
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Governments and policymakers have initiated a wide range of responses to mitigate the propagation of the disease. These responses have consisted of different policies and the devising of protocols and standards. As these responses proliferate, there is a pressing need to evaluate the stringency, effectiveness, and results of imposing them on the COVID-19 infection rates. The aim of this study is to measure the effects of policy control and restrictions on COVID-19 prevalence in the Global South. Six policy responses to COVID-19 were used to investigate and explain the stringency and effectiveness of the imposed policies in mitigating the disease’s transmission. The evaluation of these policies was based on the population’s responses as of 4 June 2020 compared to an assessment period (the median value from the five-week period between 3 January and 6 February 2020). Using geographic information systems (GIS) techniques and the analytical hierarchical process (AHP) method, an overall government response and stringency index was constructed as an effective proxy to assess populations’ responses to such policies in the Global South countries. The findings show variations in people’s responses toward the lockdown policies imposed by the countries in the Global South.
为了减轻新冠病毒的传播, 各国政府和政策制定者启用了多种应对措施, 包括政策、协议和标准。随着这些措施的扩散, 迫切需要评估它们对新冠病毒感染率的严格性、有效性和结果。本研究旨在衡量政策控制和限制对发展中国家新冠病毒流行的影响。本文采用新冠病毒政策的六项反应, 研究和解释了政策在减轻疾病传播方面的严格性和有效性。本文对比了截至2020年6月4日与评估期(2020年1月3日至2月6日五个星期的中值)人们的反应, 对这些政策进行了评估。利用地理信息系统和层次分析法, 本文构建了一个政府反应和严格程度的综合指数, 将其做为发展中国家人们对措施反应的有效替代评估指标。结果显示, 人们对发展中国家的封锁政策有不同的反应。
Gobiernos y legisladores han intentado una amplia gama de respuestas para mitigar la propagación de la enfermedad. Tales respuestas comprenden diferentes estrategias políticas y la adopción de diferentes protocolos y estándares. A medida que proliferan estas respuestas, se vislumbra también la apremiante necesidad de evaluar el rigor, efectividad y resultados de su imposición sobre las tasas de infección del COVID-19. El propósito de este estudio es medir los efectos de las políticas de control y las restricciones sobre la prevalencia del COVID-19 en el Sur Global. Se usaron seis respuestas de políticas sobre el COVID-19 para investigar y explicar el rigor y la efectividad de las políticas impuestas para mitigar la transmisión de la enfermedad. La evaluación de estas políticas se basó en las respuestas de la población hasta el 4 de junio de 2020, en comparación con un período de evaluación (el valor medio del período de cinco semanas que se extendió desde el 3 de enero hasta el 6 de febrero del 2020). Usando técnicas de los sistemas de información geográfica (SIG) y el método del proceso analítico jerárquico (AHP), se construyó un índice general de respuesta y rigor del gobierno como indicador eficaz para evaluar las respuestas de la población a tales políticas en los países del Sur Global. Los resultados muestran variaciones en las respuestas de la gente hacia las estrategias de confinamiento impuestas por los países del Sur Global.
Since the detection of the novel coronavirus in China and the propagation of COVID-19 worldwide, as well as the declaration of a pandemic by the World Health Organization (WHO), the COVID-19 pandemic has had a detrimental impact on every aspect of human life, particularly the economy, environment, social life, and health care systems (Ali and Alharbi Citation2020; Díaz de León-Martínez et al. Citation2020; International Labour Organization Citation2020b; Tobías Citation2020; Abulibdeh Citation2021). The health crises translated into an economic crisis, with governments taking measures to curb the spread of the pandemic. Several countries followed two main fundamental strategies in dealing with the pandemic. The first was a strategy that attempts to alleviate the adverse effects of the disease outbreak, and the second relies on more rigorous measures to suppress and reverse the growth trajectories (Cowling and Aiello Citation2020; Depellegrin et al. Citation2020; Nikhat and Fazil Citation2020; Qi et al. Citation2020; Tobías Citation2020). These strategies were adopted and implemented by many countries across the globe, particularly the developing nations.
A number of protective measures were enforced by governments to restrain the rapidly increasing spread of the virus and to flatten the curve of infected cases (Abulibdeh Citation2020; Dempster et al. Citation2020; Nicola et al. Citation2020). These measures included but were not limited to lockdown policies, social distancing, self-isolation, a ban on congregations, avoiding public or crowded spaces, border shutdowns, and travel restrictions (United Nations Citation2020). In addition, numerous intervention actions were taken to control disease prevalence, such as screening, medically testing people, assessing clinical severity, controlling transmission, and research on drug treatments (Chintalapudi, Battineni, and Amenta Citation2020; Díaz de León-Martínez et al. Citation2020; Fadare and Okoffo Citation2020; Lin, Liu, and Chiu Citation2020). Furthermore, the WHO has marked the health authorities’ protocols of action and has urged governments to impose containment and suppression measures to reduce the propagation of COVID-19. These measures range from strict controls on social gathering, travel, lockdown, staying at home or self-quarantining, and commercial activities to less strict measures (e.g., covering the face by wearing a disposable face mask, encouraging handwashing practices and hygiene habits, using sanitizers containing an appropriate concentration of alcohol, employing social distancing, and epidemiological surveillance) designed to shield immunologically compromised individuals and implement treatment for victims (Abulibdeh Citation2020; Anderson et al. Citation2020; Díaz de León-Martínez et al. Citation2020; Hellewell et al., Citation2020; Shim et al. Citation2020; Tahir and Batool Citation2020; Wang et al. Citation2020). The variation of rapidity in imposing mitigation measures and the strictness of the policies across countries reflect divergent assessments of the socioeconomic impacts and the public health risks of different policies (Wells et al. Citation2020).
The destructive impacts of the COVID-19 pandemic have been felt globally across societies and economies, despite the low incidence of the disease in certain regions (Khan et al. Citation2020). The COVID-19 pandemic has shown its spatial frame as well as its evolving and emerging patterns, taking advantage of our geographical settings for escalating its spread (Bertuzzo et al. Citation2020; Hass and Arsanjani Citation2021; Verity et al. Citation2020). The spread of the virus placed intense pressure on the national health systems in all countries around the world. Furthermore, the demand for intensive care beds and mechanical ventilators increased rapidly and exceeded availability in many countries (Rivera-Rodriguez and Urdinola Citation2020; Walker et al. Citation2020; Tyrrell et al. Citation2021). This pressure is notably more severe in various countries of the Global South, particularly in low-income countries with poor resources where the availability, capacity, and quality of health care services and associated resources, such as oxygen, are typically limited (Hogan et al. Citation2020; Roberton et al. Citation2020; Walker et al. Citation2020; Zwama et al. Citation2021). Similarly, compared to high-income countries, the number of hospital beds per population in these countries is lower (median 1.28 beds compared to 4.68 beds per 1,000 population; Testa, Rennó Santos, and Weiss Citation2020; Walker et al. Citation2020; Sen-Crowe et al. Citation2021). Furthermore, the average percentage of hospital beds that are in intensive care units is 1.47 percent in low-income countries compared to 3.3 percent in high-income countries (Atumanya et al. Citation2020; Walker et al. Citation2020). These countries also have a limited capacity for mechanical ventilation, which is required for most COVID-19 intensive care unit patients (Guérin and Lévy Citation2020). For example, according to a recent estimate across sub-Saharan Africa, the number of ventilators is only 172 per country (Walker et al. Citation2020). These devices are crucial in COVID-19 treatment and the mortality rate would be in the range of 90 percent to 100 percent in the absence of these devices compared to a mortality rate of 51.6 percent in patients who require mechanical ventilation in the United Kingdom, for example (Walker et al. Citation2020). In addition, the mortality rates in low-income countries were higher in persons with severe pneumonia and required hospitalization than they were for people in high-income countries (Salluh, Lisboa, and Bozza Citation2020; A. K. Singh and Misra Citation2020; Testa, Rennó Santos, and Weiss Citation2020). It was estimated that the mortality rates across all age groups were between 20 percent and 30 percent if oxygen support is available (Walker et al. Citation2020). These numbers are not similar to what was found in all countries in the Global South, however, and there is considerable heterogeneity in these rates due to the differences in both the quality of hospital care and availability of hospital infrastructures and the facilities within and between countries.
The mortality rate increases among elderly people and people with underlying comorbidities such as diabetes, hypertension, chronic obstructive pulmonary disease, and coronary vascular disease (Ghisolfi et al. Citation2020; Walker et al. Citation2020). These comorbidities serve to exacerbate symptoms of those who are infected. The prevalence of these conditions varies across populations and by age. In the Global South, many countries are witnessing a higher burden of infectious diseases such as tuberculosis, malnutrition, and HIV/AIDS compared to Global North countries (Rivera-Rodriguez and Urdinola Citation2020; Walker et al. Citation2020). These diseases usually occur in younger populations. Therefore, the risk of higher infection and mortality rates in these countries will be higher than in other countries in the Global North (Frost et al. Citation2021). Investigating the extent to which these comorbidities might elevate the infection and mortality rates in the Global South countries could help in designing policies and strategies to protect their population and reduce the propagation rate of the virus.
Considering the demographic structure, the Global North countries tend to have the oldest populations, who are more vulnerable to the effects of COVID-19 (Walker et al. Citation2020; Frost et al. Citation2021). By contrast, Global South countries are characterized by their younger populations; however, although this age cohort is at low risk of infection, health systems have limited capacity and higher intergenerational contact compared to high-income countries. These factors thus negate the benefit of having younger populations (Walker et al. Citation2020; Frost et al. Citation2021). Moreover, many countries in this region are still harshly affected by the propagation of the disease in both economic and epidemiological terms (Salye et al. Citation2021). Additionally, household size is a key element for virus transmission. For instance, the average size of households is larger in the Global South countries and the percentage of households that have residents over the age of sixty-five is also higher in Global South countries than in high-income countries in the Global North (Walker et al. Citation2020). Consequently, the overcrowding and elderly population might increase the transmission of the disease. Furthermore, in the Global South countries, the contact pattern between age groups tends to be higher compared to that in high-income countries (Walker et al. Citation2020; Salye et al. Citation2021), indicating that elderly people maintain higher rates of contact with other age cohorts. Therefore, global cooperation in the current pandemic can support countries in the Global South to minimize the risks related to the propagation of the virus either in the restriction stages or in the vaccination phases (Amaya and De Lombaerde Citation2021).
At the beginning of the pandemic, many Global North countries (i.e., Germany, Britain, France) turned more inward and became more nationalistic, prioritizing their citizens rather than increasing their collaboration with other low-income countries or global institutions. This is not an option for the Global South countries, where collaboration with international organizations and high-income countries is important to mitigate the negative effect of the propagation of the virus (Amaya and De Lombaerde Citation2021; Lai et al. Citation2021). The low-income countries in the Global South imposed different mitigation measures and strategies to slow the propagation of the disease; however, despite imposing these strategies, the pandemic rapidly overwhelmed health systems, resulting in substantial excess deaths due to the poorer health care available (Chowdhury and Jomo Citation2020).
Different studies have investigated the impact of the COVID-19 pandemic on low-income countries or the variables that elevate the propagation of the disease over space. Amaya and De Lombaerde (Citation2021) investigated the importance of regional organizations in addressing health threats in the Global South. They indicated that regional organizations can serve as a bridge between the global and national policy levels. Furthermore, these organizations can strengthen disease surveillance in this region as well as facilitate trade and mobilize the supply chain and support the production and procurement of medicines and supplies. Walker et al. (Citation2020) used various explanatory variables to examine the impact of the COVID-19 pandemic and the associated strategies for mitigation and suppression of the disease in low- and middle-income countries. They used disease severity, demography, health care quality and capacity, and contact patterns as explanatory variables to understand the factors that could cause a differential impact of the pandemic in these countries and to evaluate the potential policies and strategies for mitigation and suppression in these settings. They applied an infection fatality ratio and age-specific estimates of the rates of hospitalization and the proportion of these requiring critical care under the same level of medical care supplied during the epidemic in China, as well as under an initial assumption of a consistent underlying role of comorbidities. They expected a larger percentage of deaths to occur among people age forty and older and an increased mortality rate among the younger population due to lack of quality oxygen support. Hass and Arsanjani (Citation2021) analyzed the spatiotemporal patterns of the propagation of the pandemic over Europe as a region and Denmark as a country. They used different explanatory variables in their investigation, including regional infection rates, temperature and air pollution data, and points of interest. They applied different spatial and statistical methods such as geographically weighted regression, ordinary least squares, random forest, and applied geospatial methods (e.g., spatial autocorrelation, space–time autocorrelation) for investigating the relationship between the explanatory variables and the propagation of the pandemic in Europe and Denmark. They found that pollution levels, amenities such as bars and cafes, and population density were the most influential explanatory variables. Tribby and Hartmann (2021) investigated the relationship between different outdoor built environment characteristics and the infection rate in New York City. In their analysis, they used ZIP code tabulation data and found a positive significant correlation between the infection rate and ethnicity, the average number of people per household, and age (population over age sixty-five). Furthermore, they found a negative correlation between the infection rate and population density, percentage of sidewalks, and using public transit to travel to work.
Population movement restrictions have been globally considered as a crucial and conventional basis for fighting COVID-19 transmission. To the best of our knowledge, however, no adequate assessments of such policies have yet been conducted, particularly across the Global South. Consequently, this research aims to develop an index based on geographic information systems (GIS) that evaluates the effectiveness of population mobility restrictions in mitigating infection rates. Moreover, the developed index seeks to explain the extent to which human mobility restrictions contributed to the mitigation of infection rates across developing countries. Achieving this aim serves to address a significant gap in the existing literature of global policymaking relevant to COVID-19, in particular how certain policies have so far been successful in the prevention of the persistence of the virus in human populations in each country.
Data Set
To reduce pandemic disease prevalence, several governmental policies have been imposed in most of the Global South countries, specifically quarantines, social distancing, and population movement restrictions. The Global COVID-19 Stringency Index was published and updated by a research group from the University of Oxford (Roser et al. Citation2020). In addition, Google has provided a data set on a national scale regarding mobility trends, which measures changes in population movements during the pandemic outbreak in each country. The detected changes specifically measure the percentage of visitors to particular location categories, such as pharmacies, grocery stores, national parks, and public transportation stations (). To construct the composite index of imposing the stringent polices, six different restriction parameters were considered in the analysis; restrictions on work places, parks and outdoor activities, public transport, self-quarantine, grocery and pharmacy, and retail and recreation. These restrictions are compared to a baseline day (the median value from the five-week period between 3 January and 6 February 2020).
Table 1 Category measure
Methods
Analytical Hierarchical Process
To obtain the relative weights of the index criteria, the methodology of analytical hierarchical process (AHP) was incorporated through two essential phases: selection of the index criteria and standardization, and criteria weighting.
Criteria Generation and Standardization. At this stage, the final selection of parameters was undertaken and a spatial database was developed to include all statistical variables of restrictions. The spatial layer of the countries of the Global South was projected in ArcGIS software (Version 10.3, Esri, Redlands, CA, USA). Six different restriction variables that measured population movements during June 2020 were chosen in the analysis. Employing the AHP method is undertaken to generate and assign weights for each parameter, and this requires standardizing all criteria that are included in the analysis. Standardization makes all criteria constant and in the same format of measurement units. This technique imposes a standard normal distribution on each criterion and therefore has a mean of zero and a standard deviation of one. The formula for calculation is as follows:
where
is the mean value and σ is the standard deviation, and thus all indicators are converted into a common scale in which they are assumed to have a normal distribution.
Determination of Weights Using AHP. Once the rating of professionals and experts on stringency parameters affecting COVID-19 infection reduction is performed, the AHP method (Saaty Citation1980) is applied to illustrate the prioritization of the given criteria. This technique provides a vigorous basis for computing the comparison of targeted criteria (Handfield et al. Citation2002; R. Singh, Khilwani, and Tiwari Citation2007; Saaty Citation2008). According to AHP, criteria weights are yielded through conducting pairwise comparisons of rated factors with a view to establishing a matrix of criteria importance. To determine the relative importance of each criterion, four experts and a professional from the health, sociology, economy, and geography fields were asked to compare the criteria on a pairwise basis. To obtain fair weights, the professionals compared all criteria in pairs using a scale of one to nine. In addition, the pairwise comparison was made specifically to evaluate to what extent changes in a restriction factor (e.g., workplaces) were more influential than another factor (e.g., parks and outdoor spaces) on COVID-19 prevalence. The latter, in turn, yields a more precise ranking of factors ordered according to their significance for disease transmission mitigation. The normalization of the paired matrix provides the importance attached to each factor. The design of the pairwise comparison matrix is sustainably carried out using a scale of one to nine, where one signifies equal importance and nine indicates extreme importance of two criteria. The matrix format in the pairwise comparisons defines as follows:
where 1 indicates a rating value for factor or criterion 1. After generating all pairwise comparison matrices, the vector of weights,
is calculated following Satty’s eigenvector method. This is followed by two steps to calculate weights: The first is normalizing the pairwise comparison matrix
based on the following equation:
for all j = 1, 2, …, n.
Second, the weight for each criterion is calculated as follows:
for all i = 1, 2, …, n.
In the pairwise comparison matrix, n denotes the number of elements (Mikhailov Citation2003). One of the strengths of the AHP method is gauging the decision-makers’ inconsistencies by computing the consistency relationship (CR), which should be less than or equal to 0.1, using the following formula:
CR stands for the degree of consistency or inconsistency (Scholl et al. Citation2005). It signifies the probability that the matrix judgments were made randomly (Saaty Citation1977). The CR depends on the consistency index (CI) and random index (RI) and can be calculated as follows:
where
(allowing for deviations owing to the large numbers) is the largest eigenvalue of the matrix, and n specifies the order of the matrix. RI represents the average of the resulting consistency index depending on the order of the matrix (Saaty Citation1977). If the CR value is less than 0.10, then the pairwise consistency is fairly acceptable. On the contrary, if the value is larger than 0.10, this indicates inconsistencies in the evaluation and hence the original weights should be recalculated.
Calculation of Stringency Index
In the simplest form, assume that a composite index takes a linear form as follows:
where c1 refers to criterion 1 and w1 indicates the generated weight of criterion 1.
Results
The Spatial Distribution of Public Responses to Lockdown Policies
The spatial comparison of the impacts of the population responses to the restriction policies on the number of infected cases in the Global South countries is shown in . The responses to the implemented lockdown policies had a considerable positive effect on reducing the number of COVID-19 cases in these countries compared to the assessment period. These effects vary between the countries in the study area, however. The findings of this study revealed that there was a fundamental association between the number of COVID-19 cases and compliance with the imposed investigated mitigation policies, except for self-quarantine. In general, countries in Latin America, the Middle East, and East and Southeast Asia are witnessing the highest reduction in the total number of visitors to workplaces, parks and outdoor places, public transport stations, grocery and pharmacy stores, and retail and recreation centers. Consequently, imposing these policies resulted in a substantial decline of COVID-19 cases.
Figure 1 Change in the percentage of visitors after the COVID-19 pandemic, compared to a baseline day (the median value from the five-week period between 3 January and 6 February 2020): (A) workplaces; (B) parks and outdoor spaces; (C) public transport stations.
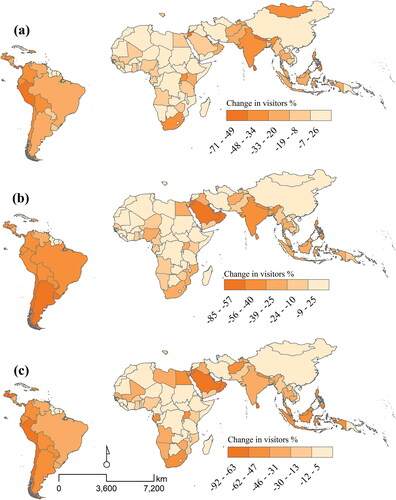
shows the population’s response to visiting the workplace after the imposition of the restrictions on workplace accessibility, with the aim of reducing the number of COVID-19 cases. This indicator reflects the real time of the state of the labor market in the Global South countries. shows that there are spatial variations between populations’ responses in many countries. The percentage of visitors to workplaces dropped significantly in some countries but increased in others compared to the baseline period. This reflects the stringency of imposing such a policy and its effectiveness in reducing the percentage of workers who move to work during the restriction. This variation can be explained by the fact that people in the countries that are witnessing a high number of infected cases are reducing their visits significantly and the level of the policy’s stringency is high. These countries are mainly in Latin America and South and Southeast Asia. On the other hand, countries such as China witnessed a low number of cases at the time of measuring this policy, and hence the country had opened its workplaces, with the percentage of visitors increasing compared to the assessment period.
Furthermore, many countries tended to close their parks and outdoor spaces to prevent the transmission of the disease through people gathering, socializing, or performing group activities. shows that almost all countries in the Global South enforced this policy, resulting in a reduction of the percentage of visitors to these areas; however, there are variations between these countries in terms of the compliance with the imposed policy, and the range varies between a 25 percent increase and an 85 percent decrease in the number of visitors to these areas. The highest response is in countries that are witnessing a high number of cases, such as those in Latin America, the Middle East, Southeast Asia, and India.
Public transport stations play a crucial role in the dissemination of the pandemic due to the fact that people are confined in limited spaces. Traveling on crowded modes of public transportation increases the risk of spreading COVID-19. Furthermore, many developing countries might have difficulties identifying passengers who could be sick, thus increasing the probability of the infection rate rising. Therefore, many countries have imposed restrictions on using public transport stations and public transport modes to reduce and eliminate the risk associated with using these services. Such restrictions have resulted in a significant decrease in the percentage of people who use public transport stations, as shown in . Although the variation is large between these countries, imposing this policy has led to a reduction in the percentage of visitors in many countries in the Global South compared to the assessment period. shows that this policy is more effective in countries in Latin America, the Middle East, Southeast Asia, and some countries in Africa. Conversely, certain countries in Asia and Africa have not imposed stringent policies and restrictions on the use of public transport stations, which might increase the likelihood of infection. The variation in peoples’ responses between these countries could be explained by the differences in the prevalence of COVID-19 in their communities and the stringency of imposing these policies.
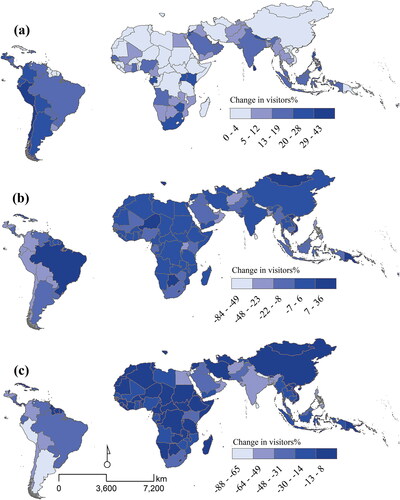
To slow the spread of the disease, many countries in the Global South promoted a stay-at-home policy. This policy restricted movements of individuals within their area of residency or across the nation and hence reduced their exposure to COVID-19 by avoiding social contact or reducing distances traveled. The extent to which this policy altered individuals’ mobility has varied across these countries, however. shows that this policy was not effective in increasing the percentage of people who stayed at home to eliminate the spread of the disease in these countries. also shows, however, that there is a spatial variation in imposing this mitigation procedure and consequently in the number of cases. It also demonstrates that the percentage of people who left their homes increased compared to the assessment period, particularly in the most infected countries, such as those in Latin America, Southeast Asia, and the Middle East. Consequently, this might have increased the number of cases, particularly in countries witnessing a high number of infections, such as in Latin America, the Middle East, India, and South Africa. Exceptions were made, however, for residents to meet their essential needs (e.g., food shopping or obtaining medical supplies) and outdoor physical activity. shows that the percentage of people who commute from their place of residency to groceries and pharmacies increased in many countries in the Global South, despite the restriction policies. This movement is significant in many countries with a high rate of cases, such as Brazil, India, and Iran. On the other hand, the restrictions imposed on retail and recreation activities (including restaurants, cafes, shopping centers, theme parks, museums, libraries, and movie theaters) were successful in reducing the percentage of visitors in many countries, as shown in . Some countries, though, witnessed an increased percentage of visitors compared to the assessment period, such as China and some countries in Africa.
Figure 2 Change in the percentage of visitors and duration spent at home after the COVID-19 pandemic compared to a baseline day (the median value from the five-week period between 3 January and 6 February 2020): (A) change in average duration spent in places of residence; (B) grocery and pharmacy stores; (C) retail and recreation (including restaurants, cafes, shopping centers, theme parks, museums, libraries, and movie theaters).
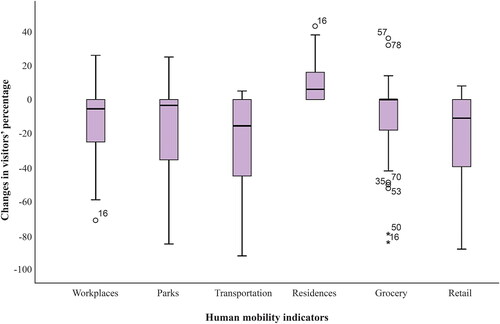
People’s response to these policies is not heterogeneous, as shown in , and varies across countries. The accessibility to workplace restriction policy significantly reduced the percentage of visitors to these places. shows that around 75 percent of visitors had their mobility to their workplaces reduced due to the imposition of this policy, with a median of less than zero. This illustrates that there were devastating effects on workers and enterprises in this region. About 25 percent (third quartile) of the visitors slightly reduced their visits to the workplace due to the imposition of this policy, however. In contrast, the percentage of workplace visitors in some countries increased compared to the assessment period. This can be explained by either the fact that the disease began to be confined, such as in China, or the enforcement of this policy was low. The same applies to the restrictions imposed on the accessibility of parks and open spaces, where around 75 percent of the visitors reduced their visits with a median less than zero. , however, shows that 25 percent of visitors slightly reduced their trips to these areas. There is a high variation between countries in the reduction of the percentage of visitors. The lockdown on the accessibility of public transport stations also resulted in a reduction in the percentage of visitors to these stations, compared with the assessment period; however, the variation is different between countries and with other policies, as shown in . Approximately 75 percent of visitors to public transport stations reduced their trips to these stations in the Global South countries. The other 25 percent of visitors slightly increased their trips to public transport stations. The stay-at-home policy was not successful in reducing the number of people who left their houses compared with the assessment period. shows that despite this policy, there was a slight increase in the percentage of people leaving their houses in almost all countries. People need to leave their houses to meet their basic needs, and this is reflected with around 50 percent of visitors increasing their visits to grocery stores and pharmacies compared to the assessment period. Furthermore, some countries allowed their citizens to visit retail and recreation locations (including restaurants, cafes, shopping centers, theme parks, museums, libraries, and movie theaters), which increased the number of people leaving their houses. shows that around 25 percent of people increased their visits to these places.
Figure 3 Box plots of the six stringent variables.
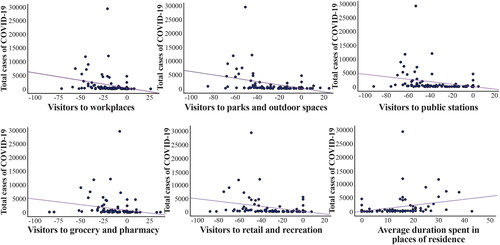
The relationship between the population’s response to these policies and the number of cases is shown in . Imposing these policies and people’s obedience resulted in reducing the number of COVID-19 cases. Imposing restrictions on accessing the workplace, parks and open spaces, public transport stations, grocery and pharmacy stores, retail and recreation places, and people’s positive response to these policies resulted in a decrease in the number of cases compared with the assessment period. On the contrary, imposing the stay-at-home policy and people’s negative response toward it resulted in a direct relationship and hence increased the number of cases.
Figure 4 Scatterplots of the relationships between the stringent variables and total cases of COVID-19 in the Global South countries.
The Effects of Stringency Measures on Infection Rate
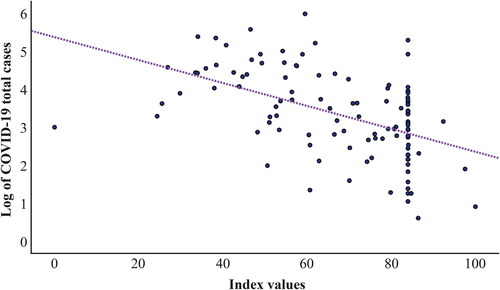
This study tracks people’s response to government policies in the Global South across a series of indicators and creates a suite of composite indexes to measure the variation of these responses across said countries. shows the index of population responses to restriction policies during the COVID-19 pandemic in the Global South countries compared to the assessment period. The index demonstrates that there is a significant variation in people’s responses to these policies across countries. In general, shows that people’s responses in countries in Latin America, the Middle East, and South Asia are the highest. Conversely, with regard to other countries, particularly in Africa, people’s responses to these policies are weak and hence could increase the number of cases. shows that there is a statistically negative correlation between the index value and the number of cases. It also illustrates that the number of cases decreases as the value of the index increases.
Figure 5 Index of population responses to stringent polices during COVID-19 pandemic in the Global South countries.
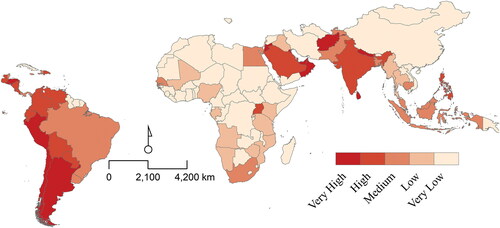
Figure 6 Pearson correlation between the index values and log of total COVID-19 cases in the Global South.
Discussion
The rapid propagation of the COVID-19 pandemic has forced governments to impose a wide range of policies to mitigate the spread of the disease. Implementing containment measures to slow the spread of the disease, protect people’s lives, and support public health has become the highest priority for countries across the globe. Governments in the Global South countries, however, have varied substantially in the methods and rules of imposing these policies, and hence there has also been variation in the people’s responses, thus affecting the propagation of the disease. This study has modeled the effectiveness of lockdown policies in reducing COVID-19 cases in the Global South countries through investigating the variation of people’s responses to these policies. Six lockdown policies were considered and analyzed to illustrate how they resulted in a decrease or increase in the number of incidents. These policies were combined to form an overall government response and stringency index to measure the extent of the people’s responses to the restriction polices during the COVID-19 pandemic in the Global South countries. People’s responses to COVID-19 mitigation policies exhibit significant variation in this area. The aforementioned might be due to the degree of the stringency of imposing these policies in each country and be contingent on local political and social contexts. The results show that people from different countries in Latin America, South Asia, the Gulf Cooperation Council, and Jordan have the highest values of the index, which indicates that the people of these countries have the highest positive response to said policies. The number of incidents in many of these countries is high, however (i.e., Brazil, India, Peru, Chile, Pakistan, Saudi Arabia), which implies that more stringent policies must be applied to eliminate the spread of the disease.
Accessibility to the workplace is restricted by many countries to avoid the transmission of the disease. In Global South countries, implementing this policy has led to a reduction in the percentage of visitors to the workplace in most countries but at different levels. The most affected regions are Latin America and South Asia (i.e., India, Nepal, Mongolia, and Pakistan), in addition to other countries such as South Africa, Jordan, and Kuwait. Imposing this policy resulted in eliminating the transmission of the disease and reducing the number of cases. This policy, however, has negative consequences for workers, particularly informal workers, and businesses, leaving them at high risk of insolvency. As a result, the fragile economy of many of the Global South countries will be worsened and more people will be at risk. Furthermore, these countries will face difficulties in protecting workers and enterprises. Effective and strong employment policies and enterprise measures need to be developed to support businesses and jobs to mitigate the economic and social consequences of the confinement period. This support can be achieved by decisive coordination and collaboration with international organizations and communities, particularly richer countries, on stimulus packages and debt relief measures. These policies associated with international collaboration are critical in making recovery more effective and sustainable.
Visiting parks and outdoor spaces is important, particularly in urban areas, for physical and mental health and social well-being. Accessibility restrictions on parks and outdoor spaces aim to reduce the risk of transmission of the disease in outdoor environments through aerosols, humidity, or wind, as well as other human factors such as crowding and social gathering (van Doremalen et al. Citation2020; Walker Citation2020). Many countries in the Global South have imposed restrictions on visiting parks and open spaces. These restrictions have been effective in reducing the number of visitors to said areas, hence eliminating the transmission of the disease through environmental or human factors. The results of the study show, however, that compliance with and the effectiveness of this policy vary across countries. Latin American, Southeast Asian, and Middle Eastern countries have witnessed the greatest reduction in visitors to parks and open spaces compared with the assessment period. Imposing this policy has resulted in reducing the number of cases. In contrast, closing parks and open spaces might be undesirable for the community and residents due to the negative impact on mental health, health inequities, overall health benefits, and the potential of riskier alternatives caused by the pandemic.
Public transport systems are the backbone of cities and are central in amplifying and accelerating the spread of a pandemic such as COVID-19 across the city or between cities. These systems have high crowd densities and enclosed spaces that provide ideal conditions for human-to-human transmission. Therefore, many countries responded to the spread of the disease with travel-related controls, including closing public transport stations with the aim of limiting or constraining human mobility to contain or slow down the spread of the disease. In the Global South countries, implementing this policy significantly reduced the percentage of travelers who use this mode of transportation in many countries. The stringency of implementing the policy and the people’s response vary between countries in this region. As the disease is spreading in many countries in Latin America, the Middle East, and Southeast Asia, these countries have witnessed the highest response from travelers by reducing their utilization of the public transport stations. Implementing this policy was significant in reducing the number of cases in these countries compared to other countries in the Global South.
Change in the average duration spent in places of residence is another measure taken by many countries to mitigate the transmission of the disease between people. Some countries issued a stay-at-home policy in response to the rising infection rate and death toll of the COVID-19 pandemic, with the aim of reducing the number of cases. Furthermore, closing many locations, including workplaces and recreation facilities, forced people to stay at their places of residence for a longer period of time. The results of this study, however, showed that despite imposition of this policy in many countries in the Global South, the percentage of people leaving their places of residency increased compared with the assessment period and consequently resulted in an increase in cases. This can be attributed to different reasons. First, people have to leave their place of residency for basic needs related to food and services. Second, the stringency of implementing this policy varies between countries in the Global South; the variation can be explained by the stringency of applying restrictions on the accessibility of work places and the closure of recreation amenities and facilities. This increases the probability of human-to-human disease transmission.
The advantage of this study is that it evaluates the stringency of imposing different policies and people’s responses to these policies in Global South countries; thus, the results reflect how the policies and responses affect the number of cases. Furthermore, this study developed an overall government response and stringency index to investigate the variation between countries in the stringency of imposing these policies and people’s responses. This index combined six policy measures imposed by the countries to mitigate the spread of the pandemic. It brings both strengths and limitations to this study. Using this index allows cross-national measures for systematic comparison across countries. Furthermore, this indicator makes it possible for governments to assess the containment policies and people’s response at a point in a country’s infection trajectory to implement more or less stringent policies. In addition, by considering and measuring a range of indicators, the probability that any single indicator might be over- or misinterpreted will be limited and mitigated. On the other hand, there are some limitations of using this approach. Using an index leaves out important information and makes strong assumptions about what kind of information counts. In addition, a composite index could introduce measurement bias if the information left out is systematically under- or overvalued compared to other indicators or is systematically correlated with the outcomes of interest. In addition, this research is limited to the absence of detailed and ancillary data at a subnational scale in each country of the Global South. Likewise, the AHP method, which has been used to assign criteria weights, is predominantly for probability measures and relies more on human judgment alternatives. To the best of our knowledge, however, this study is the first attempt to develop a quantitative index that could be used to assess the effectiveness of the human mobility restrictions on disease transmission mitigation across the Global South.
This study emphasizes the importance of geographic space in studying the propagation of the COVID-19 pandemic. The unevenness of the spatial propagation of the virus raises several questions about how the geography of the propagation of the disease might increase the infection and mortality rates across the globe. This analysis is of paramount importance for different reasons. First, identifying the factors that could increase the propagation and mortality rate of the disease in the Global South countries might help national policymakers and the international community in the definition of containment measures and the appropriate means of aid to help these countries to reduce the rate of infected and mortality cases. Second, identifying the most affected countries with limited health care facilities and infrastructure as well as a high rate of comorbidities could create collaboration between the national community and the international organizations in developing plans not only to mitigate and reduce the infection and mortality rate but also to develop plans of containment measures for these comorbidities. Finally, future geographical academic investigations of the impact of COVID-19 in the Global South countries should take into consideration the socioeconomic characteristics of each country for a more accurate assessment.
Conclusion
Despite the fact that the virus is still prevailing in many countries and lockdowns are still being implemented to control the propagation of the disease, governments have started facing the hard choice between reviving the economy and preserving public safety. This is particularly prominent in countries with vulnerable communities bearing the brunt of the health losses that lack the requisite capacities to economically balance the effects of the lockdown. Therefore, many countries in the Global South are reopening their economies after months of lockdown measures, which might have negative epidemiological and socioeconomic effects in the short and medium terms. Many of these countries have announced that the reopening will be gradual and will be based on different phases before reaching full functioning of their economies and societies. Furthermore, these countries are imposing personal protection measures: wearing masks in public; widespread COVID-19 testing; investing in personal protective equipment, hygiene, and cleansing products: and contact tracing of those who are infected. The reopening is associated with key elements including business continuity measures and building the resilience of people and business toward shifting to a new paradigm that includes safe coexistence with the virus.
Along with the main aim, this research has posed two central research objectives: first, to develop a quantitative index using AHP and the GIS-based approach for effective measurement of disease infection mitigation and, second, using the index to assess spatial variations of the effectiveness of human mobility restriction on mitigation of the COVID-19 infection rate across the Global South. The findings indicated that various human mobility restrictions, such as those on public travel and outdoor space gathering, in particular, were clearly successful in mitigating the spread of local transmission of COVID-19, whereas others were less successful. Governments initiated different policies in response to the propagation of the COVID-19 pandemic to mitigate its effect and reduce the number of cases. Therefore, it is imperative to model which existing measures are effective and which are not. The index developed in this study can serve as useful input for studies that analyze factors affecting disease progression. This study seeks to contribute to COVID-19 pandemic mitigating measures by providing comparable measures of different policies, as well as an aggregated index for Global South countries. There is significant variation in the stringency of imposing these measures, as well as in people’s response to such measures in the Global South countries.
Geographers can play a notable role in identifying the spatial distribution and propagation of the virus on the national and international levels and the associated factors that help in increasing or decreasing the infected and mortality rates. The spatial analysis includes spatial modeling and cartographic visualization of some factors that might increase the infection and mortality rates in Global South countries. Likewise, the spatial modeling and the cartographic visualization synthesis on the propagation of the COVID-19 pandemic in the Global South can aid international health organizations, international aid organizations, and the high-income countries in identifying low-income countries with high risks and with high infected and mortality rates and help low-income countries to mitigate the high risks of infection and mortality rates.
Acknowledgments
The authors thank the editor and anonymous reviewers for their insightful comments and suggestions.
Additional information
Notes on contributors
Ammar Abulibdeh
AMMAR ABULIBDEH is an Assistant Professor in the Department of Humanities, College of Arts and Science, Qatar University, Doha, Qatar. E-mail: [email protected]. His research focuses on smart urban planning and design, sustainable built environment, sustainable transportation, and the water–energy–food nexus.
Shawky Mansour
SHAWKY MANSOUR is Associate Professor of GIS in the Department of Geography and GIS, Faculty of Arts, Alexandria University, Egypt, and in the Geography Department, College of Arts and Social Sciences, Sultan Qaboos University, Muscat, Oman. E-mail: [email protected]. He is a specialist in GIS with particular interests in GIScience and spatial modeling. His research focuses on developing and utilizing advanced geospatial techniques to model and analyze the interrelationships between environmental, socioeconomic, and demographic phenomena.
Literature Cited
- Abulibdeh, A. 2020. Can COVID 19 mitigation measures promote telework practices? Journal of Labor and Society 23 (4):551–76. doi: https://doi.org/10.1111/wusa.12498.
- Abulibdeh, A. 2021. Spatiotemporal analysis of water-electricity consumption in the context of the COVID-19 pandemic across six socioeconomic sectors in Doha City, Qatar. Applied Energy 304:117864. doi: https://doi.org/10.1016/J.APENERGY.2021.117864.
- Ali, I., and O. M. Alharbi. 2020. COVID-19: Disease, management, treatment, and social impact. Science of the Total Environment 728:138861. doi: https://doi.org/10.1016/j.scitotenv.2020.138861.
- Amaya, A. B., and P. De Lombaerde. 2021. Regional cooperation is essential to combatting health emergencies in the Global South. Global Health 17: Art. 9. doi: https://doi.org/10.1186/s12992-021-00659-7.
- Anderson, R. M., H. Heesterbeek, D. Klinkenberg, and T. D. Hollingsworth. 2020. How will country-based mitigation measures influence the course of the COVID-19 epidemic? The Lancet 395 (10228):931–34. doi: https://doi.org/10.1016/S0140-6736(20)30567-5.
- Atumanya, P., C. Sendagire, A. Wabule, J. Mukisa, L. Ssemogerere, A. Kwizera, and P. K. Agaba. 2020. Assessment of the current capacity of intensive care units in Uganda: A descriptive study. Journal of Critical Care 55:95–99. doi: https://doi.org/10.1016/j.jcrc.2019.10.019.
- Bertuzzo, E., L. Mari, D. Pasetto, S. Miccoli, R. Casagrandi, M. Gatto, and A. Rinaldo. 2020. The geography of COVID-19 spread in Italy and implications for the relaxation of confinement measures. Nature Communications 11 (1):4264. doi: https://doi.org/10.1038/s41467-020-18050-2.
- Chintalapudi, N., G. Battineni, and F. Amenta. 2020. COVID-19 virus outbreak forecasting of registered and recovered cases after sixty day lockdown in Italy: A data driven model approach. Journal of Microbiology, Immunology, and Infection 53 (3):396–403. doi: https://doi.org/10.1016/j.jmii.2020.04.004.
- Chowdhury, A. Z., and K. S. Jomo. 2020. Responding to the COVID-19 pandemic in developing countries: Lessons from selected countries of the Global South. Development (Society for International Development) 63:1–171. doi: https://doi.org/10.1057/s41301-020-00256-y.
- Cowling, B. J., and A. E. Aiello. 2020. Public health measures to slow community spread of coronavirus disease 2019. The Journal of Infectious Diseases 221 (11):1749–51. doi: https://doi.org/10.1093/infdis/jiaa123.
- Dempster, H., T. Ginn, J. Graham, M. G. Ble, D. Jayasinghe, and B. Shorey. 2020. Locked down and left behind: The impact of COVID-19 on refugees’ economic inclusion. Policy Paper 179. Washington, DC: Center for Global Development and Refugees International. https://www.cgdev.org/publication/locked-down-and-left-behind-impact-covid-19-refugees-economic-inclusion.
- Depellegrin, D., M. Bastianini, A. Fadini, and S. Menegon. 2020. The effects of COVID-19 induced lockdown measures on maritime settings of a coastal region. Science of the Total Environment 740:140123. doi: https://doi.org/10.1016/j.scitotenv.2020.140123.
- Díaz de León-Martínez, L., L. de la Sierra-de la Vega, A. Palacios-Ramírez, M. Rodriguez-Aguilar, and R. Flores-Ramírez. 2020. Critical review of social, environmental and health risk factors in the Mexican indigenous population and their capacity to respond to COVID-19. Science of the Total Environment 733:139357. doi: https://doi.org/10.1016/j.scitotenv.2020.139357.
- Fadare, O. O., and E. D. Okoffo. 2020. Covid-19 face masks: A potential source of microplastic fibers in the environment. The Science of the Total Environment 737:140279. doi: https://doi.org/10.1016/j.scitotenv.2020.140279.
- Frost, I., J. Craig, G. Osena, S. Hauck, E. Kalanxhi, E. Schueller, O. Gatalo, Y. Yang, K. K. Tseng, G. Lin, et al. 2021. Modelling COVID-19 transmission in Africa: Countrywise projections of total and severe infections under different lockdown scenarios. BMJ Open 11 (3):e044149. doi: https://doi.org/10.1136/bmjopen-2020-044149.
- Ghisolfi, S., I. Almås, J. C. Sandefur, T. von Carnap, J. Heitner, and T. Bold. 2020. Predicted COVID-19 fatality rates based on age, sex, comorbidities and health system capacity. BMJ Global Health 5 (9):e003094. doi: https://doi.org/10.1136/bmjgh-2020-003094.
- Guérin, C., and P. Lévy. 2020. Easier access to mechanical ventilation worldwide: An urgent need for low income countries, especially in face of the growing COVID-19 crisis. European Respiratory Journal 55:2001271. doi: https://doi.org/10.1183/13993003.01271-2020. ].
- Handfield, R., S. V. Walton, R. Sroufe, and S. A. Melnyk. 2002. Applying environmental criteria to supplier assessment: A study in the application of the analytical hierarchy process. European Journal of Operational Research 141 (1):70–87. doi: https://doi.org/10.1016/S0377-2217(01)00261-2.
- Hass, F. S., and J. J. Arsanjani. 2021. The geography of the Covid-19 pandemic: A data-driven approach to exploring geographical driving forces. International Journal of Environmental Research and Public Health 18 (6):2803. doi: https://doi.org/10.3390/IJERPH18062803.
- Hellewell, J., S. Abbott, A. Gimma, N. I. Bosse, C. I. Jarvis, T. W. Russell, J. D. Munday, A. J. Kucharski, W. J. Edmunds, S. Funk, Centre for the Mathematical Modelling of Infectious Diseases COVID-19 Working Group, et al. 2020. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. The Lancet Global Health 8 (4):e488–96. doi: https://doi.org/10.1016/S2214-109X(20)30074-7.
- Hogan, A. B., B. L. Jewell, E. Sherrard-Smith, J. F. Vesga, O. J. Watson, C. Whittaker, A. Hamlet, J. A. Smith, P. Winskill, R. Verity, et al. 2020. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: A modelling study. The Lancet Global Health 8 (9):e1132–41. doi: https://doi.org/10.1016/S2214-109X(20)30288-6.
- International Labour Organization. 2020a. As job losses escalate, nearly half of global workforce at risk of losing livelihoods. ILO News, April 29. https://www.ilo.org/global/about-the-ilo/newsroom/news/WCMS_743036/lang–en/index.htm
- International Labour Organization. 2020b. COVID-19 and the world of work. https://www.ilo.org/global/topics/coronavirus/lang--en/index.htm.
- Khan, N., S. Fahad, M. Naushad, and S. Faisal. 2020. COVID-2019 locked down effects on oil prices and its effects on the world economy. https://doi.org/http://dx.doi.org/10.2139/ssrn.3588810
- Lai, H., Y. A. Khan, A. Thaljaoui, W. Chammam, and S. Z. Abbas. 2021. COVID-19 pandemic and unemployment rate: A hybrid unemployment rate prediction approach for developed and developing countries of Asia. Soft Computing. Advance online publication. doi: https://doi.org/10.1007/s00500-021-05871-6.
- Lin, Y.-H., C.-H. Liu, and Y.-C. Chiu. 2020. Google searches for the keywords of “wash hands” predict the speed of national spread of COVID-19 outbreak among 21 countries. Brain, Behavior, and Immunity 87:30–32. doi: https://doi.org/10.1016/j.bbi.2020.04.020.
- Mikhailov, L. 2003. Deriving priorities from fuzzy pairwise comparison judgements. Fuzzy Sets and Systems 134 (3):365–85. doi: https://doi.org/10.1016/S0165-0114(02)00383-4.
- Nicola, M., Z. Alsafi, C. Sohrabi, A. Kerwan, A. Al-Jabir, C. Iosifidis, M. Agha, and R. Agha. 2020. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. International Journal of Surgery 78:185–93. doi: https://doi.org/10.1016/j.ijsu.2020.04.018.
- Nikhat, S., and M. Fazil. 2020. Overview of COVID-19; its prevention and management in the light of Unani medicine. Science of the Total Environment 728:138859. doi: https://doi.org/10.1016/j.scitotenv.2020.138859.
- Qi, H., S. Xiao, R. Shi, M. P. Ward, Y. Chen, W. Tu, Q. Su, W. Wang, X. Wang, and Z. Zhang. 2020. COVID-19 transmission in mainland China is associated with temperature and humidity: A time-series analysis. The Science of the Total Environment 728:138778. doi: https://doi.org/10.1016/j.scitotenv.2020.138778.
- Rivera-Rodriguez, C., and B. P. Urdinola. 2020. Predicting hospital demand during the COVID-19 outbreak in Bogotá, Colombia. Frontiers in Public Health 8:582706. doi: https://doi.org/10.3389/fpubh.2020.582706.
- Roberton, T., E. D. Carter, V. B. Chou, A. R. Stegmuller, B. D. Jackson, Y. Tam, T. Sawadogo-Lewis, and N. Walker. 2020. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: A modelling study. The Lancet Global Health 8 (7):e901–8. doi: https://doi.org/10.1016/S2214-109X(20)30229-1.
- Roser, M., H. Ritchie, E. Ortiz-Ospina, and J. Hasell. 2020. Coronavirus pandemic (COVID-19). https://ourworldindata.org/coronavirus.
- Saaty, T. L. 1977. A scaling method for priorities in hierarchical structures. Journal of Mathematical Psychology 15 (3):234–81. doi: https://doi.org/10.1016/0022-2496(77)90033-5.
- Saaty, T. L. 1980. The analytical hierarchy process, planning, priority setting, resource allocation. (Decision Making Series). New York: McGraw-Hill.
- Saaty, T. L. 2008. Decision making with the analytic hierarchy process. International Journal of Services Sciences 1 (1):83–98. doi: https://doi.org/10.1504/IJSSCI.2008.017590.
- Salluh, J. I. F., T. Lisboa, and F. A. Bozza. 2020. Challenges for the care delivery for critically ill COVID-19 patients in developing countries: The Brazilian perspective. Critical Care 24 (1):593. doi: https://doi.org/10.1186/s13054-020-03278-7.
- Salye, J. S., J. Maeda, S. Sembuche, Y. Kebede, A. Tshangela, M. Moussif, C. Ihekweazu, N. Mayet, E. Abate, A. O. Ouma, et al. 2021. The first and second waves of the COVID-19 pandemic in Africa: A cross-sectional study. Lancet 397:1265–75. doi: https://doi.org/10.1016/S0140-6736(21)00632-2.
- Scholl, A., L. Manthey, R. Helm, and M. Steiner. 2005. Solving multiattribute design problems with analytic hierarchy process and conjoint analysis: An empirical comparison. European Journal of Operational Research 164 (3):760–77. doi: https://doi.org/10.1016/j.ejor.2004.01.026.
- Sen-Crowe, B., M. Sutherland, M. McKenney, and A. Elkbuli. 2021. A closer look into global hospital beds: Capacity and resource shortages during the COVID-19 pandemic. Journal of Surgical Research 260:56–63. doi: https://doi.org/10.1016/j.jss.2020.11.062.
- Shim, E., A. Tariq, W. Choi, Y. Lee, and G. Chowell. 2020. Transmission potential and severity of COVID-19 in South Korea. International Journal of Infectious Diseases 93:339–44. doi: https://doi.org/10.1016/j.ijid.2020.03.031.
- Singh, A. K., and A. Misra. 2020. Impact of COVID-19 and comorbidities on health and economics: Focus on developing countries and India. Diabetes & metabolic syndrome. Clinical Research & Reviews 14 (6):1625–30.
- Singh, R., N. Khilwani, and M. Tiwari. 2007. Justification for the selection of a reconfigurable manufacturing system: A fuzzy analytical hierarchy based approach. International Journal of Production Research 45 (14):3165–90. doi: https://doi.org/10.1080/00207540600844043.
- Tahir, M. B., and A. Batool. 2020. COVID-19: Healthy environmental impact for public safety and menaces oil market. Science of the Total Environment 740:140054. doi: https://doi.org/10.1016/j.scitotenv.2020.140054.
- Testa, A., M. Rennó Santos, and D. B. Weiss. 2020. Incarceration rates and hospital beds per capita: A cross-national study of 36 countries, 1971–2015. Social Science & Medicine 263:113262. doi: https://doi.org/10.1016/j.socscimed.2020.113262.
- Tobías, A. 2020. Evaluation of the lockdowns for the SARS-CoV-2 epidemic in Italy and Spain after one month follow up. Science of the Total Environment 725:138539. doi: https://doi.org/10.1016/j.scitotenv.2020.138539.
- Tyrrell, C. S. B., O. T. Mytton, S. V. Gentry, M. Thomas-Meyer, J. L. Y. Allen, A. A. Narula, B. McGrath, M. Lupton, J. Broadbent, A. Ahmed, et al. 2021. Managing intensive care admissions when there are not enough beds during the COVID-19 pandemic: A systematic review. Thorax 76 (3):302–12. doi: https://doi.org/10.1136/thoraxjnl-2020-215518.
- United Nations. 2020. Brief #2: Putting the UN framework for socio-economic response to COVID-19 into action: Insights. Brief Prepared by the United Nations Development Programme.
- van Doremalen, N., T. Bushmaker, D. H. Morris, M. G. Holbrook, A. Gamble, B. N. Williamson, A. Tamin, J. L. Harcourt, N. J. Thornburg, S. I. Gerber, et al. 2020. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. The New England Journal of Medicine 382 (16):1564–67. doi: https://doi.org/10.1056/NEJMc2004973.
- Verity, R., L. C. Okell, I. Dorigatti, P. Winskill, C. Whittaker, N. Imai, G. Cuomo-Dannenburg, H. Thompson, P. G. T. Walker, H. Fu, et al. 2020. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infectious Diseases 20 (6):669–77. doi: https://doi.org/10.1016/S1473-3099(20)30243-7.
- Walker, A. 2020. In the coronavirus crisis, who gets to be outside? Vox Media. Accessed March 30, 2020. https://www.curbed.com/2020/3/27/21191714/coronavirus-public-spacesparks-hiking-trails.
- Walker, P. G. T., C. Whittaker, O. J. Watson, M. Baguelin, P. Winskill, A. Hamlet, B. A. Djafaara, Z. Cucunuba, D. Olivera Mesa, W. Green, et al. 2021. The impact of COVID-19 and strategies for mitigation and suppression in low- and middle-income countries. Science 369 (6502): 413–22. Jul. doi: https://doi.org/10.1126/SCIENCE.ABC0035.
- Wang, C., P. W. Horby, F. G. Hayden, and G. F. Gao. 2020. A novel coronavirus outbreak of global health concern. The Lancet 395 (10223):470–73. doi: https://doi.org/10.1016/S0140-6736(20)30185-9.
- Wells, C. R., P. Sah, S. M. Moghadas, A. Pandey, A. Shoukat, Y. Wang, Z. Wang, L. A. Meyers, B. H. Singer, and A. P. Galvani. 2020. Impact of international travel and border control measures on the global spread of the novel 2019 coronavirus outbreak. Proceedings of the National Academy of Sciences of the United States of America 117 (13):7504–9. doi: https://doi.org/10.1073/pnas.2002616117.
- Zwama, G., K. Diaconu, A. S. Voce, F. O’May, A. D. Grant, and K. Kielmann. 2021. Health system influences on the implementation of tuberculosis infection prevention and control at health facilities in low-income and Middle- income countries: A scoping review. BMJ Global Health 6 (5):e004735. doi: https://doi.org/10.1136/bmjgh-2020-004735.