
Abstract
Background and Aims
The SARS-CoV-2 pandemic abruptly switched the healthcare service for patients with inflammatory bowel disease (IBD) towards a telemedicine dominated approach. The aim of this study was to investigate the impact of this switch on monitoring of patients and on disease activity.
Material
The pre-pandemic year included 868 patients and the first year of the pandemic included 891 patients. Medical records were retrospectively checked for contacts, changes in medical treatment, performed fecal calprotectin (FC) tests and colonoscopies.
Results
The scheduled follow-up visits to a doctor for patients with IBD shifted from mostly face-to-face pre-pandemic (from 389 to 118 appointments) to mostly telephone-based during the pandemic (from 13 to 423 appointments). There was a 21.3% increase in mean overall scheduled health contacts (p < .001) and a 20.0% increase for the mean number of FC tests (p < .001) in the year of the pandemic compared to the pre-pandemic year. The proportion of patients who had a surveillance colonoscopy was significant lower in the year of the pandemic compared to the pre-pandemic year (12.7% vs 20.1%; p = .002). There were no difference in the proportion of patients with a median FC > 200 mg/kg (18.2% vs 17.1%; p = .767) and in the proportion of patients who changed their medical treatment (24.7% vs 23.9%; p = .713) in the first year of the pandemic compared to the prepandemic year.
Conclusions
The shift towards a telemedicine oriented IBD healthcare service in the first year of the pandemic significantly increased the scheduled contacts, as well as the frequency of FC testing. However, there was a significant decrease in performed surveillance colonoscopies. Between the two periods observed, the patients showed no difference in medical treatment or in disease activity.
Introduction
At the end of 2019, patients emerged with pneumonia in Wuhan, China, caused by Severe Acute Respiratory Syndrome Corona Virus 2 (SARS-CoV-2) [Citation1]. The World Health Organization named the new disease Corona Virus Disease 2019 (COVID-19) [Citation2]. The first confirmed case in Sweden was on 28 January 2020 [Citation3] and Region Västerbotten in the Northern part of Sweden had its first case in February the same year [Citation4]. One year later, on 28 February 2021, Region Västerbotten had 14742 cases reported and 143 death [Citation4]. Although, in Sweden there was no complete lock down of the society during the pandemic, the Public Health Agency of Sweden and the Swedish government at different stages recommended restrictions on social distance, on events and on travel. For workplaces and schools the recommendation was that work tasks and teaching should be organized to be performed at home as much as possible.
For the healthcare services telemedicine has become a central part during the SARS-CoV-2 pandemic, allowing healthcare workers to reach patients in their homes [Citation5]. At the Department of Gastroenterology at the University Hospital of Umeå, the recommendation during the pandemic was to shift most of the out-patient visits to telephone visits.
Inflammatory bowel disease (IBD) includes two main chronic inflammatory bowel diseases: Ulcerative colitis (UC) and Crohn’s disease (CD) [Citation6]. UC and CD are lifelong conditions often requiring continuous treatment and frequent monitoring of disease activity [Citation7,Citation8]. In 2010 the prevalence of IBD in Sweden estimated to 0.65% [Citation9]. At our hospital, the care of patients with IBD in general includes annual, planned, follow-ups in combination with on demand services available from a IBD team consisting of IBD nurses. The patients are encouraged to contact a IBD team in suspicion of a flare of disease, or for other issues. Patients with colonic disease (mostly patients with UC) have scheduled colonoscopy controls to check for dysplasia, with start approximately ten years after onset of disease [Citation8]. Colonoscopy is also performed in patients with IBD to evaluate disease activity. Faecal calprotectin (FC) levels correlate with disease activity and is a predictor of relapse [Citation8,Citation10]. It is measured periodically during the planned follow-ups, or whenever symptoms of relapse occur. Except for shifting physical visits to telephone visits as mentioned above no other change in the organization of patients with IBD was done.
Acute and chronic stress may affect IBD disease activity [Citation7,Citation11,Citation12]. For example, a study showed an increase frequency of disease relapse in IBD patients following the Great East Japan earthquake of March 2011 [Citation13]. However, it is not known how the stress during a pandemic impacts the disease activity. In addition to general stress of the direct and indirect consequences of the pandemic, patients with IBD may worry about how SARS-CoV-2 may affect the disease behavior and the treatment of IBD. Furthermore, due to fear being infected by SARS-CoV-2, patients may have been at risk of avoiding scheduled appointments and planned investigations.
The primary aim of this study was to investigate the impact of the SARS-CoV-2 outbreak on the care of patients with IBD. Secondary aims were to explore if disease activity and changes in medical treatment differed in the year of the pandemic compared to the year before the pandemic. Finally, we explored to what extent patients with IBD had performed testing for SARS-CoV-2.
Methods
Study design
This was a retrospective observational study performed at the Department of Gastroenterology at the University Hospital of Umeå. All patients 18 years and older registered with ICD codes K50.0-9 (CD) or K51.0-9 (UC) any time between 2015 and 2021 and living in the catchment area of Umeå University Hospital were reviewed for the inclusion criteria. A review of the medical records from the Department of Medicine and Surgery was performed to confirm the diagnosis. In the analysis only patients living in the catchment area throughout the whole observed period (First of March 2019 to 28 February 2021) were included. Patients were excluded if colectomized due to UC or deceased before First of March 2019. The pre-pandemic period was set to be First of March 2019 to 29 February 2020. The time between First of March 2020 to 28 February 2021 was defined as the first year of the pandemic.
Data collection from medical records
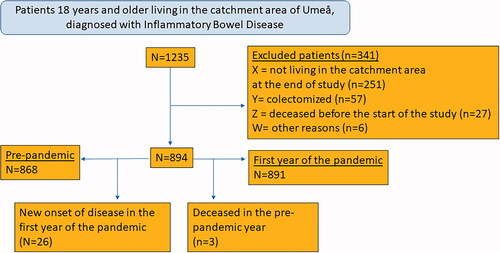
Out of 1235 patients registered with UC or CD, 341 patients were removed due to exclusion criteria, leaving 894 patients suitable for the study (). In addition, patients who deceased (N = 3) in the year pre-pandemic were excluded from the second period and patients with new onset of disease (N = 26) emerging during the first year of the pandemic were excluded from the first period (). Basal data collected from the medical records was age, gender, IBD type according to the Montreal classification [Citation14], years since diagnosis and medical treatment during the observed period.
Figure 1. Flow chart that shows the patients included in the pre-pandemic period and the period of the first year of the COVID-19 pandemic.
The healthcare interactions with patients were analyzed using the following parameters: standard, planned face-to-face-appointments, planned telephone appointments and unplanned telephone contacts with doctor (including patient letters and e-mails, with requirement of a doctor’s intervention), unplanned telephone contacts with nurse and planned face-to-face contacts with nurse (medical infusion appointments included). In addition, the number of colonoscopies, surveillance colonoscopies and cancelled colonoscopies was registered.
The number of FC tests per patient were noted. Furthermore, we collected a patient median FC value during each year for patients tested. The CALPRO method is used for FC analysis at the University Hospital of Umeå. Changes in medical treatment were observed. Increased treatment was defined as prescribing a new drug or increase dosage of an already used drug. Treatment reduction was defined as stopped or reduced dosage of a used drug. Patients with a new onset of disease was noted. Also, we registered the time in days from first visit in primary care to referral and from referral to diagnosis. The date of diagnosis was set at the first endoscopy or bowel imaging confirming signs of IBD.
Tests for SARS-CoV-2
To evaluate the frequency of SARS-CoV-2 testing, the number of tests and positive results were collected. For the patients with IBD data on SARS-CoV-2 testing was collected from the medical records. Positive tests for the whole population living in the catchment area of Umeå were collected from the webpage of the public health authority of Sweden [Citation4]. In addition, we compared the total number of tests performed in the IBD patients with the data from the entire Region Västerbotten (the numbers were only available from the entire region). Self-based test for SARS-CoV-2 available for commercial use was not included. The vaccination for SARS-CoV-2 infection in our region did not start until after the observation period had ended.
Statistical analysis
Statistical Package for the Social Sciences (SPSS) version 27.0 were used. The parametric and nonparametric quantitative data were analyzed using the Student t-test and Mann–Whitney test, respectively. Chi-squared test were used for the categorical data and were expressed in frequencies and percentages. Continuous variables were expressed as mean with standard deviation or than appropriate as median with interquartile range. p values < .05 were considered statistically significant.
Ethical statement
The study was conducted in accordance with the Swedish law for Patient Safety and the Swedish Data Protection Authority’s rules. No interventions were done. The national ethical review board considered the study to be judged as a Patient Safety report and not as research.
Results
Basal characteristics
Basal characteristics of the patients included in the survey is shown in . The use of immunomodulators (49.0% vs 22.9%; p = <.001), anti-TNF (24.8% vs 10.3%; p = <.001) was significantly more common among the patients with CD and the use of 5-ASA (85.1% vs 24.2%; p = <.001) was significantly more common in the patients with UC.
Table 1. Basal characteristics of patients with Inflammatory Bowel Disease treated at Umeå University Hospital First of Mars 2019- 28th February 2021.
Provided healthcare during the SARS-CoV-2 outbreak
The scheduled follow-ups with doctor shifted from mostly face-to-face pre-pandemic (from 388 to 118 appointments) to mostly telephone-based during the pandemic (from 13 to 423 appointments). In the first year of the pandemic the median number of planed follow-ups with doctor or nurse per patient significantly increased, as well as telephone contacts with nurse (). There was a 21.3% increase in mean overall scheduled health contacts (p < .001) and a 20.0% increase for the mean number of FC tests (p < .001) in the year of the pandemic compared to the pre-pandemic year. The proportion of patients who had a surveillance colonoscopy was significant lower in the year of the pandemic compared to the pre-pandemic year (12.7% vs 20.1%; p = .002) but the proportion of activity control colonoscopies maintained the same level. There was no change in proportion of patients cancelling their colonoscopy.
Table 2. Healthcare interactions, change in medical treatment and new diagnoses during the pre-pandemic and first year of the SARS-2-CoV pandemic.
Monitoring with faecal calprotectin and intervention in medical treatment
The proportion of patients performing a FC test increased significantly the first year of the pandemic compared to the pre-pandemic period (). In addition, the mean value of number of FC tests taken per patient significantly increased. The median of each patients median FC value decreased, significant only in patients with UC. However, between the two periods observed, there was no difference in the proportion of patients with a FC > 200 mg/kg (). Furthermore, the proportion of patients who had increased or decreased medical therapy did not differ between the observed periods ().
Table 3. The number of tests and outcome of fecal calprotectin test during the pre-pandemic and the first year of the SARS-CoV-2 pandemic.
New diagnosis of IBD
The proportion of patients with new onset of disease did not decrease significantly the first year of the pandemic (). The number of days from first contact with primary care to referral decreased during the first year of the pandemic, but the difference was not significant (median 22 days; 25th–75th percentile 6–56 days vs median 12 days; 25th–75th percentile 1–21 days; p = .07). Furthermore, there were no differences in the time from referral to diagnoses (median 17 days; 25th–75th percentile 9–65 days vs median 24 days; 25th–75th percentile 7–100 days; p = .766) nor in the total time from first contact with primary care to diagnosis (median 56 days; 25th–75th percentile 34–131 days vs median 55 days; 25th–75th percentile 21–114 days; p = .511).
Patients with IBD and SARS-CoV-2 testing
In total 53.3% of patients with IBD performed at least one SARS-CoV-2 test between First of March 2020 to 28 February 2021. The IBD patients had in total 1035 tests taken. The proportion of patients with IBD and a positive SARS-CoV-2 test did not differ from the reference population (3.4% vs 3.9%; p = .373). No patient with IBD deceased due to SARS-CoV-2 infection.
Discussion
The rapid progression of the SARS-CoV-2 pandemic has challenged the healthcare systems world-wide. This observational study focused on the care of patients with IBD in Region Västerbotten in Northern Sweden. The prominent shift towards telephone-based care at the start of the pandemic, gave us a unique possibility to compare standard care to a care more based on distance consultations.
In our IBD population there was a minor but significant increase in the number of health-care interactions during the pandemic. The increase was approximately 21% in the mean number of planned contacts with a doctor or a nurse during the year of the pandemic. A possible cause for increased number of contacts seen in the first year of the pandemic could be that the time used for consultation in some cases could be shortened when scheduled on telephone. In addition, the scheduled follow-up on telephone has the advantage of saving time for the patient, which could lead to fewer cancellations. The increased number of telephone contacts with nurse could partly be explained by the questions regarding uncertainties of the impact of concurrent medications on SARS-CoV-2 infection [Citation15].
Despite increased number of health care interactions for patients with IBD during the pandemic, the surveillance colonoscopies in UC patients decreased significantly. This is in line with other studies during the SARS-CoV-2 pandemic. For example, Alboraie et al. showed that during the pandemic, until September 2020, 99% out of the endoscopy units included in their study, from countries worldwide, had a decrease in elective endoscopy services [Citation16]. Another study showed that overall gastrointestinal endoscopies in France decreased by 91.2% in the end of March 2020 [Citation17]. The cause of the reduction in surveillance colonoscopy could be due to displacement effects due to reorganization of health care towards the care of patients with SARS-CoV 2 but could also partly be explained by that a patient canceled their colonoscopies due to fear of being virus infected at the hospital.
Interestingly, there was a 20% significant increase in the mean number of FC test per patient during the first year of the pandemic. This could presumably be explained by the increased number of planned follow-ups. Other explanations could be an increased awareness of disease, hypervigilance for gastrointestinal symptoms or an easier ability to perform the test during the quarantine. Interestingly the median FC value for all patients tested was reduced during the first year of the pandemic. However, the proportion of patients with a FC value above 200 mg/kg did not change during the pandemic, indicating that the threshold for a patient to test was lower during the pandemic.
We hypothesized that an increased psychosocial stress during the pandemic could worsen the patients with IBD disease activity. It is known that anxiety and depression negatively influence the course of IBD [Citation7,Citation11,Citation12,Citation18]. Further the earthquake in Japan in 2011 had a negative impact on IBD [Citation13]. However, in the first year of the pandemic we did not find any tendency of increased disease activity based on FC levels or activity on colonoscopy and no change in medical treatment compared to the pre-pandemic year. In addition, the number of patients with a new onset of disease did not change significantly in the first year of the pandemic. Instead, less exposure to environmental factors, increased perceived assurance and control over bowel function in the familiar milieu at home could perhaps have positive effects on disease activity.
The present study included all patients with IBD in the catchment area and therefore present data on the overall use of medical treatment for IBD and remission rates. It shows that immunomodulators is commonly used and used by a half of the patients with CD whereas biologics are only used by approximately 25% of the patients with CD and 10% of patients with UC. The study also shows that the proportion of patients with a FC level above 200 mg/kg with the CALPRO method were similar in patients with UC and CD, and that approximately one out of six (18%) of patients with IBD were above this level. There is still uncertainty what a realistic target (proportion of patients that is in clinical remission) by using modern IBD therapy is and whether a slightly elevated FC level could be accepted. However, the use of biologics at our clinic is perhaps lower than accurate and that there is a potential for getting more patients in clinical remission by increase the use of these drugs.
Our study showed that the proportion of patients with IBD and a positive SARS-CoV-2 test did not differ from the reference population. A study from India showed the same result [Citation19]. However, Attauabi et al. found the prevalence of SARS-CoV-2 in IBD patients to be significantly lower than in the background population (2.5% vs 3.7%) [Citation20]. One possible factor could be a lower threshold for testing. Another possibility are regional differences in the spread of SARS-CoV2 and testing capacity.
This study had some limitations. Firstly, the SARS-CoV-2 pandemic is still ongoing (in the fall of 2021) and using a longer observation period the healthcare of IBD as well the impact of disease activity may look different. The study only includes adult patients and perhaps the outcome in paedriatric patients would have been different. A strength in our survey is that all patients with IBD were included except those subjects who moved out from the catchment area, were colectomized or deceased. Furthermore, the two groups (pre-pandemic and pandemic) observed basically included the same patients.
In conclusion, the shift towards a telemedicine oriented IBD-healthcare service in the first year of the pandemic significantly increased the scheduled contacts, as well as the frequency of FC testing. There was an approximately increase of 21% in mean planned health contacts and a 20% increase for the mean number of FC tests in the year of the pandemic, but there was a significant decrease in performed surveillance colonoscopies. Despite these changes in IBD care between the pre-pandemic and pandemic year, the patients showed no difference in medical treatment or disease activity.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of Novel Coronavirus-infected pneumonia. N Engl J Med. 2020;382(13):1199–1207.
- World Health Organisation. Naming the coronavirus disease (COVID-19) and the virus that causes it. 2020; [cited 2021 Jan 28]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it.
- Spiteri G, Fielding J, Diercke M, et al. First cases of coronavirus disease 2019 (COVID-19) in the WHO European Region, 24 January to 21 February 2020. Euro Surveill. 2020;5(9):2000178.
- Folkhälsomyndigheten. Bekräftade fall i Sverige- daglig uppdatering; [cited 2021 Feb 02]. Available from: https://www.folkhalsomyndigheten.se/smittskydd-beredskap/utbrott/aktuella-utbrott/covid-19/statistik-och-analyser/bekraftade-fall-i-sverige/.
- Colbert GB, Venegas-Vera AV, Lerma EV. Utility of telemedicine in the COVID-19 era. Rev Cardiovasc Med. 2020;21(4):583–587.
- Abraham C, Cho JH. Inflammatory bowel disease. N Engl J Med. 2009;361(21):2066–2078.
- Mawdsley JE, Rampton DS. The role of psychological stress in inflammatory bowel disease. Neuroimmunomodulat. 2006;13(5–6):327–336.
- Lamb CA, Kennedy NA, Raine T, et al. British society of gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019;68(Suppl 3):s1–s106.
- Busch K, Ludvigsson JF, Ekstrom-Smedby K, et al. Nationwide prevalence of inflammatory bowel disease in Sweden: a population-based register study. Aliment Pharmacol Ther. 2014;39(1):57–68.
- Rokkas T, Portincasa P, Koutroubakis IE. Fecal calprotectin in assessing inflammatory bowel disease endoscopic activity: a diagnostic accuracy meta-analysis. J Gastrointestin Liver Dis. 2018;27(3):299–306.
- Frolkis A, Dieleman LA, Barkema HW, et al. Environment and the inflammatory bowel diseases. Can J Gastroenterol. 2013;27(3):e18–e24.
- Sun Y, Li L, Xie R, et al. Stress triggers flare of inflammatory bowel disease in children and adults. Front Pediatr. 2019;7:432.
- Miyazawa T, Shiga H, Kinouchi Y, et al. Long-term course of inflammatory bowel disease after the great east Japan Earthquake. J Gastroenterol Hepatol. 2018;33(12):1956–1960.
- Satsangi J, Silverberg MS, Vermeire S, et al. The montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut. 2006;55(6):749–753.
- Goodsall TM, Han S, Bryant RV. Understanding attitudes, concerns, and health behaviors of patients with inflammatory bowel disease during the coronavirus disease 2019 pandemic. J Gastroenterol Hepatol. 2020;2020:299.
- Alboraie M, Piscoya A, Tran QT. et al. The global impact of COVID-19 on gastrointestinal endoscopy units: an international survey of endoscopists. Arab J Gastroenterol. 2020;21(3):156–161.
- Belle A, Barret M, Bernardini D, et al. Impact of the COVID-19 pandemic on gastrointestinal endoscopy activity in France. Endoscopy. 2020;52(12):1111–1115.
- Mittermaier C, Dejaco C, Waldhoer T, et al. Impact of depressive mood on relapse in patients with inflammatory bowel disease: a prospective 18-month follow-up study. Psychosom Med. 2004;66:79–84.
- Ghoshal UC, Sahu S, Biswas SN, et al. Care of inflammatory bowel disease patients during coronavirus disease-19 pandemic using digital health-care technology. JGH Open. 2021;5(5):535–541.
- Attauabi M, Poulsen A, Theede K, et al. Prevalence and outcomes of COVID-19 among patients with inflammatory bowel Disease-A Danish prospective population-based cohort study. J Crohns Colitis. 2021;15(4):540–550.