
Dear Editor,
We thank Dr. Vincenzo Ricci for his interest in our study [Citation1,Citation2] and acknowledge his contribution to the readership with his critical review. We would like to address the comments made in a point-by-point fashion.
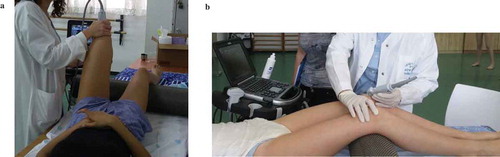
1. Unfortunately, it was not clearly clarified in the “materials and methods” that while US examination of the trochlea was evaluated in full knee flexion (with 110 knee flexion) (see )), the evaluation of the anterior, medial and lateral ligaments of the knee and of the intra-articular effusion in the supra patellar bursa was performed in mild flexion. That was performed with a 14.5 cm diameter cylinder placed under the knee as shown in ), corresponding to knee flexion of about 25 (and not in a 110-degree flexion as erroneously written). We regret this unintentional omission. The squeeze/shift effect is well recognized. This knee flexion is routinely used in clinical practice for this purpose [Citation3], allowing for stretching of the extensor mechanism without squeezing the suprapatellar bursa.
Figure 1. (a) Full flexion of the knee for trochlear cartilage evaluation; (b) Mid-flexion for tendons and suprapatellar fluid (intra-articular effusion) evaluation.
2. Respectfully, we do not agree with the point made regarding the effusion grading. At the time we designed our protocol, to the best of our knowledge there were no published, validated scoring or grading systems for supra-patellar effusion caused by mechanical pathologies in pediatric knees. The referred scoring system [Citation4] was published after our study. Furthermore, we find this classification, while very interesting and important, to be irrelevant to our study. The referenced scoring system was devised to evaluate pediatric knees with inflammatory arthritis. This is a very different population from ballet dancers. Moreover, it evaluates conjointly synovial hypertrophy and effusion, which is not really required in our cohort. We did actively look for fluid both in the midsagittal plane as well as in the parasagittal ones.
3. We did not evaluate tendons and ligaments with Doppler, as this requires highly sensitive Doppler equipment found in high-end ultrasound equipment [Citation5], while this study was performed with portable ultrasound equipment in the dance classroom. We were concerned that the sensitivity of our Doppler mode might be low for the detection of slow flow. Indeed, the absence of a Doppler signal would be impossible to differentiate, either due to a true lack of inflammation or to low sensitivity of the equipment.
Yet, we are not surprised by the low number of tendon pathologies in our dancers in their first year of intensive training: we expect tendinopathies to develop over months or years [Citation6].
4. Regarding the evaluation of femoral cartilage, it is crucial to understand that it was screened both in the transverse and longitudinal planes. We recorded any abnormality of signal and/or width, including focal thickening. In the transverse view used for morphological measurement, we did measure the cartilage thickness in the mid-portion of the 2 facets and chose the smallest measurement as a parameter for “cartilage minimal stock.” If we had chosen to calculate the average of both facet thicknesses as suggested, a cartilage thinning could have been wrongly undervalued by averaging it with the thicker facet.
5. We agree that maximal quality high resolution images should always be achieved, both in research and clinical setups. A tradeoff has to be found between optimization of the femoral cortical view and, more importantly, of the cartilage itself. However, as a well-qualified and experienced musculoskeletal ultrasound expert participated in this study, we find that the images as presented in Figure 3 of the manuscript are adequate for conducting reliable measurements and can be easily achieved by other clinicians.
Declaration of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Additional information
Funding
References
- Ricci V, Ozçakar L. Ersatz ultrasonographic measurements for the knee joint. Phys Sportsmed. 2018. DOI:10.1080/00913847.2018.1554964
- Siev-Ner I, Stern MD, Tenenbaum S, et al. Ultrasonography findings and physical examination outcomes in dancers with and without patellofemoral pain. Phys Sportsmed. 2018;46:48–55.
- Martinoli C. Musculoskeletal ultrasound: technical guidelines. Insights Imaging. 2010 Jul;1(3):99–141. doi: 10.1007/s13244-010-0032-9.
- Ting TV, Vega-Fernandez P, Oberle EL, et al. A novel ultrasound image acquisition protocol and scoring system for the pediatric knee. Arthritis Case Res. 2018 Sep 7. DOI:10.1002/acr.23746.
- Boesen MI, Boesen M, Langberg H, et al. Musculoskeletal colour/power Doppler in sports medicine: image parameters, artefacts, image interpretation and therapy. Clin Exp Rheumatol. 2010;28:103–113.
- Comin J, Cook JL, Malliaras P, et al. The prevalence and clinical significance of sonographic tendon abnormalities in asymptomatic ballet dancers: a 24-month longitudinal study. Br J Sports Med. 2013;47(2):89–92.