
Abstract
We examine pathways between indicators of fertility tempo/quantum and depressive symptoms among parents aged 55+ with at least two children, using three waves of the English Longitudinal Study of Ageing. Using standard regression approaches and path analysis within the structural equation framework, we also investigate whether fertility trajectories mediated the association between childhood disadvantage and later-life depression. Results provide limited support for direct influences of fertility trajectories on depression, but indicate indirect linkages for both women and men. Associations are mediated by partnership history, social support, wealth, later-life smoking, and functional limitation. Associations between childhood disadvantage and later-life depression are partially mediated by fertility stressors. Results confirm the influence of life course experiences on depression at older ages and demonstrate the interlinked role of family and other life course pathways on later-life well-being.
Introduction
Depression and depressive symptoms in mid- and later life are a major cause of poor health and contribute substantially to the overall burden of disease (Wittchen et al. Citation2011). In this paper, nationally representative longitudinal data from England are analysed to investigate linkages between the fertility trajectories of women and men with two or more children and the risk of later-life depression. Some trajectories may be directly related to later-life depression due to long-term effects of accumulated stress and also indirectly related via impacts of fertility pathways on subsequent life experiences that are themselves linked to depression. The paper also investigates whether fertility trajectories mediate associations between childhood disadvantage and depression at older ages.
Theoretical background
Identified current and life course socio-demographic factors associated with depressive symptoms in mid- and later adulthood include childhood circumstances, level of education, adult socio-economic resources, partnership status, social support, and physical health (Fiske et al. Citation2009; Virtanen et al. Citation2015). Fertility trajectories intersect with all these factors, and theoretical frameworks from several disciplinary traditions suggest that the tempo and quantum of fertility may be directly or indirectly related to later-life depression. These frameworks—from social psychiatry, life course epidemiology and sociology, and life history theory—all posit that biological and social factors throughout life influence later health outcomes cumulatively and interactively, and that the effects of stress are one mechanism underlying this association (Ben-Shlomo and Kuh Citation2002).
From a social psychiatry perspective, seminal research by Brown and collaborators highlighted the role of exposure to recent adverse events and chronic stressors—including having three or more children to look after—in increasing the risks of depression among women, particularly in the face of vulnerabilities arising from early loss of a parent and absence of a supportive relationship (Brown and Harris Citation1990). Consistent with this, a more recent systematic review of studies of life events, stress, and depression concluded that stressors were important influences on depression, with some moderating effect of social relationships (Tennant Citation2002). Although most studies reviewed indicated that the effect of acute stressors dissipated over time, there was evidence that prior depressive episodes sensitized individuals to subsequent stress-induced disorder, meaning that earlier stresses may have long-lasting effects. Other subsequent studies have also demonstrated the enduring effects of earlier stress burden on women's risk of depression in later life (Kasen et al. Citation2010) and the importance of relationships with partners and children (Stafford et al. Citation2011).
Life course theories in epidemiology and sociology have similarly emphasized the cumulative influence of prior circumstances, particularly those at key developmental stages, on later-life health (Ben-Shlomo and Kuh Citation2002). Adversity in childhood, for example, is associated with adult mental health disorders (Comijs et al. Citation2007; Weich et al. Citation2009; Ford et al. Citation2011; Gershon et al. Citation2013). There is, however, disagreement as to whether direct effects persist at older ages (Wainwright and Surtees Citation2002; Gershon et al. Citation2013) or whether the association arises because childhood adversity sets in train ‘chains of risk’, including poorer quality social relationships and partnerships in adulthood (Brown et al. Citation2008; Ford et al. Citation2011), which in turn increase risks of mental health problems. Childhood socio-economic position (SEP), as distinct from specific adversities, is also associated with later-life depression. Again, some studies suggest lasting direct effects (Luo and Waite Citation2005; Schaan Citation2014) whereas others indicate that associations are mediated by educational attainment, adult SEP, and adult social resources (Nicholson et al. Citation2008; Kamiya et al. Citation2013; Kendig et al. Citation2015).
Less attention has been paid to the possible role of early parenthood as a mediator of associations between childhood circumstances and later-life depression. However, childhood adversity and low childhood SEP are associated with poorer mental health in adolescence, risky behaviours including smoking and sexual risk-taking, and early parenthood (Sigle-Rushton Citation2005; Henretta Citation2007; Hobcraft Citation2008; Pudrovska and Carr Citation2009; Hale and Viner Citation2016). Associations between early parenthood and later-life depression may thus mediate—or be confounded by—links between childhood circumstances and later depression. This pathway is emphasized in the life history theories developed by evolutionary biologists, which propose that unstable and unpredictable environments favour evolution of ‘r-selected’ traits associated with high reproduction rates but low parental investment. In contrast, ‘K-selected’ traits involve low reproduction but high parental investment (Mace Citation2000). Humans lie at the K end of the continuum but there is within-species variation in reproductive strategy, and epigenetic and hormonal influences prompted by unstable environments in childhood may lead to earlier sexual maturation and poorer choice of partners (Belsky et al. Citation1991; Ellis Citation2004; Waynforth Citation2012). Consistent with this theory, a range of studies have found associations between lack of parental care and: (a) earlier sexual maturation, sexual debut, and reproduction; and (b) greater risk of own partnership breakdown (Quinlan Citation2003; Nettle et al. Citation2011). Some studies have also suggested a negative association between high-K strategies and depression (Giosan Citation2013).
Fertility trajectories and stress
Parenthood has potential benefits for mental health, including provision of a sense of purpose, performance of a valued social role, and enhanced social interaction and social support during childrearing and later phases of life (Offer and Schneider Citation2007). However, parenthood also presents challenges, particularly for those following parenting trajectories likely to involve exposure to additional stress, such as early parenthood, closely spaced births, and large family size. Very young parents may be less resilient to the physical, emotional, and economic stresses involved in raising children, have fewer stress-buffering resources, and, in some social contexts, experience stigma (Falci et al. Citation2010; Barban Citation2013). Closely spaced or multiple births are physically challenging, with higher risks of complications for both mother and babies (Conde-Agudelo et al. Citation2012). Parents of closely spaced children may experience stresses similar to those reported for parents of multiples, albeit to a lesser extent; these include physical stress, sleep deprivation, and greater risks of post-partum depression, economic strain, and social isolation (Campbell et al. Citation2004). Thorpe et al. (Citation1991), for example, found in a British nationally representative sample that mothers of twins and mothers of closely spaced singletons were both more likely than other mothers to experience depressive symptoms when the index child was aged five. High parity (which is associated with both early parenthood and short birth intervals) brings the stress of coping with the demands of several children at once and often financial strain (Townsend Citation1979).
In addition to involving exposures to stresses that themselves have possible cumulative effects on later-life mental health, certain fertility patterns may increase the risks of experiencing subsequent socio-economic and socio-demographic disadvantages linked to depression. Early parenthood may disrupt educational and career progression, and is associated with increased chances of divorce (Hofferth et al. Citation2001; Ermisch and Pevalin Citation2005), as are multiple births (Jena et al. Citation2011). Large family size constrains opportunities for undertaking other roles, including labour market involvement among mothers, and is negatively associated with wealth accumulation (Grundy and Read Citation2015).
Previous research
Most research on associations between fertility patterns and later-life mental health has focused on early motherhood, although some studies have also considered men. Results of these studies have been mixed (for a review, see Umberson et al. Citation2010). Mirowsky and Ross’s (Citation2002) analysis of a United States (US) data set suggested that for parous women, the age at first birth associated with the lowest later risk of depression was 30; for men there was a monotonic decrease in risk associated with older age at first birth. Similarly, a study based on Norwegian register data found that older age at first birth was associated with lower use of antidepressant medication in late midlife (Kravdal et al. Citation2015) and a recent analysis of Australian panel data reported an association between teenage motherhood and poor mental health among women aged 40+, after adjustment for socio-economic circumstances in early and later life (Aitken et al. Citation2016). However, Henretta et al. (Citation2008), in a comparative study of the US and Britain, found that, after controlling for early and midlife socio-economic status and midlife health, motherhood before age 21 was associated with poorer midlife mental health in the British but not the US sample. Some other analyses of US data have also found no associations or suggested that associations between early parenthood and later-life mental health reflect the influence of other measured or unmeasured confounders or mediators, such as mental health before the first birth, marital status at time of the birth, or later socio-economic or health status (Kalil and Kunz Citation2002; Koropeckyj-Cox et al. Citation2007; Spence Citation2008; Mollborn and Morningstar Citation2009; Taylor Citation2009; Patel and Sen Citation2012).
Research on associations between other aspects of fertility trajectories and later-life depressive symptoms is limited. Although mental health consequences of childlessness have been investigated (see Umberson et al. Citation2010), fewer studies have examined effects of large family size, and results are inconsistent. They report adverse effects of high parity (variously measured as three, four, or five or more children) on mothers but not fathers (Kruk and Reinhold Citation2014), on fathers but not mothers (Buber and Engelhardt Citation2008; Pudrovska Citation2008), on both (Kim et al. Citation2015), or neither (Hank Citation2010). Associations between birth intervals and mental health in mid- and later life have not, to our knowledge, been previously investigated.
A more extensive literature has reported associations between fertility stressors and later-life physical health or mortality. Adverse effects of early age at entry to parenthood, high parity, or both have been reported in studies from a range of populations, for both women and, in fewer studies, men (for reviews, see Aiken et al. Citation2012; Zeng et al. Citation2016). These include studies that have used sibling comparison models or similar approaches to try to control for selection effects (Barclay et al. Citation2016). A few studies have considered longer-term implications of birth spacing. One of these reported an association between experience of a short birth interval (<18 months) and both poorer physical functioning and accelerated functional decline in a sample of older people in the UK (Read et al. Citation2011). A later study, based on Norwegian register data, found that mothers of twins and mothers and fathers of closely spaced singleton births experienced higher mortality and made greater use of prescription medication in late midlife than parents with birth intervals of 31–41 months (Grundy and Kravdal Citation2014).
The inconsistent results from earlier studies of fertility trajectories and later-life depression may partly reflect variations in contextual influences, such as support for parents, cultural norms, and variations in access to modern methods of contraception and legal abortion in the populations studied (Grundy and Foverskov Citation2016). Differences in methods and measures and the extent of control for antecedent and later circumstances are also important. Many previous studies have controlled for factors that may lie on the causal path from fertility trajectories (early parenthood, for example) to depression, rather than examining the possible role of such factors as mediators. As such, they may ‘overcontrol’ and therefore miss potentially informative associations (see Rosendaal and Pirkle (Citation2017) for a discussion of this issue).
Research questions
In this paper a life course approach is used to examine associations between fertility trajectories and depressive symptoms in later life, with a focus on investigating mediating pathways. Based on the previous theoretical and empirical literature, we expected early parenthood, experience of a short birth interval, and high parity to be associated with later-life depression, because of lasting effects of accumulated stress and because these interrelated fertility experiences increase risks of experiencing other stressors and disadvantages, including divorce, lower labour market participation (for women), lower wealth, and worse physical health. A possible offsetting factor might be higher levels of social support for parents of large families (Grundy and Read Citation2012). Additionally, we expected poorer childhood circumstances to be related to a higher chance of early parenthood (and so to high parity) and that early parenthood would contribute to (mediate) the association between childhood circumstances and later-life depression. We expected all these associations to be stronger for women than for men because of stresses associated with pregnancy and childbirth exclusive to women, women's greater role in childrearing, and the increased domestic work associated with having children (Nomaguchi and Milkie Citation2003), as well as identified stresses associated with consequent ‘multitasking’ among mothers (Offer and Schneider Citation2011). The study is based on analysis of data from three rounds of the English Longitudinal Study of Ageing (ELSA) (Clemens et al. Citation2019), one of which collected retrospective information on childhood and adult life before enrolment in the study.
Data and methods
Data
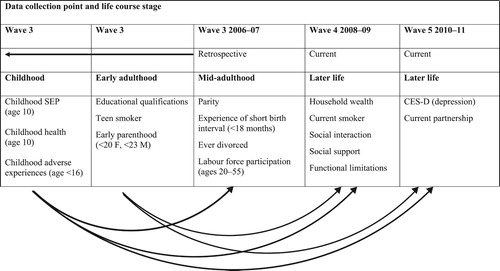
Data were drawn from Waves 3–5 of ELSA, a nationally representative study of the older population in England (Steptoe et al. Citation2013). Wave 3 was fielded in 2006–07 and the later waves at subsequent two-yearly intervals. All ELSA participants gave written informed consent to participate in the study at the recruitment wave and have reaffirmed consent at each subsequent wave. Ethical consent for the study was granted by research ethics committees of the National Health Service and University College London. The analytic sample for this study comprised ‘core’ members of the study who had had at least two children, had participated in Wave 3, and were at least 55 years old at that time (N = 5,006). (Core members of ELSA are men and women who participated in any of the 1998, 1999, or 2001 waves of the Health Survey of England (HSE), and were at least 50 years old at the time the first wave of ELSA was collected in 2002–03.) Our sample represents 54 per cent of the original core sample who had at least two children and were in our selected age group (N = 9,290) in Wave 1. The outcome, more than three depressive symptoms, was measured at Wave 5, as was current partnership status. The life history data collected in Wave 3 provided relevant measures of fertility history, childhood circumstances, teen smoking, educational attainment, experience of divorce, and labour force participation between the ages of 20 and 55. Measures of household wealth, social support, social isolation, and physical health were drawn from Wave 4, in order to reduce the probability of reverse causation (as, e.g., poor mental health may lead people to withdraw from social activities). Two indicators of smoking history were included: (a) ‘teen smoker’, included because of known associations between teenage smoking, other risky behaviours—including sexual risk-taking—and adolescent mental health (Hale and Viner Citation2016; Wilkinson et al. Citation2016; Guleria et al. Citation2017); and (b) ‘current smoker’ in later life, included because of known associations between smoking and mental health at older ages (Shahab et al. Citation2015).
presents an overview of the structure of the ELSA data used and the expected conceptual linkages underlying the analysis.
Figure 1 Overview of ELSA data structure and conceptual linkages
Measures
Outcome variable
Depressive symptoms were measured using an eight-item version of the original 20-item Center for Epidemiologic Studies Depression Scale (CES-D) (Radloff Citation1977; Eaton et al. Citation2004). The scale includes questions asking whether respondents felt depressed, sad, or lonely much of the time during the past week, had problems sleeping, or felt that everything they did required an effort. Respondents were classified as ‘having depressive symptoms’ if they reported having suffered at least three of the symptoms associated with depression, referred to here as ‘3+ CES-D’ (White et al. Citation2016). The use of this cut-off to indicate ‘caseness’ has been validated in clinical interviews based on the Diagnostic and Statistical Manual of Mental Disorders (Turvey et al. Citation1999).
Fertility history measures
Potential stressors related to fertility history comprise: an indicator of early age at entry to parenthood, defined as first birth at age <20 for women and <23 for men; experience of one or more short birth intervals (given birth to or fathered twins or two natural children born less than 18 months apart); and large family size (four or more children). These cut-off points were based on thresholds used in the previous literature and the sample distribution (Grundy and Tomassini Citation2005; Hobcraft Citation2008).
Intermediate and control variables: Childhood and early adulthood
Three indicators of retrospectively reported circumstances in childhood were used. A latent variable was derived to capture SEP (at age ten), based on parental occupational social class, housing tenure, access to household amenities, number of books in the household, and number of persons per room (see Ploubidis et al. Citation2014). Health in childhood was classified as poor if respondents reported that they had missed school, been confined to bed or in hospital for at least a month, or experienced health problems that restricted their physical activities for at least three months. Respondents were classified as having experienced adverse events in childhood if they reported one or more of the following before age 16: parents unemployed for at least six months when they wanted to work; parents argued often; parents took drugs, had mental health problems, or drank a lot of alcohol; or parents physically abused the respondent.
Highest level of educational attainment was trichotomized, distinguishing those with no formal qualifications, those with intermediate-level qualifications (generally taken in secondary school), and those with tertiary education. Additionally, we included a binary variable indicating whether or not respondents reported starting smoking before age 20.
Intermediate and control variables: Mid- and later adulthood
Wave 3 data were used to derive an indicator of respondents’ labour market participation between age 20 (or the end of full-time education, whichever was later) and age 55. A sum score was created with values of ‘0’ for each year of unemployment or non-employment, ‘0.5’ for each year of part-time employment, and ‘1’ for each year of full-time employment. This score was used to derive a variable ranging from ‘0’ to ‘10’ with every one-unit increase representing a ten percentage point increase in the proportion of time spent in full-time employment. For men the distribution of this score was highly negatively skewed; the variable used in the main analysis was therefore dichotomized (‘0’ if spent less than 50 per cent of time period in full-time employment, ‘1’ otherwise). A further dichotomous variable was created to identify respondents who had ever experienced divorce by Wave 3.
Other potential intermediate variables related to lifestyle, social support, wealth, and physical health were extracted from the Wave 4 interview. Current smoking was measured using a binary indicator (yes/no). Social support was measured using the mean value of the level of support respondents reported receiving from their partner, children, other family, and friends. Respondents rated, using a scale from ‘1’ (not at all) to ‘4’ (a lot), how much: (a) others understand the way they feel about things; (b) how much they rely on others if they have a serious problem; and (c) how much they open up to others if they need to talk about worries. Social support was coded as ‘0’ for those who reported ‘not applicable’. As the distribution of this variable was highly skewed, it was recoded as an ordinal variable ranging from ‘0’ to ‘4’, where higher values indicate more support. Additionally, a binary indicator of restricted social interaction was derived to measure social isolation, identifying those who, on average, had less than monthly face-to-face, telephone, or written contact with any child, other family member, or friend. Household wealth was based on the net value of primary and secondary property, plus business and non-housing financial wealth, divided into quintiles, and treated as an ordinal variable. Physical health was measured using the Nagi scale of mobility and functional limitation (Nagi Citation1976). Respondents were categorized as having functional limitations if they reported difficulties with one or more of the following activities: walking 100 yards (91 metres); sitting for two hours; getting up from a chair; climbing one or more flights of stairs; stooping, kneeling, or crouching; reaching or extending arms above shoulder level; pushing or pulling large objects; lifting or carrying weights over 10 pounds (4.5 kilograms); or picking up a small coin from a table. Information regarding current partnership (no partner vs. married or cohabiting) was drawn from the Wave 5 interview.
Analytic strategy
The data were analysed using standard regression methods and path analysis within the structural equation framework (Muthén and Muthén Citation2012). Age was available for all participants and was included as a continuous independent variable. Loss to follow-up is a usual problem in longitudinal studies and not all Wave 3 participants responded in Wave 5. Complete case analysis is a common way of dealing with missing data and the regression analyses reported in this paper were based on a complete case sample. However, complete case analysis can lead to bias as it rests on the assumption that missingness is completely at random and unrelated to observed or unobserved variables, whereas it is known that study dropout is often associated with various disadvantages (Chatfield et al. Citation2005). Preliminary analysis showed that in our sample loss to follow-up was associated with lower education, lower social support and higher social isolation, older age, functional limitation, and, among those aged 65+, lower wealth. In the main path analysis, we therefore used the full information maximum likelihood (FIML) method to address this problem (Acock Citation2005). This enabled inclusion of cases with missing values for any dependent variable in the path models. FIML produces estimates for means and the variance–covariance matrix, and uses these to obtain model parameters; results are generally very similar to those obtained using multiple imputation (Enders and Bandalos Citation2001; Acock Citation2005). The FIML approach is particularly suitable for complex analyses in the structural equation framework because it fits the expected model and takes into account missingness in a single run. Maximum likelihood estimation in Mplus is available for a range of different types of variable, including continuous, binary, ordinal, and count. The assumption is that if all the variables that are responsible for the missing-data-generating mechanism are included in the model, then this can be ignored and parameter estimates robustly computed for participants with missing data.
Following descriptive analysis, logistic regression was used to test associations between the fertility stressors and depression, with and without control for other variables. Although some criticisms have been raised about the comparison of logit samples across samples, because of variation in unobserved heterogeneity (Mood Citation2010), recent methodological investigations have suggested these concerns are usually misplaced (Kuha and Mills Citation2018). As a sensitivity analysis, we repeated this analysis using average marginal effects and found the results (available on request) very similar. A range of regression models (logistic, ordinal, or linear depending on the structure of the outcome variable) were then used to test associations between childhood and early adult factors and the fertility stressors, and between the stressors and expected intermediate variables (labour force participation, social support and isolation, experience of divorce, wealth, and physical health). Finally, path models were fitted to investigate indirect and direct associations in more detail. The sum of standardized indirect effects from the path models including all significant paths were calculated using the theta method as recommended by Muthén and Muthén (Citation2012). Bootstrapping was used to calculate the bias-corrected 95 per cent confidence intervals for the standardized indirect effects (Fritz et al. Citation2012).
Separate analyses were undertaken for those aged 55–64 and those aged 65+ at Wave 3 because of cohort differences in fertility patterns and in access to modern methods of contraception and legal abortion. In England, the contraceptive pill became available in 1961 and legal abortion in 1967 (Sigle-Rushton Citation2008); most of those in the younger age group, but few of those in the older, would have had access to these methods of birth control. In a sensitivity analysis we also ran models for those aged 65–74, excluding those aged 75+, and found results very close to those for the whole group aged 65+. We fitted separate models for men and women because of sex differences in relevant variables, such as work history, and because we expected associations to be stronger for women. Robust standard errors were used to allow for any non-normality of the sample. Paths that were not significant (p ≥ 0.05) were dropped from the model. The weighted least squares means and variance (WLSMV) adjusted estimator, which is suitable for categorical outcomes, was used. Model fit was measured with the Comparative Fit Index (CFI) and Root Mean Square Error of Approximation (RMSEA). A CFI value of 0.95 or above and an RMSEA value of 0.05 or below indicate a good fit to the data. The descriptive analyses and regression models were conducted using Stata version 14, while Mplus version 7.3 was used to construct the path models.
Results
Descriptive results
(a) and (b) show the distributions of men and women, respectively, by age group for variables used in the analysis. Considering the ‘current status’ variables measured at Wave 5, 15 per cent of men aged 55–64 and 18 per cent of men aged 65+ reported three or more depressive symptoms at Wave 5. Consistent with previous research, the proportions of women with depressive symptoms at these ages (20 and 30 per cent) were higher than for men and showed more differentiation by age. Proportions with no current partner were also much higher for women than men and higher for older than younger respondents.
Table 1 Distribution of sample by variables used in the analysis, by sex and age group
With regard to the retrospective variables measured at Wave 3, a larger proportion of younger men and women had had a child before the age of 23/20, fewer had had four or more children, and more had ever divorced by Wave 3 than their older counterparts. These differences are consistent with known cohort variations in fertility patterns and experience of divorce (Schoen and Baj Citation1984; Office for National Statistics Citation2018). Among those aged 55–64, 17 per cent of men and 19 per cent of women had had children born less than 18 months apart; in the older age group these proportions were 20 and 22 per cent, respectively. In both age groups, around 30 per cent of men reported poor health in childhood. Childhood SEP score was lower (worse) in the older age group; however, the proportions reporting adverse childhood experiences were similar. Among women there was a greater differentiation by age in reporting of childhood health problems, and women's reports of adverse childhood experiences were slightly higher than for men. Historical changes in education are reflected in the differences between age groups in educational attainment; compared with men aged 55–64, twice as many of those aged 65+ had no formal qualifications and a smaller proportion had degree-level qualifications. Levels of educational attainment were lower in women than men, and lower among older than younger women. Over half the men in both age groups had been teenage smokers. Reported teenage smoking was higher in the younger than the older age group for women, but lower than among men. Labour force participation scores at ages 20–55, measured at Wave 3, were similar for older and younger men. Women's labour force participation scores were much lower than those for men and slightly higher for younger than older women.
In terms of variables measured at Wave 4, differences by age group in wealth quintile distribution and the social support and interaction measures were slight, but a lower proportion of men in the older than the younger group were smokers; this may partly reflect differential survival to older ages by smoking status. Higher proportions of women than men—and of older than younger women—were in lower wealth quintiles. Social support scores were slightly higher, and the proportions who were socially isolated slightly lower, for women than men aged 55–64, and for women in this age group compared with older women. The proportions of females who smoked at Wave 4 were similar to those for men and higher among younger than older women. As would be expected, the proportions with a functional limitation were much higher in the older than the younger age group and higher for women than men.
Among the smaller sample who provided data in all survey waves, distributions were broadly similar except that the proportion lacking a current partner was higher among those present at all waves, particularly among older women (results not shown; available on request).
Associations between depressive symptoms, stressors, and socio-demographic characteristics
(a) and (b) show, for men and women, respectively, results from regression models of direct (unmediated) associations between variables of interest and the proportions reporting three or more depressive symptoms at Wave 5. We fitted three models: Model 1 was adjusted only for age, Model 2 also included variables based on reported childhood circumstances, and Model 3 added all the other variables of interest.
Among men ((a)), large family size and, for older men, early fatherhood were associated with depression in the age-adjusted model (Model 1); adjusting for other variables (Model 2) attenuated these coefficients. In the fully adjusted models (Model 3), only functional limitation and childhood adverse events (younger men) or lower childhood SEP (older men) were positively associated with depression score.
Table 2 Direct associations (β from logistic regression) between fertility and other life course stressors and having three or more depressive symptoms (CES-D) in later life
Among women in the younger age group, depressive symptoms were associated with all the fertility stressors and with experience of divorce in the age-adjusted models ((b), Model 1). Adjusting for childhood circumstances (Model 2) resulted in attenuation of most associations in this group, although the association between ever divorced and CES-D strengthened in both age groups in the fully adjusted model and remained significant for older women. In these final fully adjusted models (Model 3), childhood adversity and functional limitation, but none of the fertility variables, were significantly associated with depression. Among younger women, teen smoking and wealth were also associated with depression, the former positively and the latter negatively.
These differences between results from models adjusted just for age, for age and childhood indicators, and for all variables considered reflect substantial intercorrelations between variables, including associations between stressors and background and intermediate variables (see Table A1 in the supplementary material). Fertility history items correlated with each other as expected: early parenthood was positively associated with experience of a short birth interval and both of these with higher parity. In general, early parenthood and high parity were inversely associated with higher childhood SEP, more education, social support, and wealth and positively associated with divorce, smoking, and functional limitation. Having had a short birth interval was inversely associated with wealth and positively associated with smoking and functional limitation in the younger group of women and positively associated with divorce among older women. Controlling for all these intercorrelated variables, including possible mediators of associations between fertility characteristics and depression, as in , may thus represent an ‘over-adjustment’, masking potentially important associations. To investigate this, we used path analyses to investigate linkages between childhood factors and fertility variables, and linkages between these and depressive symptoms.
Path models for depressive symptoms
(a)–(d) show results from the path models for men and women by age group for pathways of most interest for this analysis. (Figures A2(a)–(d) in the supplementary material show all pathways.) The thickness of the arrows of the paths varies according to the strength of the association (thinner for the associations with p < 0.05 and thicker for the associations with p < 0.01). The models fitted the data well for men (younger age group χ2 = 154.64, df = 77, CFI = 0.95, RMSEA = 0.033; older age group χ2 = 169.54, df = 85, CFI = 0.96, RMSEA = 0.028) and for women (younger age group χ2 = 180.25, df = 75, CFI = 0.96, RMSEA = 0.034; older age group χ2 = 167.00, df = 77, CFI = 0.97, RMSEA = 0.027). Only statistically significant pathways are shown but, even so, the diagrams illustrate the complexity of the associations we investigate. To ease interpretation, we first comment on significant direct (unmediated) linkages between variables considered and depressive symptoms. We next consider interlinkages between the three fertility stressors of interest and pathways from these to depression. Finally, we consider antecedent factors linked to the fertility variables to address the question as to whether fertility tempo and quantum mediate associations between childhood factors and later-life depression.
Figure 2 Key results from path models showing significant direct and indirect linkages from childhood factors to fertility stressors and depression, and from fertility stressors to depression. (a) Men aged 55–64. (b) Women aged 55–54. (c) Men aged 65+. (d) Women aged 65+
Note: Thicker arrow lines p < 0.01; thinner arrow lines p < 0.05. See ‘Measures’ subsection for details of variables. Source: Authors’ calculations from ELSA, Waves 3–5.
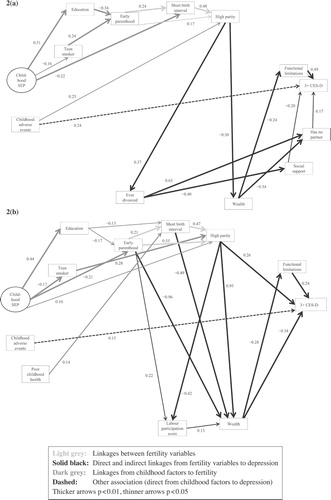
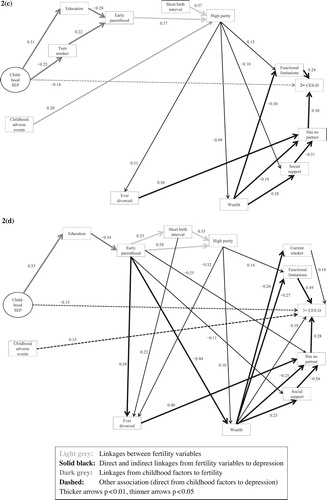
Direct (unmediated) influences on depression
(a)–(d) show that functional limitation (Wave 4) was positively associated with depressive symptoms in all age–sex groups; for older women smoking was also associated with depression. Lack of a current partner was positively associated with depression among men and older women and there was a direct link between childhood adversity (reported in Wave 3) and depression for all women and for men in the younger age group. For men and women aged 65+, higher childhood SEP was also inversely related to depression. Social support (Wave 4) was directly inversely associated with depression among men aged 55–64. For women there was an inverse association between wealth and depression for those aged 55–64, but in the older age group of women the direction of this unmediated association was positive. These risk factors were interrelated and had additional indirect effects, as discussed in the following sections. For women aged 55–64 there was a positive association between high parity and depression; otherwise none of the fertility stressors were directly linked to depressive symptoms although, as discussed later in this section, there were a number of indirect associations between fertility variables and depression.
Linkages between the fertility stressors
Early parenthood and experience of a short birth interval were both positively linked to high parity (four or more children) in all groups. There was also a positive link between early parenthood and experience of a short birth interval among men aged 55–64 and women in both age groups.
Indirect linkages between fertility stressors and depression
For men high parity was positively associated with experience of divorce which in turn was linked to depression through absence of a current partner and, in the case of younger men, lower social support. There was also an association between high parity and depression mediated by lower wealth and higher risk of functional limitation.
For women aged 65+, the association between high parity and divorce was negative but early motherhood and closely spaced births were both linked to depression through higher risk of experiencing divorce and absence of a current partner. (Among women aged 55–64 early motherhood and short birth interval were also linked to divorce, in turn associated with lack of a partner and lower social support, as shown in Figure A2(b), but in this group links between depression and current partnership and social support were not significant.) For younger women, early parenthood and experience of a short birth interval were also linked to depression through large family size.
Although there was only a direct association between large family size and depression in the younger group of women, there were a number of pathways from high parity to depression mediated through other variables. For older women, as for older men, high parity was positively associated with functional limitation and so linked to depression indirectly. For women in the younger age group high parity was negatively associated with labour force score, which was associated with wealth. However, in contrast to men, high parity among women also had an unmediated positive association with wealth, especially in the younger age group, which served to offset other adverse impacts of larger family size.
Linkages between childhood circumstances and depression mediated by fertility variables
Finally, we consider pathways from childhood circumstances to depression mediated by fertility variables. For women and men in both age groups, there was an indirect negative association between higher childhood SEP and early parenthood mediated by education (positively associated with higher childhood SEP and negatively with early parenthood) and, among men, by teen smoking (negatively associated with higher childhood SEP and positively associated with early parenthood), as well as an additional direct inverse link among women in the younger age group. Among women in the younger group, poor health in childhood was positively linked to short birth interval and, for men, childhood adversity was positively associated with large family size.
Direct, indirect, and total effects of fertility trajectories and childhood circumstances on depression
summarizes these findings and presents standardized direct (unmediated), indirect (mediated), and total (unmediated plus mediated) effects of the fertility and childhood variables on depressive symptoms. For women early motherhood and experience of a short birth interval had significant positive (adverse) indirect (and total) associations with depressive symptoms, which were stronger in the younger than the older age group. Among women aged 55–64, high parity was positively directly associated with depressive symptoms, but this was offset by a negative (beneficial) indirect association, largely mediated by the positive association with wealth already noted. Young age at fatherhood, having closely spaced children, and having a large family size all had significant positive indirect (and total) associations with depression among men, although effects were not large. In both age groups of women and the younger group of men, experience of adversity in childhood had direct effects on depression; additional indirect associations were evident for women and men in both age groups, which were partly mediated by the fertility variables. Higher childhood SEP was inversely related to depression, with associations being indirect in the younger groups (and again partly mediated by fertility) but predominantly direct among older women and men.
Table 3 Standardized direct, indirect, and total effects of fertility and childhood variables on depressive symptoms (CES-D) in later life: men and women aged 55–64 and 65+
Discussion
This paper examined associations between fertility experiences and risks of depression in later life using longitudinal data for people aged 55+ in England. Measures were based on data collected at three points in respondents’ later lives, with respondents asked about earlier life circumstances and events, including fertility history. As one of the potential fertility history stressors of interest was experience of a short birth interval, the analysis was restricted to parents of two or more children. We expected early parenthood, experience of a short birth interval, and high parity (four or more children) to be linked to depressive symptoms in later life due to both cumulative effects of stress and the impact on other sources of life course advantage and disadvantage associated with depression. We expected associations to be stronger for women than for men due to the challenges of pregnancy and childbirth, and women's greater role in childrearing. We also expected these interlinked fertility patterns, and particularly early parenthood, to mediate the effects of childhood disadvantage on later-life depressive symptoms.
Overall, results supported the hypotheses about influences of fertility stressors on later depression, but indicated that these were predominantly indirect—that is, mediated by other life course experiences—with some variation by sex and by birth cohort or age group. Initial regression analyses showed that in models adjusted for childhood circumstances (, Model 2), teen motherhood and high parity were associated with depressive symptoms among women aged 55–64 but after adjustment for later-life circumstances (Model 3), these associations were no longer significant. Similarly, for men aged 65+, there was an association between early fatherhood and depression, which ceased to be significant in the fully adjusted model. In these fully adjusted analyses, functional limitation two years before the outcome measure and either childhood adversity or childhood SEP were the variables most consistently associated with depressive symptoms among both women and men in both age groups.
Investigation of correlations between variables and the path analysis revealed a more complex pattern. For men, high parity was associated with higher chances of experiencing divorce, lower wealth and, in the older age group, lower social support—factors linked to depression through higher risk of functional limitation and lack of a partner. For women aged 55–64, high parity was linked to depression directly and early motherhood and experience of a short birth interval were indirectly linked through impacts on wealth and functional limitations. Among older women aged 65+, early parenthood was linked to experience of divorce, lower wealth, and social support, and so to depression mediated by functional limitations, smoking, social support, and absence of a current partner. Experience of a short birth interval was also positively linked to divorce, and so to depression through similar pathways. However, adverse effects of high parity on functional limitations and depression were offset, especially in the younger group of women, by a positive association between high parity and wealth. This seems surprising but, given that early motherhood and short birth intervals (associated with high parity) were both negatively associated with wealth in this group, this positive association may reflect the experience of an advantaged subgroup in these pre-second-demographic-transition cohorts, who actively chose to have a large family and had the resources to do so. As discussed later in this section, the greater availability of modern birth control methods may mean that high parity in this younger group was to a greater extent a matter of positive choice than in the older age group.
Estimation of total, direct, and indirect effects showed that among women early motherhood and experience of a short birth interval were associated with later-life depressive symptoms. Among men the total effect of all three fertility stressors on depression was significant and positive (adverse), although effects were not large. We expected associations between fertility stressors and later depression to be stronger for women than men, reflecting stresses attendant on childbirth experienced only by women and women's greater roles in childrearing and associated domestic work. Results seem to support this expectation, particularly in the younger age group, although, as we fitted models separately by sex, the significance of this difference cannot be tested. Further work on sex differences in life course impacts of fertility and parenting on later-life mental health is warranted.
Results also showed some support for the hypothesis that fertility trajectories, especially those including early parenthood, may partly mediate effects of childhood circumstances on later-life depression. Higher childhood SEP was associated positively with education and negatively with teen smoking, which were both linked (in different directions) with early parenthood. Among men, childhood adversity was also associated with high parity and, as already discussed, there were pathways from these fertility variables to depression in later life.
In interpreting these results, consideration must be paid to the different historical experiences and selection of the cohorts we consider. First, as already noted, the analyses were restricted to parents of two or more children. They thus excluded the childless (and so most of the never married) and those with only one child—groups that have higher risks of depression in later life than parents of two or more children according to previous research (Kravdal et al. Citation2015). This implies that the results reported here may be conservative in estimating the complete impact of fertility history on depression in later life. Second, those in the study needed to have survived to 2006–07. At the older end of our age distribution these survivors represent only a minority of their birth cohort. For example, while 89 per cent of males and 93 per cent of females born in 1952 survived to reach their 55th birthday in 2006–07, only 18 per cent of men and 33 per cent of women born in 1921 survived to age 85 in 2006–07 (Office for National Statistics Citation2011). Given strong social inequalities in mortality throughout the relevant period (Coleman and Salt Citation1992), this means that those considered here represent the more advantaged components of their respective birth cohorts and the extent of this social selection through prior mortality will be greater for men than women and greater at older ages. Previous research has also shown higher mortality among those with an early age at first birth and high parity (Grundy and Tomassini Citation2005; Barclay et al. Citation2016; Zeng et al. Citation2016), which again suggests that in this study of people who survived to later life, estimates may be conservative, especially for the older age group.
There are also relevant differences in the fertility of these cohorts. Only 8 per cent of females born in 1921 had a teenage birth and 16 per cent had four or more children; among those born in 1952, equivalent proportions were 25 and 10 per cent (Office for National Statistics Citation2018). These later-born women experienced their sexual debut at an earlier age and more often engaged in premarital sex than women born in the 1920s (Dunnell Citation1979). They also had greater access to modern methods of birth control and legal abortion, as the contraceptive pill first became available in 1961 and abortion was legalized in 1967. However, the pill was initially available only to married women, and use of legal abortion was limited until the mid-1970s (Sigle-Rushton Citation2008). The 1976 Family Formation Survey (FFS) found rather small differences over time in the proportion of first births described as a ‘complete accident’ (25 per cent in the 1966–67 period compared with 23 per cent in 1974–75) (Dunnell Citation1979). However, the younger group would have had more access to modern methods of birth control later in their family life cycle and this might suggest that large family size more often arose as a result of choice in the younger than the older group. Results from the FFS showed that only 30 per cent of births of orders four or higher in 1966–67 were planned (mothers reported they had been trying for a baby) compared with 53 per cent in 1974–75. This is relevant for mental health, as previous research has shown negative impacts of having an unplanned baby. For example, results based on women included in the Wisconsin Longitudinal Study, a cohort who graduated from high school in 1957, found that unintended births increased with increasing birth order and also that having a birth described as unwanted was strongly associated with poorer mental health at age 53 (Herd et al. Citation2016). Social class differences in fertility are also relevant. Before the First World War there was a substantial and graded inverse association between social class and fertility but in the middle decades of the twentieth century a J-shaped association between fertility and social class emerged, with the lowest fertility among skilled non-manual workers (clerks etc.) rather than in professional and managerial groups (Coleman and Salt Citation1992).
Study limitations and strengths
Limitations of the study include reliance on retrospective measures of circumstances in childhood and early adulthood. Although studies have shown a good correspondence between reporting of childhood circumstances and macro circumstances at the time (Havari and Mazzonna Citation2015) and have found accurate reporting of fertility history by women, men's reporting may be less good, and some recall and reporting bias is probable (Joyner et al. Citation2012). Potentially this could be influenced by mental state—although in our analysis depression was measured four years after the report of childhood circumstances and other retrospective information, so it seems unlikely that this would be a major source of bias. The data set also suffers from initial missing data (those who dropped out before Wave 3 of ELSA) and it is known that these dropouts (and decedents) include an over-representation of people in poor health and social circumstances. Our analytic strategy took account of missingness over the follow-up, but some bias may result from the initially selected sample, although comparisons with Census data have indicated that the ELSA sample has remained nationally representative (Steptoe et al. Citation2013). Strengths of the study include the theory-driven analytic strategy, the use of nationally representative longitudinal data, and the focus on understanding mediating linkages rather than just considering estimates of net effects from regression models.
Our results confirm the important influence of events and circumstances over the life course—including fertility history—on depression in older age groups. The paper also shows the usefulness of path analysis in depicting complex associations that are mediated through various factors over time and demonstrates the interlinked role of family and other life course pathways on later-life well-being. It is noteworthy that our results show direct (unmediated) influences of childhood circumstances on depressive symptoms in later life, even after the inclusion of a wide range of possible mediators. Some variations by sex and age group were found, indicating the importance of both sex and contextual issues on the association between family life courses and later mental health, both noted as important in previous studies (Umberson et al. Citation2010; Grundy and Foverskov Citation2016).
Notes and acknowledgments
1 Emily M. D. Grundy is Professor of Population Science at the Institute for Social and Economic Research, University of Essex. Sanna Read is Assistant Professorial Research Fellow at the London School of Economics. Heini Väisänen is Lecturer in Social Statistics and Demography at the University of Southampton. Please direct all correspondence to Emily Grundy, Institute for Social and Economic Research, University of Essex, Wivenhoe Park, Colchester CO4 3SQ, UK; or by E-mail: [email protected]
2 The research leading to these results received funding from the European Research Council under the European Union's Seventh Framework Programme (FP7/2007–2013)/ ERC grant agreement number 324055 and the UK Economic and Social Research Council (National Centre for Research Methods Pathways node ES/I025561/1, ES/I025561/2, and ES/I025561/3). The data were made available through the UK Data Service. ELSA was developed by a team of researchers based at NatCen Social Research, University College London, and the Institute for Fiscal Studies. The data were collected by NatCen Social Research. The funding for ELSA is provided by the US National Institute on Aging and a consortium of UK government departments coordinated by the Office for National Statistics. The developers and funders of ELSA and the UK Data Service bear no responsibility for the analyses or interpretations presented here.
Supplementary Material
Download PDF (219.4 KB)References
- Acock, Alan C. 2005. Working with missing values, Journal of Marriage and Family 67(4): 1012–1028. Available: https://doi.org/10.1111/j.1741-3737.2005.00191.x
- Aiken, Abigail R. A., Jacqueline L. Angel, and Toni P. Miles. 2012. Pregnancy as a risk factor for ambulatory limitation in later life, American Journal of Public Health 102: 2330–2335. doi: 10.2105/AJPH.2012.300791
- Aitken, Zoe, Belinda Hewitt, Louise Keogh, Anthony D. LaMontagne, Rebecca Bentley, and Anne M. Kavanagh. 2016. Young maternal age at first birth and mental health later in life: does the association vary by birth cohort? Social Science & Medicine 157: 9–17. doi: 10.1016/j.socscimed.2016.03.037
- Barban, Nicola. 2013. Family trajectories and health: A life course perspective, European Journal of Population / Revue européenne de Démographie 29(4): 357–385. doi: 10.1007/s10680-013-9296-3
- Barclay, Kieron, Katherine Keenan, Emily Grundy, Martin Kolk, and Mikko Myrskylä. 2016. Reproductive history and post-reproductive mortality: a sibling comparison analysis using Swedish register data, Social Science & Medicine 155: 82–92. doi: 10.1016/j.socscimed.2016.02.043
- Belsky, Jay, Laurence Steinberg, and Patricia Draper. 1991. Childhood experience, interpersonal development, and reproductive strategy: an evolutionary theory of socialization, Child Development 62: 647–670. doi: 10.2307/1131166
- Ben-Shlomo, Yoav and Diana Kuh. 2002. A life course approach to chronic disease epidemiology: conceptual models, empirical challenges and interdisciplinary perspectives, International Journal of Epidemiology 31(2): 285–293. doi: 10.1093/ije/31.2.285
- Brown, George W. and Tirril O. Harris. 1990. Social Origins of Depression: Study of Psychiatric Disorder in Women. London: Routledge.
- Brown, George W., Tirril Harris, Thomas K. Craig, and Rachel Handley. 2008. Parental maltreatment and adulthood cohabiting partnerships: a life-course study of adult chronic depression, Journal of Affective Disorders 110: 115–125. doi: 10.1016/j.jad.2008.01.015
- Buber, Isabella and Henriette Engelhardt. 2008. Children’s impact on the mental health of their older mothers and fathers: findings from the Survey of Health, Ageing and Retirement in Europe, European Journal of Ageing 5(1): 31–45. Available: https://doi.org/10.1007/s10433-008-0074-8
- Campbell, Doris, Edwin R. van Teilingen, and Livia Yip. 2004. Economic and social implications of multiple birth, Best Practice & Research Clinical Obstetrics & Gynaecology 18: 657–668. doi: 10.1016/j.bpobgyn.2004.04.016
- Chatfield, Mark D., Carol E. Brayne, and Fiona E. Matthews. 2005. A systematic literature review of attrition between waves in longitudinal studies in the elderly shows a consistent pattern of dropout between differing studies, Journal of Clinical Epidemiology 58(1): 13–19. Available: https://doi.org/10.1016/j.jclinepi.2004.05.006
- Clemens, S., A. Phelps, Z. Oldfield, M. Blake, A. Oskala, M. Marmot, N. Rogers, J. Banks, A. Steptoe, and J. Nazroo. 2019. English Longitudinal Study of Ageing: Waves 0–8, 1998–2017. [data collection]. 29th Edition. UK Data Service. SN: 5050. Available: http://doi.org/10.5255/UKDA-SN-5050-16
- Coleman, David and John Salt. 1992. The British Population; Patterns, Trends, and Processes, Oxford: Oxford University Press.
- Comijs, Hannie C., Aartjan T. Beekman, and Filip Smit. 2007. Childhood adversity, recent life events and depression in late life, Journal of Affective Disorders 103: 243–246. doi: 10.1016/j.jad.2007.01.012
- Conde-Agudelo, Agustín, Anyeli Rosas-Bermudez, Fabio Castaño, and Maureen H. Norton. 2012. Effects of birth spacing on maternal, perinatal, infant, and child health: a systematic review of causal mechanisms, Studies in Family Planning 43(2): 93–114. doi: 10.1111/j.1728-4465.2012.00308.x
- Dunnell, Karen. 1979. Family Formation 1976. London: HMSO.
- Eaton, William, Carles Muntaner, Corey Smith, Allen Tien, and Michele Ybarra. 2004. Center for Epidemiologic Studies Depression Scale: Review and revision (CESD and CESD-R), in Mark E. Maruish (ed), The Use of Psychological Testing for Treatment Planning and Outcomes Assessment: Volume 1: General Considerations: General Considerations, 3rd edition. Mahwah, NJ: Routledge, pp. 363–377.
- Ellis, Bruce J. 2004. Timing of pubertal maturation in girls: an integrated life history approach, Psychological Bulletin 130: 920–958. doi: 10.1037/0033-2909.130.6.920
- Enders, Craig K. and Deborah L. Bandalos. 2001. The relative performance of full information maximum likelihood estimation for missing data in structural equation models, Structural Equation Modeling: A Multidisciplinary Journal 8(3): 430–457. Available: http://dx.doi.org/10.1207/S15328007SEM0803_5
- Ermisch, John and David Pevalin. 2005. Early motherhood and later partnerships, Journal of Population Economics 18(3): 469–489. doi: 10.1007/s00148-004-0216-z
- Falci, Christina D., Jeylan T. Mortimer, and HarmoniJoie Noel. 2010. Parental timing and depressive symptoms in early adulthood, Advances in Life Course Research 15: 1–10. doi: 10.1016/j.alcr.2010.05.001
- Fiske, Amy, Julie Wetherell, and Margaret Gatz. 2009. Depression in older adults, Annual Review of Clinical Psychology 5: 363–389. doi: 10.1146/annurev.clinpsy.032408.153621
- Ford, E., C. Clark and S. A. Stansfield. 2011. The influence of childhood adversity on social relations and mental health at mid-life, Journal of Affective Disorders 133: 320–327. doi: 10.1016/j.jad.2011.03.017
- Fritz, Matthew S., Aaron B. Taylor, and David P. MacKinnon. 2012. Explanation of two anomalous results in statistical mediation analysis, Multivariate Behavioral Research 47: 61–87. doi: 10.1080/00273171.2012.640596
- Gershon, Anda, K. Sudheimer, R. Tirouvanziam, L. M. Williams, and R. O’Hara. 2013. The long-term impact of early adversity on late-life psychiatric disorders, Current Psychiatry Reports 15: 352. doi: 10.1007/s11920-013-0352-9
- Giosan, Cezar. 2013. ‘Slow’ reproductive strategy: a negative predictor of depressive symptomatology, Australian Journal of Psychology 65: 156–162. doi: 10.1111/ajpy.12016
- Grundy, Emily and Else Foverskov. 2016. Age at first birth and later life health in Western and Eastern Europe, Population and Development Review 42(2): 245–269. doi: 10.1111/j.1728-4457.2016.00128.x
- Grundy, Emily and Øystein Kravdal. 2014. Do short birth intervals have long-term implications for parental health? Results from analyses of complete cohort Norwegian register data, Journal of Epidemiology and Community Health 68: 958–964. Available: http://dx.doi.org/10.1136/jech-2014-204191
- Grundy, Emily and Sanna Read. 2012. Social contacts and receipt of help among older people in England: are there benefits from having more children? The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 67(6): 742–754. doi: 10.1093/geronb/gbs082
- Grundy, Emily and Sanna Read. 2015. Pathways from fertility history to later life health: results from analyses of the English Longitudinal Study of Ageing, Demographic Research 32(4): 107–146. doi: 10.4054/DemRes.2015.32.4
- Grundy, Emily and Cecilia Tomassini. 2005. Fertility history and health in later life: a record linkage study in England and Wales, Social Science & Medicine 61(1): 217–228. doi: 10.1016/j.socscimed.2004.11.046
- Guleria, Sonia, Kirsten E. Juul, Christian Munk, Bot Hansen, Lisen Arnheim-Dahlstrom, Kai-Li Liaw, Mari Nygard, and Susanne K. Kjær. 2017. Contraceptive non-use and emergency contraceptive use at first sexual intercourse among nearly 12 000 Scandinavian women, Acta Obstetricia et Gynecologica Scandinavica 96: 286–294. doi: 10.1111/aogs.13088
- Hale, Daniel R. and Russell M. Viner. 2016. The correlates and course of multiple health risk behaviour in adolescence, BMC Public Health 16: 458. doi: 10.1186/s12889-016-3120-z
- Hank, Karsten. 2010. Childbearing history, later-life health, and mortality in Germany, Population Studies 64(3): 275–291. doi: 10.1080/00324728.2010.506243
- Havari, Enkelejda and Fabrizio Mazzonna. 2015. Can we trust older people’s statements on their childhood circumstances? Evidence from SHARELIFE, European Journal of Population 31(3): 233–257. doi: 10.1007/s10680-014-9332-y
- Henretta, John C. 2007. Early childbearing, marital status, and women’s health and mortality after age 50, Journal of Health and Social Behavior 48(3): 254–266. doi: 10.1177/002214650704800304
- Henretta, John C., Emily M. D. Grundy, Lucy C. Okell, and Michael E. J. Wadsworth. 2008. Early motherhood and mental health in midlife: a study of British and American cohorts, Aging & Mental Health 12(5): 605–614. doi: 10.1080/13607860802343084
- Herd, Pamela, Jenny Higgins, Kamil Sicinski, and Irina Merkurieva. 2016. The implications of unintended pregnancies for mental health in later life, American Journal of Public Health 106(3): 421–429. Available: https://doi.org/10.2105/AJPH.2015.302973
- Hobcraft, John N. 2008. The timing and partnership context of becoming a parent: cohort and gender commonalities and differences in childhood antecedents, Demographic Research 19(34): 1281–1322. doi: 10.4054/DemRes.2008.19.34
- Hofferth, Sandra L., Lori Reid, and Frank L. Mott. 2001. The effects of early childbearing on schooling over time, Family Planning Perspectives 33(6): 259–267. doi: 10.2307/3030193
- Jena, Anupam B., Dana P. Goldman, and Geoffrey Joyce. 2011. Association between the birth of twins and parental divorce, Obstetrics & Gynecology 117: 892–897. doi: 10.1097/AOG.0b013e3182102adf
- Joyner, Kara., H. Elizabeth Peters, Kathryn Hynes, Asia S. Kessler, Jamie R. Taber, and Michael S. Rendall. 2012. The quality of male fertility data in major U.S. surveys, Demography 49(1): 101–124. doi: 10.1007/s13524-011-0073-9
- Kalil, Ariel and James Kunz. 2002. Teenage childbearing, marital status, and depressive symptoms in later life, Child Development, 73(6): 1748–1760. doi: 10.1111/1467-8624.00503
- Kamiya, Yumiko, Martha Doyle, John C. Henretta, and Virpi Timonen. 2013. Depressive symptoms among older adults: the impact of early and later life circumstances and marital status, Aging and Mental Health 17(3): 349–357. Available: https://doi.org/10.1080/13607863.2012.747078
- Kasen, Stephanie, Henian Chen, Joel R. Sneed, and Patricia Cohen. 2010. Earlier stress exposure and subsequent major depression in aging women, International Journal of Geriatric Psychiatry 25: 91–99.
- Kendig, Hal, Vanessa Loh, Kate O’Loughlin, Julie Byles, and James Y. Nazroo. 2015. Pathways to well-being in later life: socioeconomic and health determinants across the life course of Australian baby boomers, Population Ageing. Available: https://doi.org/10.1007/s12062-015-9132-0
- Kim, Jae-Hyun, Sang Gyu Lee, Jaeyong Shin, Kyung-Hee Cho, Jae-Woo Choi, and Eun-Cheol Park. 2015. Effects of number and gender of offspring on quality of life among older adults: evidence from the Korean Longitudinal Study of Aging, 2006–2012, BMJ Open 5: e007346. Available: http://dx.doi.org/10.1136/bmjopen-2014-007346
- Koropeckyj-Cox, Tanya, Amy Mehraban Pienta, and Tyson H. Brown. 2007. Women of the 1950s and the ‘normative’ life course: the implications of childlessness, fertility timing, and marital status for psychological well-being in late midlife, The International Journal of Aging and Human Development 64(4): 299–330. doi: 10.2190/8PTL-P745-58U1-3330
- Kravdal, Øystein, Emily Grundy, and Vegard Skirbekk. 2015. Fertility history and use of antidepressant medication in late mid-life: a register-based analysis of Norwegian women and men, Aging and Mental Health 1–10. Available: https://doi.org/10.1080/13607863.2015.1118010
- Kruk, Kai Eberhard and Steffan Reinhold. 2014. The effect of children on depression in old age, Social Science & Medicine 100: 1–11. Available: https://doi.org/10.1016/j.socscimed.2013.09.003
- Kuha, Jouni and Colin Mills. 2018. On group comparisons with logistic regression models, Sociological Methods & Research. Available: https://doi.org/10.1177/0049124117747306
- Luo, Ye and Linda J. Waite. 2005. The impact of childhood and adult SES on physical, mental, and cognitive well-being in later life, The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 60(2): S93–S101. doi: 10.1093/geronb/60.2.S93
- Mace, Ruth. 2000. Evolutionary ecology of human life history, Animal Behavior 59: 1–10. doi: 10.1006/anbe.1999.1287
- Mirowsky, John and Catherine E. Ross. 2002. Depression, parenthood, and age at first birth, Social Science & Medicine 54(8): 1281–1298. doi: 10.1016/S0277-9536(01)00096-X
- Mollborn, Stefani and Elizabeth Morningstar. 2009. Investigating the relationship between childbearing and psychological distress using longitudinal evidence, Journal of Health and Social Behavior 50: 310–326. doi: 10.1177/002214650905000305
- Mood, Carina. 2010. Logistic regression: why we cannot do what we think we can do, and what we can do about it, European Sociological Review 26: 67–82. doi: 10.1093/esr/jcp006
- Muthén, Linda K. and Bengt O. Muthén. 2012. Mplus User’s Guide. 7th edition. Los Angeles, CA: Muthén and Muthén.
- Nagi, Saad Z. 1976. An epidemiology of disability among adults in the United States, The Milbank Memorial Fund Quarterly, Health and Society 54(4): 439–467. doi: 10.2307/3349677
- Nettle, Daniel, David A. Coall and Thomas E. Dickins. 2011. Early-life conditions and age at first pregnancy in British women, Proceedings of the Royal Society B: Biological Sciences 278: 1721–1727. doi: 10.1098/rspb.2010.1726
- Nicholson, Amanda, Hynek Pikhart, Andrzej Pajak, Sofia Malyutina, R. Kubinova, A. Peasey, and Martin Bobak. 2008. Socio-economic status over the life-course and depressive symptoms in men and women in Eastern Europe, Journal of Affective Disorders 105(1–3): 125–136. Available: https://doi.org/10.1016/j.jad.2007.04.026
- Nomaguchi, Kei M. and Melissa A. Milkie. 2003. Costs and rewards of children: the effects of becoming a parent on adults’ lives, Journal of Marriage and Family 65: 356–374. Available: https://doi.org/10.1111/j.1741-3737.2003.00356.x
- Offer, Shira and Barbara Schneider. 2007. Children’s role in generating social capital, Social Forces 85: 1125–1142. doi: 10.1353/sof.2007.0049
- Offer, Shira and Barbara Schneider. 2011. Revisiting the gender gap in time-use patterns: multitasking and well-being among others and fathers in dual-earner families, American Sociological Review 76(6): 809–833. doi: 10.1177/0003122411425170
- Office for National Statistics. 2011. 2010-based national population projections lifetable template, Demographic Analysis Unit. (Crown Copyright)
- Office for National Statistics. 2018. Childbearing for women born in different years, England and Wales: 22 November 2018.
- Patel, Payal H. and Bisakha Sen. 2012. Teen motherhood and long-term health consequences, Journal of Maternal and Child Health 16: 1063–1071. doi: 10.1007/s10995-011-0829-2
- Ploubidis, George B., Lenka Benova, Emily Grundy, Daniel Laydon, and Bianca DeStavola. 2014. Lifelong socio economic position and biomarkers of later life health: testing the contribution of competing hypotheses, Social Science & Medicine 119: 258–265. Available: https://doi.org/10.1016/j.socscimed.2014.02.018
- Pudrovska, Tetyana. 2008. Psychological implications of motherhood and fatherhood in midlife: evidence from sibling models, Journal of Marriage and Family 70: 168–181. doi: 10.1111/j.1741-3737.2007.00469.x
- Pudrovska, Tetyana and Deborah Carr. 2009. Age at first birth and fathers’ subsequent health: evidence from sibling and twin models, American Journal of Men’s Health 3(2): 104–115. doi: 10.1177/1557988307306424
- Quinlan, Robert J. 2003. Father absence, parental care, and female reproductive development, Evolution and Human Behavior 24: 376–390. doi: 10.1016/S1090-5138(03)00039-4
- Radloff, Lenore S. 1977. The CES-D scale a self-report depression scale for research in the general population, Applied Psychological Measurement 1(3): 385–401. Available: https://doi.org/10.1177/014662167700100306
- Read, Sanna, Emily Grundy, and Douglas A. Wolf. 2011. Fertility history, health, and health changes in later life: a panel study of British women and men born 1923–49, Population Studies 65(2): 201–215. doi: 10.1080/00324728.2011.572654
- Rosendaal, Nicole T. A. and Catherine M. Pirkle. 2017. Age at first birth and risk of later-life cardiovascular disease: a systematic review of the literature, its limitation, and recommendations for future research, BMC Public Health 17: 627. doi: 10.1186/s12889-017-4519-x
- Schaan, Barbara. 2014. The interaction of family background and personal education on depressive symptoms in later life, Social Science & Medicine 102: 94–102. Available: https://doi.org/10.1016/j.socscimed.2013.11.049
- Schoen, R. and J. Baj. 1984. Twentieth-century cohort marriage and divorce in England and Wales, Population Studies 38: 439–449. doi: 10.1080/00324728.1984.10410302
- Shahab, Lion, Gail Gilchrist, Gareth Hagger-Johnson, Aparna Shankar, Elizabeth West and Robert West. 2015. Reciprocal associations between smoking cessation and depression in older smokers: findings from the English Longitudinal Study of Ageing, British Journal of Psychiatry 207: 243–249. doi: 10.1192/bjp.bp.114.153494
- Sigle-Rushton, Wendy. 2005. Young fatherhood and subsequent disadvantage in the United Kingdom, Journal of Marriage and Family 67(3): 735–753. doi: 10.1111/j.1741-3737.2005.00166.x
- Sigle-Rushton, Wendy. 2008. England & Wales: stable fertility and pronounced social status differences, Demographic Research 19: 455–502 (Special collection 7, Childbearing Trends and Policies in Europe). doi: 10.4054/DemRes.2008.19.15
- Spence, Naomi J. 2008. The long-term consequences of childbearing: physical and psychological well-being of mothers in later life, Research on Aging 30(6): 722–751. Available: https://doi.org/10.1177/0164027508322575
- Stafford, Mai, Anne McMunn, Paola Zaninotto, and James Nazroo. 2011. Positive and negative exchanges in social relationships as predictors of depression: evidence from the English Longitudinal Study of Aging, Journal of Aging and Health 23: 607–628. doi: 10.1177/0898264310392992
- Steptoe, Andrew, Elisabeth Breeze, James Banks, and James Nazroo. 2013. Cohort profile: the English longitudinal study of ageing, International Journal of Epidemiology 42(6): 1640–1648. Available: https://doi.org/10.1093/ije/dys168
- Taylor, Julie L. 2009. Midlife impacts of adolescent parenthood, Journal of Family Issues 30: 484–510. doi: 10.1177/0192513X08329601
- Tennant, Christopher. 2002. Life events, stress and depression: a review of recent findings, Australian and New Zealand Journal of Psychiatry 36: 173–182. doi: 10.1046/j.1440-1614.2002.01007.x
- Thorpe, Karen, Jean Golding, Ian MacGillivray, and Rosemary Greenwood. 1991. Comparison of prevalence of depression in mothers of twins and mothers of singletons, British Medical Journal 302: 875–878. doi: 10.1136/bmj.302.6781.875
- Townsend, Peter. 1979. Poverty in the United Kingdom. London: Allen Lane and Penguin Books.
- Turvey, Carolyn L., Robert B. Wallace, and Regula Herzog. 1999. A revised CES-D measure of depressive symptoms and a DSM-based measure of major depressive episodes in the elderly, International Psychogeriatrics 11: 139–148. doi: 10.1017/S1041610299005694
- Umberson, Debra, Tetyana Pudrovska, and Corinne Reczek. 2010. Parenthood, childlessness, and well-being: a life course perspective, Journal of Marriage and Family 72: 612–629. doi: 10.1111/j.1741-3737.2010.00721.x
- Virtanen, Marianna, Jane E. Ferrie, G. David Batty, Marko Elovainio, Markus Jokela, Jussi Vahtera, Archana Singh-Manoux, and Mika Kivimäki. 2015. Socioeconomic and psychosocial adversity in midlife and depressive symptoms post retirement: a 21-year follow-up of the Whitehall II study, American Journal of Geriatric Psychiatry 23(1): 99–109. doi: 10.1016/j.jagp.2014.04.001
- Wainwright, Nicolas W. and Paul G. Surtees. 2002. Childhood adversity, gender and depression over the life course, Journal of Affective Disorders 72(1): 33–44. doi: 10.1016/S0165-0327(01)00420-7
- Waynforth, David. 2012. Life-history theory, chronic childhood illness and the timing of first reproduction in a British birth cohort. Proceedings of the Royal Society B: Biological Sciences 279(1740): 2998–3002. Available: https://doi.org/10.1098/rspb.2012.0220
- Weich, Scott, Jacoby Patterson, Richard Shaw, and Sarah Stewart-Brown. 2009. Family relationships in childhood and common psychiatric disorders in later life: systematic review of prospective studies. British Journal of Psychiatry 194: 392–398. doi: 10.1192/bjp.bp.107.042515
- White, James, Paola Zaninotto, Kate Walters, Mika Kivimaki, Panayotes Demakakos, Jane Biddulph, Meena Kumari, Cesar De Oliveira, John Gallacher, and David Batty. 2016. Duration of depressive symptoms and mortality risk: The English Longitudinal Study of Ageing (ELSA), British Journal of Psychiatry 208: 337–342. doi: 10.1192/bjp.bp.114.155333
- Wilkinson, Andra L., Carolyn T. Halpern, and Amy H. Herring. 2016. Directions of the relationship between substance use and depressive symptoms from adolescence to young adulthood, Addictive Behaviour 60: 60–64. doi: 10.1016/j.addbeh.2016.03.036
- Wittchen, Hans-Ulrich, Frank Jacobi, Jürgen Rehm, Anders Gustavsson, Mikael Svensson, Bengt Jonsson, Jes Olesen, Christer Allgulander, Jordi Alonso, Carlo Faravelli, Laura Fratiglioni, Poul Jennum, Roselind Lieb, Andreas Maercker, Jim van Os, Martin Preisig, Luis Salvador-Carulla, Roland Simon, and Hans-Christoph Steinhausen. 2011. The size and burden of mental disorders and other disorders of the brain in Europe 2010, European Neuropsychopharmacology 21: 655–679. doi: 10.1016/j.euroneuro.2011.07.018
- Zeng, Yun, Ze-min Ni, Shu-yun Liu, Xue Gu, Qin Huang, Jun-an Liu, and Qi Wang. 2016. Parity and all-cause mortality in women and men: a dose-response meta-analysis of cohort studies, Scientific Reports 6: 19351. Available: https://doi.org/10.1038/srep19351