

Abstract
The prediction of successful labour induction is difficult, indicating a need for a biomarker test. Little is known about the effect of Foley catheter (FC) induction on biochemical mediators in the cervix, such as the insulin-like growth factor binding protein-1 (IGFBP-1), matrix metalloproteinases (MMP) and their inhibitors (TIMP). We enrolled 35 nulliparous women with singleton pregnancies, intact amniotic membranes and cephalic presentation ≥40 gestational weeks scheduled for labour induction by FC. Serial cervical swab samples were collected at FC insertion and expulsion. The concentrations of IGFBP-1, PhIGFBP-1, MMP-8, MMP-2, MMP-9, TIMP-1 and TIMP-2 were analysed. The IGFBP-1 and phIGFBP-1 concentrations increased during the FC-induced cervical ripening. In contrast, MMP-8 and MMP-9 concentrations decreased. However, these changes did not predict the outcome of the labour induction, thus appearing not suitable for clinical use.
What is already known on this subject? During cervical ripening, various constituents interact in a complex network. Insulin-like growth factor binding protein-1 (IGFBP-1), matrix metalloproteinases (MMP) and their tissue inhibitors (TIMP) appear to play a role in cervical ripening. The mechanism of Foley catheter on cervical ripening consists of direct mechanical stretching of the cervix and lower uterine segment, and the stimulation of local secretion of endogenous prostaglandins.
What do the results of this study add? This study investigated the role of cervical biochemical mediators during Foley catheter-induced cervical ripening, and their predictive value in a successful labour induction and vaginal delivery. The IGFBP-1 and phosphorylated IGFBP-1 concentrations increased, whereas MMP-8 and MMP-9 concentrations decreased during the Foley catheter-induced cervical ripening in nulliparous women. However, these changes did not predict the outcome of labour induction, thus appearing not suitable for clinical use.
What are the implications of these findings for clinical practice and/or further research? Prediction of a successful labour induction is difficult, indicating a need for a biomarker test. Future studies with larger data are needed for investigating the role of these cervical biomarkers in successful labour induction, and in developing a future bedside a screening tool for clinical use.
Impact statement
Introduction
Induction of labour (IOL) is a common obstetric procedure. However, prediction of successful labour induction is difficult on the basis of maternal characteristics, the Bishop score or transvaginal ultrasonography of the cervix (Crane Citation2006). During cervical ripening, various constituents, such as hyaluronic acid, cytokines and inflammatory mediators appear to interact in a complex network (Aalberts et al. Citation2007). The mechanism of Foley catheter (FC) on cervical ripening consists of direct mechanical stretching of the cervix and lower uterine segment combined with the stimulation of local secretion of endogenous prostaglandins (Manabe et al. Citation1982). Little is known of the effect of FC on the biochemical mediators in the cervix.
Insulin-like growth factor binding protein-1 (IGFBP-1), synthesised by the foetal and maternal liver and decidua, increases during pregnancy (Rutanen et al. Citation1982). The non-phosphorylated isoform of IGFBP-1 is a major protein in the amniotic fluid from the second trimester onwards, while the decidual cells secrete predominantly the phosphorylated isoforms (phIGFBP-1) (Westwood et al. Citation1994). The concentration of phIGFBP-1 reflects cervical ripeness and increases during the cervical ripening with prostaglandins (Nuutila et al. Citation1999).
Matrix metalloproteinases (MMPs) are genetically distinct but are structurally related endopeptidases with many functions, including the remodelling and degradation of the extracellular matrix and non-matrix bioactive substrates (Weiss et al. Citation2007). The proteolytic activity of MMPs is inhibited by the tissue inhibitors of metalloproteinases (TIMPs) (Brew and Nagase Citation2010). Several MMPs (-1, -2, -3, -7, -8 and -9) and TIMP-1 and -2 are found in the foetal membranes during gestation (Weiss et al. Citation2007). MMPs are important mediators in the pathological processes resulting in preterm labour but they also appear to play a role in the initiation of labour at term. Especially MMP-8, -9, and TIMP-1 and -2 seem to be involved in cervical ripening (Sennstrom et al. Citation2003; Heng et al. Citation2012).
The aim of the study was to evaluate changes in cervical biochemical mediators IGFBP-1, phIGFBP-1, MMPs-2, -8, -9, TIMP-1 and -2 during FC-induced cervical ripening in nulliparous women. We also wanted to analyse these biomarkers in relation to the outcome of labour induction.
Materials and methods
This prospective study was conducted at the Department of Obstetrics and Gynaecology of Helsinki University Hospital between September 2014 and June 2015. The study protocol was approved by the Helsinki and Uusimaa Hospital District ethic committee (Nr. 268/13/03/03/2012). The approval to carry out the study was granted by the Hospital district of Helsinki and Uusimaa (§41/17.10.2012). Written informed consent was obtained from all women.
Participants
We enrolled pregnant nulliparous women with gestational age of ≥40+0 weeks, cephalic presentation, intact amniotic membranes, obstetric indication for IOL, reassuring foetal cardiotocography and an unripe cervix with a Bishop Score <6 (Bishop Citation1964) at the time of admission. The duration of pregnancy was defined by the foetal crown-rump length measurement performed at the time of the first trimester ultrasound screening. Women with hypertensive disorders, pre-eclampsia, foetal growth restriction, vaginal bleeding, any symptom or sign of infection, HIV and hepatitis-B or -C were excluded from the study. None of the participants had regular contractions or any evidence of rupture of membranes at the time of enrolment. The same physician (HK) examined all women, collected all samples and managed the FC procedure.
Cervical samples
Before insertion of the FC, four swab samples were collected by inserting a sterile swab into the cervical canal and rotating it for 15 s during speculum examination. The swabs were then each swirled in their respective extraction solution for 15 s. The sample solutions were frozen and stored at −20 °C until the analysis of IGFBP-1, phIGFBP-1, MMP-2, MMP-8, MMP-9, TIMP-1 and TIMP-2 concentrations. After expulsion of the FC, four serial swab samples were again collected as described earlier. The samples were obtained by the same obstetrician with a maximum delay of 10 min before insertion and after expulsion of the FC. All samples were analysed in the same laboratory (Medix Biochemica, Espoo, Finland), which was blinded to the clinical status and the outcome of labour induction.
Analysis of IGFBP-1 and phIGFBP-1 by immunoenzymometric assays
The concentrations of cervical IGFBP-1 and phIGFBP-1 were measured by two immunoenzymometric assays using monoclonal antibodies (Medix Biochemica, Espoo, Finland). The IGFBP-1 assay employing monoclonal antibody 6305 detects the non-phosphorylated and less phosphorylated isoforms of IGFBP-1, while phIGFBP-1 assay employing monoclonal antibody 6303 recognises the highly phosphorylated forms (Nuutila et al. Citation1999). The detection limit of both the assays was 0.3 µg/L. All samples were measured in duplicates.
Analysis of MMP-8 by immunoenzymometric assay
MMP-8 was quantitated with a solid-phase immunoenzymometric assay (MMP-8 IEMA, Medix Biochemica, Espoo, Finland) (Nieminen et al. Citation2015). This sandwich assay uses two monoclonal antibodies against human MMP-8. Microplate wells were coated with one monoclonal antibody against MMP-8. The other antibody was conjugated to HRP forming the enzyme conjugate used to detect the presence of MMP-8. The analyses were performed according to the manufacturer’s instructions, and the absorbance of the solutions in the wells was measured at 414 nm using a microplate reader (Multiskan, Thermo Fisher Scientific, Vantaa, Finland).
Analysis of MMP-2, -9, TIMP-1 and -2 by ELISA
MMP-2 and MMP-9 analyses were carried out by using commercially available ELISA kits (Biotrak ELISA Systems; GE Healthcare Life Sciences for MMP-2 and TIMP-1, and Quantikine ELISA Kit; R and D Systems for MMP-9 and TIMP-2) according to the manufacturer’s instructions. The balance between the quantities of MMP-8 and TIMP-1 was roughly estimated from our data on the basis of the molar ratio.
Foley catheter insertion
A single balloon catheter (Rüsch 2-way Foley, Couvelaire tip, catheter size 22 Ch, Teleflex Medical, Athlone, Ireland) was introduced through the endocervix during speculum examination. The balloon was inflated with 50 mL of saline, a light traction was applied so that the balloon rested on the internal os, and the catheter was taped to the inner thigh. A transvaginal ultrasound was performed to assure balloon placement. The status was monitored every two hours for vaginal expulsion, and light traction was reapplied if necessary. After a spontaneous expulsion of the balloon, amniotomy was performed if the Bishop score was ≥6, and the induction was continued with oxytocin if spontaneous contractions did not occur. If the Bishop score remained <6 after the balloon expulsion, cervical ripening was continued according to the hospital management guidelines, using misoprostol 25 µg vaginally or 50 µg orally every 4 h until the Bishop score was ≥6.
Outcomes
The data on the study population characteristics and outcomes were obtained from the hospital records. Labour arrest in the first stage of labour was defined as a failure to progress despite ruptured membranes and a minimum of 4 h of adequate uterine activity without a cervical change (Caughey et al. Citation2014). A failed induction was diagnosed after ruptured membranes and 12 h of oxytocin administration without a cervical change (Caughey et al. Citation2014). The induction-to-delivery interval was defined as the time from insertion of the FC to delivery.
Statistical analysis
All calculations were carried out using the Microsoft Statistical Package for Social Sciences (SPSS Inc., Chicago, IL) for Windows v18.0. Categorical variables were compared with a Chi-square test and Fisher’s exact test when appropriate. The continuous variables were assessed with a T-test when the data was normally distributed, and with a Mann–Whitney U test if the data did not follow a normal distribution. The correlations between the cervical biomarker concentrations (at FC insertion, at FC expulsion, and the change in concentration) and the labour outcomes were analysed using Pearson’s correlation coefficient. A p value of < .05 was considered as significant.
Results
A total of 35 nulliparous women were enrolled. One woman was excluded due to the rupture of membranes after insertion of the FC. The characteristics and obstetric outcomes of the study population are shown in . Half of the women (n = 17) had Bishop Score ≤3 at the start of IOL (). The main indication for IOL was post-term pregnancy (79.4%) (). The mean (SD) time from FC insertion to expulsion was 255 (±169) minutes, with the range of 1.5–18.2 h. The mean (SD) induction-to-delivery interval was 1681 (±802) min.
Table 1. Patient characteristics and obstetric outcomes.
shows the baseline concentrations of the cervical biomarkers. The median IGFBP-1 and phIGFBP-1 concentrations increased (from 1.8 to 23.5 µg/L; p = .008 and from 5.5 to 75.5 µg/L; p = .001, respectively), and the MMP-8 and MMP-9 concentrations decreased (from 446.0 to 230.0 µg/L; p < .001 and from 431.5 to 178.4 µg/L; p < .001, respectively) during the FC-induced cervical ripening ( and ). The mean MMP-2 concentration at the start of IOL was low and did not change (). The concentrations of TIMP-1 did not significantly change, whereas the concentrations of TIMP-2 decreased (from 9.3 to 5.6 µg/L; p = .02) during the FC ripening ().
Figure 1. Cervical IGFBP-1 and phIGFBP-1 concentrations increase during Foley catheter cervical ripening.
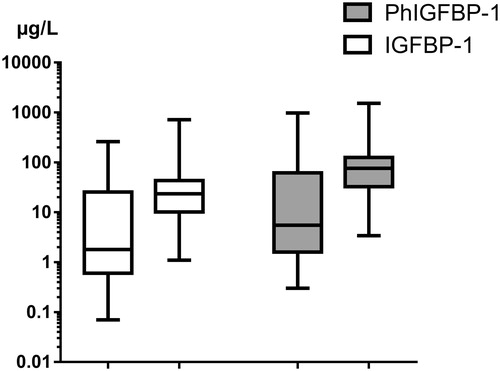
Figure 2. Cervical MMP-8 and MMP-9 concentrations decrease during Foley catheter cervical ripening. MMP-2 concentration does not significantly change.
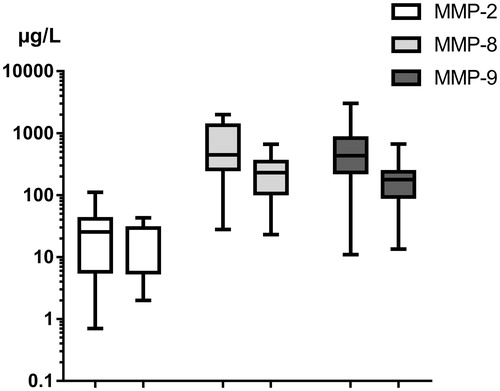
Figure 3. Cervical TIMP-1 concentration does not significantly change, whereas TIMP-2 concentration decreases during Foley catheter cervical ripening.
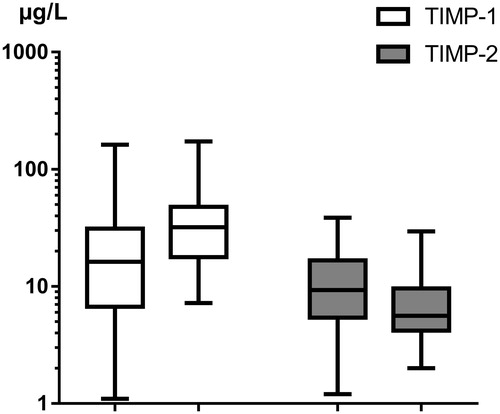
Table 2. The baseline concentrations (µg/l) of the cervical biomarkers prior to Fc insertion.
Of the cervical biomarkers, only MMP-8 differed between the women with Bishop Scores of ≤3 and >3 at the start of IOL (593.0 [41–1998] vs. 408 [28–1335] µg/L [median [range]]; p = .02). Also, the concentration of MMP-8 decreased more in the women with a Bishop score <3, compared with the women having Bishop score of 4–6 (443.0 [346–1834] vs. 209.0 [293–1001] µg/L [median [range]]; p = .01). The six (17.6%) women whose Bishop score remained <6 after an FC expulsion had similar biomarker concentrations compared to the 28 women with a successful FC ripening.
The median (range) concentrations of IGFBP-1 and phIGFBP-1 increased more in women who started having spontaneous contractions compared to the women who needed oxytocin induction (15.4 [−61.0 to 716.7] vs. 9.5 [−195.0 to 70.7] µg/L; p = .02 for IGFBp-1 and 30.8 [−162.0 to 1527.1] vs. 24.5 [−843.0 to 187.0] µg/L; p = .05). When comparing the mode of delivery, no significant differences in the baseline concentrations of the cervical biomarkers were observed between the women with a vaginal delivery and the women who delivered by caesarean section due to a failure to progress ().
Table 3. The cervical biomarker concentrations at FC insertion and labour outcomes.
Discussion
Our results suggest that IGFBP-1, phIGFBP-1, MMP-8, MMP-9 and TIMP-2 are involved in the process of cervical ripening induced by FC. We studied only nulliparous women, since the concentrations of phIGFBP-1 and MMP-8 differ between nulliparous and multiparous women (Rahkonen et al. Citation2009a, Citation2009b). Almost 80% of the women were post-term with half of the women having Bishop score ≤3 at the start of IOL. The CS rate in our study was high, but similar rates in post-term nulliparous women with an unfavourable cervix have been reported by several previous studies (Frederiks et al. Citation2012; Marroquin et al. Citation2013; Kruit et al. Citation2015). A recent study suggested that cell-free foetal DNA may initiate the process of cervical ripening and labour (Phillippe Citation2014). However, the exact mechanism and biochemical mediators are yet to be uncovered. Cervical ripening is characterised by a leucocyte infiltration and the remodelling of extracellular matrix proteins, such as collagen (Riskin-Mashiah and Wilkins Citation1999). A study of cervical mucus plugs in 17 women during active labour reported a large quantity of MMP-2, MMP-8, MMP-9, and their inhibitors TIMP-1 and TIMP-2 in the cervical mucus (Becher et al. Citation2004). The proteolytic or non-proteolytic effects of MMPs and TIMPs in the cervical mucus may include a degradation of local extracellular matrix components thereby enhancing a cervical softening and affecting the overlying cervical membranes. Hyaluronic acid in the extracellular matrix may also play a role, resulting in cervical softening and swelling (Hascall et al. Citation2004). The mechanism of Foley catheter on cervical ripening constitutes direct mechanical stretching of the cervix and lower uterine segment, and stimulation of endogenous prostaglandin release by stripping the foetal membranes (Manabe et al. Citation1982; Keirse et al. Citation1983). Mechanically stretching the cervix during parturition has also been shown to augment the production of hyaluronic acid in uterine cervical fibroblast cells (Takemura et al. Citation2005).
Nuutila et al. (Citation1999) found a higher IGFBP-1 concentrations in women with a ripe cervix (Bishop Score >6) compared with women having an unripe cervix. In our study, only women with an unripe cervix were included. The study by Nuutila et al. (Citation1999) also demonstrated an increase in cervical IGFBP-1 concentration after application of prostaglandin E2 gel for cervical ripening. A similar increase in cervical IGFBP-1 and phIGFBP-1 following cervical ripening by FC was seen in our study. However, the cervical IGFBP-1 concentrations did not predict induction to delivery interval, as also seen in the previous study (Nuutila et al. Citation1999). In a recent study by Kosinska-Kaczynska et al. (Citation2015), the presence of cervical phIGFBP-1 predicted spontaneous onset of labour and successful vaginal delivery in term and post-term pregnancies. This was not seen in our study, since the IGFBP-1 and phIGFBP-1 concentrations did not differ between women who delivered vaginally and those who delivered by caesarean section due to failure to progress. In Kosinska-Kaczynska’s study, women with the positive phIGFBP-1 test also developed regular uterine contractions earlier after cervical ripening (Kosinska-Kaczynska et al. Citation2015). A similar trend was also seen in our study, in which the IGFBP-1 and phIGFBP-1 increased more in women who started having spontaneous contractions following the FC ripening.
The concentrations of MMP-8 and MMP-9 are higher in term women with labour compared with women not in labour (Dubicke et al. Citation2008). A recent study of 18 cervical samples, collected by an extra-amniotic irrigation or cervical biopsy, concluded that FC may induce cervical ripening through changes in biochemical mediators (Lim et al. Citation2013). MMP-8 expression was higher in the women with a spontaneous onset of labour, and after expulsion of FC, when compared with the non-pregnant women or the women before FC insertion at term (Lim et al. Citation2013). Also, the concentrations of MMP-8 increased over time during the FC ripening (Lim et al. Citation2013). However, the sample size was smaller and their sampling method differed from ours. In contrast, in our study the MMP-8 concentration decreased during the FC-induced ripening. Surprisingly, MMP-8 concentration was higher in women with less ripe (Bishop Score ≤3) cervices at start of IOL, and the decrease was greater during cervical ripening. MMP-8 and MMP-9 deficient mouse models and human studies have revealed that physiological MMP-8 and -9 levels, modifying extracellular matrix and immune responses, have destructive and defensive effects (Sorsa et al. Citation2006; Saarinen et al. Citation2016). The decreased MMP-8 and -9 concentrations recorded here may reflect a reduced defensive potential associated with a labour induction by FC.
The activities of the metalloproteinases are highly dependent on the interaction and balance with the TIMPs. TIMP-1 and TIMP-2 significantly increase in spontaneous labour (Heng et al. Citation2012). An increase of TIMP-1 concentrations in cervical tissue with progressive cervical dilatation (from 2 cm to 6 cm) during labour has previously been observed (Winkler and Rath Citation1999). In our study, the TIMP-1 concentrations were low and did not significantly change during the FC ripening, whereas the TIMP-2 concentrations decreased. This may reflect the homeostatic regulation of extracellular matrix remodelling by TIMP-1 and TIMP-2 (Heng et al. Citation2012). Nevertheless, TIMPs exert growth-factor-like properties independent of an MMP-inhibition (Chirco et al. Citation2006; Stetler-Stevenson Citation2008).
The major limitations of the study are the relatively small number of patients and the lack of power analysis. Also, there may have been inter-individual biological variation reflected in the cervical concentrations of IGFBP-1, phIGFBP-1, MMPs and TIMPs, differences in the bacterial flora of the upper vagina, and differences of cellularity of the cervical mucus. Although samples were collected by the same person, there may have been variation in extraction from the swab into the sample buffer which may have influenced the concentrations. Another weakness of the study are the ACOG definitions used for failed induction and labour arrest in the first stage of labour. These definitions were accurate during the research undertaken, but are no longer up-to-date. The main strength of this study is the well-defined patient group with a uniform dating of pregnancy by the first trimester ultrasound. Also, the sampling technique, determination of cervical status, and management of the FC cervical ripening were standardised and performed by the same obstetrician.
In conclusion, the data indicates an increase in the IGFBP-1 and phIGFBP-1 concentrations, and a decrease in MMP-8, MMP-9 and TIMP-2 concentrations in the cervix during an FC-induced ripening in nulliparous women. However, these cervical biomarkers appear not suitable for clinical use in predicting the outcome of labour induction.
Acknowledgements
We thank Ms. Irina Mats from Medix Biochemica, Espoo, Finland, for the analyses of the cervical samples.
Disclosure statement
The authors report no declarations of interest.
Additional information
Funding
References
- Aalberts M, Van Dissel-Emiliani FM, van Tol HT, Taverne MA, Breeveld-Dwarkasing VN. 2007. High iNOS mRNA and protein levels during early third trimester suggest a role for NO in prelabor cervical ripening in the bovine. Molecular Reproduction and Development 74:378–385.
- Caughey AB, Cahill AG, Guise JM, Rouse DJ, American College of Obstetricians and Gynecologists, Society for Maternal-Fetal Medicine. 2014. Safe prevention of the primary cesarean delivery. American Journal of Obstetrics and Gynecology 210:179–193.
- Becher N, Hein M, Danielsen CC, Uldbjerg N. 2004. Matrix metalloproteinases and their inhibitors in the cervical mucus plug at term of pregnancy. American Journal of Obstetrics and Gynecology 191:1232–1239.
- Bishop EH. 1964. Pelvic scoring for elective induction. Obstetrics and Gynecology 24:266–268.
- Brew K, Nagase H. 2010. The tissue inhibitors of metalloproteinases (TIMPs): an ancient family with structural and functional diversity. Biochimica Et Biophysica Acta 1803:55–71.
- Chirco R, Liu XW, Jung KK, Kim HR. 2006. Novel functions of TIMPs in cell signaling. Cancer Metastasis Reviews 25:99–113.
- Crane JM. 2006. Factors predicting labor induction success: a critical analysis. Clinical Obstetrics and Gynecology 49:573–584.
- Dubicke A, Akerud A, Sennstrom M, Hamad RR, Bystrom B, Malmstrom A, et al. 2008. Different secretion patterns of matrix metalloproteinases and IL-8 and effect of corticotropin-releasing hormone in preterm and term cervical fibroblasts. Molecular Human Reproduction 14:641–647.
- Frederiks F, Lee S, Dekker G. 2012. Risk factors for failed induction in nulliparous women. The Journal of Maternal-Fetal and Neonatal Medicine 25:2479–2487.
- Hascall VC, Majors AK, De La Motte CA, Evanko SP, Wang A, Drazba JA, et al. 2004. Intracellular hyaluronan: a new frontier for inflammation? Biochimica Et Biophysica Acta 1673:3–12.
- Heng YJ, Di Quinzio MK, Liong S, Permezel M, Rice GE, Georgiou HM. 2012. Temporal investigation of matrix metalloproteinases and their inhibitors in human cervicovaginal fluid in late pregnancy and labor. Reproductive Sciences 19:55–63.
- Keirse MJ, Thiery M, Parewijck W, Mitchell MD. 1983. Chronic stimulation of uterine prostaglandin synthesis during cervical ripening before the onset of labor. Prostaglandins 25:671–682.
- Kosinska-Kaczynska K, Bomba-Opon D, Bobrowska K, Kozlowski S, Brawura-Biskupski-Samaha R, et al. 2015. Phosphorylated IGFBP-1 in predicting successful vaginal delivery in post-term pregnancy. Archives of Gynecology and Obstetrics 292:45–52.
- Kruit H, Heikinheimo O, Ulander VM, Aitokallio-Tallberg A, Nupponen I, Paavonen J, et al. 2015. Management of Foley catheter induction among nulliparous women: a retrospective study. BMC Pregnancy and Childbirth 15:276-015-0715-9.
- Lim SY, Kim YH, Kim CH, Cho MK, Kim JW, Kang WD, et al. 2013. The effect of a Foley catheter balloon on cervical ripening. Journal of Obstetrics and Gynaecology: The Journal of the Institute of Obstetrics and Gynaecology 33:830–838.
- Manabe Y, Manabe A, Takahashi A. 1982. F prostaglandin levels in amniotic fluid during balloon-induced cervical softening and labor at term. Prostaglandins 23:247–256.
- Marroquin GA, Tudorica N, Salafia CM, Hecht R, Mikhail M. 2013. Induction of labor at 41 weeks of pregnancy among primiparas with an unfavorable bishop score. Archives of Gynecology and Obstetrics 288:989–993.
- Nieminen MT, Vesterinen P, Tervahartiala T, Kormi I, Sinisalo J, Pussinen PJ, et al. 2015. Practical implications of novel serum ELISA-assay for matrix metalloproteinase-8 in acute cardiac diagnostics. Acute Cardiac Care 17:46–47.
- Nuutila M, Hiilesmaa V, Karkkainen T, Ylikorkala O, Rutanen EM. 1999. Phosphorylated isoforms of insulin-like growth factor binding protein-1 in the cervix as a predictor of cervical ripeness. Obstetrics and Gynecology 94:243–249.
- Phillippe M. 2014. Cell-free fetal DNA–a trigger for parturition. The New England Journal of Medicine 370:2534–2536.
- Rahkonen L, Rutanen EM, Unkila-Kallio L, Nuutila M, Nieminen P, Sorsa T, et al. 2009a. Factors affecting matrix metalloproteinase-8 levels in the vaginal and cervical fluids in the first and second trimester of pregnancy. Human Reproduction 24:2693–2702.
- Rahkonen L, Unkila-Kallio L, Rutanen EM, Paavonen J. 2009b. Factors affecting decidual IGFBP-1 levels in the vagina and cervix in the first and mid-second trimester of pregnancy. BJOG: An International Journal of Obstetrics and Gynaecology 116:45–54.
- Riskin-Mashiah S, Wilkins I. 1999. Cervical ripening. Obstetrics and Gynecology Clinics of North America 26:243–257.
- Rutanen EM, Bohn H, Seppala M. 1982. Radioimmunoassay of placental protein 12: levels in amniotic fluid, cord blood, and serum of healthy adults, pregnant women, and patients with trophoblastic disease. American Journal of Obstetrics and Gynecology 144:460–463.
- Saarinen R, Pitkaranta A, Kolho KL, Tervahartiala T, Sorsa T, Lauhio A. 2016. Decreased salivary matrix metalloproteinase-8 reflecting a defensive potential in juvenile parotitis. International Journal of Pediatric Otorhinolaryngology 80:74–77.
- Sennstrom MB, Brauner A, Bystrom B, Malmstrom A, Ekman G. 2003. Matrix metalloproteinase-8 correlates with the cervical ripening process in humans. Acta Obstetricia Et Gynecologica Scandinavica 82:904–911.
- Sorsa T, Tjaderhane L, Konttinen YT, Lauhio A, Salo T, Lee HM, et al. 2006. Matrix metalloproteinases: contribution to pathogenesis, diagnosis and treatment of periodontal inflammation. Annals of Medicine 38:306–321.
- Stetler-Stevenson WG. 2008. Tissue inhibitors of metalloproteinases in cell signaling: metalloproteinase-independent biological activities. Science Signaling 1:re6
- Takemura M, Itoh H, Sagawa N, Yura S, Korita D, Kakui K, et al. 2005. Cyclic mechanical stretch augments hyaluronan production in cultured human uterine cervical fibroblast cells. Molecular Human Reproduction 11:659–665.
- Weiss A, Goldman S, Shalev E. 2007. The matrix metalloproteinases (MMPs) in the decidua and fetal membranes. Frontiers in Bioscience 12:649–659.
- Westwood M, Gibson JM, Davies AJ, Young RJ, White A. 1994. The phosphorylation pattern of insulin-like growth factor-binding protein-1 in normal plasma is different from that in amniotic fluid and changes during pregnancy. The Journal of Clinical Endocrinology and Metabolism 79:1735–1741.
- Winkler M, Rath W. 1999. Changes in the cervical extracellular matrix during pregnancy and parturition. Journal of Perinatal Medicine 27:45–60.