, and thus two siblings and mortality, rather than the relationship between one additional sibling and mortality. A twin birth is a very strong predictor of family size (Åslund and Grönqvist Citation2010), which means that there is a very close relationship between the experience of a twin birth in the family and higher completed family size (compare also ). It should be noted that there is a closer relationship between twin births and eventual number of siblings at birth orders above two. Previous examples of the application of this approach can be seen in Glick et al. (Citation2007) and Jacobsen et al. (Citation1999). Reduced form estimates possess many attractive features, although they are less easily interpreted than traditional instrumental variable estimates (Chernozhukov and Hansen Citation2008). Our models were similar to the survival analysis models described earlier, and use the same period, cohort, and age restrictions. However, the twin-focused models exclude covariates for birth order. The effect of an exogenous twin birth on the mortality of siblings born before the twin birth was based on the inclusion of a binary covariate indicating the existence or absence of a subsequent twin birth. Hence, the vector of observable covariates used in the previous version of models included a dummy variable distinguishing individuals who experienced a twin birth after their own birth. The coefficient corresponding to the twin birth measures the effect of ‘randomly assigned’ additional siblings, because twins are an exogenous source of variation in family size.
Table 3 Correlation of twin births with sibling group size according to birth order of twins
A large number of studies using Swedish and Nordic data have used and evaluated the exogeneity of a twin birth and have found that it meets stringent demands on exogeneity (Black et al. Citation2005, Citation2010; Åslund and Grönqvist Citation2010; Holmlund et al. Citation2013). Additionally, the relevance of this instrument is assessed in our own analysis in . The correlation between a twin birth and family size varies from 0.733 at early parities to 0.818 at later parities.
The most important socio-demographic determinant (and potential confounder) of the probability of a twin birth, maternal age, was adjusted for in our models. We studied cohorts born before the introduction of assisted reproductive technologies (the first in vitro fertilization birth in Sweden took place in 1982), as their introduction reduces the degree to which multiple births can be considered an exogenous shock.
An important challenge that arises using the approach proposed by Rosenzweig and Wolpin (Citation1980) is related to the fact that the medical literature shows that children in multiple births tend to be born with a lower birthweight, which is in turn related to poorer health outcomes later in life. A solution proposed by Black et al. (Citation2010) relies on restricting the sample to the older siblings of children born in the multiple births. Specifically, we constructed an indicator of a multiple birth at birth n, limited the analytical sample to children born in families that experienced at least n births, and then examined the mortality of children born before the nth birth. In other words, multiple births were used to construct an instrumental variable, but the mortality of the twins themselves was not analysed. Using this restricted research strategy, we ran statistical models on several samples. Our first sample consisted of first-born men and women from a sibling group with two or more children. The second sample consisted of first- and second-born from a sibling group with three or more children. The third sample consisted of first-, second-, and third-born from a sibling group with four or more children. Finally, the fourth sample consisted of first- to fourth-born from sibling groups with five or more children. We ran separate models for men and women. We included a binary variable for whether there was a twin birth directly after the birth of the individuals included in the sample (e.g., a twin birth at parity two in the first-born sample, a twin birth at parity three in the sample with first-born and second-born, etc.).
Results
Results from frailty models
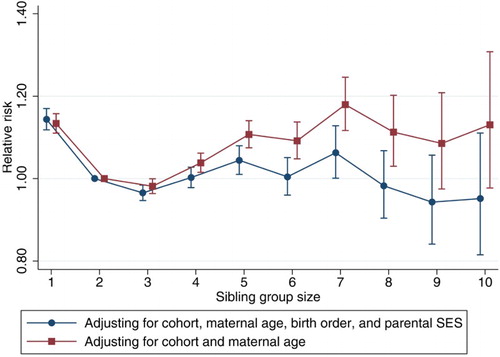
We estimated a series of frailty hazard models examining the relationship between the size of the sibling group and adult mortality for men and women, with hierarchical inclusion of control variables. shows the relative risks and confidence intervals for men. Model 1 shows the results without adjusting for birth order or parental social class. The reference category is men in sibling groups with two children (i.e., with one sibling). We find that mortality is 13 per cent higher for men from a one-child sibling group (i.e., with no siblings) than for men from a two-child sibling group. Mortality is similar for men from a three-child sibling group and men from a two-child sibling group, but among men from larger sibling groups, the relative risk increases. Men from a four-child sibling group experience a 4 per cent higher relative risk of mortality, men from a seven-child sibling group have an 18 per cent higher relative risk of mortality, and men from a ten-child sibling group have a 13 per cent higher relative risk of mortality. In all these comparisons, there is a statistically significant increase in the relative risk of mortality, with the exception of men from three-child sibling groups and men from nine- and ten-child sibling groups. Overall there is not a clear pattern of difference in mortality by sibling group size, as men in sibling size groups of between four and eight children have higher mortality, but so do ‘only children’.
Table 4 Results: sibling group size and mortality among Swedish men born 1938–72, based on Gompertz shared frailty hazard model analysis
Model 2 shows the results for the relationship between the size of the sibling group and adult mortality when adjusting for birth order in addition to the other covariates. As can be seen, the size of the coefficients decreases substantially, except for the case of men with no siblings, who now have a 17 per cent higher risk of mortality relative to men from a two-child sibling group. Men from a three-child sibling group experience a significantly lower relative risk of mortality than men from a two-child sibling group. Men from sibling groups with seven children still have an elevated risk of mortality relative to men from a two-child sibling group, but the size of the relative risk has decreased in comparison with the results from Model 1. The results for the largest sibling groups are not statistically significant. Additionally, Model 3 presents the results after controlling for social class of parents, with results very similar to those in Model 2. The results from Models 1 and 3 for men are shown in . Again, it appears that mortality is not associated with sibling group size for the most common sibling group sizes, two to four children. Furthermore, the elevated mortality of individuals from very large sibling groups largely diminishes after adjusting for birth order and parental SES. Overall, after adjusting for SES and birth order, there appears to be no association between mortality in adulthood and number of siblings. Individuals from one-child sibling groups, or ‘only children’, are the only group distinguished from children in larger sibling groups by substantially higher mortality rates. We can also conclude that birth order has a large significant impact on mortality in the models independent of sibling group size, and it is birth order that seems to be the stronger predictor of mortality.
Figure 1 The relative risk of mortality by sibling group size among men born in Sweden from 1938 to 1972
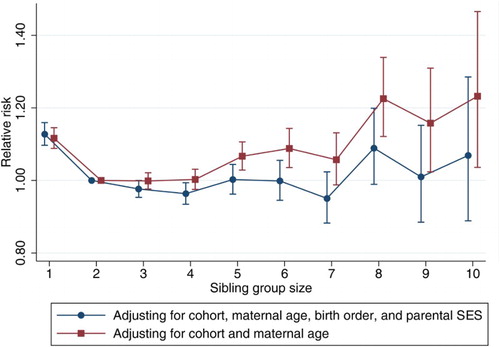
shows the results for the relationship between the size of the sibling group and mortality for women. Model 1 shows the results without adjusting for birth order or social class of the parents. Relative to women from a two-child sibling group, women from a one-child sibling group experience a 12 per cent higher risk of mortality. There is no substantive or statistically significant difference for women from three- or four-child sibling groups, but the relative risk is greater for women from sibling groups with five or more children (with the exception of a seven-child sibling group). Women from a five-child sibling group have a 7 per cent higher risk of mortality, while women from an eight-child or ten-child sibling group have a 23 per cent higher risk of mortality. Among women there is a smaller difference in terms of impact of siblings on mortality risk than for men, at least among the most common sibling group sizes found in Sweden, those with one to four children.
Table 5 Results: sibling group size and mortality among Swedish women born 1938–72, based on Gompertz shared frailty hazard model analysis
Model 2 in shows the results for the relationship between the size of the sibling group and adult mortality for women after adjusting for birth order. As with the results from Model 1, women from a one-child sibling group experience an elevated risk of mortality relative to women from a two-child sibling group. There is no statistically significant difference in the relative risk for women raised in families with three children or more. This lack of statistical significance is notable given the very high statistical power in this analysis. Again, these results support the assertion that if resource dilution is the underlying explanation for the relationship between the size of the sibling group and mortality, it would be experienced through the interaction of birth order and birth intervals, rather than the final size of the sibling group. The results from Models 1 and 3 for women are shown in . As is the case for men, it is clear that among women the size of the sibling group does not appear to affect mortality in a substantive way after accounting for birth order. Mortality rates vary little between women from the most common multi-child sibling group sizes, two to four children, and the elevated mortality of women from sibling groups with five to ten children disappears after adjusting for birth order and parental SES. It is only women with no siblings who have elevated mortality after adjusting for birth order, cohort, maternal age at the time of birth, and parental SES.
Figure 2 The relative risk of mortality by sibling group size among women born in Sweden from 1938 to 1972
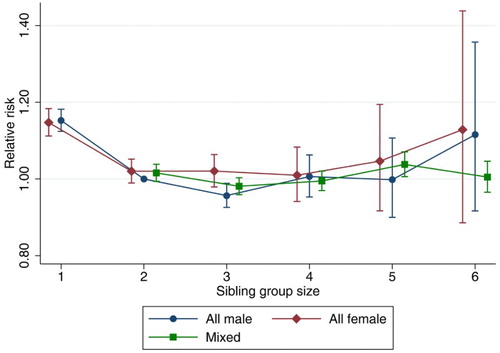
We also examined the effects of the number of siblings across specific causes of mortality. We examined mortality attributable to neoplasms (cancers), diseases of the circulatory system, external causes, and all remaining causes pooled together. These results are shown in and , for men and women, respectively (Tables A1 and A2 in the supplementary material present full results from this analysis). The results shown in and are based on survival analyses where we adjust for cohort, maternal age at the time of birth, birth order, and parental SES (Model 3). Overall, these results demonstrate a pattern that is largely similar to that seen in the all-cause mortality results. Mortality attributable to circulatory problems and external causes is somewhat higher among men who were raised as ‘only children’. Among women, mortality attributable to diseases of the circulatory system is elevated among both ‘only children’ and women raised in families with six children. We have also conducted analyses to examine whether all-cause mortality differs by the sex composition of the sibling group. These results are shown in . As can be seen, there are no clear differences in adult mortality at any sibling group size among those who were raised in an all-male, all-female, or mixed-sex sibling group.
Figure 3 The relative risk of cause-specific mortality by sibling group size among men born in Sweden from 1938 to 1972
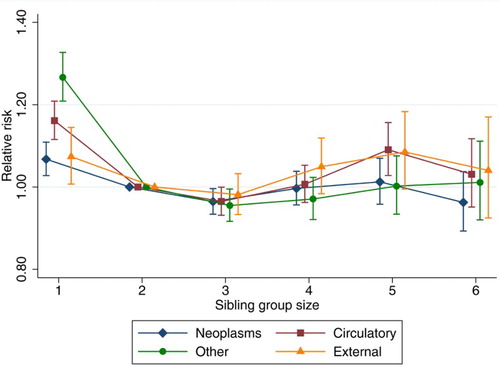
Figure 4 The relative risk of cause-specific mortality by sibling group size among women born in Sweden from 1938 to 1972
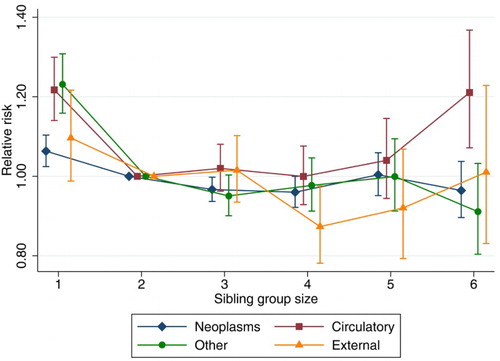
Figure 5 The relative risk of all-cause mortality by sibling group size according to the sex of siblings, for people born in Sweden from 1938 to 1972
As a sensitivity analysis, considering substantial twentieth-century changes in fertility and mortality, we experimented with separate models for different cohort groupings (see Tables A3 and A4 in the supplementary material). However, all these models consistently indicated the same conclusion about the lack of substantial effects of sibship size (except for only children). Additionally, we carried out analysis with interactions between sibship size and birth order, and the results from this analysis also confirmed our earlier findings.
Results from hazard models using twins data
While the frailty hazard models control for a wide range of characteristics of children and their parents, they cannot take into account the unobserved aspects of parental resources that differ across siblings and change across time. In order to reveal the causal effects of the number of siblings, we applied methods that take advantage of data on multiple births in order to exploit this source of exogenous variation in family size (Tables A5 and A6 in the supplementary material present the association between family size and mortality for the samples used in the twins-based analysis; that is, they present estimates of the same models as and , but using the twins-based analysis sample). and show the results for men and women from models examining whether a twin birth has an effect on mortality for the preceding children. Hence, we show how a random shock to a person’s sibling group size, through the birth of a later-born pair of twins, affects mortality.
Table 6 Results: birth of subsequent twin siblings and mortality among first-, second-, third-, and fourth-born Swedish men born 1938–72, based on Gompertz hazard model analysis
Table 7 Results: birth of subsequent twin siblings and mortality among first-, second-, third-, and fourth-born Swedish women born 1938–72, based on Gompertz hazard model analysis
Our results, presented in for men, show that a subsequent twin birth has no substantial impact on adult mortality. In fact, the relative risk is typically lower than for individuals not experiencing a subsequent twin birth, though it is not statistically significant except for siblings experiencing a twin birth at parity five. Therefore, for men we can rule out any clear effect of an exogenous sibling on mortality, though our estimates are not very precise. The results for women in show that a twin birth increases the relative risk of mortality for individuals born before the twin, but that the differences are small and not statistically significant. These results for women are more ambiguous than those for men and we are unable to make any clear conclusions about the relationship between the experience of a subsequent twin birth and adult mortality. Overall, these analyses are consistent with earlier associational models presented in and suggesting no substantive relationship between number of siblings and mortality.
As a form of sensitivity analysis, we also estimated cohort-specific instrumental variable models with a binary mortality indicator in specific age ranges. The conclusions that we reached based on those models were similar to the main results presented in this paper, with no clear relationship emerging between sibling group size and mortality.
Summary and discussion
In the study reported in this paper, we examined the relationship between the size of the sibling group and mortality risk in adulthood for Swedish men and women born between 1938 and 1972. The main finding is that growing up in a large family does not have a substantive impact on mortality in adulthood either for men or for women. This conclusion is based on survival analyses where we attempted to adjust for confounding in the relationship between the size of the sibling group and mortality by including covariates for birth order and the social class of the parents, as well as from models that exploited the occurrence of twin births to examine the impact of an exogenous increase in completed family size. The overall conclusion is also consistent for the results from models examining various causes of death. While the economic, sociological, and epidemiological literature provides a number of arguments concerning the disadvantages of growing up in a large family, it appears that these mechanisms do not mediate the relationship between the completed size of the sibling group and mortality in adulthood in contemporary Sweden once birth order and SES are controlled for. This is one of the first studies to explicitly focus on the relationship between the size of the sibling group and adult mortality in a Western developed society. The few previous studies addressing this question in developed societies examine it over a very brief and specific age range (Lundberg Citation1993).
The only incongruity to this conclusion is the fact that both men and women who were raised as ‘only children’ experience an elevated mortality risk in adulthood in comparison to men and women from multi-child sibling groups in our non-causal models. The focus of this study was to examine the main effects of the size of the sibling group of origin on adult mortality, and we therefore did not attempt to test the potential mechanisms that might link the lack of siblings and mortality. Furthermore, alternative methodological strategies to rule out confounding factors and the endogeneity of parental decisions to have only one child (such as data on miscarriages) were not available to us. It is possible that there may be some specific confounders for ‘only children’ that simultaneously affect parents’ decisions to have no more than one child (Kristensen et al. Citation2003) and affect their longevity. One example is selective mortality among parents of our individuals. Adults who die during their reproductive years tend to have fewer children. If low fecundity is related to underlying health, and that poor underlying health is heritable, then that may be an important pathway by which very small family size is associated with mortality. Further research could examine whether these findings are relevant to low fertility societies.
Our results may also be affected by the decrease in infant and child mortality over time as our data are conditioned on survival to 1960. The most profound decline in infant mortality in Sweden took place in the first two decades of the twentieth century, and by 1950 it reached the lowest level in the world (Burström Citation2003). As our data lack information on mortality before 1960, our information on siblings in earlier cohorts will be based on more select and robust adult sibling sets. As the frailest individuals are unobserved, this could mean that we underestimate the relationship between number of siblings and mortality. However, survival to age 20 was above 0.98 for the 1940 cohort and increased to over 0.99 for the 1965 cohort (Statistics Sweden Citation2010). This implies that the childhood experience of the overwhelming majority of sibling sets in our study would not be affected by such pre-adult mortality. Still, if the deaths of the siblings in earlier cohorts were tied to larger family size, this correlation between mortality and fertility could be a source of bias in our estimates. An additional shortcoming of our study is that we could not measure the specific factors that mediate the impact of siblings, such as the degree of overcrowding at any specific point during childhood, as we lack household data.
Although a number of theories have been proposed for why being raised in a larger sibling group should be related to a number of detrimental health outcomes in adulthood (Becker and Lewis Citation1973; Becker and Tomes Citation1976; Blake Citation1989; Downey Citation2001), our finding that the size of the sibling group of origin is not related to adult mortality in a substantively meaningful way is consistent with other recent research from the Nordic region. Research using twins as an exogenous impact on family size based on register data from Norway and Sweden has suggested that the size of the sibling group of origin is not substantially related to educational attainment, labour market success, or fertility (Black et al. Citation2005; Åslund and Grönqvist Citation2010; Kolk Citation2015). It has been argued that while resource access in childhood may be important, a measure for the completed size of the sibling group is an imprecise measure of resource access, in particular for earlier-born siblings. It is likely that a joint consideration of birth order and birth intervals would provide a more accurate measure of resource access within the household in early childhood than completed family size, as only the last-born child will be born into a household where the number of children corresponds to the completed fertility of the parents. A first-born, on the other hand, experiences periods of childhood as an only child, then in a two-child sibling group, and so on, up until parental fertility is completed. Furthermore, birth order effects on educational attainment and mortality have been observed in sibling groups of all sizes (Black et al. Citation2005; Barclay Citation2015; Barclay and Kolk Citation2015).
Our study focused on mortality before age 74. Life expectancy for the cohorts in our study is high (Statistics Sweden Citation2010) and the majority of our population survives until right censoring in 2012. Previous research has suggested that the effect of early life conditions is stronger at younger ages and declines over the life course (Myrskylä Citation2010). Although a growing body of literature has demonstrated the importance of early life conditions for later-life outcomes, including mortality, the findings presented in this study are consistent with the overall pattern that the trade-off between the quantity of siblings and their education is strong in countries with a liberal economic system, but very weak or non-existent in countries with welfare state arrangements that support families with children (Park Citation2008; Xu Citation2008). Indeed, our study was based on register data from Sweden, one of the highest income countries in the world, where parents with children are provided with very generous support from the welfare state. Regardless of social and ethnic background, families with children may take advantage of a publicly funded early childhood education and care system, as well as health care services that are free of charge for children. One explanation for our finding—the absence of a relationship between adult mortality and growing up in a large family—is that parents may not necessarily face a strong trade-off between having many children and providing each child with favourable conditions for good health in such a context.
Online Appendix
Download PDF (38.8 KB)Notes
1 Anna Baranowska-Rataj is at the Institute of Statistics & Demography, Warsaw School of Economics, and the Department of Sociology, Umeå University, Mediagränd 14, Beteendevetarhuset, SE 901 87 Umeå, Sweden. E-mail: [email protected]. Kieron Barclay is at the Department of Social Policy, London School of Economics & Political Science, the Max Planck Institute for Demographic Research, and the Department of Sociology, Stockholm University. Martin Kolk is at the Department of Sociology, Stockholm University.
2 This work was supported by the Vetenskapsrådet (Swedish Research Council) [grant number 340-2013-5164]; Forte (Swedish Council for Working Life and Social Research) [grant numbers 2013:1037 and 2014:1146]; and the Ministry of Science and Higher Education, Republic of Poland [grant number 896/MOB/2012/0]. Kieron Barclay was supported by an ERC Starting Grant to Mikko Myrskylä (COSTPOST: 336475).
Related Research Data
References
- Aassve, Arnstein, Stefano Mazzuco, and Letizia Mencarini. 2006. An empirical investigation into the effect of childbearing on economic wellbeing in Europe, Statistical Methods and Applications 15(2): 209–227. doi: 10.1007/s10260-006-0020-x
- Aksan, Anna-Maria. 2014. Effects of childhood mortality and morbidity on the fertility transition in sub-Saharan Africa, Population and Development Review 40(2): 311–329. doi: 10.1111/j.1728-4457.2014.00675.x
- Åslund, Olof and Hans Grönqvist. 2010. Family size and child outcomes: Is there really no trade-off? Labour Economics 17(1): 130–139. doi: 10.1016/j.labeco.2009.05.003
- Baez, Javier E. 2008. Does more mean better? Sibling sex composition and the link between family size and children’s quality, IZA Discussion Paper 3472.
- Baker, Michael, Dillip Das, Kamalesh Venugopal, and Philippa Howden-Chapman. 2008. Tuberculosis associated with household crowding in a developed country, Journal of Epidemiology and Community Health 62(8): 715–721. doi: 10.1136/jech.2007.063610
- Barclay, Kieron. 2015. Birth order and educational attainment: evidence from fully adopted sibling groups, Intelligence 48: 109–122. doi: 10.1016/j.intell.2014.10.009
- Barclay, Kieron and Martin Kolk. 2015. Birth order and mortality: a population–based cohort study, Demography 52(2): 613–639. doi: 10.1007/s13524-015-0377-2
- Becker, Gary S. and Gregg Lewis. 1973. On the interaction between the quantity and quality of children, Journal of Political Economy 81(2): S279–88. doi: 10.1086/260166
- Becker, Gary S. and Nigel Tomes. 1976. Child endowments and the quantity and quality of children, Journal of Political Economy 84(4): S143–S162. doi: 10.1086/260536
- Bengtsson, Tommy and Martin Lindström. 2000. Childhood misery and disease in later life: The effects on mortality in old age of hazards experienced in early life, southern Sweden, 1760–1894, Population Studies 54(3): 263–277. doi: 10.1080/713779096
- Bengtsson, Tommy and Göran Broström. 2009. Do conditions in early life affect old-age mortality directly and indirectly? Evidence from 19th-century rural Sweden, Social Science and Medicine 68(9): 1583–1590. doi: 10.1016/j.socscimed.2009.02.020
- Bengtsson, Tommy and Geraldine P. Mineau. 2009. Early-life effects on socio-economic performance and mortality in later life: A full life-course approach using contemporary and historical sources, Social Science and Medicine 68(9): 1561–1564. doi: 10.1016/j.socscimed.2009.02.012
- Berkman, L. F. 1984. Assessing the physical health effects of social networks and social support, Annual Review of Public Health 5(1): 413–432. doi: 10.1146/annurev.pu.05.050184.002213
- Berkman, Lisa F. and Thomas Glass. 2000. Social integration, social networks, social support, and health, in L. F. Berkman and I. Kawachi (eds.), Social Epidemiology. New York: Oxford University Press, pp. 137–173.
- Black, Sandra E, Paul J. Devereux, and Kjell G. Salvanes. 2005. The more the merrier? The effect of family size and birth order on children's education, The Quarterly Journal of Economics 120(2): 669–700.
- Black, Sandra E., Paul J. Devereux, and Kjell G. Salvanes. 2010. Small family, smart family? Family size and the IQ scores of young men, Journal of Human Resources 45(1): 33–58. doi: 10.1353/jhr.2010.0001
- Blake, Judith. 1981. Family size and the quality of children, Demography 18(4): 421–442. doi: 10.2307/2060941
- Blake, Judith. 1989. Family Size and Achievement. Studies in Demography, Volume 3. Berkeley: University of California Press.
- Burström, Bo. 2003. Social differentials in the decline of infant mortality in Sweden in the twentieth century: the impact of politics and policy, International Journal of Health Services 33(4): 723–741. doi: 10.2190/9GMR-TA8W-LA3B-5E2A
- Burström, Bo, Finn Diderichsen, and Lars Smedman. 1999. Child mortality in Stockholm during 1885–1910: the impact of household size and number of children in the family on the risk of death from measles, American Journal of Epidemiology 149(12): 1134–1141. doi: 10.1093/oxfordjournals.aje.a009768
- Case, Anne and Christina Paxson. 2010. Causes and consequences of early-life health, Demography 47(1): S65–S85. doi: 10.1353/dem.2010.0007
- Chernozhukov, Victor and Christian Hansen. 2008. The reduced form: A simple approach to inference with weak instruments, Economics Letters 100(1): 68–71. doi: 10.1016/j.econlet.2007.11.012
- Cleland, John. 2001. The effects of improved survival on fertility: A reassessment, Population and Development Review 27: 60–92.
- Cohen, Sheldon. 2004. Social relationships and health, American Psychologist 59(8): 676–684. doi: 10.1037/0003-066X.59.8.676
- Conley, Dalton. 2000. Sibship sex composition: Effects on educational attainment. Social Science Research 29(3): 441–457. doi: 10.1006/ssre.2000.0678
- Currie, Janet and Brigitte C. Madrian. 1999. Health, health insurance and the labor market, Handbook of Labor Economics 3: 3309–3416. doi: 10.1016/S1573-4463(99)30041-9
- Doblhammer, Gabriele. 2000. Reproductive history and mortality later in life: a comparative study of England and Wales and Austria, Population Studies 54(2): 169–176. doi: 10.1080/713779087
- Donrovich, Robyn Nicole, Paul Puschmann, and Koenraad Matthijs. 2014. Rivalry, solidarity, and longevity among siblings: A life course approach to the impact of sibship composition and birth order on later life mortality risk, Antwerp (1846–1920), Demographic Research 31: 1167–1198. doi: 10.4054/DemRes.2014.31.38
- Downey, Douglas B. 2001. Number of siblings and intellectual development: The resource dilution explanation, American Psychologist 56(6–7): 497–504. doi: 10.1037/0003-066X.56.6-7.497
- Downey, Douglas B., Dennis J. Condron, and Deniz Yucel. 2015. Number of siblings and social skills revisited among american fifth graders, Journal of Family Issues 36(2): 273–296. doi: 10.1177/0192513X13507569
- Edvinsson, Sören, Anders Brändström, John Rogers, and Göran Broström. 2005. High-risk families: The unequal distribution of infant mortality in nineteenth-century Sweden, Population Studies 59(3): 321–337. doi: 10.1080/00324720500223344
- Eng, Patricia M., Eric B. Rimm, Garrett Fitzmaurice, and Ichiro Kawachi. 2002. Social ties and change in social ties in relation to subsequent total and cause-specific mortality and coronary heart disease incidence in men, American Journal of Epidemiology 155(8): 700–709. doi: 10.1093/aje/155.8.700
- Engelman, Michal, Emily M. Agree, Kathryn M. Yount, and David Bishai. 2010. Parity and parents’ health in later life: The gendered case of Ismailia, Egypt, Population Studies 64(2): 165–178. doi: 10.1080/00324721003660511
- Erikson, Robert, John H. Goldthorpe, and Lucienne Portocarero. 1979. Intergenerational class mobility in three Western European societies: England, France and Sweden, The British Journal of Sociology 30(4): 415–441. doi: 10.2307/589632
- Eriksson, Johan G., Tom Forsen, Jaakko Tuomilehto, Paul D. Winter, Clive Osmond, and David J. P. Barker. 1999. Catch-up growth in childhood and death from coronary heart disease: longitudinal study, British Medical Journal 318(7181): 427–431. doi: 10.1136/bmj.318.7181.427
- Evans, Gary W. 2006. Child development and the physical environment, Annual Review of Psychology 57: 423–451. doi: 10.1146/annurev.psych.57.102904.190057
- Gagnon, Alain and Ryan Mazan. 2009. Does exposure to infectious diseases in infancy affect old-age mortality? Evidence from a pre-industrial population, Social Science and Medicine 68(9): 1609–1616. doi: 10.1016/j.socscimed.2009.02.008
- Gagnon, Alain and Nora Bohnert. 2012. Early life socioeconomic conditions in rural areas and old-age mortality in twentieth-century Quebec, Social Science and Medicine 75(8): 1497–1504. doi: 10.1016/j.socscimed.2012.06.007
- Galobardes, Bruna, John W. Lynch, and Davey Smith. 2004. Childhood socioeconomic circumstances and cause-specific mortality in adulthood: systematic review and interpretation, Epidemiologic Reviews 26(1): 7–21. doi: 10.1093/epirev/mxh008
- Garg, Ashish and Jonathan Morduch. 1998. Sibling rivalry and the gender gap: Evidence from child health outcomes in Ghana, Journal of Population Economics 11(4): 471–493. doi: 10.1007/s001480050080
- Glick, Peter J., Alessandra Marini, and David E. Sahn. 2007. Estimating the consequences of unintended fertility for child health and education in Romania: An analysis using twins data, Oxford Bulletin of Economics and Statistics 69(5): 667–691. doi: 10.1111/j.1468-0084.2007.00476.x
- Gluckman, Peter D., Mark A. Hanson, Cyrus Cooper, and Kent L. Thornburg. 2008. Effect of in utero and early-life conditions on adult health and disease, New England Journal of Medicine 359(1): 61–73. doi: 10.1056/NEJMra0708473
- Grundy, Emily and Øystein Kravdal. 2007. Reproductive history and mortality in late middle age among Norwegian men and women, American Journal of Epidemiology 167(3): 271–279. doi: 10.1093/aje/kwm295
- Hank, Karsten. 2010. Childbearing history, later-life health, and mortality in Germany, Population Studies 64(3): 275–291. doi: 10.1080/00324728.2010.506243
- Hart, Carole and Davey Smith. 2003. Relation between number of siblings and adult mortality and stroke risk: 25 year follow up of men in the Collaborative study, Journal of Epidemiology and Community Health 57(5): 385–391. doi: 10.1136/jech.57.5.385
- Hatton, Timothy J. and Richard M. Martin. 2010. The effects on stature of poverty, family size, and birth order: British children in the 1930s, Oxford Economic Papers 62(1): 157–184. doi: 10.1093/oep/gpp034
- Hemminki, Xinjun Li, Kamila Plna, Charlotta Granström, Kari Pauli Vaittinen. 2001. The nation-wide Swedish family-cancer database—updated structure and familial rates, Acta Oncologica 40(6): 772–777. doi: 10.1080/02841860152619214
- Henderson, Daniel J., Daniel L. Millimet, Christopher F. Parmeter and Le Wang. 2008. Fertility and the health of children: A nonparametric investigation, Advances in Econometrics 21: 167–195. doi: 10.1016/S0731-9053(07)00007-2
- Hertwig, Ralph, Jennifer Nerissa Davis, and Frank J. Sulloway. 2002. Parental investment: How an equity motive can produce inequality, Psychological Bulletin 128(5): 728–745. doi: 10.1037/0033-2909.128.5.728
- Hoem, B. and J. M. Hoem. 1996. Sweden's family policies and roller-coaster fertility. Journal of Population Problems 52(3–4): 1–22.
- Holmlund, Helena, Helmut Rainer, and Thomas Siedler. 2013. Meet the parents? Family size and the geographic proximity between adult children and older mothers in Sweden, Demography 50(3): 903–931. doi: 10.1007/s13524-012-0181-1
- Huang, Cheng and Irma T. Elo. 2009. Mortality of the oldest old Chinese: The role of early-life nutritional status, socio-economic conditions, and sibling sex-composition, Population Studies 63(1): 7–20. doi: 10.1080/00324720802626921
- Jacobsen, Joyce P., James Wishart Pearce III, and Joshua L. Rosenbloom. 1999. The effects of childbearing on married women's labor supply and earnings: using twin births as a natural experiment, Journal of Human Resources 34(3): 449–474. doi: 10.2307/146376
- Jaine, Richard, Michael Baker, and Kamalesh Venugopal. 2011. Acute rheumatic fever associated with household crowding in a developed country, The Pediatric Infectious Disease Journal 30(4): 315–319. doi: 10.1097/INF.0b013e3181fbd85b
- Kaplan, Hillard. 1996. A theory of fertility and parental investment in traditional and modern human societies, American Journal of Physical Anthropology 101(s23): 91–135. doi: 10.1002/(SICI)1096-8644(1996)23+<91::AID-AJPA4>3.0.CO;2-C
- Knipscheer, K. and T. Van Tilburg. 2013. Generational contact and support among late adult siblings within a verticalized family, in M. Silverstein and R. Giarrusso (eds.), Kinship and Cohort in an Aging Society: From Generation to Generation. Baltimore: The John Hopkins University Press, pp. 59–76.
- Kolk, Martin. 2014. Multigenerational transmission of family size in contemporary Sweden, Population Studies 68(1): 111–129. doi: 10.1080/00324728.2013.819112
- Kolk, Martin. 2015. The causal effect of an additional sibling on completed fertility: An estimation of intergenerational fertility correlations by looking at siblings of twins, Demographic Research 32: 1409–1420. doi: 10.4054/DemRes.2015.32.51
- Kristensen, Petter, Lorentz M. Irgens, and Tor Bjerkedal. 2003. Impact of low birthweight on subsequent fertility: population-based register study. Paediatric and Perinatal Epidemiology 17(1): 10–16. doi: 10.1046/j.1365-3016.2003.00467.x
- Lundberg, Olle. 1993. The impact of childhood living conditions on illness and mortality in adulthood, Social Science and Medicine 36(8): 1047–1052. doi: 10.1016/0277-9536(93)90122-K
- Mercy, James A. and Lala Carr Steelman. 1982. Familial influence on the intellectual attainment of children, American Sociological Review 47(4): 532–542. doi: 10.2307/2095197
- Millimet, Daniel L. and Le Wang. 2011. Is the quantity-quality trade-off a trade-off for all, none, or some? Economic Development and Cultural Change 60(1): 155–195. doi: 10.1086/661216
- Moffitt, Robert. 2005. Remarks on the analysis of causal relationships in population research, Demography 42(1): 91–108. doi: 10.1353/dem.2005.0006
- Morduch, Jonathan. 2000. Sibling rivalry in Africa, The American Economic Review 90(2): 405–409. doi: 10.1257/aer.90.2.405
- Mucci, Lorelei A., Chung-Cheng Hsieh, Paige L. Williams, Paul W. Dickman, Lars Björkman, and Nancy L. Pedersen. 2004. Birth order, sibship size, and housing density in relation to tooth loss and periodontal disease: a cohort study among Swedish twins, American Journal of Epidemiology 159(5): 499–506. doi: 10.1093/aje/kwh063
- Myrdal, Alva and Gunnar Myrdal. 1934. Kris i befolkningsfrågan [Crisis in the Population Question]. Stockholm: Bonnier.
- Myrskylä, Mikko. 2010. The relative effects of shocks in early-and later-life conditions on mortality, Population and Development Review 36(4): 803–829. doi: 10.1111/j.1728-4457.2010.00358.x
- Parish, William L. and Robert J. Willis. 1993. Daughters, education, and family budgets Taiwan experiences, Journal of Human Resources 28(4): 863–898. doi: 10.2307/146296
- Park, Hyunjoon. 2008. Public policy and the effect of sibship size on educational achievement: A comparative study of 20 countries, Social Science Research 37(3): 874–887. doi: 10.1016/j.ssresearch.2008.03.002
- Perrenoud, A. 1984. The mortality decline in long-term perspective, in Tommy Bengtsson, Gunnar Fridlizius, and Rolf Ohlsson (eds.), Pre-industrial Population Change: The Mortality Decline and Short-Term Population Movements. Stockholm: Almquist and Wiksell International, pp. 41–69.
- Powell, Brian and Lala Carr Steelman. 1989. The liability of having brothers: Paying for college and the sex composition of the family, Sociology of Education 62(2): 134–147. doi: 10.2307/2112845
- Powell, Brian and Lala Carr Steelman. 1990. Beyond sibship size: Sibling density, sex composition, and educational outcomes, Social Forces 69(1): 181–206. doi: 10.2307/2579613
- Preston, Samuel H. 1978. The Effects of Infant and Child Mortality on Fertility. New York: Academic Press.
- Rodgers, J. L. 2001. What causes birth order–intelligence patterns? The admixture hypothesis, revived. American Psychologist 56(6–7): 505–510. doi: 10.1037/0003-066X.56.6-7.505
- Rosenzweig, Mark R. and Kenneth I. Wolpin. 1980. Testing the quantity-quality fertility model: The use of twins as a natural experiment, Econometrica: Journal of the Econometric Society 48(1): 227–240. doi: 10.2307/1912026
- Rosenzweig, Mark R. and Junsen Zhang. 2009. Do population control policies induce more human capital investment? Twins, birth weight and China's one-child policy, The Review of Economic Studies 76(3): 1149–1174. doi: 10.1111/j.1467-937X.2009.00563.x
- Rostila, Mikael, Jan Saarela, and Ichiro Kawachi. 2012. The forgotten griever: a nationwide follow-up study of mortality subsequent to the death of a sibling, American Journal of Epidemiology 176(4): 338–346. doi: 10.1093/aje/kws163
- Schultz, T. Paul. 2007. Population policies, fertility, women's human capital, and child quality, Handbook of Development Economics 4: 3249–3303. doi: 10.1016/S1573-4471(07)04052-1
- Scrimshaw, Susan C. M. 1978. Infant mortality and behavior in the regulation of family size, Population and Development Review 4(3):383–403. doi: 10.2307/1972856
- Seeman, Teresa E. 2000. Health promoting effects of friends and family on health outcomes in older adults, American Journal of Health Promotion 14(6): 362–370. doi: 10.4278/0890-1171-14.6.362
- Smith, Ken R., Geraldine P. Mineau, Gilda Garibotti, and Richard Kerber. 2009. Effects of childhood and middle-adulthood family conditions on later-life mortality: evidence from the Utah Population Database, 1850–2002, Social Science and Medicine 68(9): 1649–1658. doi: 10.1016/j.socscimed.2009.02.010
- Solari, Claudia D. and Robert D. Mare. 2012. Housing crowding effects on children’s wellbeing, Social Science Research 41(2): 464–476. doi: 10.1016/j.ssresearch.2011.09.012
- StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: Stata Corporation.
- Statistics Sweden. 2010. Cohort Mortality in Sweden - Mortality Statistics Since 1861. Stockholm: Statistics Sweden (SCB).
- Steelman, Lala Carr, Brian Powell, Regina Werum, and Scott Carter. 2002. Reconsidering the effects of sibling configuration: Recent advances and challenges, Annual Review of Sociology 28: 243–269. doi: 10.1146/annurev.soc.28.111301.093304
- Sundin, Jan and Sam Willner. 2007. Social Change and Health in Sweden: 250 Years of Politics and Practice. Stockholm: Swedish National Institute of Public Health.
- Taylor, Carl E., Jeanne S. Newman, and Narindar U. Kelly. 1976. The child survival hypothesis, Population Studies 30(2): 263–278. doi: 10.1080/00324728.1976.10412734
- Van den Berg, Gerard J., Gabriele Doblhammer, and Kaare Christensen. 2009. Exogenous determinants of early-life conditions, and mortality later in life, Social Science and Medicine 68(9): 1591–1598. doi: 10.1016/j.socscimed.2009.02.007
- Vaupel, James and Trifon I. Missov. 2014. Unobserved population heterogeneity: A review of formal relationships, Demographic Research 31: 659–686. doi: 10.4054/DemRes.2014.31.22
- Weitoft, Gunilla Ringbäck, Anders Hjern, Bengt Haglund, and Måns Rosén. 2003. Mortality, severe morbidity, and injury in children living with single parents in Sweden: a population-based study, The Lancet 361(9354): 289–295. doi: 10.1016/S0140-6736(03)12324-0
- Whiteman, Shawn D., Susan M. McHale, and Anna Soli. 2011. Theoretical perspectives on sibling relationships, Journal of Family Theory and Review 3(2): 124–139. doi: 10.1111/j.1756-2589.2011.00087.x
- Xu, Jun. 2008. Sibship size and educational achievement: The role of welfare regimes cross-nationally, Comparative Education Review 52(3): 413–436.
- Yamada, Tadashi. 1984. Causal relationships between infant mortality and fertility in developed and less developed countries, NBER Working Paper (1528).
- Yeung, W. Jean, Miriam R. Linver, and Jeanne Brooks–Gunn. 2002. How money matters for young children's development: Parental investment and family processes, Child Development 73(6): 1861–1879. doi: 10.1111/1467-8624.t01-1-00511