
Abstract
Virtual Reality (VR)-based treatments for anxiety disorders are efficacious but there is a lack of research examining anxious responses to VR erotica, which could innovate treatments for sexual difficulties. We examined erotica features that elicited anxiety and sexual presence in women. Thirty-eight women viewed erotic videos from different modalities (2D, VR) and points of view (1st, 3rd person) and completed anxiety and sexual presence measures before and after each video. Women experienced greater anxiety for VR than 2D films and reported the most anxiety for VR 1st person films. Sexual presence was affected by modality and point of view.
Introduction
VR immerses the user in a three-dimensional (3D) computer-generated world that provides sensory inputs, including visual, audio, and tactile feedback, giving them the impression of being in a new, life-like environment. Capital contributions from large corporations have allowed VR software to be run on smartphones and desktop computers (Cipresso, Giglioli, Raya, & Riva, Citation2018; Freeman et al., Citation2017). Further, development platforms (e.g., Unity) can be used to design VR environments at a low-cost (Cipresso, Serino, & Riva, Citation2016). These recent changes have led to VR being applied in several fields, including education (Radianti, Majchrzak, Fromm, & Wohlgenannt, Citation2020), physical therapy (Howard, Citation2017), surgical medicine (Mao et al., Citation2021), social skills training (Howard & Gutworth, Citation2020), and mental health (Freeman et al., Citation2017).
Cippresso and associates’ (2018) network and cluster analysis of VR-related literature revealed psychological treatment as the 5th most popular VR research area. Freeman and associates (2017) highlighted several avenues through which these technologies can innovate mental health research and clinical practice. Available data suggest that virtual environments (VE) can inform our understanding of mental disorders. For example, research has shown that VEs can elicit psychiatric symptoms in certain clinical samples and have been used to assess fear in individuals with Specific Phobias (Mühlberger, Bülthoff, Wiedemann, & Pauli, Citation2007) and social perception deficits in patients with Schizophrenia (Kim et al., Citation2007). Further, VR has been included in several treatment programs for anxiety disorders, with the use of this technology varying considerably among interventions. For instance, some protocols use VR to assist in the administration of interventions, such that patients engage in therapy to learn therapeutic skills, and then they may be immersed within VEs to practice techniques as one treatment component (Meyerbröker & Morina, Citation2021). In contrast, Virtual Reality exposure therapy (VRET), which involves the patient being immersed in a VE of their feared object/situation, has a greater focus on a VR component, although it is often combined with cognitive interventions (Meyerbröker & Morina, Citation2021). VRET has been used to treat several Specific Phobias, including fear of heights (Emmelkamp et al., Citation2002), flying (Rothbaum, Hodges, Smith, Lee, & Price, Citation2000, Rothbaum et al., Citation2006), and spiders (Donker et al., Citation2019).
A meta-analysis of controlled studies showed that VRET is as effective as classical evidence-based approaches for the treatment of anxiety disorders (Opriş et al., Citation2012). Specifically, there was no difference between VRET and cognitive behavioral therapy involving in vivo or imaginal exposure on reductions in participants’ anxiety symptoms, assessed via self-report or by clinician administered interviews (Opriş et al., Citation2012). Further, Emotional Processing Theory posits that fear must be activated for effective exposure to occur (Foa & Kozak, Citation1986). In the VR literature, presence has been identified as a key mechanism that allows for anxiety to be felt during VRET. Presence is the experience that one is within the VE despite knowledge that they are not there; it is a subjective perception influenced by how the viewer interprets stimuli presented by the VR system (Kyrlitsias & Michael-Grigoriou, Citation2022; Slater, Citation2009). A meta-analysis that reviewed 33 VRET studies examined the link between presence and anxiety, and showed a positive relationship with a medium effect (Ling, Nefs, Morina, Heynderickx, & Brinkman, Citation2014). VR’s ability to invoke presence and alter users’ anxiety paired with the wide array of possible VE environments offers exciting opportunities. This technology could be used to treat fear-based problems not easily addressed in-person, such as sexual dysfunction.
In their review of current uses of VR in sexology, Lafortune and associates (2020) point out that anxiety is central to the etiology of several sexual concerns, such as erectile dysfunction (Nguyen, Gabrielson, & Hellstrom, Citation2017), Genito-Pelvic Pain/Penetration Disorder (Desrochers, Bergeron, Landry, & Jodoin, Citation2008), and sexual aversion (Borg, de Jong, & Elgersma, Citation2014). Thus, individuals experiencing these sexual difficulties may benefit from VRET. Unfortunately, there is a lack of research examining people’s reactions to erotic VR content. Lafortune and associates’ (2022) recent study aiming to validate a VE for the treatment of sexual aversion represents a step forward in VR applications in sexuality research.
Sexual aversion involves an extreme aversion, strong dislike or disgust towards sex and erotic stimuli that causes distress and interpersonal difficulties, and affected individuals cope via avoidance of sexual activity (Borg et al. Citation2014). A survey study that used a representative sample (n = 8000) of the Dutch population aged 15–71 years revealed that approximately 4.5% of women and 2.4% of men experienced regular symptoms of sexual aversion (Kedde, Citation2012). Lafortune and associates (2022) examined the ability of a VE to elicit emotional responses consistent with sexual aversion (i.e., anxiety and disgust). Participants low and high in sexual aversion were immersed within VR sexual scenarios, and both groups reported an increase in anxiety and disgust as the sexual scenarios became more intense, although this effect was greater for individuals high in sexual aversion. The authors concluded that their VE could be a component of an efficacious treatment for sexual aversion, given that it appears safe and elicits levels of fear sufficient for exposure therapy within the high-sexual aversion group. However, the researchers acknowledged limitations of their computer-generated stimuli.
First, the authors reasoned that the increase in negative affect across scenarios for the low-sexual aversion group may be explained by the uncanny valley phenomenon, such that human-looking entities provoke aversion in human observers (Lafortune, Lapointe, Canivet, Godbout, & Boislard, Citation2022; Palomäki et al., Citation2018). If researchers are aiming to understand whether VR erotic stimuli elicit anxiety responses, they should investigate users’ reactions to stimuli depicting real people engaging in sexual acts in addition to computer-generated avatars. Second, Lafortune and associates (2022) note that their study did not include virtual simulations of conditions that typically elicit sexual aversion, for example one’s own nudity or genital contact between sexual partners. Whether depictions of various sexual activities in VR evoke different levels of anxiety is a question that requires further exploration. Third, the researchers chose VR sexual scenes that involved the viewer in a limited way, given that their virtual body was not a part of the sexual activities.
Recently, Milani et al. (Citation2022) explored women’s user experiences of VR erotica featuring human actors shown from different points of view (POV). The VR films immersed women in sexual encounters with a 180-degree field of view. These stimuli depicted dyads (one woman and a man or two women) engaging in consensual sexual activity that included kissing, genital touching, cunnilingus, and vaginal penetration. One VR film was shown from the 3rd person perspective, such that the participant viewed two actors having sex, as if she was on the edge of the bed that the actors were located on. The other video was from the 1st person perspective, and it was as if the participant was looking out of the eyes of one of the actors in the scene, who was lying on their back and receiving sexual stimulation. Notably, this latter condition provided the viewer with a self-avatar, a virtual representation of a body that could be accepted as their own (Gonzalez-Franco & Peck, Citation2018). Research has shown that self-avatars can induce an embodiment illusion (Peck & Gonzalez-Franco, Citation2021; Peck & Tutar, Citation2020), whereby the participant immersed within a VE perceives, to some degree, that the self-avatar has replaced their body at a physical or functional level (Gonzalez-Franco & Peck, Citation2018). If the participants viewing the VR 1st person film experienced the embodiment illusion, it is possible that they would experience the sexual acts in the video as happening to them. As a result, some women may have perceived that their physical space was being invaded, and given that they were not able to interact with the human actor (i.e., virtual sexual partner), they may have experienced the sexual encounters as non-consensual or coercive. All of these experiences would reasonably elicit anxiety. However, in Milani and associates’ (2022) study, women’s anxiety responses to these stimuli were not investigated.
Researchers may wish to capitalize on publicly available VR erotica when designing VRET paradigms due to the disadvantages of human-like avatars, the importance of exposing individuals with sexual concerns to a variety of sexual acts, and emerging data suggesting that VR videos from a 1st person perspective may boost embodiment. In addition, behavioral realism, the extent to which a VR character/actor behaves in a way that is similar to how an actual person would, predicts social presence, the sense that one is sharing a virtual space with another person (Oh, Bailenson, & Welch, Citation2018). Theoretically, this is important for the selection of stimuli for VRET programs because a clinician/scientist would want to provide the patient with an experience that mimics reality, which may facilitate the skills that they learn in the VR space being transferred to their real life. Given the complicated body language and speech that is required for sexual interaction, programming computer-generated avatars that act as realistic sexual partners is a challenge. Until the field can overcome this hurdle, using VR sexual films featuring human actors allows for stimuli that are realistic, show a range of sexual interactions, and easily switch between POVs.
As a proof of concept for this novel VRET methodology, we aimed to understand which, if any, stimuli features elicit distress in healthy controls (i.e., a non-clinical sample of women). Understanding how video modality and point of view impact the anxiety of healthy controls is important for two reasons. First, given that women with sex-related fear are likely to experience greater anxiety when viewing erotic stimuli than those without these concerns, if certain videos elicit levels of anxiety that overwhelm controls, they may not be suitable for use with clinical samples. Second, exposure treatment is typically done gradually, beginning with exposures to scenarios that elicit low levels of fear in phobic patients, and once their anxiety has habituated and/or they are confident in their ability to tolerate distress brought on by this situation, they will then complete more difficult exposures. If we find that healthy controls’ anxiety varies as a function of erotica features, these data will inform hypotheses about how clinical samples will respond to certain stimuli. The answer to these foundational research questions will enable the next phase of this research, which will include individuals with sexual dysfunction and will investigate the levels of VR-elicited anxiety that might make this paradigm useful in future VRET studies.
The current study
The primary goal of the present study was to investigate women’s state-level anxiety in response to erotic videos shown in different stimulus modalities (i.e., VR vs. 2D) and from different POVs (i.e., 1st person vs. 3rd person). We also explored how women’s sexual presence- their perception of being present and engaged within a real erotic encounter (Fontanesi and Renaud Citation2014)- was affected by stimulus modality and POV, and how sexual presence related to state-level anxiety. The data used in this paper were drawn from an existing dataset of self-report variables from a sample of women who viewed a series of VR and 2D sexual videos (Milani et al., Citation2022). We examined women’s changes in state-level anxiety before and after watching four types of erotic videos (i.e., VR 1st person, VR 3rd person, 2D 1st person, and 2D 3rd person). We also investigated their sexual presence after each film and correlated these with post-video state-level anxiety. We predicted that women’s anxiety and sexual presence would be greater in response to VR relative to 2D videos, and that participants would report more anxiety and sexual presence after viewing VR sexual encounters from 1st relative to 3rd POV. For each video, we anticipated that women’s post-film state-level anxiety would be positively correlated with their sexual presence.
Materials and methods
Participants
A convenience sample of 46 women was recruited through the University of British Columbia’s Human Subject Pool in the Department of Psychology. Participants were required to meet the following eligibility criteria: 1) self-identify as a woman; 2) 18+ years of age; 3) be comfortable watching erotic videos showing nude actors engaging in sexual activity. Data from eight women (seven who did not complete all study components; 1 due to a technical error) were excluded. Complete data were obtained from 38 cisgender women.
Materials
2D and VR videos
Participants were shown neutral videos depicting nature scenes and erotic videos showing either 1) a man and a woman, or 2) two women engaging in sexual activity including kissing, genital touching, cunnilingus, and vaginal penetration. Erotic videos focused on women’s pleasure and did not depict violence, fetish, bondage, discipline, dominance, or submission. Erotic films were selected from companies with ethical production practices and whose Terms of Use permitted noncommercial use of their videos.
Apparatus
The experiment was designed with Unity version 2019.1.7f1. A commercially available device used to view 3D content, the Oculus Quest VR headset, was used to show all videos (neutral and erotic). The Quest has a 360-degree field of view, a resolution of 1440 × 1600 pixels per eye, and a refresh rate of 72 Hz. Participants used the Oculus Touch VR controllers to respond to survey questions (see VR session measures below) within the headset, play/pause videos, and adjust volume.
Baseline measures
Demographics and sexual history
Participants were asked to provide standard demographics including age, education, ethnicity, religion, sexual orientation, relationship status, relationship length, previous erotica use, and previous VR experience. Women were asked to indicate, by selecting yes or no, whether they were experiencing any sexual difficulties at the time of the study. Participants who selected yes to this question were given the option to describe their sexual difficulty.
Anxiety
The anxiety subscale of the 42-item Depression, Anxiety, and Stress Scales (DASS) (Lovibond et al., 1995) was used to measure participants’ anxiety levels. Women were asked to rate the degree that various statements (e.g., I found myself in situations that made me so anxious that I was relieved when they ended) applied to them over the past week using a numeric scale ranging from 0 (did not apply to me at all) to 3 (applied to me very much, or most of the time). A total score was calculated for each participant by summing individual items with higher scores suggesting greater anxiety. The anxiety subscale of the DASS showed strong internal consistency in the current sample (ω = 0.89).
VR session measures
State-level anxiety
The shortened 6-item version of the State scale of the State-Trait Anxiety Inventory (STAI-6) (Marteau & Bekker, Citation1992) was used to assess participants’ state-level anxiety. Women completed this measure before and after viewing each erotic film and used a numeric scale to indicate how well six statements (e.g., I am tense) represented their current feeling state, with responses ranging from 1 (not at all) to 4 (very much so). STAI-6 total scores were calculated by summing individual items and ranged from 6–24, with higher scores suggesting greater state-level anxiety. The shortened STAI-6 demonstrated adequate internal consistency in the current sample (ω = 0.76), and scores on this measure are highly correlated with the full 20-item S-STAI, r > .90 (Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, Citation1983; Tluczek, Henriques, & Brown, Citation2009).
Sexual presence
Renaud and associates’ (Citation2016) 10-item Subjective Sexual Presence Scale (SSPS) was administered following each erotic film. Sexual presence involves motivational, emotional, and physical feelings experienced in response to erotic stimuli (Fontanesi & Renaud, Citation2014). The instrument includes 7 items that assess involvement with the presented media (e.g., To what extent did you feel as if you were witnessing live sexual intercourse taking place in front of you) and 3 items that measure realism of the scene (e.g., To what degree did you feel sexual arousal similar to any felt in a real sexual situation). Respondents used a numeric scale ranging from 1 (not at all) to 7 (completely) to rate the extent to which each item represented their experience. Total scores ranging from 10 to 70 were calculated by summing individual items, with higher scores suggesting greater sexual presence. This measure demonstrated strong internal consistency in our sample (ω = 0.80).
Procedure
Women signed up for the study through the University of British Columbia’s Department of Psychology Human Subject Pool. The study coordinator contacted them via email to schedule their lab session. One day prior to their in-lab participation, each woman received an individualized link sent by email that they used to complete a series of questionnaires via an online survey tool (Qualtrics). Upon arrival to the laboratory, participants were given an overview of study procedures by the research assistant, and they provided written consent. Participants were asked to confirm their age and comfort viewing erotic videos. The research assistant then provided instructions about the video paradigm, explained how the VR equipment worked, and assisted the participant to put on the VR headset. Participants completed a brief practice trial including a short nature film followed by some practice questions, which they answered using the VR controllers. After the research assistant left the room, women read a message in the headset that instructed them to select their preferred erotic film category (i.e., films depicting a woman and a man or films depicting two women) using the controllers. There were two video blocks (i.e., VR and 2D). When women viewed the VR videos, they were immersed in a 180-degree virtual space, whereas for the 2D condition they were seated in a virtual living room containing a 2D television screen that displayed the videos. For erotic videos shown from the 1st person stance, women viewed the sexual encounter as if their body was that of the female actor within the sexual scene. For erotic videos shown from the 3rd person stance, women viewed the sexual encounter as an onlooker not involved in the scene. Participants were randomly assigned to one of eight possible video presentation orders.
Participants completed a measure of anxiety within the headset using the VR controllers before and after viewing each erotic video, and measures of sexual presence, arousal, and attention after each video. Erotic videos were 5 min in length and were separated by 2-min nature videos to facilitate the return of participants’ sexual arousal to baseline (Huberman, Dawson, & Chivers, Citation2017). After watching the first block of videos, participants read instructions in the headset asking them to remove it to reduce the likelihood of eyestrain, headache, or other symptoms of cybersickness and contact the experimenter via intercom. The research assistant re-entered the testing room and informally asked about the participant’s wellbeing. Afterwards, participants completed a measure of general presence using an iPad. After a brief break, the research assistant helped the participant put the VR headset back on and left the testing room so participants could view the second block of videos. At the end of the video viewing session, participants ranked the videos based on their preference from 1 (most enjoyable) to 4 (least enjoyable). Findings pertaining to sexual arousal, attention, general presence, and video rankings were previously published (Milani et al., Citation2022). Participants read a message in the VR headset saying that they had completed the video viewing session and used an intercom to tell the research assistant that they had finished. The researcher re-entered the testing room, debriefed the participant, and reminded them that they would receive a final survey in 72 h, which assessed responsive desire. Women received two course credits to compensate for their time participating in the study. All study procedures were approved by the Behavioral Research Ethics Board at the University of British Columbia (#H10-00527).
Power analysis
The study was based on a secondary power analysis. Given that this was the first study to examine differences in women’s state-level anxiety in response to VR and 2D erotic films from different points of view, our analysis was exploratory in nature and no specific effect sizes were anticipated. An a priori power analysis conducted in G*Power 3.1 software for a repeated measures analyses of variance (ANOVA) indicated that to detect medium effects (ηp2 = .06) with power = .90, a sample of n = 23 would be required, which our sample (n = 38) surpassed. Thus, we were sufficiently powered to detect medium effects for anxiety (primary endpoint).
Data analysis
To examine the effects of video characteristics on women’s anxiety levels, we subjected STAI-6 scores to a 2 (modality: VR vs. 2D) x 2 (POV: 3rd person vs. 1st person) x 2 (time: pre-video vs. post-video STAI score) repeated measures ANOVA. Modality, POV, and time served as within-subject factors. To investigate the impact of erotic film features on women’s sexual presence, we subjected participants’ total SSPS scores to a 2 (modality: VR vs. 2D) x 2 (POV: 3rd person vs. 1st person) repeated measures ANOVA, with modality and POV as within-subjects factors. Interactions were further investigated using post-hoc pairwise comparisons. Bonferroni corrections were applied to account for family-wise error rates. Effect sizes were reported as eta-squared estimates for the repeated measures ANOVA (.01 = small, .06 = medium, .14 = large) and Cohen’s d (.20 = small, .50 = medium, .80 = large) for post-hoc comparisons. To examine the relationship between sexual presence and state-level anxiety, we conducted a Pearson correlation between total post-film STAI-6 and SSPS scores (summed across videos), as well as correlations between post-video STAI-6 and SPSS scores for each film. Although one outlier (i.e., 3 SD above group mean) was identified for the pre-video STAI-6 score for the 2D 1st POV condition, we retained it for data analyses because 1) there was no indication that the outlying score was due to a technical error or misreporting, and 2) only one of the eight repeated measures slightly violated normality and ANOVA is relatively robust to this assumption violation (Gravetter & Wallnau, Citation2014). Thus, analyses are based on all participants (n = 38).
Results
Sample characteristics and stimuli selection
The sample ranged in age from 19 to 31 years (Mage = 20.79, SD = 2.23). The 38 women reported the following ethnicities: East Asian (n = 16, 42.1%), Euro-Canadian (n = 13, 34.2%), South Asian (n = 4, 10.5%), multiethnic (n = 2, 5.3%), African (n = 1, 2.6%), Southeast Asian (n = 1, 2.6%), and one participant (2.6%) chose not to respond. Most participants identified as heterosexual (n = 32, 84.2%), while the remainder identified as bisexual (n = 4, 10.5%) or pansexual (n = 1, 2.6%) and one participant chose not to disclose their sexual identity. At the time of the study, half of the women reported being single (n = 19, 50%), 11 were in a relationship (28.9%), six were dating (15.8%), and two were common-law (5.3%). A subset of the sample reported previous experience with VR technology (n = 11, 28.9%).
Considering self-reported clinical characteristics, women’s scores on the anxiety subscale of the DASS reflected mild anxiety symptoms (M = 8.56, SD = 7.80) (Lovibond and Lovibond, Citation1995), 28.9% reported a history of non-consensual sexual contact, and four participants (10.5%) reported sexual difficulties at the time of the study. Among them, three participants disclosed difficulties reaching orgasm and one described low desire due to medication use. Concerning the type of erotic films viewed by participants, 78.9% (n = 30) elected to watch videos depicting one man and one woman actor and 21.1% (n = 8) selected films showing two woman actors.
Pre- to post-erotic video changes in state-level anxiety
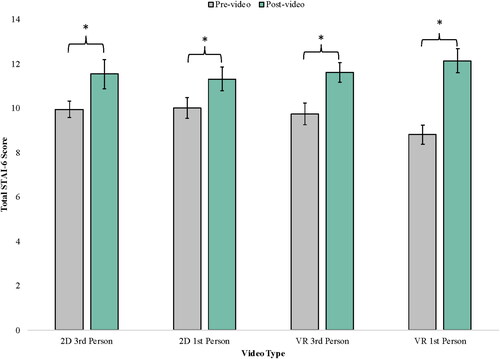
The 2 (modality: VR vs. 2D) x 2 (POV: 3rd vs. 1st person) x 2 (time: pre-video vs. post-video STAI score) repeated measures ANOVA revealed a significant main effect of time, F(1,37) = 30.37, p < .001, ηp2 = 0.45, with anxiety scores increasing from pre- to post-video across all conditions, and no significant main effects of modality, F(1,37) = 0.15, p = .7, ηp2 = 0.00, or POV, F(1,37) = 0.56, p = .5, ηp2 = 0.02. The significant main effect was qualified by a significant two-way interaction between modality and time, F(1,37) = 8.55, p = .006, ηp2 = 0.19, where increases in pre- to-post video anxiety scores were higher for VR (2.61, p < .001, d = 0.97) than for 2D videos (1.45, p < .001, d = 0.59). Two-way interactions between modality and POV, F(1,37) = 0.11, p = .7, ηp2 = 0.00, and POV and time, F(1,37) = 2.17, p = .1, ηp2 = 0.06, were non-significant. The significant two-way interaction was qualified by a significant three-way interaction between modality, POV, and time, F(1,37) = 4.42, p = .042, ηp2 = 0.12. Post-hoc examination of this three-way interaction revealed that the greater increase in anxiety scores after watching VR versus 2D videos was mostly attributable to the 1st person POV videos, and was twice as large (mean increase in anxiety: 3.34, p < .001, d = 0.87) as the increase in anxiety scores in the other three conditions (2D 3rd person: 1.58, p = .002, d = 0.56; 2D 1st person: 1.32, p = .005, d = 0.49; VR 3rd person: 1.87, p < .001, d = 0.61; see ).
Figure 1. Women’s self-reported pre- and post-video total STAI-6 scores are shown for each video type. Error bars represent standard errors of the mean. Scale ranges from 6–24. *p < 05. A bar graph showing women’s self-reported pre- and post-video total STAI-6 scores for the 2D 3rd person, 2D 1st person, VR 3rd person, and VR 1st person videos. Significant increases in STAI-6 scores for each video, with the largest pre- to post-video increase for the VR 3rd person film.
Sexual presence
The 2 (modality: VR vs. 2D) x 2 (POV: 3rd vs. 1st person) repeated measures ANOVA showed significant main effects of modality, F(1,37) = 69.00, p < .001, ηp2 = 0.65, and POV, F(1,37) = 7.02, p = .012, ηp2 = 0.16. Specifically, women reported greater sexual presence in response to VR relative to 2D erotic films (mean differences in SPSS scores = 11.18, p<.001, d = 1.35), and after viewing videos shown from the 1st rather than the 3rd person POV (mean difference = 2.89, p = .012, d = 0.43). The two-way interaction between modality and POV did not approach statistical significance, F(1,37) = 1.97, p = .2, ηp2 = 0.05. The total SSPS scores for each film were as follows: 2D 3rd POV (M = 31.39, SD = 8.11), 2D 1st POV (M = 32.55, SD = 10.70), VR 3rd POV (M = 40.84, SD = 7.37), and VR 1st POV (M = 45.46, SD = 11.09).
Relationship between state anxiety and sexual presence
The Pearson correlation between total post-video STAI-6 and SSPS scores revealed a positive relationship between state-level anxiety and sexual presence, r(36) = 0.44, p = .005. However, the Pearson correlations between post-video STAI-6 and SPSS scores ranged considerably for individual films. Specifically, there was a positive relationship between anxiety and sexual presence for the 2D 3rd POV film, r(36) = 0.39, p = .017, and for the VR 1st POV film, although this correlation did not reach statistical significance, r(36) = 0.23, p = .2. In contrast, there was no meaningful relationship between post-video STAI-6 and SSPS scores for the 2D 1st POV, r (36) = 0.07, p = .7, or VR 3rd POV condition, r(36) = 0.00, p = .9.
Discussion
Interpretation
In this study participants reported an increase in state-level anxiety for all erotic films shown. Considering how this pattern of findings fits into existing literature is challenging, given the lack of research examining women’s experiences of erotica (Ashton, McDonald, & Kirkman, Citation2018). While studies evaluating women’s emotional responses to sexual films indicate that low levels of anxiety, threat, or aversion can occur (Laan, Everaerd, van Bellen, & Hanewald, Citation1994; Peterson, Janssen, & Laan, Citation2010), a recent systematic review exploring women’s experiences of pornography indicated a diversity of reactions to these stimuli (Ashton et al., Citation2018). Considering VR erotic stimuli, the marked elevation in women’s state-level anxiety after viewing the 1st person VR sexual scene is in keeping with Dekker et al. (Citation2021) finding that men reported greater fear after viewing a VR film relative to a 2D erotic film from the same perspective, although in that study, this effect was small in magnitude. It is also of note that although participants experienced the greatest increase in anxiety scores for the VR 1st POV film, they also had the lowest pre-video anxiety for this condition. Taking this into consideration alongside the novelty of the present investigation, the question of whether women consistently experience greater state-level anxiety in response to VR relative to 2D erotic stimuli requires further study.
When considering why the VR 1st POV video elicited greater anxiety in our sample compared to the other stimuli, there are several factors to consider. First, given that women reported the greatest sexual presence in this condition, it is possible that they felt as if they were within the sexual scene, and that their personal space was being invaded, causing feelings of discomfort. The area 0–1 feet around one’s body is considered intimate space, where smell and touch are potentially exchanged (Hall, Citation1963). A robust literature illustrates that invasion of the intimate distance zone elicits defensive behavioral reactions, physiological stress responses, and reports of greater anxiety (Bergman, Citation1972; Felipe & Sommer, Citation1966). Researchers have shown that personal space invasions provoke similar responses in virtual environments, such that perceived intrusion into one’s personal distance zone by stereoscopically projected 3D images of people cause significant increases in viewer discomfort (Wilcox, Allison, Elfassy, & Grelik, Citation2006). In the VR 1st POV video employed in the current study, participants remarked that it felt as if the actor was directly on top of them, and at times very close to their face. In contrast, in the 3rd POV condition women perceived that the couple engaging in sexual activity was located across the virtual room. Thus, some of the anxiety women felt in the VR 1st POV condition could be related to a perceived invasion of their intimate space. Second, since women were not able to communicate with the actor engaging with their virtual body, and therefore had minimal control over the activities portrayed (although they could always remove the headset), it is possible that the videos felt coercive or non-consensual. However, it should be noted that although there was a positive relationship between sexual presence and anxiety overall, this correlation only reached statistical significance in the 2D 3rd POV condition. Consequently, the link between sexual presence and anxiety requires further study. Notably, the measure of sexual presence used in the current study assessed the extent to which women felt that they were engaged within a realistic sexual encounter, but was not a validated measure of embodiment, a related but separate construct. It is possible that a sense of embodying the self-avatar, such that the participants feels that their body has been replaced in a physical and functional sense by the self-avatar (Gonzalez-Franco & Peck, Citation2018), is a better predictor of anxiety responses to VR erotic stimuli than overall sexual presence. Both of our hypothesized mechanisms, personal space invasion and feelings of non-consent, rely on some degree of embodiment, and specifically, body ownership. Future researchers should include measures of embodiment in VR studies of this nature. Third, some participants chose to share with the researchers that they were not physically attracted to the actor in the VR 1st POV film and found that the increased realism in this video amplified their lack of attraction to the character, which could have indirectly increased their self-reported anxiety. Since it is easy to access and include VR erotica in research, future studies should consider offering participants a range of stimuli/characters to select from. Taken together, it is possible that each of these factors—i.e., personal space invasion, lack of control over the scene, and being unattracted to the actor - intensified feelings of discomfort and therefore anxiety.
Implications
The present study has important implications for future research. First, our results indicated that the non-clinical sample in this study did not experience any adverse events in the short-term in response to viewing VR erotica. In our study an adverse event constituted an unanticipated problem reflecting that the experiment was related to greater risk to participants than expected. For example, participants having panic attacks or dissociative episodes in response to the sexual stimuli, or dropping out due to high levels anxiety, disgust, or fear. No participants dropped out and increases in anxiety after viewing VR sexual videos were not especially large overall. However, future studies should conduct formal evaluations of safety of VR sexual stimuli, which would involve administering follow-up interviews with participants to assess whether exposure to VR sexual films influenced their real-life sexual behavior, and in what ways. Second, our results have implications for clinical samples who experience both anxiety and sexual difficulties. While all the erotic videos (2D and VR) elicited increases in state-level anxiety in our sample, it is likely that these stimuli would elicit greater anxiety in individuals who experience fear in anticipation of or during sex. While our findings suggest that 2D and VR erotica could be used in VRET programs aiming to treat fear-based sexual dysfunction, this requires further exploration in future studies.
VRET immerses patients in a 3D simulation of their feared situation. This approach has been used to treat several types of Specific Phobias, defined as persistent fears about situations that are out of proportion to the level of danger presented, causing impairment and/or distress (American Psychiatric Association, Citation2013). This novel intervention has been used to treat fear of heights (Emmelkamp et al., Citation2002), flying (Rothbaum et al., Citation2000; Rothbaum et al.,Citation2006), and spiders (Garcia-Palacios, Hoffman, Carlin, Furness, & Botella, Citation2002; Michaliszyn, Marchand, Bouchard, Martel, & Poirier-Bisson, Citation2010). Notably, systematic reviews of controlled studies suggest that VRET has comparable treatment efficacy to classical, evidence-based approaches (Opriş et al., Citation2012) and is as effective as in vivo (i.e., real-life) exposure for reducing behavioral avoidance in persons with Specific Phobias (Morina, Ijntema, Meyerbröker, & Emmelkamp, Citation2015). Research supporting the efficacy of VRET has excited scholars and clinicians alike, given that VR exposure may serve as an innovative solution for the treatment of anxiety-related concerns that pose ethical and practical barriers to conventional in-person exposure. In particular, the application of VRET as an intervention for sexual dysfunction is a research area that is both scarce and holds great research and clinical potential (Freeman et al., Citation2017; Lafortune, Dion, & Renaud, Citation2020).
A particular case in point is that VRET may be useful for people with Vaginismus, who experience intense fear of vaginal penetration accompanied by involuntary tightening of the pelvic floor muscles leading to persistent difficulties with vaginal intercourse (ter Kuile, Melles, de Groot, Tuijnman-Raasveld, & van Lankveld, Citation2013). A robust literature suggests that fear and avoidance of vaginal penetration are central to the etiology of Vaginismus, indicating that this disorder may be characterized by phobic features (Desrochers et al., Citation2008). Specifically, the Fear-Avoidance Model of Vaginismus (ter Kuile, Both, & van Lankveld, Citation2010) posits that maladaptive, catastrophic thoughts about penetrative sex elicit intense fear of penetration. To cope, individuals avoid vaginal intercourse, gynecological exams, and tampons. Critically, if the pelvic floor muscle tightening represents a defensive reflex, then gradual exposure to feared sexual stimuli may lead to an extinction of the phobic response, allowing for vaginal penetration to take place. While two studies conducted in the Netherlands revealed that therapist-guided exposure for Vaginismus, which involves an individual inserting vaginal dilators in the presence of a mental health practitioner, is highly effective (ter Kuile et al., Citation2009; ter Kuile et al., Citation2013), this treatment option is not available in North America due to institutional restrictions and licensing regulations. Thus, VRE for Vaginismus could allow affected individuals to undergo progressive exposure to feared sexual stimuli in a controlled environment and has the potential to dramatically improve care for people affected by this sexual difficulty.
Our findings shed light on how different types of erotic stimuli could be included in a VRET program for fear-based Vaginismus. When conducting real-life exposure therapy with individuals with Specific Phobias, the clinician works collaboratively with the client to create a fear hierarchy that provides a framework for treatment. The client will begin at the bottom of the hierarchy with exposures that elicit low levels of fear, and after the client is able to tolerate this distress, or their fear habituates with prolonged exposure and repetition, they will move up the hierarchy to more difficult exposures. This gradual approach provides the client with control over the therapy process and prevents them from being too overwhelmed to engage meaningfully in treatment. The VR 1st POV erotic video elicited greater anxiety in our sample relative to the 2D and VR 3rd POV films. Considering the realism and sense of presence invoked by these videos (Milani et al., Citation2022), it is likely that stimuli of this nature will elicit high levels of anxiety in individuals who experience fear in anticipation of or during sex. Thus, any future VRET program for Vaginismus might begin with patients viewing 2D erotic scenes, moving to VR films shown from the 3rd person perspective, and finally to VR 1st POV sexual stimuli. However, researchers should examine whether and how various erotica features, including modality and POV, affect a patient’s negative affect, and seek to identify stimuli that elicit low levels of negative affect for the earliest stages of exposure therapy.
Future directions
As a first step to developing a VRET program for Vaginismus, the present data suggest that researchers would be well-advised to examine how individuals with Vaginismus respond to VR erotica to determine whether these stimuli elicit sufficient levels of fear to allow for effective exposure. It is also recommended that investigators work with individuals with lived experience of Vaginismus to understand whether this treatment approach would be acceptable and feasible for this population. Additional avenues for investigation include exploring VR erotic video characteristics that may elicit discomfort. In particular, exploring how participants respond to sexual partners that they know are 3D erotic agents, virtual characters whose behaviors are determined by a computer algorithm, compared to users’ avatars, a character whose behaviors are being controlled by a user, is of great interest (Kyrlitsias & Michael-Grigoriou, Citation2022). Further, investigators should alter aspects of the participants’ self-avatar in the 1st person films to increase embodiment, such as improving multisensory integration, providing users with agency over the virtual body, and matching the gender and/or race to the user (Gonzalez-Franco & Peck, Citation2018). This would allow researchers to develop an understanding of the potential link between embodiment and anxiety in VR erotic scenes. Other promising lines of investigation include identifying other negative emotional responses that may occur to VR erotica, such as feelings of disgust and shame, which have been shown to play a role in sexual dysfunction (de Jong, van Overveld, & Borg, Citation2013; Pulverman & Meston, Citation2020). Focusing more broadly on sexuality research, researchers may wish to explore how VR film features, such as field of view, type of sexual activity depicted, the virtual environment containing the actors/avatars, and “fit” between the actors’/avatars’ and participants’ bodily characteristics, impact user experience more generally, beyond just anxiety. This information would help both clinicians and researchers in the future to select VR stimuli that best suits their therapy or research goals.
Limitations
This study was the first examination of women’s negative affect in response to VR erotica; thus, our findings require replication. Although the aim of the study was to examine women’s state-level anxiety in response to VR relative to 2D erotica and evaluate how film POV affected this outcome, the present study did not have the power to measure and/or examine the impact of several variables that could have acted as mediators or moderators. For example, we did not assess the effect of women’s previous sexual trauma on their anxiety during the experiment, given that a minority of our sample reported a history of non-consensual sexual contact. Examining the effects of trait-level anxiety, sexual victimization, sexual functioning, physiological sexual arousal, and attention on negative affective responses to erotic stimuli represents a promising line of future inquiry. Further, while our measure of state-level anxiety, the STAI-6, has been widely used in the literature we are not aware of published cut-off scores. We encourage future researchers to consider other measures of state-level anxiety with available guidelines for score interpretation.
It is also worth noting that the generalizability of our findings to other populations is constrained by the fact that our participants were drawn from a university human subject pool, and that most identified as East-Asian or Euro-Canadian. Additionally, it is possible that our results were affected by volunteer bias, as past work suggests that persons who are more likely to volunteer in sexuality studies report greater sexual experience, positive sexual attitudes, and more exposure to erotic materials (Dawson et al., Citation2019; Strassberg & Lowe, Citation1995). Thus, it is possible that a more representative sample of women would exhibit higher levels of anxiety.
Conclusions
This study is the first to evaluate women’s anxiety within 3D simulations of sexual scenarios using high quality, women-centred erotica, and VR equipment. We observed that women reported an increase in anxiety after viewing all sexual films. However, relative to 2D sexual videos, women reported greater elevations in state-level anxiety in response to VR films. This effect was largely explained by women’s heightened anxiety to VR stimuli where they perceived themselves to be in the position of one of the actors in the sexual scene (i.e., first-person point of view). Women also reported greater sexual presence for VR relative to 2D films, and for videos shown from the 1st relative to the 3rd person perspective. Our findings constitute one of the first steps in the future exploration of VR erotica’s potential usability as a therapeutic tool in the treatment of sexual dysfunctions (e.g., Vaginismus).
Disclosure statement
The authors report there are no competing interests to declare.
Additional information
Funding
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: APA. doi:10.1176/appi.books.9780890425596
- Ashton, S., McDonald, K., & Kirkman, M. (2018). Women’s experiences of pornography: A systematic review of research using qualitative methods. The Journal of Sex Research, 55(3), 334–347. doi:10.1080/00224499.2017.1364337
- Bergman, B. A. (1972). The effects of group size, personal space, and success-failure upon physiological arousal, test performance, and questionnaire response (unpublished doctoral dissertation). Temple University.
- Borg, C., de Jong, P. J., & Elgersma, H. (2014). Sexual Aversion and the DSM-5: An excluded disorder with unabated relevance as a trans-diagnostic symptom. Archives of Sexual Behavior, 43(7), 1219–1223. doi:10.1007/s10508-014-0341-z
- Cipresso, P., Giglioli, I. A. C., Raya, M. A., & Riva, G. (2018). The past, present, and future of Virtual and Augmented Reality research: A network and cluster analysis of the literature. Frontiers in Psychology, 9, 2086.doi:10.3389/fpsyg.2018.02086
- Cipresso, P., Serino, S., & Riva, G. (2016). Psychometric assessment and behavioral experiments using a free virtual reality platform and computational science. BMC Medical Informatics and Decision Making, 16(1), 37. doi:10.1186/s12911-016-0276-5
- Dawson, S. J., Huberman, J. S., Bouchard, K. N., McInnis, M. K., Pukall, C. F., & Chivers, M. L. (2019). Effects of individual difference variables, gender, and exclusivity of sexual attraction on volunteer bias in sexuality research. Archives of Sexual Behavior, 48(8), 2403–2417. doi:10.1007/s10508-019-1451-4
- de Jong, P. J., van Overveld, M., & Borg, C. (2013). Giving in to arousal or staying stuck in disgust? Disgust-based mechanisms in sex and sexual dysfunction. The Journal of Sex Research, 50(3–4), 247–262. doi:10.1080/00224499.2012.746280
- Dekker, A., Wenzlaff, F., Biedermann, S. V., Briken, P., & Fuss, J. (2021). VR porn as “empathy machine”? Perception of self and others in Virtual Reality pornography. The Journal of Sex Research, 58(3), 273–278. doi:10.1080/00224499.2020.1856316
- Desrochers, G., Bergeron, S., Landry, T., & Jodoin, M. (2008). Do psychosexual factors play a role in the etiology of provoked vestibulodynia? A critical review. Journal of Sex & Marital Therapy, 34(3), 198–226. doi:10.1080/00926230701866083
- Donker, T., Cornelisz, I., van Klaveren, C., van Straten, A., Carlbring, P., Cuijpers, P., & van Gelder, J.-L. (2019). Effectiveness of self-guided app-based virtual reality cognitive behavior therapy for acrophobia: A randomized clinical trial. JAMA Psychiatry, 76(7), 682–690. doi:10.1001/jamapsychiatry.2019.0219
- Emmelkamp, P. M. G., Krijn, M., Hulsbosch, A. M., de Vries, S., Schuemie, M. J., & van der Mast, C. a. P. G. (2002). Virtual Reality treatment versus exposure in vivo: A comparative evaluation in acrophobia. Behaviour Research and Therapy, 40(5), 509–516. doi:10.1016/s0005-7967(01)00023-7
- Felipe, N. J., & Sommer, R. (1966). Invasions of Personal Space. Social Problems, 14, 206. doi:10.2307/798618
- Foa, E. B., & Kozak, M. J. (1986). Emotional processing of fear: Exposure to corrective information. Psychological Bulletin, 99(1), 20–35. doi:10.1037/0033-2909.99.1.20
- Fontanesi, L., & Renaud, P. (2014). Sexual presence: Toward a model inspired by evolutionary psychology. New Ideas in Psychology, 33, 1–7. doi:10.1016/j.newideapsych.2013.10.001
- Freeman, D., Reeve, S., Robinson, A., Ehlers, A., Clark, D., Spanlang, B., & Slater, M. (2017). Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychological Medicine, 47(14), 2393–2400. doi:10.1017/S003329171700040X
- Garcia-Palacios, A., Hoffman, H., Carlin, A., Furness, T. A., & Botella, C. (2002). Virtual reality in the treatment of spider phobia: A controlled study. Behaviour Research and Therapy, 40(9), 983–993. doi:10.1016/s0005-7967(01)00068-7
- Gonzalez-Franco, M., & Peck, T. C. (2018). Avatar embodiment. Towards a standardized questionnaire. Frontiers in Robotics and AI, 5, 74. doi:10.3389/frobt.2018.00074
- Gravetter, F. J., & Wallnau, L. B. (2014). Essentials of statistics for the behavioral sciences (8th Edition). Wadsworth, Cengage Learning.
- Hall, E. T. (1963). A system for the notation of proxemic behavior. American Anthropologist, 65(5), 1003–1026. doi:10.1525/aa.1963.65.5.02a00020
- Howard, M. C. (2017). A meta-analysis and systematic literature review of Virtual Reality rehabilitation programs. Computers in Human Behavior, 70, 317–327. doi:10.1016/j.chb.2017.01.013
- Howard, M. C., & Gutworth, M. B. (2020). A meta-analysis of Virtual Reality training programs for social skill development. Computers & Education, 144, 103707. doi:10.1016/j.compedu.2019.103707
- Huberman, J., Dawson, S., & Chivers, M. (2017). Examining the time course of genital and subjective sexual responses in women and men with concurrent plethysmography and thermography. Biological Psychology, 129, 359–369. doi:10.1016/j.biopsycho.2017.09.006
- Kedde H. (2012). Seksuele disfuncties in Nederland: Prevalentie en samenhangende factoren. Tijdschrift voor Seksuologie, 36, 98–108.
- Kim, K., Kim, J.-J., Kim, J., Park, D.-E., Jang, H. J., Ku, J., Kim, C.-H., Kim, I. Y., & Kim, S. I. (2007). Characteristics of social perception assessed in schizophrenia using Virtual Reality. CyberPsychology & Behavior, 10(2), 215–219. doi:10.1089/cpb.2006.9966
- Kyrlitsias, C., & Michael-Grigoriou, D. (2022). Social interaction with agents and avatars in immersive virtual environments: A survey. Frontiers in Virtual Reality, 2, 786665. doi:10.3389/frvir.2021.786665
- Laan, E., Everaerd, W., van Bellen, G., & Hanewald, G. (1994). Women’s sexual and emotional responses to male- and female-produced erotica. Archives of Sexual Behavior, 23(2), 153–169. doi:10.1007/BF01542096
- Lafortune, D., Dion, L., & Renaud, P. (2020). Virtual Reality and sex therapy: Future directions for clinical research. Journal of Sex & Marital Therapy, 46(1), 1–17. doi:10.1080/0092623X.2019.1623357
- Lafortune, D., Lapointe, V. A., Canivet, C., Godbout, N., & Boislard, M. A. (2022). Validation of a virtual environment for sexual aversion. Journal of Behavioral and Cognitive Therapy, 32(2), 85–98. doi:10.1016/j.jbct.2021.11.001
- Ling, Y., Nefs, H. T., Morina, N., Heynderickx, I., & Brinkman, W.-P. (2014). A meta-analysis on the relationship between self-reported presence and anxiety in virtual reality exposure therapy for anxiety disorders. PloS One, 9(5), e96144. doi:10.1371/journal.pone.0096144
- Lovibond, S. H., Lovibond, P. F. (1995). Manual for the depression anxiety stress scales. New South Wales, Australia: Psychology Foundation of Australia.
- Mao, R. Q., Lan, L., Kay, J., Lohre, R., Ayeni, O. R., Goel, D. P., & Sa, D. de. (2021). Immersive Virtual Reality for surgical training: A systematic review. Journal of Surgical Research, 268, 40–58. doi:10.1016/j.jss.2021.06.045
- Marteau, T. M., & Bekker, H. (1992). The development of a six-item short-form of the state scale of the Spielberger State—Trait Anxiety Inventory (STAI). British Journal of Clinical Psychology, 31(3), 301–306. doi:10.1111/j.2044-8260.1992.tb00997.x
- Meyerbröker, K., & Morina, N. (2021). The use of Virtual Reality in assessment and treatment of anxiety and related disorders. Clinical Psychology & Psychotherapy, 28(3), 466–476. doi:10.1002/cpp.2623
- Michaliszyn, D., Marchand, A., Bouchard, S., Martel, M.-O., & Poirier-Bisson, J. (2010). A randomized, controlled clinical trial of in virtuo and in vivo exposure for spider phobia. Cyberpsychology, Behavior and Social Networking, 13(6), 689–695. doi:10.1089/cyber.2009.0277
- Milani, S., Jabs, F., Brown, N., Zdaniuk, B., Kingstone, A., & Brotto, L. (2022). Virtual Reality erotica: Exploring general presence, sexual presence, sexual arousal, and sexual desire in women. Archives of Sexual Behavior, 51(1), 565–576. doi:10.1007/s10508-021-02111-8
- Morina, N., Ijntema, H., Meyerbröker, K., & Emmelkamp, P. M. G. (2015). Can Virtual Reality exposure therapy gains be generalized to real-life? A meta-analysis of studies applying behavioral assessments. Behaviour Research and Therapy, 74, 18–24. doi:10.1016/j.brat.2015.08.010
- Mühlberger, A., Bülthoff, H. H., Wiedemann, G., & Pauli, P. (2007). Virtual Reality for the psychophysiological assessment of phobic fear: Responses during virtual tunnel driving. Psychological Assessment, 19(3), 340–346. doi:10.1037/1040-3590.19.3.340
- Nguyen, H. M. T., Gabrielson, A. T., & Hellstrom, W. J. G. (2017). Erectile dysfunction in young men—A review of the prevalence and risk factors. Sexual Medicine Reviews, 5(4), 508–520. doi:10.1016/j.sxmr.2017.05.004
- Oh, C. S., Bailenson, J. N., & Welch, G. F. (2018). A systematic review of social presence: Definition, antecedents, and implications. Frontiers in Robotics and AI, 5, 114. https://www.frontiersin.org/articles/10.3389/frobt.2018.00114 doi:10.3389/frobt.2018.00114
- Opriş, D., Pintea, S., García-Palacios, A., Botella, C., Szamosközi, Ş., & David, D. (2012). Virtual Reality Exposure therapy in anxiety disorders: A quantitative meta-analysis. Depression and Anxiety, 29(2), 85–93. doi:10.1002/da.20910
- Palomäki, J., Kunnari, A., Drosinou, M., Koverola, M., Lehtonen, N., Halonen, J., Repo, M., & Laakasuo, M. (2018). Evaluating the replicability of the uncanny valley effect. Heliyon, 4(11), e00939. doi:10.1016/j.heliyon.2018.e00939
- Peck, T. C., & Gonzalez-Franco, M. (2021). Avatar embodiment. A standardized questionnaire. Frontiers in Virtual Reality, 1, 575943. doi:10.3389/frvir.2020.575943
- Peck, T. C., & Tutar, A. (2020). The impact of a self-avatar, hand collocation, and hand proximity on embodiment and stroop interference. IEEE Transactions on Visualization and Computer Graphics, 26(5), 1964–1971. doi:10.1109/TVCG.2020.2973061
- Peterson, Z. D., Janssen, E., & Laan, E. (2010). Women’s sexual responses to heterosexual and lesbian erotica: The role of stimulus intensity, affective reaction, and sexual history. Archives of Sexual Behavior, 39(4), 880–897. doi:10.1007/s10508-009-9546-y
- Pulverman, C. S., & Meston, C. M. (2020). Sexual dysfunction in women with a history of childhood sexual abuse: The role of sexual shame. Psychological Trauma: Theory, Research, Practice, and Policy, 12(3), 291–299. doi:10.1037/tra0000506
- Radianti, J., Majchrzak, T. A., Fromm, J., & Wohlgenannt, I. (2020). A systematic review of immersive Virtual Reality applications for higher education: Design elements, lessons learned, and research agenda. Computers & Education, 147, 103778. doi:10.1016/j.compedu.2019.103778
- Renaud, P., Neveu, S. M., Rouleau, J. L., & Joyal, C. (2016). Sexual presence: A qEEG analysis of sexual arousal to synthetic pornography. International Journal of Telepresence, 1, 1–3.
- Rothbaum, B. O., Anderson, P., Zimand, E., Hodges, L., Lang, D., & Wilson, J. (2006). Virtual Reality exposure therapy and standard (in vivo) exposure therapy in the treatment of fear of flying. Behavior Therapy, 37(1), 80–90. doi:10.1016/j.beth.2005.04.004
- Rothbaum, B. O., Hodges, L., Smith, S., Lee, J. H., & Price, L. (2000). A controlled study of Virtual Reality exposure therapy for the fear of flying. Journal of Consulting and Clinical Psychology, 68(6), 1020–1026. doi:10.1037//0022-006x.68.6.1020
- Slater, M. (2009). Place illusion and plausibility can lead to realistic behaviour in immersive virtual environments. Philosophical Transactions of the Royal Society B: Biological Sciences, 364(1535), 3549–3557. doi:10.1098/rstb.2009.0138
- Spielberger, C., Gorsuch, R., Lushene, R., Vagg, P., & Jacobs, G. (1983). Manual for the State-Trait Anxiety Inventory (Form Y1 – Y2). In Palo Alto, CA: Consulting Psychologists Press; Vol. IV.
- Strassberg, D. S., & Lowe, K. (1995). Volunteer bias in sexuality research. Archives of Sexual Behavior, 24(4), 369–382. doi:10.1007/BF01541853
- ter Kuile, M. M., Both, S., & van Lankveld, J. J. D. M. (2010). Cognitive behavioral therapy for sexual dysfunctions in women. Psychiatric Clinics of North America, 33(3), 595–610. doi:10.1016/j.psc.2010.04.010
- ter Kuile, M. M., Bulté, I., Weijenborg, P. T. M., Beekman, A., Melles, R., & Onghena, P. (2009). Therapist-aided exposure for women with lifelong vaginismus: A replicated single-case design. Journal of Consulting and Clinical Psychology, 77(1), 149–159. doi:10.1037/a0014273
- ter Kuile, M. M., Melles, R., de Groot, H. E., Tuijnman-Raasveld, C. C., & van Lankveld, J. J. D. M. (2013). Therapist-aided exposure for women with lifelong vaginismus: A randomized waiting-list control trial of efficacy. Journal of Consulting and Clinical Psychology, 81(6), 1127–1136. doi:10.1037/a0034292
- Tluczek, A., Henriques, J. B., & Brown, R. L. (2009). Support for the reliability and validity of a six-item State Anxiety Scale derived from the State-Trait Anxiety Inventory. Journal of Nursing Measurement, 17(1), 19–28. doi:10.1891/1061-3749.17.1.19
- Wilcox, L. M., Allison, R. S., Elfassy, S., & Grelik, C. (2006). Personal space in virtual reality. ACM Transactions on Applied Perception, 3(4), 412–428. doi:10.1145/1190036.1190041