

Abstract
Strategies to prevent mortality from obstetric venous thromboembolism begin with identification, risk stratification and subsequently, implementation of prophylactic measures. We sought to identify the burden of pharmacologic thromboprophylaxis in postpartum women, including the main clinical indications and its uptake in a multireligious population, with Islam as the official religion. A total of 2514 deliveries between 1st January to 31st December 2016, across three centres in Malaysia were reviewed retrospectively from hospital-based registries. 770 (30.62%) patients fulfilled the criteria for thromboprophylaxis based on the revised 2015 criteria proposed by the Royal College of Obstetricians and Gynaecologists. A combination of age, parity, BMI, caesarean section and preterm births were the main indications. One out of the five patients who delivered vaginally required thromboprophylaxis. In our setting with a sizable Muslim population, low molecular weight heparin was the thromboprophylaxis of choice in more than two-third of the patients. The information obtained from this study allows better local resource planning.
What is already known on this subject: Risk factors for venous thromboembolism in pregnancy and puerperium are largely drawn from registries due to the rarity of the index event. Up to 7% of women require antenatal thromboprophylaxis based on the criteria proposed by the Royal College of Obstetrician and Gynaecologists in 2009.
What do the results of this study add: Using the RCOG guideline revised in 2015, a significant proportion of women delivering vaginally would require postnatal thromboprophylaxis based on age, parity and BMI. When either age or parity, both with relatively low odds ratio for thrombosis were omitted, a substantial proportion of women would not achieve the threshold for prophylaxis. Despite a sizable Muslim population in the country, the uptake of low molecular weight heparin was relatively high.
What are the implications of these findings for clinical practice and/or future research: Cost-benefit studies should consider the adjusted odds ratio of individual indications on a VTE event. While uptake and acceptability is high, prospective studies on medication adherence is equally pertinent.
Impact statement
Introduction
Obstetric venous thromboembolism (VTE) has received increasing attention from the medical community in recent times, as it is one of the leading cause of maternal mortality in developed countries, including the United Kingdom. A total of 64 cases of maternal deaths attributable to VTE were reported between 2009 and 2013 in the UK (Nelson-Piercy Citation2015). Similar trends were seen in the Asia-Pacific region, where 14 maternal deaths due to VTE were reported in Japan between 2010 and 2012, representing 6.5% of all maternal deaths (Hasegawa et al. Citation2016). Locally, 39 mothers succumbed to thromboembolism during the 2006–2008 triennium (Ministry of Health Malaysia Citation2013). The significance of this condition is magnified in part by the reduction in ‘traditional’ causes of maternal deaths such as haemorrhage and hypertensive disorders in pregnancy (Ministry of Health Malaysia Citation2013; Nelson-Piercy Citation2015).
Strategies to prevent such deaths begin with increasing awareness amongst healthcare professionals and patients, development of succinct yet comprehensive guidelines for identification and risk stratification and subsequently, implementation of evidence-based prophylactic measures. However, this is not a forthright task, as evidenced by the different risk scoring recommendations from various authoritative obstetric societies (The American College of Obstetricians and Gynecologists Citation2011; Chan et al. Citation2014; Royal College of Obstetricians and Gynaecologists Citation2015). One possible reason for this is because most risk factors were identified through retrospective cohorts, giving rise to different odds ratios for a given risk factor (Heit et al. Citation2005; James et al. Citation2006; Sultan et al. Citation2013). Admittedly, however, retrospective case identification and review of risk factors are the most reasonable methods for rare, but potentially fatal events, such as VTE.
The lack of concrete evidence for mechanical or pharmacological prophylaxis and the ideal duration when prophylaxis is indicated adds fuel to fire. Most trials are extrapolated or drawn from the non-obstetric population (Royal College of Obstetricians and Gynaecologists Citation2015). In fact, increasing patient awareness and clinical vigilance per se has been suggested in women who are able to accept VTE risks (Bain et al. Citation2014; Bates et al. Citation2016).
Nevertheless, the overall burden of VTE prompted the implementation of the Sarawak Obstetric Venous Thromboembolism Prevention Programme. The cause specific mortality for VTE-related deaths in Sarawak was for the 4.8–6.6 per 100,000 live births compared to the national average of 2.0–3.1 per 100,000 live births during the 2010–2012 triennium (Sarawak State Health Department Citation2013). With minor modifications, the risk scoring of the programme adopted the Royal College of Obstetricians and Gynaecologists’ recommendations (RCOG). Women with a postpartum score of 2 or more were offered low molecular weight heparin (LMWH) as a first line, for a minimum of 10 days. Formal counselling was given by the pharmacists, which included methods of self-administration and disposal of used needles. Women were given the alternative of unfractionated heparin (UFH) if LMWH was unacceptable to them, including on religious grounds. Women who declined any form of pharmacological prophylaxis were re-counselled by a consultant and advised for anti-embolism stockings.
Women who were at risk received information pamphlets on obstetric VTE and notification to the primary health clinics were done as part of the electronic discharge notification. Their VTE score would be keyed into the Sarawak Birth Informatics (Informatik Kesihatan Sarawak) by the midwife of the respective hospitals before discharge. All women who required VTE prophylaxis were made aware of the signs and symptoms of VTE and when to seek help.
The primary purpose of this study is to review the proportion of women who fulfil a minimum VTE risk score of 2 and above, thereby requiring pharmacological thromboprophylaxis. Although most women delivering by caesarean section would meet this criteria, the proportion of women delivering vaginally is less clear. In addition, the study would also look at the frequency of individual risk factors which contribute to the VTE risk score.
Materials and methods
Design
This was a multicentre, retrospective observational study conducted between 1st January to 31st December 2016. The study involved three small district hospitals, namely Sri Aman Hospital, Sarikei Hospital and Kapit Hospital. We hypothesise that certain maternal demographic characteristics such as maternal age, parity and body mass index >30 kg/m2 (BMI) would collectively add to the VTE risk score.
As of January 2013, all pregnant women in the state have undergone individualised, documented serial risk assessment for venous thromboembolism based on the RCOG recommendations. The scoring system used in this paper is based on the modification of the updated April 2015 criteria, and has been in place since July 2015 (Royal College of Obstetricians and Gynaecologists Citation2015). Under this scoring system, all postpartum women who were assigned a score of 2 and above, would require 10 days of thromboprophylaxis. Consequently, any woman who delivered via emergency caesarean section would require thromboprophylaxis while women who delivered via elective caesarean section with one additional risk factor would similarly qualify. Women who delivered vaginally on the other hand, would require two risk factors to fulfil the threshold criteria. One modification we implemented was to initiate thromboprophylaxis in all women delivering via caesarean section.
Enoxaparin 40 mg (ClexaneTM, Sanofi-Aventis) was the LMWH used in women weighing between 50 and 90 kg. Doses of 20 mg and 60 mg were used if the women’s weight were below 50 kg or beyond 90 kg, respectively. Unfractionated heparin 5000 units (HeparinolTM-5000, Ain Medicare) was the alternative for women who declined LMWH.
Each hospital kept a registry of all postpartum women who required thromboprophylaxis and this was reviewed for case identification. Cross-checking of this information was performed by reviewing the electronic discharge notification issued to the primary health clinics or by using the Sarawak Birth Informatics, a statewide online registry of all women who have delivered in the state. Each pregnant woman possessed a single, unique database which is allocated to her throughout her reproductive history.
Individual case notes would then be traced from the Medical Records Unit of the respective hospitals in the event of ambiguity for further clarification of patients’ demographic or clinical risk factors. This would be performed independently by the site investigators. Essential information would then be transferred to a standardised proforma. The delivery rate in each hospital would be identified through the hospitals’ primary delivery registry. This study received approval from the Ministry of Health’s Medical Research and Ethics Committee (MREC), NMRR ID 16-2049-32789.
Inclusion criteria
All postnatal women who delivered beyond 24 + 0 weeks of gestation, regardless of mode, with a venous thromboembolism score of two or more.
Exclusion criteria
Exclusion criteria were missing or untraceable previous admission case notes resulting in inability to confirm venous thromboembolism score.
Statistical analysis
Data collected from the proforma will be keyed-in to SPSS version 19 (SPSS, Chicago, IL). Descriptive analysis would be performed for patient demographics to obtain mean values, range and standard deviation. Primary outcomes would be analysed using percentages or proportion, with the denominator based on total delivery rates/year and vaginal delivery rates/year.
Results
A total of 2514 deliveries were conducted in the three centres over the period of the study. The mean age of the patients were 30.12 ± 7.13; obesity rates were 10.46% with a cumulative caesarean section rate of 14.20%. 770 (30.62%) patients fulfilled the criteria for thromboprophylaxis. one out of the five women who delivered vaginally required thromboprophylaxis. The breakdown by individual centres are shown in .
Table 1. Mode of delivery, professed religion and thromboprophylaxis.
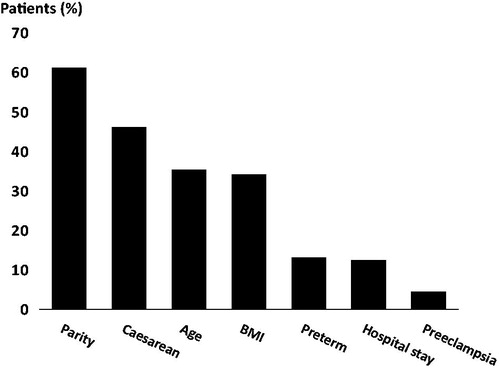
The main indications for thromboprophylaxis are shown in , whereby more than half have parity (471/770) as a risk factor, while more than a third had either caesarean section (355/770), age (272/770) or BMI ≥30 kg/m2 (263/770) as a risk factor. Preterm birth, which was incorporated as a risk factor for thromboembolism in the 2015 RCOG guideline, was one of the top five indications. This excluded preterm births for iatrogenic indications.
Figure 1. Main indications for postpartum thromboprophylaxis.
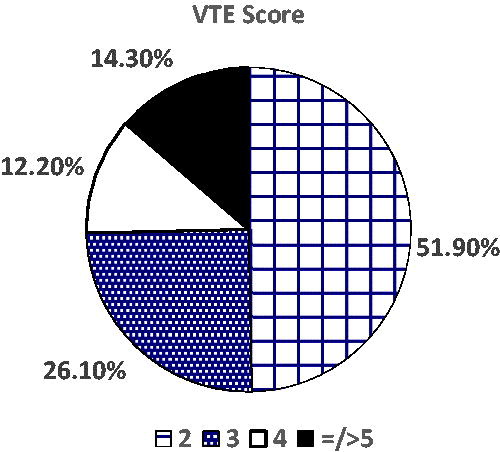
The majority of patients who required thromboprophylaxis had a score of 2, but of concern, 14.3% of patients scored 5 or more. An example of such a patient would be a 36-year-old lady in her third pregnancy with pre-eclampsia, who required an emergency caesarean section in labour for foetal compromise.
The uptake of pharmacological thromboprophylaxis was remarkably high with only two out of the 770 patients declining any form of thromboprophylaxis. LMWH was the first line medication offered and generally acceptable to the cohort scrutinised. However, 29% (47/162) of the Muslim patients opted for unfractionated heparin instead, citing concerns over the porcine derivative of LMWH. This meant that about 70% of Muslims in our population were able to accept the use of LMWH.
Discussion
Indication
Maternal age ≥35 years, parity ≥3 and BMI ≥30 kg/m2 were the main maternal risk factors contributing to the use of thromboprophylaxis. Grandmultiparity is more common in Malaysia, and the country is also suffering from an increasingly obese population (Institute for Public Health Citation2015). Consequently, the indirect impact is a greater proportion of obstetric population who require thromboprophylaxis.
While the elevated risk of VTE in women with higher BMI is well-recognised, the adjusted odds ratio of age and parity is more contentious (Heit et al. Citation2005; Royal College of Obstetricians and Gynaecologists Citation2015). The college recognises that any increase in risk due to age is modest at best and available evidence appears conflicting (Won et al. Citation2011; Colmorn et al. Citation2014; Royal College of Obstetricians and Gynaecologists Citation2015). Omission of age would have excluded 116/770 (15.06%) women from the use of thromboprophylaxis. Similarly, the evidence on parity is less robust, with adjusted odds ratio of a VTE event higher for primiparous women compared to those in their second and third pregnancy. Omission of parity per se in our population would have excluded 243/770 (31.56%) women from achieving a VTE risks score of 2.
Although it is recognised that emergency caesarean sections confer a higher risk towards a VTE event than elective caesarean sections, the fact remained that any caesarean section increased this risk by 2- to 6-fold, compared to vaginal deliveries. (Jacobsen et al. Citation2008; Royal College of Obstetricians and Gynaecologists Citation2015). In the Sarawak Obstetric Venous Thromboembolism Prevention Programme, all women who delivered by caesarean section were given a VTE risk score of 2. During the initial stages of implementation, we found that it provided a platform for uniformity and reduced confusion amongst the supporting staff.
Assigning a score of 1 for elective caesarean sections would have a marginal effect on the overall usage of thromboprophylaxis; a reduction of 12/770 (1.55%). This was because the majority of patients who underwent elective caesarean sections had additional risk factors and would have still reached the threshold for starting thromboprophylaxis.
Duration
While VTE risk scoring is useful to distinguish those who are low from intermediate risk, beyond the postnatal score of 2, higher scores still receive a standard 10-day thromboprophylaxis. This is despite evidence that the risk of VTE remains elevated even after 3 weeks postpartum (Tepper et al. Citation2014). It would be difficult to fathom that the 14.3% of patients, with a score of 5 or more in our cohort, be managed similar to another with a score of 2 (). Prolonging the duration of thromboprophylaxis is an option, although this has to be balanced against additional cost and compliance, which are beyond the context of this paper.
Figure 2. VTE risk score amongst women who were started on thromboprophylaxis.
Uptake
Any programme aimed at prevention is only as good as its uptake by the targeted population. Malaysia is a multireligious country with Islam, Christianity, Buddhism and Hinduism having a significant following. With Islam as the official religion, we recognised that there may be conflicting views amongst Muslim patients, with regards to the use of low molecular weight heparin, which is derived from porcine deoxyribonuceic acid (Department of Statistics Citation2011). Religious edicts or fatwas falls under the jurisdiction of individual states and may influence patients’ decisions. Alternatives available to such patients include unfractionated heparin and fondaparinux (ArixtraTM, Aspen). Likewise, patients professing other faiths have expressed concerns about the bovine content of medications (Shagar Citation2016). Unfractionated heparin, which requires regular platelet monitoring due to the risk of heparin-induced thrombocytopenia, is one such example (Fausett et al. Citation2001).
Reassuringly, the uptake of thromboprophylaxis is generally high in these centres because of the level of trust towards healthcare providers and awareness from antenatal and preoperative counselling. In addition, the cost of thromboprophylaxis is borne by the provider.
Conclusions
Understanding the extent of thromboprophylaxis required in both vaginal and caesarean deliveries in a population is central in planning the use of resources. Awareness of the risk factors contributing to the threshold score and its uptake are pertinent cogitations in its successful implementation.
Strength and limitations
This study examined patients who received thromboprophylaxis after documented, systematic scoring for risk of VTE rather than a cohort of potentially eligible patients. With data from over 2500 patients reviewed over a one-year period, it provided a more comprehensive estimate of thromboprophylaxis use compared to previous studies (Revell and Smith Citation2011). In addition, there are no studies evaluating the rate of thromboprophylaxis after vaginal delivery, using either the 2009 or 2015 RCOG guidelines, although one paper examined the rate of VTE regardless of the mode of delivery (Alalaf et al. Citation2015).
Although the individual centres were small, they reflect the patient profile of many remote district hospitals in our country, served by a single obstetrician. However, in centres with higher caesarean section rate, the overall use of thromboprophylaxis would increase accordingly. We did not examine the antenatal use of thromboprophylaxis, which has been estimated in the region of 0.45–7% in other studies (Revell and Smith Citation2011; Kutuk et al. Citation2014). While religion did not seem to be a major barrier towards the use of thromboprophylaxis, our high uptake rate at the time of discharge may not reflect subsequent medication adherence.
An understanding of the contribution of each risk factor to the VTE score and its impact towards a VTE event is fundamental. Financial resources are not infinite and this study is hoped to provide preliminary data for resource planning and future cost-effectiveness analysis.
Acknowledgements
The authors would like to thank the Director-General, Ministry of Health Malaysia for permission for publication.
Disclosure statement
The authors report no declarations of interest.
References
- Alalaf SK, Jawad RK, Muhammad PR, Ali MS, Al Tawil NG. 2015. Bemiparin versus enoxaparin as thromboprophylaxis following vaginal and abdominal deliveries: a prospective clinical trial. BMC Pregnancy and Childbirth 15:72.
- Bain E, Wilson A, Tooher R, Gates S, Davis LJ, Middleton P. 2014. Prophylaxis for venous thromboembolic disease in pregnancy and the early postnatal period. Cochrane Database of Systematic Reviews 2:CD001689.
- Bates SM, Middeldorp S, Rodger M, James AH, Greer I. 2016. Guidance for the treatment and prevention of obstetric-associated venous thromboembolism. Journal of Thrombosis and Thrombolysis 41:92–128.
- Chan WS, Rey E, Kent NE. for the VTE in Pregnancy Working Group. 2014. Venous thromboembolism and antithrombotic therapy in pregnancy. Journal of Obstetrics and Gynaecology Canada 36:527–553.
- Colmorn LB, Ladelund S, Rasmussen S, Secher NJ. 2014. Risk of a venous thromboembolic episode due to caesarean section and BMI: a study in northern Denmark covering 2000–2010. Journal of Obstetrics and Gynaecology 34:313–316.
- Department of Statistics. 2011. Population distribution and basic demographic characteristic report 2010; [cited 2016 Nov 26]. Available from: http://<www.dosm.gov.my
- Fausett MB, Vogtlander M, Lee RM, Esplin MS, Branch DW, Rogers GM, et al. 2001. Heparin-induced thrombocytopenia is rare in pregnancy. American Journal of Obstetrics and Gynecology 185:148–152.
- Hasegawa J, Sekizawa A, Tanaka H, Katsuragi S, Osato K, Murkoshi T, et al. 2016. Current status of pregnancy-related maternal mortality in Japan: a report from the Maternal Death Exploratory Committee in Japan. BMJ Open 6:e010304.
- Heit JA, Kobbervig CE, James AH, Petterson TM, Bailey KR, Melton IIILJ. 2005. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-year population-based study. Annals of Internal Medicine 143:697–706.
- Institute for Public Health. 2015. National Health and Morbidity Survey 2015. Non-communicable disease, risk factors & other health problems: Volume II; [cited 2017 Mar 22]. Available from: http://www.iku.gov.my/images/IKU/Document/REPORT/nhmsreport2015vol2.pdf
- Jacobsen AF, Skjeldestad FE, Sandset PM. 2008. Ante- and postnatal risk factors of venous thrombosis: a hospital-based case-control study. Journal of Thrombosis and Haemostasis 6:905–912.
- James AH, Jamison MG, Brancazio LR, Myers ER. 2006. Venous thromboembolism during pregnancy and the postpartum period: incidence, risk factors, and mortality. American Journal of Obstetrics and Gynecology 194:1311–1315.
- Kutuk MS, Terzioglu A, Ozgun MT, Uludag S, Dolanbay M, Tas M. 2014. A critical analysis of low molecular weight heparin use during pregnancy in a tertiary referral centre. Journal of Obstetrics and Gynaecology 34:131–134.
- Ministry of Health Malaysia, Division of Family Health Development. 2013. Report on the Confidential Enquiries into Maternal Deaths in Malaysia 2006–8; [cited 2016 Nov 26]. Available from: http://www.ogsm.org.my/docs/CEMD-report-2006-2008.pdf
- Nelson-Piercy C. 2015. Prevention and treatment of thrombosis and thromboembolism. In: Knight M, Tuffnell D, Kenyon S, Shakespeare J, Gray R, Kurinczuk JJ, editors. Saving Lives, Improving Mothers’ Care—Surveillance of maternal deaths in the UK 2011–13 and lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2009–2013. Oxford: National Perinatal Epidemiology Unit. p. 43–52.
- Revell BJ, Smith RP. 2011. Thrombosis and thromboembolism in pregnancy and the puerperium, reducing the risk: what proportion of patients reach the threshold for thromboprophylaxis? Obstetric Medicine: The Medicine of Pregnancy 4:12–14.
- Royal College of Obstetricians and Gynaecologists. 2015. Reducing the Risk of Venous Thromboembolism during Pregnancy and the Puerperium; [cited 2016 Aug 31]. Available from: http://<www.rcog.org.uk/en/guideline-research-services/guidelines
- Shagar LK. 2016. Hindu groups want vaccines without beef gelatine. The Star; [cited 2016 Nov 16]. Available from: http://www.thestar.com.my/news/nation/2016/07/28/hindu-groups-want-vaccines-without-beef-gelatine
- Sarawak State Health Department, Division of Family Health. 2013. Extracted from the Confidential Enquiry into Maternal Deaths in the State of Sarawak, 2010–2012.
- Sultan AA, Tata LJ, West J, Fiaschi L, Fleming KM, Nelson-Piercy C, et al. 2013. Risk factors for first venous thromboembolism around pregnancy: a population-based cohort study from the United Kingdom. Blood 121:3953–3961.
- Tepper NK, Boulet SL, Whiteman MK, Monsour M, Marchbanks PA, Hooper WC, et al. 2014. Postpartum venous thromboembolism: incidence and risk factors. Obstetrics and Gynecology 123:987–996.
- The American College of Obstetricians and Gynecologists. 2011. Thromboembolism in Pregnancy. Practice Bulletin Number 123. Obstetrics and Gynecology 118:718–729.
- Won HS, Kim DY, Yang MS, Lee SJ, Shin HH, Park JB. 2011. Pregnancy induced hypertension but not gestational diabetes mellitus, is a risk factor for venous thromboembolism in pregnancy. Korean Circulation Journal 41:23–27.