
ABSTRACT
Background: The opioid epidemic continues to generate a significant mental and physical health burden on patients, and claims the life of almost 150 Americans daily. Making matters worse, an increase in relapses and/or opioid-related deaths has been reported in more than 40 U.S. states since the start of the COVID-19 pandemic. Opioid use disorder (OUD) is one of the single most expensive disorders in the United States, generating average medical costs of $60B from just 2 million Americans diagnosed with the disorder. In commercial use since 2019, reSET-O is a non-drug, prescription digital therapeutic (PDT) that delivers evidence-based neurobehavioral treatment for OUD and helps overcome the barriers associated with access to care, stigma, and social distancing. Although shown to be cost effective and efficacious in clinical trials and real-world evidence studies, respectively, information on its value for money from a health utilities and cost per quality-adjusted life-year is needed to inform policy discussions.
Objectives: To evaluate the impact of reSET-O on health utilities and assess its overall cost per quality-adjusted life year (QALY) gained vs. treatment-as-usual (TAU).
Methods: Decision analytic model comparing reSET-O plus TAU to TAU alone (i.e. buprenorphine, face-to-face counseling, and contingency management) over 12 weeks. Clinical effectiveness data (abstinence and health utility) were obtained from a clinical trial, and resource utilization and cost data were adapted from a recent claims data analysis to reflect less frequent face-to-face counseling with the therapeutic.
Results: The addition of reSET-O to TAU decreases total health care costs by -$131 and resulted in post-treatment utility values within population norms, with a corresponding gain of 0.003 QALYs. reSET-O when used adjunctively to TAU was economically dominant (less costly, more effective) vs. TAU alone.
Conclusion: reSET-O is an economically-dominant adjunctive treatment for OUD and is associated with an overall reduction in total incremental cost vs TAU.
Introduction
As the United States continues to suffer the impact of the third wave of the opioid epidemic [Citation1], which causes the deaths of close to 50,000 Americans every year [Citation2], events such the recent economic downturn, social turmoil, and the ongoing public health impacts stemming from the COVID-19 pandemic have created even more challenging conditions for the prevention and management of opioid use disorder (OUD) [Citation3,Citation4]. This third wave of opioid-related deaths is driven by the increased availability of synthetic opioids, primarily illicitly manufactured fentanyl, and in recent years has been accompanied by an increased use of (and mortality from) stimulants such as cocaine and methamphetamines [Citation5]. The COVID-19 pandemic made matters worse by disrupting treatment and increasing social isolation and stress in this already vulnerable population [Citation4,Citation6]. It is therefore not surprising that over 40 U.S. states have reported dramatic increases in opioid related relapses and deaths since the start of the pandemic [Citation7,Citation8], and that 12-month overdose death estimates experienced the largest monthly increases ever documented in the first three months of the pandemic (March-May 2020) [Citation5]. Even prior to the COVID-19 pandemic, OUD was already one of the costliest health conditions in the U.S., generating an estimated $40-70 USDB in direct medical costs annually [Citation9,Citation10] from just two million Americans affected by the disorder [Citation11]. The recent increase in relapse rates can therefore be expected to further increase the use of emergency department [ED] visits and inpatient [IP] stays (including treatment in the intensive care unit [ICU]), which are the main cost drivers in this condition [Citation9,Citation10].
Fortunately, changes in healthcare resource utilization are dramatic among those entering treatment programs. A recent U.S. claims analysis showed a 67% reduction in total annual medical costs (from $18,000 USD to $6,000, USD the majority of which was due to a reduction in inpatient stays) with buprenorphine treatment when adherence levels of at least 60% were achieved [Citation12]. Moreover, there is an ever-expanding body of real-world observations confirming robust cost and mortality reductions with OUD interventions [Citation13–17].
The CDC considers medication-assisted therapy (MAT)/Medications for Opioid Use Disorder (MOUD) as the best treatment option for OUD, and a recent study showed that MAT/MOUD has the strongest evidence of effectiveness among the available treatment options [Citation13,Citation18]. However, access to trained clinicians represents a significant gap in the treatment of OUD [Citation19] and the drop-out rate from MAT/MOUD is high, at approximately 50% after three months [Citation20]. MAT/MOUD provide pharmacologic support for cravings and withdrawal symptoms, to complement neurobehavioral support which increases resilience and moves patients into recovery [Citation21–23]. The Community Reinforcement Approach (CRA) is a type of OUD-specific neurobehavioral support that seeks to build drug refusal skills while improving vocational, social, family and recreational aspects of patients’ lives in order to make a non-drug using lifestyle more rewarding than one with substance use [Citation21].
reSET-O is a prescription digital therapeutic (PDT) that delivers OUD-specific neurobehavioral treatment (comprised of OUD-specific CRA learning modules, fluency training [FT] to reinforce comprehension of important therapeutic concepts, and contingency management [CM] to reward and reinforce positive and constructive behaviors) and is indicated for increasing retention in treatment when used as an adjunct to buprenorphine therapy [Citation24–26]. PDTs are a subset of digital therapeutics that are available only through consultation with a prescribing clinician, and that have had their efficacy, safety, quality and security assessed and approved by the FDA. PDTs are applications that run on a smartphone or tablet, and help bridge the gap between the shortage of trained counselors and the patients in need of evidence-based therapy for their condition, while reducing patient barriers to treatment from a reduced need to travel to the medical office or take time away from work or family in order to receive neurobehavioral therapy. reSET provides treatment through a series of 67 CRA modules; each module is followed by a brief fluency training session to increase retention of the key takeaways from each module, and patients are instructed to complete four modules per week in order to provide an opportunity to interact with as much content as possible and maximize the odds of retention and adherence [Citation27]. Contingency management is managed wholly within the therapeutic to provide positive reinforcement for the completion of each module and FT dyad (rewards are in the form of a virtual ‘thumbs-up’ or take the form of electronic gift cards of nominal value that can be redeemed at various food and services vendors). Patients also receive CM for each urine drug screen showing nonuse of illicit opioids, and there were no negative consequences stemming from positive urine drug screens (i.e. rewards were not adjusted to a lower level). reSET-O was approved by the FDA for the treatment of OUD in late 2018.
Although studies using health economic models and real-world data analyses have confirmed the clinical and economic benefits of reSET-O [Citation16,Citation27,Citation28], no study has explored the impact of reSET-O on health utilities or conducted a cost-utility analysis to understand the incremental cost-effectiveness ratio (ICER) of reSET-O in combination with treatment-as-usual (TAU) compared to TAU alone (i.e. buprenorphine, face-to-face counseling, and contingency management), using inputs from the pivotal clinical trial population evaluated for reSET-O’s FDA clearance [Citation29,Citation30].
Methods
Study design and model structure
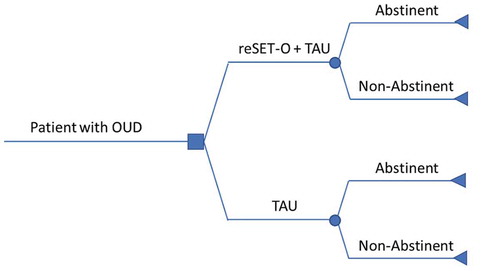
A decision analytic model to evaluate the cost-effectiveness of reSET-O + TAU relative to TAU (i.e. oral buprenorphine, face-to-face counseling, and CM) alone. The perspective of the model was a third-party payer perspective and the time horizon of the model was 12 weeks (the duration of one prescription for reSET-O). Patients treated with reSET-O + TAU or TAU alone were considered either abstinent (i.e. no opioid or cocaine use) or non-abstinent as objectively determined by urine tests 3 times per week during weeks 9–12 ().
Figure 1. Decision analytic model evaluating the cost-effectiveness of reSET-O + TAU vs. TAU (i.e. oral buprenorphine, face-to-face counseling, and CM) alone
Decision analytic model inputs
Clinical inputs – effectiveness and health state utilities
Clinical inputs were obtained from the same population as in the published clinical trial by Christensen et al. (NCT00929253) [Citation29,Citation30], which was reviewed by FDA in granting clearance for reSET-O. Briefly, this study included patients responding to radio/newspaper advertisements or flyers, or referred (by existing participants, or by local clinics) to the Center for Addiction Research, University of Arkansas for Medical Sciences (UAMS), who tested positive for opioids at screening. Study participants had a mean age of 34.4 years, 54% male, had 5.7 years of opioid use on average, and 14% were injection drug users. Participants were randomized using minimum likelihood allocation (accounting for differences in characteristics likely to influence outcomes: buprenorphine stabilization dose, distance from clinic, receipt of previous treatment for opioid dependence, and cocaine use in last 30 days) into two groups: the digital therapeutic precursor to reSET-O known as the Therapeutic Education System (TES) in addition to treatment as usual (TAU), or to TAU alone (consisting of buprenorphine, minimal therapist counseling, and contingency management). This study found significantly greater retention rates for the TES+TAU vs. TAU after 12 weeks (digital therapeutic+TAU 82.6% vs. TAU 68.4%; HR 0.49, 95% CI 0.26–0.92; p = .02) [Citation30]. The estimate of the likelihood of abstinence from opioids and cocaine during weeks 9–12 in this trial population was used as the model input, and was determined by a generalized estimating equation model for testing negative for opioids and cocaine (to ensure true abstinence from opioids that was not replaced by use of another common substance at the time of the trial) at any time point during the last month of treatment (digital therapeutic+TAU: 75.9%, vs. TAU: 60.6%; OR 2.05, 95% CI 1.07–3.90; p = .03) [Citation30] (). Health state utilities were obtained for abstinent and non-abstinent patients by mapping the addiction severity index (ASI) score and patient characteristics from Christensen et al. to baseline, week 12, and change from baseline (at week 12) SF-6D utility scores for reSET-O + TAU and TAU [Citation31] (). SF-6D population norm scores range between 0.77 and 0.80 [Citation32]. A change in SF-6D score >0.03 indicates a clinically meaningful change in health utility levels [Citation33].
Table 1. Clinical and economic model inputs for reSET-O + TAU vs. TAU cost-effectiveness model
CM, contingency management; CMS, Centers for Medicare and Medicaid Services; SF, Short-Form; TAU, treatment-as-usual; WAC, wholesale acquisition cost.
Economic inputs – treatment intervention costs
The cost of a 12-week prescription of reSET-O was assumed to be $1,440 USD based on the Red Book wholesale acquisition cost (WAC) cost of $1,665 USD and assuming a 13.5% discount (5% discounts off WAC, plus 8.5% reimbursement for non-engaging patients (based on a recent claims analysis of patients prescribed reSET-O). CM implementation and administration costs of $350 USD were only included for TAU alone as these are already included in the reSET-O cost. TAU costs over 12 weeks were equal for both treatment arms (total of $3,086 USD) and included office visit costs that accounted for a reduced number of face-to-face counseling visits for reSET-O (3 visits at $33 USD/visit for reSET-O, and 6 visits at $33 USD/visit for TAU), urinalysis costs (12 urinalyses at $70 USD/urinalysis), and buprenorphine costs (3 prescriptions at $123 USD/prescription) ().
Economic inputs – medical costs
The medical costs of buprenorphine-adherent vs. non-adherent were obtained from a recent evaluation of the Truven Health MarketScan® Commercial and Medicare Supplemental Research Databases [Citation27]. Adherence to treatment was defined as the proportion of days covered (PDC) by buprenorphine across the 12 weeks. Patients with a proportion of days covered (PDC) ≥0.8 and <0.8 over 12 weeks were categorized as adherent and nonadherent, respectively. Twelve-week medical costs for patients categorized as adherent ($3,887) and nonadherent ($11,291) to buprenorphine treatment were utilized as estimates of medical costs for patients who were abstinent and non-abstinent, respectively. The cost for the reSET-O + TAU and TAU arms was calculated using the formulas below:
MedicalCostreSET-O + TAU = MedicalCostAbstinent × RetentionreSET-O + TAU + TAU+ MedicalCostNon-abstinent × (1 – AbstinencereSET-O + TAU)
MedicalCostTAU = MedicalCostAbstinent × RetentionTAU + MedicalCostNon-abstinen × (1 – AbstinenceTAU)
Analyses
Clinical and economic consequences are presented in disaggregated form. Clinical effectiveness is presented as the number of quality-adjusted life years (QALYs) for each treatment arm assuming no carry over effect after 12 weeks. Disaggregated costs for the two treatment arms included the cost of reSET-O, CM costs, treatment intervention costs (i.e. office visits, urinalyses, and buprenorphine), and medical costs associated with abstinence or non-abstinence. The cost-effectiveness was calculated as the incremental total cost over 12 weeks divided by the incremental QALYs over 12 weeks.
Sensitivity analyses were conducted to determine the impact of using alternate plausible model values using: (1) Health utility change values added to the study population’s baseline health utility value (), and (2) Population-derived utility values from the Institute for Clinical and Economic Review report [Citation37] (utility on MAT without illicit use of opioids = 0.766 and utility on MAT with illicit use of opioids (50% not injected + 50% injected) = (0.694 + 0.574)/2 = 0.634) for abstinent and non-abstinent patients, respectively (for both reSET-O + TAU and TAU alone).
Results
Base case
Over 12 weeks, the incremental costs and QALYs-gained with reSET-O + TAU vs. TAU were -$131 and 0.003, corresponding to economic dominance vs. TAU ().
Table 2. Base case clinical and economic consequences and cost-effectiveness of reSET-O + TAU vs. TAU
CM, contingency management; QALY, quality-adjusted life year; TAU, treatment-as-usual.
Sensitivity analyses
Results of the two sensitivity analyses using alternate plausible values resulted in greater QALY gains compared to the base case. Results are presented in .
Table 3. Sensitivity analyses for reSET-O + TAU vs. TAU cost-effectiveness model
ICER, incremental cost-effectiveness; QALY, quality-adjusted life year; TAU, treatment-as-usual.
Discussion
Results of this model showed population-level gains in quality-adjusted life years and savings of -$131 over 12 weeks with reSET-O treatment, representing a greater than 100% return on investment. In addition to clinical value, these results emphasize the limited economic risk of reSET-O as an adjunct to TAU, based on the economic dominance shown in this model.
The main drivers of this model were 1) the favorable odds of abstinence with reSET-O, 2) greater and clinically meaningful changes in health utilities in abstinent patients, and 3) reduced medical costs in patients achieving abstinence. Importantly, this model used abstinence and health utility values derived from the same clinical trial population of reSET-O-treated patients and randomized control patients avoiding the pitfalls of obtaining from a potentially dissimilar patient population. Notably, the baseline health utility values for this trial population (0.745) were below U.S. population norms (0.77–0.80) [Citation32], indicating a poorer health status than the general U.S. population. In contrast, abstinence was associated with health utilities within or just below U.S. population norms, regardless of treatment arm. Clinically meaningful changes in health utility levels (>0.03) [Citation33] were observed in reSET-O abstinent, and non-abstinent patients, while changes in health utilities in TAU patients did not achieve clinical meaningfulness, worsening in patients not achieving abstinence. Cost reductions with MAT/MOUD have been observed in previous studies and have been explained by a reduction in the risk of ED visits and hospitalizations [Citation12–16]. MAT/MOUD attenuates the physiologic drivers of illicit opioid use (i.e. cravings and withdrawal symptoms) through medications, while helping patients develop productive coping mechanisms and resilience to promote short-term harm reduction (reduced exposure to illicit opioids) through OUD-specific neurobehavioral therapy [Citation38]. Without MAT/MOUD, patients are much more frequently exposed to the harms of illicit opioids, which include overdoses, infectious disease (HCV, HIV, endocarditis), trauma, and violence, and more likely to be frequent users of the hospital facility services [Citation6,Citation12,Citation17,Citation22,Citation39]. This high rate of healthcare resource use and recidivism is driven by the ease with which accidental overdoses occur as a result of the increased tolerance to the euphoric effects of opioids, which require higher and more frequent doses over time [Citation40]. Greater doses increase the potential for crossing the threshold for respiratory depression and arrest, end organ damage, and ultimately death [Citation41]. OUD, just like any other chronic disease, requires ongoing and evolving treatment in order to achieve long-term success [Citation42], and PDTs can help deliver safe, effective treatments, via platforms with demonstrated quality as an extension of the clinical care team during critical times marked by social distancing and isolation and potential treatment interruptions. Telehealth solutions may also benefit from scaling up the number of patients with access to asynchronous neurobehavioral treatment that is highly specific to OUD.
The limitations of this study are similar to any modeling study, as models are only an approximation of real-world conditions [Citation43], and are unable to fully replicate a conditions as complex as OUD, which is influenced by different societal, social, economic, and health factors [Citation44], and factors related to subgroups, such as gender or duration of disease. Cost-effectiveness analyses are designed to measure the potential impact across an entire population of patients [Citation43], and will likely not reflect the true value in patient populations that have made a decision with their clinician to undergo treatment with a PDT. Nevertheless the results of this model show that at the population level, more than 100% of the initial investment in the PDT is recouped within three months, while also producing a net QALY benefit. These results therefore provide an important benchmark on the potential value of a health care technology which helps inform policy discussions. Another limitation is that health utilities were not directly measured in the clinical trial but instead were derived from the addiction severity index, a validated instrument which has been previously shown to map to SF-6D scores [Citation31]. However, this lack of direct measurement of utilities is not expected to have a significant impact on the findings of this model, as baseline and week 12 health utility values were comparable to other published US values, with slightly higher health utilities values for the reSET-O population at both the initiation stage of treatment and with stabilized treatment [Citation45]. Lastly, the results of this model are limited to 12 weeks, as the goal was to show the short-term value for money of reSET-O using non-extrapolated clinical trial data. As real-world evidence for the impact of reSET-O beyond 12 weeks becomes available it will provide better data about reSET-O’s effectiveness. For example, a recent analysis of the first real-world, intent-to-treat cohort of patients prescribed reSET-O and with available health care claims data showed IP, ICU, and ED utilization and net cost reduction of $2,150 USD/patient in the 6 months following initiation of the therapeutic, despite these patients exhibiting high levels of adherence to buprenorphine treatment during the baseline 6-month period (i.e. before the initiation of reSET-O) [Citation16]. Since its launch reSET-O has been prescribed to over 5,000 patients with OUD as an adjunct to buprenorphine MAT/MOUD, creating a broad platform for future long-term analyses of its real-world effectiveness.
Conclusion
This economic analysis found that reSET-O is a cost-effective treatment option for OUD. Reductions in medical costs following the initiation of reSET-O offset more than the initial cost of the PDT while increasing health utilities and QALYs. reSET-O was shown to be cost-effective compared to TAU alone over 12 weeks and exhibited economic dominance, and sensitivity analyses around utility values resulted in greater utility gains and more-favorable ICERs. These results underscore the limited economic risk of providing access to reSET-O, as part of the overall effort to help patients safely avoid, and eventually cease, the use of illicit opioids.
Transparency
Declaration of financial/other relationships
FV, HFL and RG are all employees of Pear Therapeutics Inc.
BP, DMD, DCM are consultants to Pear Therapeutics Inc.
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Declaration of interest
No potential conflict of interest was reported by the authors.
Acknowledgments
Writing and editorial support for the preparation of this abstract was provided by Natalie C. Edwards, MSc of Health Services Consulting Corporation and funded by Pear Therapeutics, Inc.
Additional information
Funding
References
- Center for Disease Control and Prevention (CDC). Opioid Overdose. Understanding the Epidemic [Cited 2020 Dec 3]. Available from: https://www.cdc.gov/drugoverdose/epidemic/index.html.
- Centers for Disease Control and Prevention, National Center for Health Statistics. Multiple Cause of Death 1999-2018 on CDC WONDER Online Database, released January, 2020 [Cited 2020 Dec 3]. Available from: https://www.drugabuse.gov/drug-topics/trends-statistics/overdose-death-rates.
- Wakeman SE, Green TC, Rich J. An overdose surge will compound the COVID-19 pandemic if urgent action is not taken. Nat Med. 2020 Jun;26(6):819–820.
- Becker WC, Fiellin DA. When epidemics collide: coronavirus disease 2019 (COVID-19) and the opioid crisis. Ann Intern Med. 2020;173(1):59–60.
- Centers for Disease Control and Prevention (CDC). Health advisory (CDCHAN-00438). Increase in Fatal Drug Overdoses Across the United States Driven by Synthetic Opioids Before and During the COVID-19 Pandemic. 2020 [Cited 2021 Jan 5]. Available from: https://emergency.cdc.gov/han/2020/han00438.asp?ACSTrackingID=USCDC_511-DM44961&ACSTrackingLabel=HAN%20438%20-%20General%20Public&deliveryName=USCDC_511-DM44961.
- The Opioid Response Network. The opioid epidemic and COVID-19: how social determinants of health create differential impacts. 2020 [Cited 2021 Jan 5]. Available from: https://opioidresponsenetwork.org/documents/SDH_OUD-COVID-19.pdf
- American Medical Association (AMA). Issue brief: reports of increases in opioid-related overdose during COVID pandemic. 2020 [Cited 2020 Dec 3]. Available from: https://www.ama-assn.org/system/files/2020-11/issue-brief-increases-in-opioid-related-overdose.pdf.
- Slavova S, Rock P, Bush HM, et al. Signal of increased opioid overdose during COVID-19 from emergency medical services data. Drug Alcohol Depend. 2020;214:108176.
- Society of Actuaries. Economic Impact of Non-Medical Opioid Use in the United States [Cited 2020 Dec 3]. Available from: https://www.soa.org/globalassets/assets/files/resources/research-report/2019/econ-impact-non-medical-opioid-use.pdf.
- Florence C, Luo F, Rice K. The economic burden of opioid use disorder & fatal opioid overdose in the United States, 2017. Drug Alcohol Depend. 2020. In Press. DOI:10.1016/j.drugalcdep.2020.108350
- Substance Abuse and Mental Health Services Administration (SAMHSA). Key substance use and mental health indicators in the United States: Results from the 2018 National Survey on Drug Use and Health (HHS Publication No. PEP19-5068, NSDUH Series H-54). 2019 [Cited 2020 Dec 3]. Available from: www.samhsa.gov/data/.
- Ruetsch C, Tkacz J, Nadipelli VR, et al. Heterogeneity of nonadherent buprenorphine patients: subgroup characteristics and outcomes. Am J Manag Care. 2017 Jun 1;23(6):e172–e179.
- Wakeman SE, Larochelle MR, Ameli O, et al. Comparative effectiveness of different treatment pathways for opioid use disorder. JAMA Network Open. 2020;3(2):e1920622–e1920622. .
- Ronquest NA, Willson TM, Montejano LB, et al. Relationship between buprenorphine adherence and relapse, health care utilization and costs in privately and publicly insured patients with opioid use disorder. Subst Abuse Rehabil. 2018;9:59–78.
- Lynch FL, McCarty D, Mertens J, et al. Costs of care for persons with opioid dependence in commercial integrated health systems. Addict Sci Clin Pract. 2014 [2014 08 14];9(1):16. .
- Velez FF, Colman S, Kauffman L, et al. Real-world reduction in healthcare resource utilization following treatment of opioid use disorder with reSET-O, a novel prescription digital therapeutic. Expert Review of Pharmacoeconomics & Outcomes Research. 2020.
- Johnson K, Hills H, Jifeng M, et al. Treatment for opioid use disorder in the Florida medicaid population: using a cascade of care model to evaluate quality. Am J Drug Alcohol Abuse. 2020;1–9. DOI:10.1080/00952990.2020.1824236
- Centers for Disease Control and Prevention (CDC). Opioid Overdose: Assessing and Addressing Opioid Use Disorder (OUD). 2018 [Cited 2021 Jan 5]. Available from: https://www.cdc.gov/drugoverdose/training/oud/accessible/index.html
- Madras B, Ahmad NJ, Wen J, et al., and the Prevention, Treatment, and Recovery Working Group of the Action Collaborative on Countering the U.S. Opioid Epidemic. Improving Access to Evidence-Based Medical Treatment for Opioid Use Disorder: Strategies to Address Key Barriers Within the Treatment System 2020 [Cited 2020 Dec 3]. Available from: https://nam.edu/improving-access-to-evidence-based-medical-treatment-for-opioid-use-disorder-strategies-to-address-key-barriers-within-the-treatment-system/.
- Hser Y-I, Saxon AJ, Huang D, et al. Treatment retention among patients randomized to buprenorphine/naloxone compared to methadone in a multi-site trial. Addiction. 2014;109(1):79–87.
- NIDA. 2020, June 1. Community Reinforcement Approach Plus Vouchers (Alcohol, Cocaine, Opioids)[Cited 2020 Dec 3]. Available from: https://www.drugabuse.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition/evidence-based-approaches-to-drug-addiction-treatment/behavioral-therapies/community-reinforcement-approach-vouchers.
- McLellan AT, Arndt IO, Metzger DS, et al. The effects of psychosocial services in substance abuse treatment. JAMA. 1993;269(15):1953–1959.
- Marsch LA, Dallery J. Advances in the psychosocial treatment of addiction: the role of technology in the delivery of evidence-based psychosocial treatment. Psychiatr Clin North Am. 2012;35(2):481–493.
- Pear Therapeutics Inc. reSET-O - Clinician Instructions for Use. 2019 [Cited 2020 Aug 17]. Available from: https://peartherapeutics.com/wp-content/uploads/2019/08/PEAR-MKT-025-reSET-O-Clin-Brief-Sum_Dec2019.pdf.
- Vilardaga R, Fisher T, Sabo PL, et al. (2020). Review of popularity and quality standards of opioid-related smartphone apps. Current Addiction Reports. DOI: 10.1007/s40429-020-00344-6
- Tkacz J, Volpicelli J, Un H, et al. Relationship between buprenorphine adherence and health service utilization and costs among opioid dependent patients. J Subst Abuse Treat. 2014;46(4):456–462.
- Maricich YA, Xiong X, Gerwien R, et al. Real-world evidence for a prescription digital therapeutic to treat opioid use disorder. Curr Med Res Opin. 2020. DOI:10.1080/03007995.2020.1846023
- Wang W, Gellings Lowe N, Jalali A, et al. Economic modeling of reSET-O, a prescription digital therapeutic for patients with opioid use disorder. J Med Econ. 2020. DOI:10.1080/13696998.2020.1858581
- Christensen DR, Landes RD, Jackson L, et al. Adding an internet-delivered treatment to an efficacious treatment package for opioid dependence. J Consult Clin Psychol. 2014;82(6):964–972. .
- Maricich YA, Bickel WK, Marsch LA, et al. Safety and efficacy of a prescription digital therapeutic as an adjunct to buprenorphine for treatment of opioid use disorder. Curr Med Res Opin. 2020. DOI:10.1080/03007995.2020.1846022
- Pyne JM, Tripathi S, French M, et al. Longitudinal association of preference-weighted health-related quality of life measures and substance use disorder outcomes. Addiction. 2011;106(3):507–515.
- Fryback DG, Dunham NC, Palta M, et al. U.S. norms for six generic health-related quality-of-life indexes from the national health measurement study. Med Care. 2007;45(12):1162–1170. .
- Walters SJ, Brazier JE. What is the relationship between the minimally important difference and health state utility values? The case of the SF-6D. Health Qual Life Outcomes. 2003;1(1):4.
- IBM Micromedex RED BOOK [Internet]. IBM Watson Health™, an IBM Company; c2017. [cited 2019 Feb 20]. Available from: https://www.ibm.com/us-en/marketplace/micromedex-red-book.
- Sindelar JL, Olmstead TA, Peirce JM. Cost-effectiveness of prize-based contingency management in methadone maintenance treatment programs. Addiction. 2007;102(9):1463–1471.
- Petry NM, DePhilippis D, Rash CJ, et al. Nationwide dissemination of contingency management: the veterans administration initiative. Am J Addict. 2014;23(3):205–210.
- Institute for Clinical and Economic Review (ICER). Extended-Release Opioid Agonists and Antagonist Medications for Addiction Treatment (MAT) in Patients with Opioid Use Disorder: Effectiveness and Value. 2018 [Cited 2020 Dec 3]. Available from: https://icer-review.org/wp-content/uploads/2018/04/ICER_Opioid_Use_Disorder_Draft_Evidence_Report_090718-1.pdf.
- Bickel WK, Marsch LA, Buchhalter AR, et al. Computerized behavior therapy for opioid-dependent outpatients: a randomized controlled trial. Exp Clin Psychopharmacol. 2008;16(2):132–143.
- Proctor R, Taylor MP, Quinn M, et al. Alarming rate of substance use in motor vehicle collisions at an appalachian trauma center. Cureus. 2020 December 03;12(12):e11863.
- Cahill CM, Walwyn W, Taylor AMW, et al. Allostatic mechanisms of opioid tolerance beyond desensitization and downregulation. Trends Pharmacol Sci. 2016 Nov;37(11):963–976.
- Montandon G, Slutsky AS. Solving the opioid crisis: respiratory depression by opioids as critical end point. Chest. 2019 Oct;156(4):653–658.
- Morse ED. Addiction is a chronic medical illness. N C Med J. 2018 May-Jun;79(3):163–165. . PMID: 29735618
- Chisholm D, Evans DB. Economic evaluation in health: saving money or improving care? J Med Econ. 2007;10(3):325–337.
- Sulley S, Ndanga M. Inpatient opioid use disorder and social determinants of health: a nationwide analysis of the national inpatient sample (2012-2014 and 2016-2017). Cureus. 2020 November 03;12(11):e11311.
- Wittenberg E, Bray JW, Aden B, et al. Measuring benefits of opioid misuse treatment for economic evaluation: health-related quality of life of opioid-dependent individuals and their spouses as assessed by a sample of the US population. Addiction. 2016;111(4):675–684.