
COVID-19 has strongly impacted sporting participation at all levels of competition, with many large-scale events postponed or even canceled. Mass gatherings at sporting events have also been severely restricted [Citation1]; such gatherings are a known source of infectious disease transmission, with the potential for global spread upon return to home country [Citation2]. Moreover, it has been previously reported from the 2018 Winter Olympics that infectious diseases, in particular respiratory tract infections, may spread readily within the same sporting discipline or team [Citation2]. This presents strong rationale to manage the participating athletes appropriately to prevent further outbreak of COVID-19.
The postponed Tokyo 2020 Olympic Games were supposed to be the most attended gathering in sport of 2020, with the expected participation of 11,090 Olympic athletes and 4400 Paralympic athletes [Citation3]. Now rescheduled to begin in July 2021 (but with the potential for further deferral), it is paramount that the COVID-19 status of athletes is managed appropriately to ensure smooth sporting participation and to avoid unnecessary impedance of participants during their training, travel and stay.
The COVID-19 athlete passport
The passport presents a novel way of managing elite athletes, whereby they retain an electronic document (for example, on their phone or through an official IOC app) that reports their status regarding previous exposure to the virus, testing, results and vaccination. The system could be integrated so that the team manager/doctor also have access to the information of all athletes under their care. From this, appropriate precautions can be tailored to each athlete during their travel and stay in Tokyo, and risk can be stratified in the unfortunate event of an on-site COVID-19 exposure or outbreak.
The components and interpretation of a COVID-19 passport may change over time with the introduction of new evidence and innovation, but we outline here key items and recommendations based on current understanding. An example passport is included ().
Figure 1. COVID passport
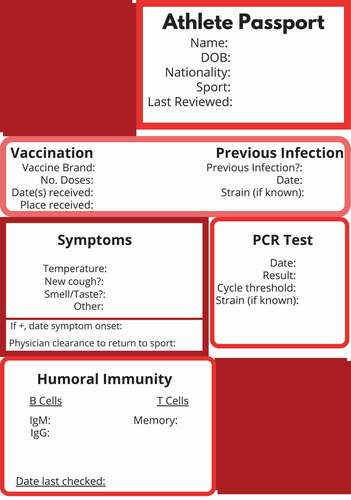
The rationale and interpretation of each component of the passport, based on current understanding (which may change in the interim between now and the Tokyo 2020 Olympic Games), are outlined below, to stratify risk for different athlete populations.
The passport should be forwarded to a committee of qualified doctors and advisors tasked with managing COVID-19 over the duration of the event, for review prior to departure for the Games, and additionally presented on entry to the Olympic Village by all athletes, to identify nonimmune and high-risk athletes at several stages, before they integrate with the wider athletic community. The athlete’s passport may be additionally requested at any point during their stay. Additional measures can then be taken for the individual (i.e. vaccination). In developing nations, where there may be a financial barrier to the athlete, the IOC could consider covering the costs of vaccination, to promote equal sporting opportunity. This may have to be delivered upon entry to the host country, or even the village, to ensure vaccine delivery. These athletes may have to be held separately until the delivery of their second dose. Vaccines should only be provided to asymptomatic athletes with a negative test. Under recent pressures, the IOC have said that they hope for all athletes to be vaccinated for the Games. There are currently no plans to selectively vaccinate athletes, but they are working with the WHO Covax project to accelerate vaccine roll-out in emerging nations [Citation4,Citation5].
For some athletes, a passport may need to be created upon arrival at the Village; they should remain in isolation until this is completed, which may additionally act as a deterrent toward athlete/team noncompliance with the passport. Group isolation could be considered in this case, with adequate equipment for an athlete to continue their preparations, and permitted visits from support staff in full PPE.
COVID-19 naïve athletes
This may only be relevant in the advent the IOC accepts athletes into the Village without requiring vaccination. The IOC and Japanese authorities are not currently making vaccination a mandatory requirement, but are strongly recommending it, and this may change with increasing doubt as to the feasibility of the Games running in 2021 [Citation4,Citation6]. Athletes who have not previously had a COVID-19 vaccination should be treated as naïve to the virus. It is important to identify who these athletes are, in order to isolate them as quickly as possible upon possible exposure. These athletes should be treated in accordance with local COVID-19 guidance for contacts.
In the event, a previously unexposed athlete becomes exposed to the virus, a negative PCR test should be interpreted with some caution, due to a reported sensitivity of between 70% and 98%; allowing for a conservative estimate of at least 70% [Citation7,Citation8]. Indeed, if the patient has a high pretest probability (i.e COVID symptoms (which should be recorded on the passport) or there is a high R value in the population being tested), then infection may still be likely, regardless of result [Citation7].
Athletes with a previously positive PCR test
Athletes who have previously been exposed to the virus and subsequently test positive on RT-PCR should be treated as either having current or recent infection, due to the high specificity of a positive test [Citation7]. Where available, the cycle threshold (Ct) value should be included, as a score >34 (potentially as low as >25, depending on the particular PCR test used) also indicates a low likelihood of viral transmission [Citation9,Citation10]. These two factors together can help determine the timeframe for re-integration with the sporting team without risk of re-infection, as well as indicate the likelihood of infectiousness on the date of testing. Reporting the experienced severity of the illness on the passport is also useful for athlete management, as increased severity may correlate to a more prolonged virus excretion [Citation9]. If the PCR test is taken within the previous 81 days, the Ct value may remain elevated, and for this reason, it is not recommended to retest athletes within this timeframe [Citation10]. The passport provides useful information in managing this, as well as informing the decision to reisolate (which may be unnecessary) [Citation10].
Antibody testing
The decision to test antibodies varies across national policies and it is at the discretion of the IOC as to whether this should be tested for the Olympic Games. In the circumstance where antibodies are measured, the test should report both IgM and IgG values for maximum sensitivity [Citation11,Citation12], and ideally this should test neutralizing antibodies, at least in the first instance. The exact type of test performed should be recorded on the passport. The strain of virus, if known, should also be a feature of the passport.
T Cell immunity
T cells, and in particular memory T cell immunity to COVID-19, is a strong indicator for long-term immunity that likely persists for years [Citation13]. Preliminary evidence suggests a robust memory T cell response in recovered individuals regardless of the presence of circulating antibodies (particularly in mild infection) [Citation13,Citation14]. Indeed, T cells have been identified in a minority of patients previously unexposed to the virus, which may impact individual susceptibility [Citation13,Citation15].The COVID-19 passport should therefore contain specific information regarding the athlete's T cell immunity, in particular the presence of memory T cells.
Vaccination history
The athlete’s vaccination date(s) should be recorded. Due to the differing rates of immunity attributable to different vaccines, the particular brand of vaccine given and number of doses received should be noted as well as the location of where the vaccination was given.
Return to sport post-infection
Clearance from a physician to return to sport post-COVID-19 infection should be included on an athlete’s passport. It is particularly important to assess the athlete for signs of myocardial involvement [Citation16,Citation17].
Conclusion
The World Health Organization have formulated recommendations to sport organizers in the context of COVID-19 [Citation18]; the COVID-19 passport should work within this generalized framework to stratify the individual risk to athletes. The passport should act to protect the athlete, their team and contacts wherever they travel. If implemented by the IOC, it could be presented by the athlete at any time, for regular review and as a source of succinct, important information. The IOC and TOCOG would also potentially have access to the entire athlete population when mounting a response to a potential outbreak or report of viral transmission.
Disclosure of Interest
The authors report no conflicts of interest.
Additional information
Funding
References
- Parnell D, Widdop P, Bond A, et al. COVID-19, networks and sport. Manag Sport Leisure. 2020;1–7. doi:https://doi.org/10.1080/23750472.2020.1750100
- Hoang VT, Al-Tawfiq JA, Gautret P. The Tokyo Olympic games and the risk of COVID-19. Curr Trop Med Rep. 2020;7:126–132.
- Gallego V, Nishiura H, Sah R, et al. The COVID-19 outbreak and implications for the Tokyo 2020 summer Olympic games. Travel Med Infect Dis. 2020;34:101604.
- Reuters K JIJI IOC plans to vaccinate every Olympic athlete to save Tokyo Games: report. 2021 23 01.
- IVETT I. IOC ‘in talks with World Health Organisation to accelerate process of getting athletes vaccinated’ in attempt to save Tokyo Games after Japanese government categorically denied summer showcase will be cancelled. Daily Mail; 2021.
- International Olympic committee president Thomas Bach discusses preparations for Olympic games Tokyo 2020 with six months to go until the opening ceremony [press release]. International Olympic Committee (IOC) & Tokyo; 2020 Jan 22.
- Watson J, Whiting PF, Brush JE. Interpreting a covid-19 test result. BMJ. 2020;369:m1808.
- Woloshin S, Patel N, Kesselheim AS. False negative tests for SARS-CoV-2 infection — challenges and implications. N Engl J Med. 2020;383(6):e38.
- Singanayagam A, Patel M, Charlett A, et al. Duration of infectiousness and correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to May 2020. Euro Surveill. 2020;25(32):2001483.
- Group SRA. Interpretation of PCR results and infectivity; 2020 Jul 30. [cited 2021 Jan 22]. Available from: https://covid-19.sciensano.be/sites/default/files/Covid19/30300630_Advice_RAG_interpretation%20PCR.pdf
- Mahajan A, Manchikanti L. Value and validity of coronavirus antibody testing. Pain Physician. 2020;23(4s):S381–s90.
- Xie J, Ding C, Li J, et al. Characteristics of patients with coronavirus disease (COVID-19) confirmed using an IgM-IgG antibody test. J Med Virol. 2020;92(10):2004–2010.
- Sekine T, Perez-Potti A, Rivera-Ballesteros O, et al. Robust T cell immunity in convalescent individuals with asymptomatic or mild COVID-19. Cell. 2020;183(1):158–68.e14.
- Altmann DM, Boyton RJ. SARS-CoV-2 T cell immunity: specificity, function, durability, and role in protection. Sci Immunol. 2020;5(49):eabd6160.
- Le Bert N, Tan AT, Kunasegaran K, et al. SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature. 2020;584(7821):457–462.
- Schellhorn P, Klingel K, Burgstahler C. Return to sports after COVID-19 infection. Eur Heart J. 2020;41(46):4382–4384.
- Hull JH, Loosemore M, Schwellnus M. Respiratory health in athletes: facing the COVID-19 challenge. Lancet Respir Med. 2020;8(6):557–558.
- WHO. Considerations for sports federations/sports event organizers when planning mass gatherings in the context of COVID-19: interim guidance; 2020 Nov 21. [cited 2021 Jan 22]. Available from: https://www.who.int/publications/i/item/considerations-for-sports-federations-sports-event-organizers-when-planning-mass-gatherings-in-the-context-of-covid-19-interim-guidance.