
Abstract
Improved conflict handling is important to reduce relational discord. Touch potentially has beneficial effects on three important characteristics of conflict discussions, i.e., physiological reactivity, affect and communication behavior. We studied effects of hand-holding between partners during conflict discussions (N = 47 student couples) and after conflict discussions (N = 53 student and N = 45 clinical couples). During conflict discussions hand-holding caused lower heart rate reactivity, higher positive affect and improved communication in men, and in women lower positive affect but improved communication. After conflict discussions hand-holding resulted in lower heart rate reactivity and higher heart rate variability in student couples and higher positive affect in student and clinical couples. Touch seems a promising add-on intervention in couple therapy.
Relational discord is present in about 30% of all couples and is fueled by frequent and destructive conflicts between partners (Kluwer & Johnson, Citation2007; Whisman, Beach, & Snyder, Citation2008). Improvement of conflict handling is therefore an important aim in couple therapy. However, couple conflicts are hard to control because it requires co-regulation between partners which is complex (Bloch, Haase, & Levenson, Citation2014; Levenson, Haase, Bloch, Holley, & Seider, Citation2015). Specifically, effective conflict handling demands adequate management within each partner of physiological reactivity, emotions, cognitions, and behavior, but also coordination at these levels between partners (Bloch et al., Citation2014; Levenson et al., Citation2015). This complexity means that disagreements easily escalate. For instance, within partners the physiological arousal geared by conflicts is associated with negative affect, negative partner attributions, and overlearned destructive interaction behavior (Gottman, Citation1994; Kiecolt-Glaser & Newton, Citation2001; Randall & Bodenmann, Citation2009), whereas between partners, tendencies to justify own behavior and criticize partner behavior can result in anger and reciprocal negative communication behavior like blaming and withdrawal resulting in further escalation.
Traditionally, couple therapies intervene at a verbal level, e.g., communication or problem-solving skills, to reverse dysfunctional spiraling during conflicts. This study examined touch as a non-verbal approach to improve conflict handling, i.e., hand-holding during and after conflict discussions. Touch is a basic way to communicate affection and seems an effective intervention since it has beneficial effects on physiological reactivity, affect, cognitions and interaction behavior, and enhances intimacy and affiliation (Hertenstein, Verkamp, Kerestes, & Holmes, Citation2006). If hand-holding proves to have positive effects during and after conflict discussions, it could be an interesting add-on intervention in couple therapy.
Beneficial effects of touch on conflict handling
To substantiate touch as a promising intervention, we discuss three important characteristics of conflict handling that can be improved by touch to make disagreements more constructive, i.e., physiological reactivity, affect and communication behavior. Potential pathways through which touch may exert its impact are mentioned.
First, attenuation of physiological reactivity is important in conflict handling as it helps partners to stay calm which enhances clear thinking and the application of constructive communication (Gottman, Citation1994). An important effect of touch is the buffering of stress (Field, Citation2010; Hertenstein et al., Citation2006; Jakubiak & Feeney, Citation2017). Observational studies found links between touch and reduced physiological reactivity in terms lower blood pressure and heart rate (Light, Grewen, & Amico, Citation2005), which was confirmed in several experimental studies (Ditzen et al., Citation2007; Grewen, Anderson, Girdler, & Light, Citation2003; Holt-Lunstad, Birmingham, & Light, Citation2008). These attenuating effects presumably are driven by increased oxytocin and reduced cortisol levels. Observational studies found associations between touch and such neuro-endocrine changes (Ditzen, Hoppman, & Klumb, Citation2008; Light et al., Citation2005), whereas the causal relationship between both was confirmed by experimental studies (Ditzen et al., Citation2007; Holt-Lunstad et al., Citation2008).
Second, affect plays an important role in conflict handling because one partner’s negative affect tends to trigger similar affect in the other partner resulting in reciprocity of affect (Gottman, Citation1994). Enhancement of positive affect and reduction of negative affect is therefore important in making conflict handling more constructive. Touch was found to be associated with positive affect in an observational study (Debrot, Schoebi, Perrez, & Horn, Citation2013), whereas experimental studies found reductions of self-reported and observed stress by touch after a laboratory task (Robinson, Hoplock, & Cameron, Citation2015) and, importantly, during a conflict discussion between partners (Jakubiak & Feeney, Citation2019).
Third, quality of the communication behavior itself largely determines the constructiveness of conflicts. For example, negative communication by one partner is likely to evoke similar communication in the other partner resulting in negative spiraling of communication (Gottman, Citation1994). Prevention or interruption of such escalation is important. Touch was found to be associated with easier conflict resolution in an observational study (Gulledge, Gulledge, & Stahmann Citation2003), whereas one experimental study demonstrated that touch enhanced communication behavior during a conflict discussion (Jakubiak & Feeney, Citation2019). Touch may exert its positive effect on communication through several pathways. As discussed above, touch causes higher oxytocin levels, and (experimentally) increased oxytocin was found to enhance constructive communication (Ditzen et al., Citation2009). Increased oxytocin also leads to enhanced trust (Kosfeld, Heinrichs, Zak, Fischbacher, & Fehr, Citation2005) which may support cooperation. In line with this Jakubiak and Feeney (Citation2017) postulated a cognitive pathway in which the interpretation of touch as signs of security and connectedness facilitates conflict handling. Indeed, experiments showed that touch causes positive perceptions of the toucher (Erceau & Guéguen, Citation2007). Finally, touch enhances compliant behavior (Field, Citation2010) which may promote fulfillment of the partners’ needs and prevent escalation of conflict.
Of note, the mentioned pathways through which touch may affect conflict handling are likely to be intertwined and supposedly bidirectional. Although theoretically important, examination of underlying mechanisms was not the scope of the current study. We aimed at testing whether touch had beneficial effects on the described characteristics of conflict discussions, i.e., physiological reactivity, affect and communication behavior.
Gender differences
Although touch potentially may have beneficial effects on partner conflicts, gender differences may exist. Compared to women, higher arousal during couple conflicts was found in men by Gottman and Levenson (Citation1988), whereas others found the reverse (Kiecolt-Glaser et al., Citation1996), or no gender differences at all (Verhofstadt, Buysse, Ickes, De Clercq, & Peene, Citation2005). Further, wives were found to be more influential than men in emotion co-regulation (Bloch et al., Citation2014; Nolen-Hoeksema & Jackson, Citation2001), whereas others found husband’s negativity to have more impact (Ferrer & Nesselroade, Citation2003; Gilbert, Fiske, & Lindzey, Citation1998). Finally, women were found to be more effective in calming physiological arousal by offering support than men (Glynn, Christenfeld, & Gerin, Citation1999). In sum, we conclude that research findings are inconsistent. Therefore, in the current study gender differences in the effects of touch were analyzed on an exploratory basis.
The current study
Almost all earlier research was limited in two respects: (a) the nature of the stressor applied, i.e., electric shock or standardized speech tasks instead of conflict discussions, and (b) the timing of touch relative to the stressor: i.e., prior to the stressor, which is not feasible in daily life since partner disagreements often arise spontaneously. Therefore, we studied effects of hand-holding during and after conflict discussions, which is potentially important for clinical practice. Only one of the studies discussed above examined the effects of hand-holding during conflict discussions (Jakubiak & Feeney, Citation2019). This study was conducted simultaneously with the current study and largely paralleled our ideas, although our study differed in several important respects. First, we too examined effects of hand-holding during conflict discussions which may facilitate prevention of escalation (study 1), however, additionally we examined the effects of hand-holding after conflict discussions, which is important in repairing destructive effects of escalation, rebuilding connectedness and thus creating a more solid basis for future discussions (study 2). Second, we also measured observed communication behavior (study 1), however, additionally we assessed two other important characteristics of conflict discussions and subsequent recovery periods: physiological reactivity and affect (study 1 and 2). Further, in study 2 we instructed partners to combine hand-holding with gazing at each other in order to strengthen pro-relation effects such as positive affect (c.f. a recent extensive review by Conty, George, & Hietanen, Citation2016). Finally, because of the lack of studies in clinical samples we included a clinical sample next to a student sample in study 2.
Hypotheses
Based on the literature reviewed we hypothesized that hand-holding would be associated with: (1) attenuated physiological stress (Ditzen et al., Citation2007; Grewen et al., Citation2003; Light et al., Citation2005) as indicated by lower heart rate reactivity in studies 1 and 2 and higher heart rate variability in study 2; (2) enhanced affect (Conty et al., Citation2016; Debrot et al., Citation2013; Robinson et al., Citation2015) in studies 1 and 2; and (3) enhanced communication behavior (Ditzen et al., Citation2009; Feldman, Citation2012; Jakubiak & Feeney, Citation2019) in study 1.
Methods study 1
Participants, design, and procedure
Study 1 was conducted from June till December 2013. Participants were undergraduate psychology students who brought their partner with them, from now on referred to as “study 1 student couples.” Couples (N = 47) with a close heterosexual relationship lasting longer than half a year were included. Because of ECG measurements couples were excluded when one or both partners suffered from a heart disease or used heart medication. Partners were instructed to refrain from coffee drinking, smoking and intense physical exercise 2 hours in advance of the experiment in order to prevent confounding of heart rate. The psychology student of the couple earned research credit points, or 20 euro. Socio-demographics and means of study variables are reported in supplementary material Table S1. Partners on average were about 20.5 years of age, mean relationship duration was almost 2 years, almost 90% were dating and relationship satisfaction (Dyadic Adjustment Scale; DAS) was high.
Four master students were thoroughly trained in the study protocolFootnote1 in three 2-hour sessions. Partners sat at opposing sides of a table. Importantly, the table was divided by a screen to prevent partner contact during all phases of the experiment except for the actual interaction during the conflict discussion. After attaching heart rate measurement devices partners had a resting period of 15 minutes, during which they read the information brochure, consented, and completed a general questionnaire (socio-demographics and assessment of confounders for heart rate) and the DAS.
Then we measured baseline heart rate during 3 minutes with the partners sitting at the table. Thereafter, topics on which both partners disagreed most strongly (DAS Consensus scale), were suggested for discussion. Next, partners got pencil and paper and had 3 minutes to prepare the discussion independently from each other. Then the screen was removed and depending on randomization, we applied a between-subjects design, partners were instructed to hold hands (or not) during the conflict discussion. The conflict discussion consisted of four parts. During the first 3 minutes the partners were free to speak and listen (free discussion-1). The next 6 minutes partners four times alternated speaking and listening to their partner. Each listening and speaking period was 90 seconds in length therefore partners listened and spoke twice. The listening period was used for the manipulation check. It was randomly determined who would speak first. The conflict discussion ended with 3 minutes of free discussion (free discussion-2). After the conflict discussion the screen was replaced and partners independently rated their affect during the discussion. Finally, they were debriefed and asked whether they felt safe after the conflict discussion or needed psychological support. The study was approved by the Ethics Committee of the University of Amsterdam (2013-CP-2762).
Measures
The general questionnaire contained questions about socio-demographics and potential confounders of heart rate (i.e., coffee, tobacco, alcohol, high blood pressure, heart disease, use of heart medication, birth control pill, and heavy exercising prior to the experiments).
The Dyadic Adjustment Scale (DAS; Spanier, Citation1976) measures relationship satisfaction. The Consensus subscale was used to select a topic for the discussion. The scale consists of 15 issues on which partners can disagree, e.g., finances. Cronbach’s alphas for this and other measures are reported per sample for both genders separately in supplementary material Table S1.
Heart rate reactivity, i.e., heart rate during the experiment minus heart rate during baseline, was measured as an indicator of autonomic stress responsiveness (Ditzen et al., Citation2007). For this a Polar CS600X device was attached to the thorax of each of the partners. Comparable Polars were evaluated as excellent with regard to reliability and validity (Essner, Sjöström, Ahlgren, & Lindmark, Citation2013). They assess bpm each second. We summed measurements to bpm per 15 seconds.
Affect during the conflict discussion was measured with the Positive and Negative Affect Scale (PANAS; Watson, Clark, & Tellegen, Citation1988). The PANAS consists of two subscales each measured by 10 items: Positive affect, sample item “interested,” and Negative affect, example item “nervous.” The items were scored by 5-point Likert scales ranging from 1 (“very little”) to 5 (“very much”).
As a measure of communication behavior, we observed interactions with the Communication Skills Test (CST; Floyd, Citation2007). The CST measures positive and negative communication and problem-solving proficiency exhibited by partners when discussing a relational issue. The quality of the communication of each speech turn was rated on a 5-point scale: (1) very negative (e.g., blame, mind reading, denying responsibility, withdrawal, very negative tone); (2) negative (e.g., confused problem-talk, disagree without rationale, leading and avoiding questions, negative tone); (3) neutral (problem talk, information, question); (4) positive (e.g., agree, disagree with rationale, accept responsibility, empathy, positive tone); and (5) very positive (e.g., summarize other/both, checking out, opinion/feeling probe, solution proposal, meta-communication, validation, soft feeling statement). The CST is a reliable and valid instrument (Floyd, Citation2007). To guarantee that observations were done blind for condition, i.e., hand-holding or not, only the audio recording of the discussion was scored and not the video. This presumably resulted in a conservative measure underestimating effects, since visual expressions of affiliation were not scored. Three undergraduate students were thoroughly trained in the CST and rated each speech turn of the discussions. One student rated all discussions, the other two each half of the discussions. Interobserver reliability was substantially, i.e., Cohen’s kappa’s of .70 and .72. To maximize reliability we summed and averaged the ratings of the observers per speech turn and collapsed the 5-point scale into a 3-point scale (negative, neutral and positive). Analyses were done on negative and positive turn scores separately. For each partner we summed the number of negative, neutral and positive turns per minute and divided this by the number of turns this partner spoke during this minute, resulting in the proportion of turns during the first and second free discussions that a partner showed negative, neutral or positive communication. For technical reasons the videos of 10 couples could not be scored. These couples did not significantly differ from the other 37 couples on socio-demographics and DAS scores.
Statistical analyses
Data were analyzed using multilevel modeling as implemented by the Linear Mixed Models module in SPSS ( Bryk & Raudenbush, Citation1987), which has a number of advantages over other methods such as ANOVA. First, the interdependence of measurements between partners within couples could be accounted for by including a random intercept at the level of couples, or, in case of communication behavior, random slopes at the individual level. Second, the interdependence of repeated measurements over time was controlled for by including an autoregressive model (AR1). Third, mixed models are adequate for dealing with partially missing data by using all obtained data in the model estimation. The independent variables: condition (hand-holding vs. non-hand-holding), sex and their interactions were included in the models as fixed effects. Time was added as covariate. In the final models we removed non-significant interaction effects with time. Heart rate reactivity (see below) was one dependent variable. The 3-minute baseline measurement of heart rate was included as covariate in the model. All analyses were repeated with the raw score of heart rate. The results obtained did not change. The single measurements of Negative and Positive Affect, and the repeatedly measured Negative and Positive Communication and Problem-solving behavior were the other four dependent variables.
Preliminary, we checked whether heart rate was confounded by coffee, tobacco, alcohol, high blood pressure, heart disease, use of heart medication, birth control pill, and heavy exercising prior to the experiments. Therefore, we added the main effect of each confounder and its interaction with condition (hand-holding vs. non-hand-holding) at once to the mixed model as described above. Outcome was heart rate during the listening period, and in case of study 2, during the first minute of the recovery periods. Because no significant interactions of confounder × condition appeared, we computed the models without confounders. Significance levels for all models were set at α < .05 (two tailed).
Agreed upon methods for power estimation of three level models, i.e., couples (level 3), individual partners (level 2) and repeated measurements (level 1) were not available at the time. However, Maas and Hox (Citation2005) recommend a sample size of at least 50 at level 2. Therefore, we assume that sample sizes would be sufficient with 94 partners (47 student couples) in Study 1, and 106 partners (53 student couples) and 90 partners (45 clinical couples) in Study 2.
The amount of missing data was negligible. Heart rate scores were missing in 4.0% of the cases in study 1 and in 0.4% in the study 2 student sample and in 0.3% in the study 2 clinical sample. The PANAS was missing in 4.1% of the cases in study 1 and 0.0% in study 2. Regarding the CST scores 0.33% was missing in study 1. Finally, effect sizes (Cohen’s ds) were computed, using the estimated marginal means and the SDs of the corresponding raw means (Feingold, Citation2009).
Results study 1
Manipulation check
We checked whether heart rate was increased by the conflict discussion. Therefore, we compared heart rate during the first minute of the baseline measurement with heart-rate during the first minute of the listening period during the conflict discussion. The listening period was selected, because otherwise speaking activity confounds heart-rate. The model revealed a significant main effect for condition (baseline vs. listening) within couples (F = 8.402; p=.006), implying the manipulation by the conflict discussion succeeded in increasing heart rate (73.99; SE = 1.15 vs. 76.90; SE = 1.16; Δ = +2.91 bpm; Cohen’s d = 0.26).
Effects of hand-holding on heart rate reactivity during conflict discussions
The linear mixed model for the conflict discussion revealed no significant main effect of condition, but a significant interaction for condition*sex ( and and ). In men hand-holding during the discussion resulted in lower heart rate reactivity than non-hand-holding (74.55; SE = 1.04 vs. 77.70; SE = 1.05; Δ = −3.15 bpm; deviation scores from baseline: 1.99; SE = 1.04 vs. 5.14; SE = 1.05; Cohen’s d = 0.61), whereas for women heart rate largely remained the same (77.52; SE = 1.03 vs. 78.60; SE = 1.06; Δ = −1.08 bpm; deviation scores from baseline: 4.95; SE = 1.03 vs. 6.03; SE = 1.06; Cohen’s d = 0.21).
Figure 1. Study 1: Effect of (non-)hand-holding by sex during conflict discussions on heart rate reactivity.
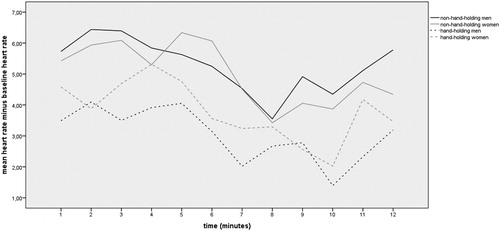
Table 1. Study 1 and 2: Effects of Hand-holding on Heart Rate Reactivity and Variability, Affect and Communication Behavior
Table 2 Study 1 and 2: Estimated Marginal Means and Effect Sizes of Significant Differences of Hand-holding vs. Non-Hand-holding
Effects of hand-holding on affect during conflict discussions
The mixed model for self-reported Negative affect (PANAS) during the conflict discussion revealed no significant main or interaction effects of hand-holding (). Concerning Positive affect, the interaction of condition*sex was significant ( and ). For men hand-holding resulted in a higher score on Positive affect than non-hand-holding (30.35; SE = 1.36 vs. 27.92; SE = 1.34; Δ = +2.43; Cohen’s d = 0.37), whereas for women hand-holding resulted in a lower score than non-hand-holding (25.91; SE = 1.36 vs. 31.46; SE = 1.36; Δ = −5.55; Cohen’s d = 0.83).
Effects of hand-holding on observed communication behavior during conflict discussions
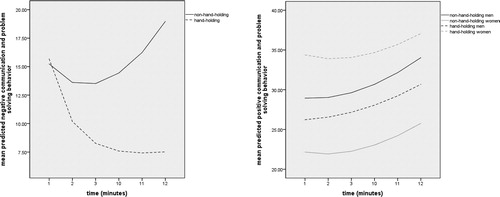
Negative communication and problem-solving behavior ( and and ) showed a significant interaction effect for condition × time, meaning that the proportion of Negative communication became increasingly lower during the conflict discussion in the hand-holding group compared to the non-hand-holding group. At the end of the discussion the proportions showed the greatest difference, i.e., approximately Δ = 0.14; Cohen’s d = 0.72. Concerning Positive communication ( and and ) we found a significant interaction effect for condition × sex, implying that, compared to non-handholding, handholding in women resulted in a higher proportion of Positive communication (0.37; SE = 0.04 vs. 0.25; SE = 0.03; Δ = +0.12; Cohen’s d = 0.79), but not in men (0.29; SE = 0.04 vs. 0.33; SE = 0.03; Δ = −0.04; Cohen’s d = 0.26).
Figure 2. (a and b) Study 1: Effect of (non-)hand-holding during the 1st and 2nd free discussions on negative and positive communication and problem solving behavior.
Methods study 2
Participants and procedure
Study 2 was designed to examine the effects of hand-holding after conflict discussions. For study 2 we used two samples, i.e., a new student sample (N = 53), from now on referred to as “study 2 student couples,” tested at the University of Amsterdam from December 2014 till February 2015, and a clinical sample of couples (N = 45) tested from January 2015 till April 2016. These clinical couples were in the final stage of relationship therapy at a Mental Health institution in Zeeland because of sexual problems or because one partner suffered from anxiety, mood disorder or trauma combined with cluster B or C personality disorder. See study 1 for inclusion and exclusion criteria and pre-experiment instructions. Compared to the study 2 student couples the clinical couples were about 20 years older, 14 years longer together, 75% more couples were married or cohabited, their level of educational attainment was lower, as was their relationship satisfaction (102 vs. 114) (Supplementary material Table S1). All differences were statistically significant.
Four master students were thoroughly trained during three 2-hours sessions in the study protocol. Like in study 1 the screen was placed on the table during the entire experiment except for the conflict discussions and the recovery periods with hand-holding. Unlike study 1 conflict discussions were followed by a recovery period in order to measure the effects of hand-holding after the conflict discussions.
The experiments started with a 15-minute resting period identical to the one in study 1. A 3-minute baseline measurement of heart rate followed. Partners sat still at opposing sides of a table while holding a small ball in each hand to imitate the hand-holding posture.
The experiment consisted of two conflict discussions, each followed by a recovery period. With a within-subjects design we compared the effects of hand-holding and gazing between partners during one recovery period with the other recovery period during which partners had no-contact. The two conflict discussions took place divided by a 4-minute resting period. Both conflict discussions had an identical structure and timing. First, partners had 3 minutes to prepare the topic of discussion determined with the DAS Consensus subscale like in study 1. Thereafter, the screen was removed and partners engaged in an 8-minute conflict discussion. Then a 3-minute recovery period followed in which partners were instructed to (a) hold hands and gaze at each other without moving or talking to prevent confounding of heart rate by muscular activity, or (b) the screen was replaced and partners had no contact during 3 minutes but held a ball in each hand. We counterbalanced possible order effects by randomizing the sequence of the (non-)hand-holding recovery periods. Affect (PANAS) during recovery was rated by partners independently after each recovery period. Then they were debriefed and asked whether they felt safe after the discussion or needed psychological support. Respondents received either research credit points or 20 euro. The study was approved by the Ethics Committee of the University of Amsterdam (2014-CP-3894).
Measures
For descriptions of the general questionnaire, the DAS and the PANAS, see study 1.
By means of ECG we measured heart rate reactivity, i.e., heart rate during the experiment minus heart rate during baseline, as an indicator of autonomic stress responsiveness, and heart rate variability (not assessed in study 1), as an indicator of flexibility of emotion regulation (Porges, Citation2009). Three electrodes were attached to the thorax of each partner. With the Versatile Stimulus Response Registration Program (Technical Support Group of the Department of Psychology, University of Amsterdam), we obtained heart rate, averaged to bpm per 15 seconds, and heart rate variability, calculated as RMSSD (root mean square of successive differences in RR intervals).
Statistical analyses
Mixed models were used for the same reasons as in study 1. The specified model was similar to that of study 1, however, a major difference with study 1 was the within-couple design of study 2, i.e., each couple was in both the hand-holding and the non-hand-holding recovery conditions. Therefore, “order” (first vs. second recovery period) was added to the model as a repeated measure one level above time, so that the interdependence of conditions was taken into account by the autoregressive model (AR1). Main effects of condition (hand-holding vs. non-hand-holding), sex, order, time and their interactions were included in the models as fixed effects. Non-significant interaction effects of time were removed from the final models. Baseline heart rate (variability) was included as covariate. As in study 1, no significant interactions of confounder*condition did appear, therefore we computed the models without confounders. Models were run separately for study 2 student and study 2 clinical couples. Significance levels were set at α < .05 (two tailed).Footnote2
Results study 2
Manipulation check
We checked whether the conflict discussions raised heart rate by comparing heart rate during the first minute of the baseline measurement with heart rate during the first minute after each conflict discussion.Footnote3 The mixed model revealed a main effect of condition (baseline vs. first minute first recovery period) in study 2 student couples (F = 11.992; p = .001; 70.50; SE = 1.13 vs. 73.87; SE = 1.05; Δ = +3.37 bpm; Cohen’s d = 0.30). A similar significant effect (F = 4.668; p = .035; 70.27; SE = 1.10 vs. 72.36; SE = 1.00; Δ = +2.09 bpm; Cohen’s d = 0.19) was found for the comparison between baseline and the second recovery period. This implies that both conflict discussions succeeded in increasing heart rate. However, in the clinical couples, non-significant differences were found, implying that the conflict discussion did not increase heart rate. As such, no further analyses concerning heart rate (variability) were conducted in this sample.
Effects of hand-holding on heart rate reactivity and variability after conflict discussions
The linear mixed model revealed significant main effects of condition, order and time on heart rate reactivity ( and and Supplementary material Figure S1), implying that study 2 student couples showed lower heart rate while holding hands after the discussion compared to non-hand-holding couples (70.14; SE = 0.48 vs. 71.61; SE = 0.48; Δ = −1.47 bpm; deviation scores: −3.26; SE = 0.48 vs. −1.79; SE = 0.48; Cohen’s d = 0.30). Concerning heart rate variability ( and and Supplementary material Figure S2) a significant main effect of handholding was found implying that heart rate variability during hand-holding was greater than during non-hand-holding (51.69; SE = 1.02 vs. 49.46; SE = 1.02; Δ = +2.23; deviation scores: 7.07; SE = 1.02 vs. 4.84; SE = 1.02; Cohen’s d = 0.24).
Effects of handholding on affect after conflict discussions
The mixed model for self-reported Negative affect (PANAS) during the recovery period after the conflict discussion revealed no significant main or interaction effects of condition in study 2 student couples or study 2 clinical couples (). Concerning Positive affect, a main effect of condition was revealed ( and ). In the hand-holding condition higher positive affect was reported than in the non-hand-holding condition by both study 2 student couples (28.24; SE = 0.92 vs. 21.46; SE = 0.92; Δ = +6.89; Cohen’s d = 0.72) and study 2 clinical couples (28.08; SE = 1.03 vs. 23.11; SE = 1.03; Δ = +4.97; Cohen’s d = 0.51).
Discussion
We examined the effects of hand-holding during and after conflict discussions between romantic partners in three samples. During conflict discussions we found in study 1 student couples that hand-holding in men was associated with a calming effect on physiological reactivity, a rise in positive affect and less negative communication behavior, while in women there was no effect on physiological reactivity, a drop in positive affect, but less negative and more positive communication. After conflict discussions we found a calming effect on physiological reactivity in both men and women of study 2 student couples, i.e., lower heart rate reactivity and higher heart rate variability, and a rise in positive affect in both men and women in study 2 student couples and clinical couples.
Potential implications for couple relationships
Apart from decreased positive affect in women holding hands during the conflict discussion, we consistently found positive effects of hand-holding during and after conflict discussions, which is in line with previous research (Debrot et al., Citation2013; Ditzen et al., Citation2007, Citation2009; Feldman, Citation2012; Grewen et al., Citation2003; Jakubiak & Feeney, Citation2019; Light et al., Citation2005).
During the discussion hand-holding improved several aspects of emotion regulation within study 1 student couples, i.e., male physiological reactivity, male affect, and male and female communication behavior. Together these effects may facilitate better co-regulation between partners. Gottman (Citation1994) suggested that reduced arousal may cause more constructive conflict regulation, since increased arousal gears dysfunctional beliefs and destructive communication behavior. Our findings suggest support for this in men. Hand-holding resulted in reduced physiological reactivity and more positive affect and less negative communication behavior in men. However, in women hand-holding did not significantly reduce physiological reactivity during the discussion. Nevertheless, their communication behavior became less negative and more positive. Apparently, reduction of physiological reactivity is not a necessary prerequisite for more constructive communication. An alternative explanation may be that merely the intimacy of holding hands (Burgoon, Citation1991) makes it harder to discuss matters harshly.
Interestingly, only one less beneficial effect of handholding was found. This appeared to be the lower positive affect during the conflict discussion in study 1 student women which contradicted with their increased constructive communication behavior. No such contradiction was found prior to a stressor in previous studies (Ditzen et al., Citation2007; Grewen et al., Citation2003; Robinson et al., Citation2015), during a conflict discussion (Jakubiak & Feeney, Citation2019) or after a conflict discussion (the current study 2). Perhaps women experienced the obligation to physically touch the partner while discussing relational problems as a constriction in expressing themselves which may have resulted in an internal conflict explaining the opposite effects on affect and communication behavior. In men, on the other hand, hand-holding possibly gave them some confidence that the discussion would not escalate, i.e., increased felt security (Jakubiak & Feeney, Citation2017). This could explain their converging outcomes, i.e., attenuated physiological reactivity, higher positive affect and less negative communication. Unfortunately, we did not ask partners about their thoughts concerning hand-holding while discussing relational issues.
After the conflict discussion hand-holding only had positive effects, i.e., a calming effect on physiological reactivity in study 2 student couples and a substantially increased positive affect in both study 2 student and study 2 clinical couples. It is noteworthy these effects occurred after discussing a topic of disagreement, i.e., the partner that first acted as a stressor subsequently functioned as a source of comfort and positive affect. The relatively small attenuating effect of hand-holding after the discussion on physiological reactivity may be due to gazing. A recent review shows that gazing heightens positive arousal (Hietanen, Citation2018).
Unexpected was the absence of effect on self-reported negative affect both during and after the conflict discussion in both sexes. This finding is contrary to the hypothesis of a stress-reducing effect of hand-holding, and inconsistent with a previous study (Robinson et al., Citation2015). One reason for this might be a low base rate of negative affect during the conflict discussion, suggesting the discussion was less stressful than anticipated.
Potential implications for clinical work with couples
One needs to be cautious when formulating clinical implications, since we did examine the effects of hand-holding in clinical couples only after and not during the conflict discussion (the latter being restricted to student couples). Nevertheless, we found several important indications that touch might be a helpful add-on intervention.
During conflict discussions hand-holding had converging, positive effects in male study 1 students on physiological reactivity, affect and communication behavior, but somewhat mixed effects in female study 1 students, i.e., a drop in positive affect and an increase of constructive communication behavior. Nevertheless, we consider the substantial, beneficial effect on communication and problem-solving behavior in both sexes to be crucial, since it facilitates prevention of escalation of disagreements.Footnote4 Further, we speculate that the effects of this improved communication might spread within and between partners over time, i.e. after applying hand-holding repeatedly during discussions, possibly resulting in improved affect too. Therefore, the drop in positive affect in study 1 student women might eventually prove to be temporarily. Moreover, beneficial effects of hand-holding might be magnified when applied during therapy as was demonstrated by Johnson et al. (Citation2013). Clinicians might therefore closely monitor the effects of hand-holding on arousal, affect, thoughts, and communication behavior, and discuss the associated changes in co-regulation with the partners.
Although hand-holding during discussions seem beneficial, it could be that imposing intimacy by touch may prove aversive for severely distressed clinical couples. We speculate that such discomfort, e.g. less positive affect and higher stress reactivity, may in particular surface in the short-term like in exposure. This might be seen as an indication of deeper emotional experiencing. Depth of experiencing is previously found to be positively associated with outcome in therapy (Pos et al., Citation2003) and is suggested as treatment enhancer in relationship interventions (Conradi, Dingemanse, Noordhof, Finkenauer, & Kamphuis, Citation2017). Nevertheless, for some couples hand-holding may remain aversive. In these cases touch might be used by the clinician as a diagnostic behavioral experiment to identify distress and aversion and discuss underlying fears and unfulfilled needs with the couple (Conradi, Noordhof, Boyette, & de Jonge, Citation2020).
Hand-holding and gazing after conflict discussions seem to have consistent positive effects, i.e., a modestly faster return to baseline arousal in study 2 student couples and substantially increased positive affect in both study 2 student and clinical couples. Therefore it can be suggested in clinical work as closure of partner discussions. Post-discussion hand-holding may rebuild and strengthen connectedness (Jakubiak & Feeney, Citation2017), the base upon which future discussions depart from. Clinically this means that hand-holding combined with gazing may prevent or soften long enduring aftermaths of conflicts.
Limitations and future research
Several limitations should be taken into account when interpreting our findings. First, with the conducted experiments we are not able to identify pathways through which hand-holding exerts its influence on heart rate reactivity, affect and behavior. For clinical practice, however, the specific pathway may not be that relevant. What matters is that hand-holding helps couples to achieve a more constructive discussion. Second, the current study 1 had no active control condition. Future studies may include such a condition, though it might be hard to design an adequate active control condition. Perhaps touching something that is uncommon to touch during a conflict discussion is an option, e.g., holding a wet towel or holding a stress ball. The latter was applied in study 2 in which we found beneficial effects of touch. Third, we are not able to disentangle effects of hand-holding and other non-verbal behavior, especially gazing in study 2. In future experiments these effects might be separated from each other. For clinical practice, however, we do not think this is a serious limitation, because it seems unlikely that partners will hold both hands without looking at all at each other. Fourth, we were unable to test the effect of hand-holding after the discussion on physiological reactivity in the clinical couples. This was due to the failure to increase physiological reactivity by the conflict discussion in the clinical couples, leaving no room for attenuation. An explanation for this may be the fact these couples were at the closure of treatment meaning they already discussed disagreements extensively in therapy. Another explanation is the fact that compared to the study 2 student couples the clinical couples already displayed a lower heart rate variability during baseline. Further, future research has to determine whether the positive effect of hand-holding on communication behavior during the discussion can be replicated in clinical samples. Finally, the effects of hand-holding appeared in an artificial lab setting. It is likely that the intensity of relational conflict in daily life is stronger than what can be induced in an experiment (Gottman, Citation1994). This may limit external validity, however, at the same time it indicates that even artificial circumstances produce effects on a single occasion. Therefore, a next step is a study applying hand-holding in an actual therapy setting. At the moment we are conducting a series of studies addressing these issues.
Conclusion
In sum, we found beneficial effects of hand-holding which are of clinical relevance. This is even more so because hand-holding is easily applied and, apart from abusive relationships, not subject to suspicions of inappropriateness. Learning how to de-escalate, tackling reciprocal negativity, and enhance positivity between partners are essential in stabilizing and strengthening relationships (Gottman, Citation1994). Taken together, we believe these studies have identified a promising avenue for research in treatment innovation in couple therapy.
Supplemental Material
Download MS Word (68.7 KB)Supplemental Material
Download PDF (138.4 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
Notes
1 Two other experiments were conducted in study 1 and 2. First, interpersonal distance between the partners was unobtrusively measured, and second, two heart rate measurements were done during which participants sat 3 minutes at the table with a screen in the middle, followed by 3 minutes while hand-holding and gazing.
2 The within-subjects design meant participants were aware of both conditions, i.e., (non-)hand-holding. This could have resulted in contrast effects in which participants overstated beneficial effects of hand-holding. Therefore, we additionally compared (non-)hand-holding after the first conflict discussion only. These between-subjects comparisons yielded identical results to the within-subjects comparisons over the two after discussion recovery periods, ruling out possible contrast effects.
3 Comparison of heart rate during baseline with heart rate during the conflict discussion would be confounded by speaking effects and was therefore not considered. The first minute of the recovery period was chosen because partners were silent at that moment while arousal of the conflict discussion should be still measurable.
4 Interestingly, the significant interaction of time and negative communication suggests support for reciprocity of communication as described by Gottman (Citation1994). Without hand-holding this resulted in increasing negative communication and with hand-holding in decreasing negative communication over time.
References
- Bloch, L., Haase, C. M., & Levenson, R. W. (2014). Emotion regulation predicts marital satisfaction: More than a wives’ tale. Emotion, 14(1), 130–144. doi:10.1037/a0034272
- Bryk, A. S., & Raudenbush, S. W. (1987). Application of hierarchical linear models to assessing change. Psychological Bulletin, 101 (1), 147–158. doi:10.1037/0033-2909.101.1.147.
- Burgoon, J. K. (1991). Relational message interpretations of touch, conversational distance, and posture. Journal of Nonverbal Behavior, 15, 233–259. doi:10.1007/BF00986924
- Conradi, H. J., Noordhof, A., Boyette, L. L., & de Jonge, P. (2020). Physical distance between romantic partners as marker for attachment in couples: A proof of concept study. Australian and New Zealand Journal of Family Therapy, 41(1), 91–106. doi: 10.1002/anzf.1398
- Conradi, H. J., Dingemanse, P., Noordhof, A., Finkenauer, C., & Kamphuis, J. H. (2017). Effectiveness of the ‘Hold me Tight’ relationship enhancement program in a self-referred and a clinician-referred sample: An emotionally focused couples therapy-based approach. Family Process, 57(3), 613–628. doi:10.1111/famp.12305
- Conty, L., George, N., & Hietanen, J. K. (2016). Watching eyes effects: When others meet the self. Consciousness and Cognition, 45, 184–197. doi:10.1016/j.concog.2016.08.016
- Debrot, A., Schoebi, D., Perrez, M., & Horn, A. B. (2013). Touch as an interpersonal emotion regulation process in couples’ daily lives: The mediating role of psychological intimacy. Personality and Social Psychology Bulletin, 39, 1373–1385. doi:10.1177/0146167213497592
- Ditzen, B., Hoppman, C., & Klumb, P. (2008). Positive couple interactions and daily cortisol: On the stress-protecting role of intimacy. Psychosomatic Medicine, 70, 883–889.
- Ditzen, B., Neumannc, I. D., Bodenmann, G., von Dawanse, B., Turnerf, R. A., Ehlerta, U., & Heinrichse, M. (2007). Effects of different kinds of couple interaction on cortisol and heart rate responses to stress in women. Psychoneuroendocrinology, 32, 565–574 doi:10.1016/j.psyneuen.2007.03.011
- Ditzen, B., Schaer, M., Gabriel, B., Bodenmann, G., Ehlert, U., & Heinrichs, M. (2009). Intranasal oxytocin increases positive communication and reduces cortisol levels during couple conflict. Biological Psychiatry, 62, 1187–1190. doi:10.1016/j.biopsych.2008.10.011
- Erceau, D., & Guéguen, N. (2007). Tactile contact and evaluation of the toucher. The Journal of Social Psychology, 147(4), 441–444. doi:10.3200/SOCP.147.4.441-444
- Essner, A., Sjöström, R., Ahlgren, E., & Lindmark, B. (2013). Validity and reliability of Polar® RS800CX heart rate monitor, measuring heart rate in dogs during standing position and at trot on a treadmill. Physiology & Behavior, 114–115, 1–5. doi:10.1016/j.physbeh.2013.03.002
- Feingold, A. (2009). Effect sizes for growth-modeling analysis for controlled clinical trials in the same metric as for classical analysis. Psychological Methods, 14(1), 43–53. doi:10.1037/a0014699
- Feldman, R. (2012). Oxytocin and social affiliation in humans. Hormones and Behavior, 61, 380–391. doi:10.1016/j.yhbeh.2012.01.008
- Ferrer, E., & Nesselroade, J. R. (2003). Modeling affective processes in dyadic relations via dynamic factor analysis. Emotion, 3, 344–360. doi:10.1037/1528-3542.3.4.344
- Field, T. (2010). Touch for socioemotional and physical well-being: A review. Developmental Review, 30, 367–383. doi:10.1016/j.dr.2011.01.001
- Floyd, F. J. (2007). Communication Skills Test (CST) observational system for couples’ problem-solving skills. In P. K. Kerig & D. H. Baucom (Eds.), Couple observational coding systems (pp. 143–157). New York, NY: Routledge.
- Gilbert, D. T., Fiske, S. T., & Lindzey, G. (1998). The handbook of social psychology (4th ed. Vol. 1). New York, NY: Oxford University Press.
- Glynn, L. M., Christenfeld, N., & Gerin, W. (1999). Gender, social support, and cardiovascular responses to stress. Psychosomatic Medicine, 61, 234–242.
- Gottman, J. M. (1994). What predicts divorce? The relationship between marital processes and marital outcomes. Hillsdale, NJ: Erlbaum.
- Gottman, J. M., & Levenson, R. W. (1988). The social psychophysiology of marriage. In P. Noller & M. A. Fitzpatrick (Eds.), Perspectives on marital interaction (pp. 182–200). Clevedon: Multilingual Matters.
- Grewen, K. M., Anderson, B. J., Girdler, S. S., & Light, K. C. (2003). Warm partner contact is related to lower cardiovascular reactivity. Behavioral Medicine, 29, 123–130. doi:10.1080/08964280309596065
- Gulledge, A. K., Gulledge, M. H., & Stahmann, R. F. (2003). Romantic physical affection types and relationship satisfaction. The American Journal of Family Therapy, 31, 233–242. doi:10.1080/01926180390201936
- Holt-Lunstad, J., Birmingham, W. S., & Light, K. C. (2008). Influence of a “Warm Touch” support enhancement intervention among married couples on ambulatory blood pressure, oxytocin, alpha amylase, and cortisol. Psychosomatic Medicine, 70, 976–985.
- Hertenstein, M. J., Verkamp, J. M., Kerestes, A. M., Holmes, R. M. (2006). The communicative functions of touch in humans, nonhuman primates, and rats: A review and synthesis of the empirical research. Genetic, Social, and General Psychology Monographs, 132(1), 5–94. doi:10.3200/MONO.132.1.5-94
- Hietanen, J. K. (2018). Affective eye contact: An integrative review. Frontiers in Psychology, 9, 1587. doi:10.3389/fpsyg.2018.01587
- Jakubiak, B. L., & Feeney, B. C. (2017). Affectionate touch to promote relational, psychological, and physical well-being in adulthood: A theoretical model and review of the research. Personality and Social Psychology Review, 21(3), 228–252. doi:10.1177/1088868316650307
- Jakubiak, B. L., & Feeney, B. C. (2019). Hand-in-hand combat: Affectionate touch promotes relational well-being and buffers stress during conflict. Personality and Social Psychology Bulletin, 45(3), 431–446. doi:10.1177/0146167218788556
- Johnson, S. M., Burgess Moser, M., Beckes, L., Smith, A., Dalgleish, T., Halchuk, R. … Coan, J. A. (2013). Soothing the threatened brain: Leveraging contact comfort with emotionally focused therapy. PLoS One, 8(11), e79314. doi:10.1371/journal.pone.0079314
- Kiecolt-Glaser, J., & Newton, T. (2001). Marriage and health: His and hers. Psychological Bulletin, 127(4), 472–503. doi:10.1037/0033-2909.127.4.472
- Kiecolt-Glaser, J. K., Newton, T., Cacioppo, J. T., MacCallum, R. C., Glaser, R., & Malarkey, W. B. (1996). Marital conflict and endocrine function: Are men really more physiologically affected than women? Journal of Consulting and Clinical Psychology, 64(2), 324–332. doi:10.1037/0022-006X.64.2.324
- Kluwer, E. S., & Johnson, M. D. (2007). Conflict frequency and relationship quality across the transition to parenthood. Journal of Marriage and Family, 69, 1089–1106. doi:10.1111/j.1741-3737.2007.00434.x
- Kosfeld, M., Heinrichs, M., Zak, P. J., Fischbacher, U., & Fehr, E. (2005): Oxytocin increases trust in humans. Nature, 435, 673–676. doi:10.1038/nature03701
- Levenson, R. W., Haase, C. M., Bloch, L., Holley, S. R., & Seider, B. J. (2015). Emotion regulation in couples. In J. J. Gross (Ed.), Handbook of emotion regulation (2nd ed.). New York, NY: Guilford.
- Light, K. C., Grewen, K. M., & Amico, J. A. (2005). More frequent partner hugs and higher oxytocin levels are linked to lower blood pressure and heart rate in premenopausal women. Biological Psychology, 69, 5–21. doi:10.1016/j.biopsycho.2004.11.002
- Maas, C. J. M. & Hox J. J. (2005). Sufficient sample sizes for multilevel modeling. Methodology, 1(3), 86–92. doi:10.1027/1614-2241.1.3.86.
- Nolen-Hoeksema, S., & Jackson, B. (2001). Mediators of the gender difference in rumination. Psychology of Women Quarterly, 25, 37–47. doi:10.1111/1471-6402.00005
- Porges, S. W. (2009). The polyvagal theory: New insights into adaptive reactions of the autonomic nervous system. Cleveland Clinic Journal of Medicine, 76, S86–S90. doi:10.3949/ccjm.76.s2.17
- Pos, A. E., Greenberg, L. S., Goldman, R. N., & Korman, L. M. (2003). Emotional processing during experiential treatment of depression. Journal of Consulting and Clinical Psychology, 71(6), 1007–1016. doi:10.1037/0022-006X.71.6.1007.
- Randall, A. K., & Bodenmann, G. (2009). The role of stress on close relationships and marital satisfaction. Clinical Psychology Review, 29, 105–115. doi:10.1016/j.cpr.2008.10.004
- Robinson, K. J., Hoplock, L. B., & Cameron, J. J. (2015). When in doubt, reach out: Touch is a covert but effective mode of soliciting and providing social support. Social Psychological & Personality Science, 6, 831–839. doi:10.1177/1948550615584197
- Spanier, G. B. (1976). Measuring dyadic adjustment: New scales for assessing the quality of marriage and other dyads. Journal of Marriage and Family, 38, 15–28. doi:10.2307/350547
- Verhofstadt, L. L., Buysse, A., Ickes, W., De Clercq, A., & Peene, O. J. (2005). Conflict and support interactions in marriage: An analysis of couples’ interactive behavior and on-line cognition. Personal Relationships, 12(1), 23–42. doi:10.1111/j.1350-4126.2005.00100.x
- Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070. doi:10.1037/0022-3514.54.6.1063
- Whisman, M. A., Beach, S. R. H., & Snyder, D. K. (2008). Is marital discord taxonic and can taxonic status be assessed reliably? Results from a national, representative sample of married couples. Journal of Consulting and Clinical Psychology, 76, 745–755. doi:10.1037/0022-006X.76.5.745