

Abstract
Objective
Patients with benign recurrent intrahepatic cholestasis (BRIC) suffer from recurrent episodes of cholestatic jaundice. Treatment options remain limited and are mainly symptomatic. In case reports rifampicin, plasmapheresis, and nasobiliary drainage have been reported to be effective. In this case series, we present long-term experience indicating disease-modifying effects of non-invasive treatment with rifampicin for recurrent cholestasis in BRIC type 1 (BRIC1).
Materials and methods
We included all adult BRIC1 patients diagnosed and followed up at a single centre in Bergen, Norway. Data regarding clinical and biochemical features during BRIC attacks with and without rifampicin treatment were retrieved from medical journals and a data registry.
Results
Five males with BRIC1 were included. Median age at diagnosis was 22 years (range 15–41). Together they had suffered from 65 cholestatic attacks (including four documented abortive attacks). Twenty-eight attacks were treated with rifampicin alone over the last 12 years; all cases showed symptomatic relief and reduction in the levels of bilirubin and alkaline phosphatase in blood. The attacks treated with rifampicin seemed to have shorter duration and were less likely to result in complications or hospitalization compared to attacks prior to the introduction of rifampicin. No side effects attributable to rifampicin were noted.
Conclusions
Episodic treatment of recurrent BRIC1 attacks with rifampicin seems to ameliorate severity and shorten the duration of attacks. Timely diagnosis and effective treatment are of major importance in BRIC, not only to decrease complications but also improving patients’ quality of life.
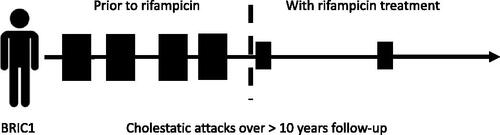
GRAPHICAL ABSTRACT
Author contributions
MV is the guarantor of the article and supervised the project. MV and GF conceived and designed the study. GF and HH collected the clinical and laboratory data. HH, GF, and MV contributed to the analysis and interpretation of data. HH drafted the manuscript. All authors reviewed the manuscript for critical content and approved the final version of the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s). MV received speaker’s honoraria from Intercept and GE Healthcare, unrelated to the present study.
Data availability statement
The original anonymous dataset is available on request from the corresponding author at e-mail: [email protected].