

Abstract
The decrease in pH in monochorionic (MC) second twin may exceed that of dichorionic (DC) second twin during vaginal twin delivery. The aim of this study was to investigate the effect of chorionicity on the umbilical artery pH of the second twin in relation to increased twin-to-twin delivery time interval (DTI) from 30 weeks of gestation. A hospital based cohort of all twin deliveries after 30 completed weeks of gestation with the first twin delivered vaginally between 2007 and 2012 in four delivery units in Stockholm county was conducted. The changes of umbilical pH in MC twins compared to DC twins in relation to twin-to-twin DTI was studied using linear regression. The predictors for acidosis (pH ≤ 7.10) in the second twin were studied by logistic regression. The cohort included 681 DC and 186 MC twin pairs. There was a correlation between the umbilical pH and the twin-to-twin DTI but independent of the chorionicity, the pH decreased in average by 0.0012 units/min (p < .001). Twin-to twin DTI was a predictor for acidosis of the second twin (p < .01).
What is already known on this subject? Vaginal twin deliveries are a major obstetrical challenge because of the increased risk for the second twin after the delivery of the first twin, and are suggested to increase among premature second twins. Previous studies report a continuous decline in the pH of the second twin during the second stage of labour, with an increased risk for acidosis (pH < 7.10) and Apgar scores <7 for twin-to-twin delivery time interval (DTI) as short as 15–30 min. Major studies have not discriminated between MC and DC vaginally delivered twins and the question rise if there is a reason for different delivery guidelines for MC diamniotic second twin compared to DC second twin.
What do the results of this study add? The results of the present study show a correlation between umbilical pH and twin-to-twin DTI, but independent of chorionicity, from gestational week 30 to term. A main predictor for acidosis (pH ≤ 7.10) is the twin-to-twin DTI.
What are the implications of these findings for clinical practice and/or future research? In cases of uneventful MC pregnancies, we find no support to suggest different vaginal delivery guidelines for MC diamniotic twins compared to DC twins. The risk for acidosis in the second twin increased with 1%/min during the second stage. Active management may be recommended after 15–30 min.
IMPACT STATEMENT
Introduction
Vaginal twin deliveries are a major obstetrical challenge because of the increased risk for the second twin after delivery of the first twin. Thus, the second twin is at an increased risk for foetal distress and low Apgar scores, and is suggested to increase among premature second twins (Thorngren-Jerneck and Herbst Citation2001; Hartley and Hitti Citation2005; Herbst and Källén Citation2008). Several investigators have reported a continuous decline in the pH of the second twin during the second stage of labour (Tak-Yeung et al. Citation2002; Tak-Yeung et al. Citation2004; Caprice and David Citation2005; Suh et al. Citation2007; Stein et al. Citation2008), with an increased risk for acidosis (pH < 7.10) and Apgar scores <7 at 1, 5 and 10 min for a twin-to-twin delivery time interval (DTI) as short as 15–30 min. (Hartley and Hitti Citation2005; Stein et al. Citation2008). Major available published studies have not discriminated between monochorionic (MC) and dichorionic (DC) vaginally delivered twins when examining the relationship between umbilical pH and twin-to-twin DTI. However, a recent study found no effect of chorionicity and twin-to-twin DTI on the short-term outcome of second twin after 36 weeks of gestation (Hjortø et al. Citation2014). But there is a risk for substantial bias, as a higher incidence of complications during pregnancy are probably to be found in MC twins and the problematic ones are possibly selected for caesarean section (Ylilehto et al. Citation2017). A higher prevalence of preterm delivery, severe birthweight discordance (>20%), twin-to-twin transfusion syndrome and stillbirths has been found in MC twins (Hoffman et al. Citation2012). Vaginal delivered preterm MC second twin may be at an increased risk compared to DC preterm second twin, a difference that may diminishes towards term, as foetuses at risk are already sorted out (Joseph and Kramer Citation2017). A stated hypothesis is that the decrease in pH in MC second twin may exceed that of DC second twin, which was not confirmed in vaginally delivered twin pregnancies at term (Hjortø et al. Citation2014). The aim of the present study was to investigate the effect of chorionicity on umbilical pH in relation to increasing twin-to-twin DTI from 30 weeks of gestation and compare the outcome before and after 34 weeks of gestation. The predictors for acidosis in the second twin were also calculated.
Materials and methods
We conducted a retrospective hospital based cohort analysis of all twin deliveries in Stockholm born after 30 completed weeks of gestation, with the first twin born vaginally, between 1 January 2007 and 31 August 2012. The pregnancies excluded were <30 weeks of gestation, the first twin born by caesarean section and those with the intrauterine death of either one of the twins. The data was obtained from four obstetric departments using the same clinical protocol for monitoring twin pregancies and deliveries (Karolinska University Hospital Huddinge, Karolinska University Hospital Solna, Danderyd Hospital and Stockholm South General Hospital). A computerised obstetric database (Obstetrix®) was used. The data collected included the maternal age, gestational length, preeclampsia, chorionicity, twin-to-twin DTI, presentation of second twin, birthweight, small for gestational age (SGA, <5 percentile according to Swedish standard), umbilical pH at birth, base excess, an Apgar score of <7 at 5 min, admission to NICU secondary to asphyxia (based on diagnosis according to ICD-10), assisted vaginal delivery (vacuum extraction, forceps delivery, or extracted breech) and the caesarean section of the second twin.
The gestational age at birth was determined in the completed weeks of gestation based on the ultrasound estimated delivery date. Dichorionicity was determined with the presence of the lambda-sign on the ultrasound examination, the heterogeneous sex of the children, or the medical text where the ultrasound data was missing in the database. Monochorionicity was determined with the T-sign on ultrasound examination or by the medical text. The twin-to-twin DTI was defined as the delivery interval in minutes between the birth of the first and second twin. Acidosis was determined as a pH ≤7.10. For those children where only the pH from the umbilical vein was registered (n = 72), we withdrew 0.03 from the pH value to get an estimated arterial value (Westgate et al. Citation1994; Wiberg et al. Citation2010).
Statistical analysis
The data is given as the mean ± the standard deviation, the median (min. – max.) or the numbers as appropriate. The univariate analysis was conducted using the Chi-square test for the categorical variables and independent samples t-test or the Mann-Whitney U test for the continuous variables according to distribution. The multivariate analysis was conducted for the predictors of acidosis. The linear regression model was used to determine the relationship between DTI and umbilical pH at birth. The paired sampled t-test was used when comparing the short-time outcome of the first versus the second twin to test the expected worse outcome of the second twin. The P values of < .05 were considered statistically significant. Statistica© was used for the statistical analysis of all data. Ethical approval was given by the local ethics committee of Stockholm, Sweden (D:nr 2013/1586-31/2).
Results
Of a total of 2,170 twin deliveries during the study period, 867 twins with 1,734 children met the inclusion criteria. Six hundred and eighty-one (79%) were DC and 186 (21%) MC. There were 13 cases of unknown chorionicity. Of the vaginally delivered twin-pairs, 56 twin-pairs were excluded due to a gestational age <30 weeks or an intrauterine fetal death of one or both twins. There were no intrapartum deaths. Eighty-six (1%) first twins and 69 (0.8%) second twins had an unknown umbilical pH. Two second twins had an unknown Apgar at 5 min.
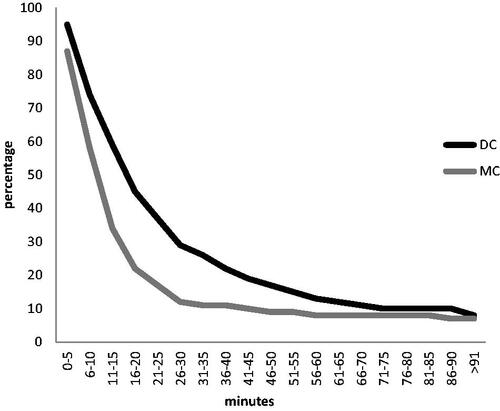
The median twin-to-twin DTI in the whole study group was 16 (1–266) minutes. The DTI was somewhat shorter for the MC second twins (12 [1–106] min) compared to DC second twins (17 [2–266] min, p < .001). illustrates the percentage of undelivered DC and MC twins per 5 min intervals. The DTI was slightly shorter for twins born <34 weeks (12.5 [2–69] min) compared to those born >34 weeks (16 [1–266] min, p < .05). However, the DTI did not differ between MC and DC second twin below 34 weeks (12 [2–22] vs. 13 [3–69] min.).
Figure 1. Undelivered second twins over time (percent), categorised by MC/DC.
shows maternal characteristics in relation to chorionicity. The mean gestational length was shorter for MC twins (36.4 ± 1.9 [30 + 0–40 + 0]) versus DC twins (36.9 ± 2.1 [30 + 0–41 + 0]) (p < .01). There was no difference in the proportion of MC/DC delivered twins <34 gestational weeks compared to >34 weeks.
Table I. Maternal characteristics
The intrapartum and neonatal characteristics for second twins in relation to chorionicity are shown in . DC second twins had a higher birthweight (p < .001), a longer twin-to-twin DTI (p < .001) and a higher number of caesarean sections (p < .05) compared to MC second twins. The mean umbilical pH was slightly lower in DC second twins compared to MC second twins (7.23 ± 0.1 vs. 7.25 ± 0.09, p < .01). The difference in umbilical pH was not seen for those born <34 weeks of gestation. There was no significant difference in the number of second twins born with pH ≤7.10 in relation to chorionicity (p = .06), but a tendency to more DC second twins with acidosis. No statistical difference was found concerning the presentation, SGA, instrumental delivery, Apgar <7 at 5 min or admission to NICU secondary to birth asphyxia in relation to chorionicity for second twins. This was also true for second twins born below 34 weeks.
Table II. Second twin intra partum characteristics and short-term outcome
DC first twins had a higher birthweight than MC first twins (p < .05). No significant difference was found concerning SGA, instrumental delivery, mean umbilical pH, Apgar <7 at 5 min and admission to NICU secondary to birth asphyxia in relation to chorionicity for first twins.
Independent of chorionicity, second twins had a significantly lower umbilical pH (7.23 ± 0.1 vs. 7.31 ± 0.06, p < .001) and more often pH ≤7.10 (8.4% vs. 0.5%, p < .001), Apgar scores <7 at 5 min (2.3% vs. 0.8%, p < .05) and admissions to NICU secondary to asphyxia (1.3% vs. 0.3%, p < .05) compared to first twins.
The correlation between twin-to-twin DTI and umbilical pH in DC and MC second twins was calculated with a linear regression model. An upper limit of 120 min was used for the DTI (four cases excluded as outliers, none with pH ≤7.10). The regression model of pH and DTI on chorionicity (logarithmic values) showed no statistical difference in the reduction rate of pH in MC compared to DC second twins (p = .46). The umbilical pH for all second twins during late second stage of labour decreased in average by 0.0012 units/min (p < .001).
The possible predictors for acidosis in the second twin, defined as an umbilical pH ≤7.10, were calculated with univariate analyses (). Inter delivery time was a predictor for acidosis in the second twin (p < .01) whereas the chorionicity, gestational length <34 weeks, fetal presentation and SGA were not of major importance. Second twins with a pH ≤7.10 were more often delivered by caesarean section, instrumental delivery or breech extraction whereas second twins with umbilical pH >7.10 were significantly more often delivered spontaneously.
Table III. Predictors for acidosis in second twin, univariate
OR (95% CI) was calculated with multiple logistic regression for the independent variables DTI, chorionicity and gestational length <34 weeks. DTI was a statistic significant predictor for acidosis in the second twin, increasing the risk for acidosis by 1%/min from the delivery of the first twin (1.01 [1.00–1.02]). Chorionicity nor gestational length <34 weeks predicted acidosis in the second twin (0.53 [0.26–1.09], respectively 1.93 [0.59–6.34]).
Discussion
In this study, we found no difference in the reduction rate of umbilical artery pH during second stage of labour for MC second twins compared to DC second twins, rejecting the hypothesis that MC second twins detoriate faster. Neither was there a difference in Apgar scores <7 at 5 min or admissions to NICU secondary to asphyxia between MC and DC second twins. The DTI was, on the other hand, shorter for MC second twins, which is in agreement with Hoffman et al. (Citation2012). If this is a result of earlier active management due to signs of fetal distress in MC second twins or spontaneous shorter DTI cannot be proven in this study. The included centres in this retrospective study follow the same regional clinical recommendations regarding vaginal twin delivery, including the same management for MC and DC during active stage of delivery. The fact that the group with longer DTI, the DC second twins, had a tendency to a higher number of individuals with acidosis, and that the median DTI for MC second twin was as short as 12 min may support a spontaneous shorter DTI rather than operative delivery due to fetal distress in this group. In addition, a second twin with acidosis was more often delivered by caesarean section or by operative vaginal delivery, a situation that requires time and may increase the DTI.
There was no difference in the DTI in regard to chorionicity below 34 weeks of gestation. Chorionicity did not alter fetal outcome of the second twin between gestation weeks 30–34. The studied cohort showed no increased risk for acidosis at a gestation age 30–34 weeks compared to those born >34 weeks. These sub-analyses have to be interpreted with great caution as there is an obvious risk for underpower with the studied cohort. It is an area of debate whether the premature second twins (30–34 weeks) are at higher risk for acidosis and perinatal death and if vaginal delivery should only be recommended for those at gestational age >34 weeks. A Swedish study from 2008 with 22,938 twin-pairs showed a lower neonatal mortality for second twins after caesarean delivery (indication breech) compared to vaginal delivery before 34 weeks of gestation. At term, mortality was low irrespective of the delivery mode (Herbst and Källén Citation2008).
A number of studies have shown that the second twin has a lower blood gas status in comparison with the first twin at birth, irrespective of chorionicity. Delivery intervals >30 min have been strongly associated with higher risks for acidosis (pH <7.10) and low Apgar scores (Tak-Yeung et al. Citation2002; Tak-Yeung et al. Citation2004; Armson et al. Citation2006; Suh et al. Citation2007; Stein et al. Citation2008; Kwon et al. Citation2011; Hjortø et al. Citation2014). Stein et al. studied the influencing factors on DTI and found that breech, transverse lie, birth weight discordance with second twin to be at least 20% larger, fetal distress, vaginal operative delivery and caesarean section were found to be related to a prolonged DTI. A Canadian study with 5,138 twin pairs showed that second twins face a six-fold higher risk of fetal distress and a two-fold higher risk for a low 5-min Apgar score than their vaginally-delivered, vertex co-twins. Gestational age at delivery, infant sex combination and second twin presentation did not alter these differences. However, the excess risk was not seen among twins with the shortest DTI (0–14 min) (Armson et al. Citation2006), which is in agreement with the present results. In the univariate analysis in this study, DTI and mode of delivery, i.e. caesarean section and assisted vaginal delivery (vacuum extraction, forceps, breech extraction), were associated with acidosis (pH ≤7.10) while chorionicity, gestational age (being born before or after 34 weeks of gestation), presentation (vertex vs. breech), maternal age and SGA did not show any effect. The multivariate analysis confirmed that DTI is a predictor for acidosis and that chorionicity and gestational age do not seem to play a major role in twin pregnancies selected for vaginal delivery.
The risk for selection bias in the studied cohort has to be addressed. The population is a selected group as twin pregnancies are closely controlled during the latter half of pregnancy according to national recommendations. Twin pregnancies with expected compromise during vaginal delivery are most likely already excluded due to the decision of an elective caesarean section, including not only those with the first twin in a non-vertex presentation. This is an inherent problem with the retrospective design. We believe that the cohort is representative for vaginal twin deliveries after 30 weeks of gestation in general, since it includes all twins in the region over a period of almost six years and the same protocol was used for monitoring twin pregnancy and delivery.
In conclusion, differences between selected MC twins and DC twins are small during second stage of labour. Close monitoring is still warranted during twin pregnancies. In cases of uneventful MC pregnancies, we find no support to suggest different delivery guidelines for MC diamniotic twins compared to DC twins. Lower umbilical pH at birth for DC second twins seems to partly depend on a longer median DTI for DC twins compared to MC twins.
Second twins are at a higher risk for acidosis compared to first twins. A main predictor for acidosis seems to be the twin-to-twin DTI. The statistical calculated risk for acidosis, defined as umbilical pH ≤7.10, in the second twin increased by almost 1%/min during the second stage of labour. An absolute upper limit for DTI cannot be supported by the results of this study. However, it may be reasonable to recommend active management after 15–30 min to lower the risk for acidosis of the second twin. To further try to support this, a clinical prospective randomised trial would be of value.
Acknowledgements
We are most grateful to Eva Eneroth and Margareta Norman who contributed to patient data, and to Henry Nisell for statistical considerations. The study was supported by Karolinska University Hospital. No specific funding was obtained.
Disclosure statement
The authors have no interest of conflict to declare.
Related Research Data
References
- Armson BA, O'Connell C, Persad V, Joseph KS, Young DC, Baskett TF. 2006. Determinants of perinatal mortality and serious neonatal morbidity in the second twin. Obstetrics and Gynecology 108:556–564.
- Caprice DM, David RB. 2005. Intertwin time interval: how it affects the immediate neonatal outcome of the second twin. American Journal of Obstetrics Gynecology 192:1420–1422.
- Hartley RS, Hitti J. 2005. Birth order and delivery interval: analysis of twin pair perinatal outcomes. Journal of Fetal and Neonatal Medicine 17:375–380.
- Herbst A, Källén K. 2008. Influence of mode of delivery on neonatal mortality in the second twin, at and before term. BJOG: An International Journal of Obstetrics and Gynaecology 115:1512–1517.
- Hjortø S, Nickelsen C, Petersen J, Secher NJ. 2014. The effect of chorionicity and twin-to-twin delivery time interval on short-time outcome of the second twin. The Journal of Maternal-Fetal & Neonatal Medicine 27:42–47.
- Hoffman E, Oldenburg A, Rode L, Tabor A, Rasmussen S, Skibsted L. 2012. Twin births: Cesarean section or vaginal delivery? Acta Obstetricia Et Gynecologica Scandinavica 91:463–469.
- Joseph KS, Kramer MS. 2017. The fetuses-at-risk approach: survival analysis from a fetal perspective. Acta Obstet Gynecol Scand. 97:454–465.
- Kwon JY, Yoon WS, Lee GSR, Kim SJ, Shin JC, Park IY. 2011. Umbilical arterial blood gas and perinatal outcome in the second twin according to the planned mode of delivery. International Journal of Medical Sciences 8:643–648.
- Stein W, Misselwitz B, Schmidt S. 2008. Twin-to-twin delivery time interval: influencing factors and effect on short-term outcome of the second twin. Acta Obstetricia Et Gynecologica Scandinavica 87:346–353.
- Suh YH, Park KH, Hong J-S, Yoon BH, Shim S-S, Park JS, et al. 2007. Relationship between twin-to-twin delivery interval and umbilical artery acid-base status in the second twin. Journal of Korean Medical Science 22:248–254.
- Tak-Yeung L, Wing-Hung T, Tse-Ngong L, Ingrid HL, Tze-Kin L. 2002. Effect of twin-to-twin delivery interval on umbilical cord blood gas in the second twins. BJOG: An International Journal of Obstetrics and Gynaecology 109:63–67.
- Tak-Yeung L, Ingrid HL, Wing-Hung T, Tse-Ngong L, Tze-Kin L. 2004. Detoriation in cord blood gas status during the second stage of labour is more rapid in the second twin than in the first twin. BJOG: An International Journal of Obstetrics and Gynaecology 111:546–549.
- Thorngren-Jerneck K, Herbst A. 2001. Low 5-minute Apgar score: a population-based register study of 1 million term births. Obstetrics and Gynecology 98:65–70.
- Westgate JA, Garibaldi JM, Greene KR. 1994. Umbilical cord blood gas analysis at delivery: A time for quality data. British Journal of Obstetrics and Gynaecology 101:1054–1063.
- Wiberg N, Källen K, Herbst A, Olofsson P. 2010. Relation between umbilical cord blood pH, base deficit, lactate, 5-minute Apgar score and development of hypoxic ischemic encephalopathy. Acta Obstetricia Et Gynecologica Scandinavica 89:1263–1269.
- Ylilehto E, Palomäki O, Huhtala H, Uotila J. 2017. Term twin birth - impact of mode of delivery on outcome. Acta Obstetricia Et Gynecologica Scandinavica 96:589–596.