

Abstract
Men can be essential sources of support in maternal health, even more so in case of severe acute maternal morbidity (SAMM), affecting 1–2% of childbearing women in low-resource settings. In a qualitative study using semi-structured interviews, we explored the perspectives of nine male partners of women who suffered from (pre-)eclampsia six to seven years earlier in rural Tanzania. Male partners considered their role to be pivotal regarding finances, decision-making in healthcare-seeking and family planning and provided physical and emotional support. After SAMM, households may be affected in the long run. Some men took over their female partner’s household duties until up to two years after birth. Providing men with more information on complication readiness and birth preparedness would enable them to extend their role in maternal morbidity prevention.
What is already known on this subject? The essential role of male partners in maternal health in low- and middle-income countries is well-studied in relation to its impact on care-seeking behaviour. After childbirth, the long-term role of male partners has not yet been studied.
What do the results of this study add? We demonstrated the important role of men during, but also after SAMM. Households may be affected years after women suffered from SAMM. For women with the most urgent support needs, this study suggest that at least some men feel responsible for their partner and have different pivotal roles.
What are the implications of these findings for clinical practice and/or further research? Because of their motivation to support their female partner, strategies to reduce recurring complications in subsequent pregnancies should include targeting male partners, for example, by increasing birth preparedness and complication readiness. Further studies should confirm the results from our innovative but small-scale study, as well as investigate the long-term role of male partners after uncomplicated births. Other studies could investigate the separation of couples after SAMM, family planning decisions after SAMM and strategies for involving men and increasing complication readiness and birth preparedness.
IMPACT STATEMENT
Introduction
Male partners play an essential role in maternal health in low- and middle-income countries, especially in terms of their influence on care-seeking behaviour (Aborigo et al. Citation2018). Because of their roles in the division of labour, control of means and power in decision making, involvement of men can improve maternal and newborn health by supporting health-promoting and care-seeking behaviour (Comrie-Thomson et al. Citation2015, Mbalinda et al. Citation2015). The need for male support may become more urgent for women who suffered from severe acute maternal morbidity (SAMM), that is, ‘a woman who nearly died but survived a complication that occurred during pregnancy, childbirth or within 42 days of termination of pregnancy’ (Mbalinda et al. Citation2015). Obstetric complications affect 1520% of childbirths globally, or 20 million women annually (Geller et al. Citation2018). Using more restricted SAMM criteria (Ronsmans Citation2009), figures are usually lower, between 1 and 2% of births in resource-poor settings (Koblinsky et al. Citation2012). In Tanzanian hospitals, a SAMM incidence of 24 to 36 per 1,000 live births has been reported (Nelissen et al. Citation2013, Litorp et al. Citation2014). Hypertensive disorders such as pre-eclampsia and eclampsia are among the leading causes of maternal morbidity and mortality (Duley Citation2009). SAMM can have several long-lasting effects; 69% of women in Morocco reported at least one medical problem eight months after SAMM (Assarag et al. Citation2015). In Tanzania, more than 20% of women had postpartum depression two to six weeks after pre-eclampsia or eclampsia (Mbarak et al. Citation2019). The incidence of depression in Morocco and Benin was more than twice as high among women with SAMM compared to uncomplicated deliveries (Filippi et al. Citation2010, Assarag et al. Citation2015). In these settings, some women also suffered from their male partner’s physical violence, promiscuity and resultant divorce (Assarag et al. Citation2015). Although some studies point to these forms of negative impact of men on women’s well-being after SAMM, their care and support can have an important positive effect on women’s long-term health and coping abilities (Mbalinda et al. Citation2015, Munguambe et al. Citation2016). To our knowledge, the role of male partners in terms of support in the long run, more than one year following SAMM, has not yet been studied. Therefore, this study sought to explore the role of male partners in supporting women at the time of SAMM, and in the years after.
Materials and methods
This is a cross-sectional, explorative qualitative study of male partners of women who were treated for severe pre-eclampsia and eclampsia. These women were included in a previous observational study about short-term outcomes of 81 episodes of severe pre-eclampsia and eclampsia in 80 women between 2011 and 2012 (Mooij et al. Citation2015). Inclusion criteria and definitions used for severe pre-eclampsia and eclampsia have been reported elsewhere (Mooij et al. Citation2015).
Participants were approached in April and May 2018, six to seven years after the index pregnancy. Demographic and obstetric characteristics of the women were noted. Male partners were interviewed about their experiences and accounts of the roles they played during and after SAMM. Partners were included if they were the same as the ones during the time of the index pregnancy. Exclusion criteria were age under 18 years, learning disabilities or significant chronic or acute physical illness when participation would have been more than a minor burden.
Setting
Ndala Hospital is located in a rural area in Tabora region of Western Tanzania (Haverkamp et al. Citation2014). Ndala Hospital is a faith-based hospital situated at the border of Nzega and Uyui districts. The majority (90%) of the area’s inhabitants, mainly Nyamwezi and Sukuma ethnic groups, are involved in farming and animal husbandry (Haverkamp et al. Citation2014). Tabora has the highest rate of male illiteracy in the country (34%) (Anon Citation2016). There is a patriarchal societal structure and more than a quarter of married women are in a polygamous relation (Anon Citation2016). Less than 5% of women and 8% of men in Tabora have health insurance (Anon Citation2016). Governmental maternal health services are free of charge, private hospitals (such as Ndala Hospital) charge user fees (Kruk et al. Citation2008). The total fertility rate is the highest in the country, with 6.7 (Anon Citation2016).
Ethics approval
Ethical approval was obtained from the ethical board of the University of Dodoma (UDOM/DRP/134/VOL IV/41). Informed written consent was sought for all participants who could sign, and informed verbal consent for those who could not. Participants were informed of the criteria for their selection for the study, objectives of the study, and that there would be no consequences if they chose not to participate. Consent was sought for the interview a) to be carried out, b) recorded, and c) for anonymous quotes to be used in reports and publications. Participants that were found to have either physical or psychological problems were referred to Ndala mission hospital for review. Data were collected in participant’s homes or preferred convenient location. Anonymity and confidentiality have been upheld during sharing of information and report writing. No names or identifying information have been mentioned in this report. All digital data has been password protected. Paper forms have been securely stored by one of the research team members.
Data collection and analysis
The original study sample consisted of a group of 80 women who were managed for severe pre-eclampsia and eclampsia in Ndala Hospital between July 2011 and December 2012 (Mooij et al. Citation2015). Hospital records were used to identify and trace these women. Participants were approached by two local motorbike drivers/translators, co-author Ruth R. Kapanga (RRK) and Jessica A. Kofi, member of the research team.
Quantitative data were managed in Excel (Microsoft Office, Redmond, WA, USA). Descriptive statistics were done with Epi Info 7 (CDC, Atlanta, GA, USA). Semi-structured interviews by the male partners, conducted by RRK were conducted in Swahili at participant’s home or other relatively private location chosen by them (e.g. under a tree near their homes). All interviews, ranging from 20 to 40 minutes, were audio-recorded, transcribed verbatim in Swahili, and translated into English. An independent interpreter compared a random sample of three of the Swahili transcripts to their English translations for the second time to validate for consistency of translation. Using Atlas.ti (ATLAS.ti Scientific Software Development GmbH, Berlin, Germany), data were coded and analysed thematically by the interviewer (RRK); we categorised data according to different roles played by the male partners in terms of their care and support of women who suffered from SAMM. Emerging themes from the first round of interviews yielded more topics to be addressed, and with their consent, four male participants were re-interviewed by phone to address these new topics. During this follow up, consistency with prior responses was also checked in order to assess the reliability of findings.
Results
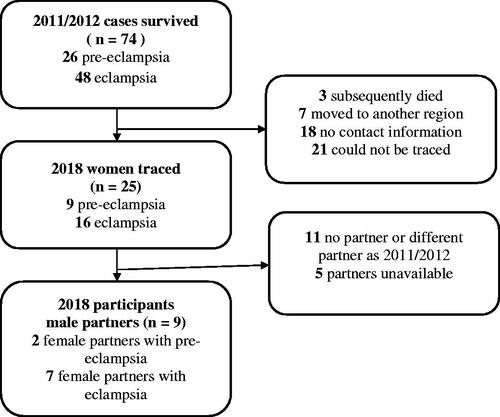
Twenty-five women who experienced SAMM five to six years ago could be traced. Eleven women were not together with the man who was their partner during the SAMM event, either because they were never married (1), divorced and currently living alone (3) or divorced and remarried (7). None were widowed. Of the 21 women currently living together with a male partner, 18 were in a monogamous relationship. Of the 14 women who lived together with the same male partner as the one during the index pregnancy, nine male partners (12% of the original number of women) were present at the day of the visit, and all consented to be interviewed ().
Figure 1. Selection of participants flowchart.
All participants came from Uyui and Nzega districts and lived between 2 and 87 km from Ndala Hospital. Characteristics of the women are summarised in .
Table 1. Sociodemographic characteristics and obstetric history of the nine women living with the same male partner six to seven years after SAMM.
presents the socio-demographic profiles of the nine male respondents. Most had received primary or no education; all but two were farmers. All had monogamous marriages, and the majority had two children with their partners.
Table 2. Profiles of male participants.
Our analysis identified five domains in which male partners played a role during and after SAMM, related to finances, decision-making in seeking healthcare and family planning, and provision of physical and emotional support.
Role in finances
In their narratives, male partners expressed feeling responsible for their families’ financial needs during the period of their female partner’s SAMM up to recovery.
I was outside, and spoke to my mother [who accompanied his female partner] and gave her some money then left. I left money for daily use and treatment. Participant 1
All men described providing financial support. Expenditures included: transport to the hospital, food and essential personal care items (e.g. cloths, soap), hospital bills for their spouses or newborns, and prescribed medication. None of the participants indicated having insurance coverage. Ease of payment for medical services varied. One participant acknowledged that he could save money to prepare for complications during delivery. Two male partners incurred debts to cover costs for the hospital stay and subsequent treatment; they borrowed money from relatives. Other participants found other ways of meeting financial needs, for example, selling livestock or other property:
So, I decided to go home and look for money. I came home and sold a cow and went back [to the hospital]. Participant 7
Some participants indicated that during and after SAMM, they could not ‘look for money’, because of frequent hospital visits and taking care of a sick person. For instance, one man reported that for up to two years after birth, his female partner’s health condition remained poor. During this period, he was unable to perform paid work and generate income, taking up household chores instead, including cooking. Thus, in these instances, SAMM gave rise to long term financial consequences.
Role in decision-making: seeking healthcare
Male partners indicated that they played a decision-making role concerning healthcare-seeking and transport to health facilities. Some participants took their female partner to the hospital themselves, primarily by motorbike, and others hired a vehicle or called for an ambulance.
She kept complaining of a headache. After the headache, I gave her painkillers, but later she got convulsions. It really confused me […]. In the morning […] my wife’s health changed. She developed convulsions. I was forced to call for an ambulance. Participant 4
Several men, however, described problems in arranging transport and delays occurring on the road, for example, due to heavy rains. Before any complication occurred, male partners also took decisions concerning the place of birth and accessing care. One participant indicated that he agreed to let his female partner go to her parental home towards the end of the pregnancy. Even though not taking care of her himself, he made sure she was supported at the time of birth.
Men’s decision-making capacities were affected by lack of knowledge, sometimes causing delay in reaching the hospital.
I was thinking the convulsions occur before someone has given birth. For her, it happened after delivery, so it really confused me. But after reaching the hospital, they informed me that it was eclampsia. Participant 4
The men’s narratives pointed to the need for information that could help them decide how best to support their female partners. Most did not understand the cause of their female partner’s illness. Participant 4 had some information about eclampsia but did not know of warning signs or the possibility of convulsions after birth. Men sought information from healthcare workers (HCWs), relatives and friends. Some participants indicated that they had not asked about the details of the condition of their female partner, nor were they informed by HCWs. Most participants said they received precautions regarding subsequent pregnancies. These were used to make better decisions in the future, being prepared in case of recurrence. During the interviews, many participants admitted lacking knowledge about warning signs before their experience with severe pre-eclampsia or eclampsia and some showed keenness on getting more information on how to act in a next pregnancy.
This eclampsia, what causes it most of the time? (…) I feel it has cleared but does it really clear or is it a question of time and it will reoccur? Participant 9
Thus, men reported that they take various decisions affecting their female partners’ care but appeared to need more information on risk of recurrence and warning signs to better help them prepare.
Role in decision making: family planning
Participants talked about their role in pregnancy spacing, sometimes taking the initiative, sometimes in a more facilitating role.
At the hospital, say a day before we were discharged, [the doctors] sat down with us and explained to us about sterilisation. I felt like it was a good thing, but I didn’t have the means [finances] at that time. So it meant I had to prepare for that… Because after that incident, each one of us didn’t have the desire for it [children] anymore. Participant 7
This participant had seven children with his female partner. Three months after birth, they went to a health centre, and she got a tubal ligation. This account shows that family planning relates to financial resources as well as the power to make decisions. When asked if they had had a specific number of children in mind when they got married, one participant answered that their desired number of children was higher than of children they had, but that life (and thus, being alive) was more important, leading to the use of birth control measures. In other accounts, the difficult choice between reproduction and protecting the health of the female partner was mentioned. Participant 9 was advised by neighbours to stop having children after his female partner suffered two stillbirths due to pre-eclampsia.
[Neighbours would ask] ‘Are you ready to lose your wife because of a baby? Then have a hysterectomy done and then you live with her just like that [without children]. Participant 9
He did not follow this advice, and fortunately, later, his female partner gave birth to two healthy babies. Hence, looking at the longer run, men played an essential role in making decisions regarding family planning, supporting their female partner. Having experienced SAMM, some framed delaying or stopping childbearing as a way to promote their female partner’s health or even to protect her life.
Physical support
During the period of SAMM, hospitalisation and immediate period of recovery, participants offered various forms of physical support.
I attended to her by bringing her food. Sometimes helping her when she needed to relieve herself. At that point she couldn’t walk, she was relieving herself right in bed. Participant 7
One participant stayed with his female partner in the hospital for two weeks. Most saw the need for their female partner to have a period of physical recovery after hospital discharge. One man allowed his female partner to decide when she felt well enough to join in farm duties. Another took up his female partner’s chores for around two years:
I took [her duties] up. Cooking for example. These children you see here just grew up recently. I was there [to take care of the children too]. I had too many thoughts [about taking on her duties]. But later I was content. Participant 6
Through physical assistance when needed and taking over duties, male partners are seen to support their female partner’s physical health for up to two years after childbirth.
Emotional support
Support was not merely physical. When asked whether, and in what ways, they offered their female partner emotional or psychological support during SAMM, most did not explicitly state that they provided emotional support. Nevertheless, it could be inferred that they did so from their narratives.
Support was to stay close to her. Stay with her and observe how she was faring on. Participant 3
Most participants were present during the time of SAMM, hospitalisation and recovery. One participant, whose female partner had experienced a stillbirth due to eclampsia, encouraged his spouse by telling her that other women have suffered worse complications. This participant, a high school teacher, also thought that discussing permanent family planning methods with his female partner when they did not have any child would ‘mess her up psychologically’. He kept his feelings of worry and concern from his female partner as a way of supporting her, trying to ease her psychological distress. According to him, this strategy helped since she was able to overcome her grief, conceived, and delivered two children safely afterwards.
The accounts show that by offering companionship, comforting and withholding painful information, emotional support was offered, even though men did not explicitly call it as such.
Discussion
We identified five themes that male partners discussed. First, male partners felt responsible for mobilising and controlling financial resources when SAMM occurs. In African settings, it is common for men to be the main financial providers of the family (Singh et al. Citation2014). In addition to direct costs (hospital fees), men and women encountered various indirect costs and loss of income (Kruk et al. Citation2008). Earlier studies in Burkina Faso described severe and long-lasting economic consequences for women and their households following SAMM (Storeng et al. Citation2008; Citation2013). Insurance or reimbursement programs only pay for direct costs and cannot protect against these indirect costs. Furthermore, men’s ability to fulfil their financial role may be limited, especially when after SAMM they also take on caring duties. This may put a strain on their relationships. An ethnographic study of near miss experiences in Burkina Faso found that its financial consequences could result in tensions between the woman and her spouse, and even marriage dissolution, especially if the complications led to loss of the baby (Storeng et al. Citation2010).
Women are described to have three roles in society, related to reproduction; productive or income generating work; and work undertaken at the local community or neighbourhood level (Moser Citation1989). Storeng et al. described how women’s productive role might interfere with their reproductive role and general well-being after SAMM (Storeng et al. Citation2013). They described how some women resume work activities after a SAMM experience at the expense of restorative rest or chronic illness, ensuring short-term economic survival but potentially interfering with recovery (Storeng et al. Citation2013). Our study found that men too have multiple gender roles which can interfere with each other. Notably, apart from their role as provider, in their narratives the men discussed how they supported their female partners. However, their control over finances and decision-making can be a barrier for women to access healthcare (Munguambe et al. Citation2016). Earlier research confirms that men’s greater power in terms of financial means and decision-making appears a problem for some women in the area. Van Vuuren observed women around Ndala strive for financial independence by having their own income sources to achieve greater independence within their marriage and more autonomy in the decision-making process within their household (van Vuuren Citation2003).
Decision-making related to healthcare-seeking, the second theme, is based on prior information, especially from HCWs. Thus, by improving men’s knowledge, maternal health after SAMM may be enhanced. This has been advocated in other areas of maternal health (Mosha et al. Citation2013), but this study highlights the relevance of informing couples after SAMM (e.g. about recurrence risks and warning signs). Other studies about the role of men in African countries have sometimes observed behaviour that mag suggest an apparent lack of interest in women’s health issues, for example by discouraging revealing pregnancy in early gestation and unfamiliarity with warning signs (Munguambe et al. Citation2016), or embarrassment to accompany their wife to antenatal clinic visits (Aborigo et al. Citation2018). Men who have stayed with their female partners may not be representative of all men, but our findings show that they wanted to care for them when complications arose and in the aftermath of SAMM. The experience of the life-threatening situation their female partner was in, as well as the long-term consequences, may have heightened their motivation and involvement.
A study in northern Tanzania showed that men had little interest in family planning issues, the third theme, but considered themselves key decision-makers regarding child spacing and decision on the number of children (Mosha et al. Citation2013). In their narratives, some men considered contraception a way to allow their female partner to recover, using contraception as a method of support. However, the use of ‘modern’ contraceptives is not common in Tabora region; 21% among currently married women compared to 32% at national level (Anon Citation2016). This is due mainly to local preferences since the low unmet need for contraception of 22% does not explain the lower prevalence in Tabora (Anon Citation2016). According to the 2015 Tanzania Demographic and Health Survey, the average desired family size in Western Tanzania is almost six children (Anon Citation2016). Hence, it is understandable that one participant thought that discussing permanent family planning methods with his partner without having a child would make her unhappy. In general, perinatal deaths are common in SAMM, and in our original sample of 81 episodes of (pre-) eclampsia the perinatal death rate was 30% (Mooij et al. Citation2015). This means long-term effects after SAMM arise not only due to persistent maternal illness but also because of the perinatal loss in childbearing (de Kok et al. Citation2010; Mooij et al. Citation2021).
Lastly, our findings indicate that at least some men support their female partners physically and emotionally. Male partners described companionship and comforting their female partner, even to the point of withholding information. This was, however, often not called emotional support in the interviews, perhaps due to language or cultural barriers. As such, both the experience of emotional and psychological distress and forms of emotional or psychological support following SAMM deserves a more in-depth exploration, with investigation into its cultural, linguistic and educational components. This may lead to a greater understanding of how, and to what extent, such emotional and psychological matters are culturally embedded and manifested, and what this implies for the development of culture-responsive interventions.
Almost half of the women (11/25, 44%) were not together anymore with the same male partners as during the SAMM-complicated pregnancy. SAMM may have led to divorce; a consequence of SAMM which has been described before (Kaye et al. Citation2014). There may be other reasons for separation however, since female-led households are not unusual in LICs in general and in Ndala in particular (Moser Citation1989; van Vuuren Citation2003). Van Vuuren’s thesis explores the differences in livelihood strategies between male-headed households and different types of female-headed households (unmarried, separated and widowed) around Ndala (van Vuuren Citation2003). In this study, 58% of 120 households were headed by a male, with on average a larger total household size compared to households headed by women.
Although our study did not aim to assess delays in receiving quality maternal health care, the three phases of delay described by Thaddeus and Maine (Thaddeus and Maine Citation1994), and the possible role of men, are easily recognised in the accounts of the participants. Lack of knowledge of danger signs appeared to contribute to the first phase of delay, the decision to seek healthcare. Strategies to increase men’s knowledge, such as birth preparedness and complication readiness, are essential to reduce delays and seem particularly welcomed by these participants (Thaddeus and Maine Citation1994; August et al. Citation2015). After seeing the consequences of SAMM in their families, they might be more motivated to gain more knowledge. A study from rural Rukwa in Tanzania showed that birth preparedness (knowledge of preparations to be made for childbirth) was low among expecting couples but higher after having experienced preterm birth (Moshi et al. Citation2018). Our study focussed on the period following birth and did not assess ANC. Better information and communication during ANC, involving more women and their male partners, will likely be an effective method to reduce the first delay (August et al. Citation2015). Still, a recent study in Tanzania found that only half of the male partners attending ANC visits, and HIV testing was cited as a reason not to attend (Kabanga et al. Citation2019). Thus, men may be interested to attend ANC and received information about birth, but other barriers may stop them from accompanying their wives, and these barriers need to be addressed.
During the second phase, delays in identifying and reaching health care facilities, occurred when a smaller facility could not give adequate care. Participants also talked about problems finding transport or getting to the hospital, living up to 87 km of Ndala. Ndala Hospital has no maternity waiting home. For women without relatives living close to the hospital, the construction of such a building could ensure less delay in reaching the hospital (Vermeiden and Stekelenburg Citation2017). Another strategy could be to offer community-saving transport schemes (Munguambe et al. Citation2016), although in their narratives men did not specifically mention costs of transport as a barrier to reach healthcare. A recent study into maternal mortality in India with eclampsia as the main cause of death found that the major contributors were phase 1 and 2 delays (Sk et al. Citation2019).
Further studies are necessary to investigate if couples separate more often after SAMM and the experiences of these divorced couples. There is also a need to study how couples make family planning decisions after SAMM, and to what extent these decisions are shared. Women’s social status within the household may diminish after SAMM, especially in case of perinatal loss (de Kok et al. Citation2010; Storeng et al. Citation2010), and this may further compromise her already limited reproductive health decision-making power. More studies are needed as well to evaluate strategies for involving men and increasing complication readiness and birth preparedness. Based on earlier studies identifying barriers, we recommend such strategies to be gender transformative, by increasing both men’s and women’s decision-making power (Moser Citation1989; van Vuuren Citation2003; Anon Citation2007; Comrie-Thomson et al. Citation2015; Munguambe et al. Citation2016; Kabanga et al. Citation2019).
Strengths and limitations
Only nine couples from the original 74 could be traced and were available for this study. These low numbers and the resulting possibility of selection bias are study limitations. However, this explorative study shows that long-term follow-up in a low-resource setting is possible, and our study is the first to report on male partners after SAMM, six to seven years after the event. This long follow-up period means there is a risk of recall bias, but enabled us to explore an important, under-studied aspect: long-lasting consequences of SAMM. Another strength is that participants were found far from Ndala Hospital; the furthest participant lived 87 km away. Other studies have excluded patients that live further away because of logistical reasons (Storeng et al. Citation2008), while people living far from the hospital have different perspectives to add. We did not include a control group, so they cannot be compared to male partners of women who did not experience SAMM. Furthermore, this study relies on self-reports, and participants may have given answers that they felt were desirable. This can only be addressed by conducting long-term ethnographic research, which we recommend, but was not feasible for this study. Moreover it is also valuable to gain insight into what is considered socially desirable. The number of interviews (9) was determined by the availability of male partners, not by data saturation. Interviews were conducted with men who have stayed with their female partners since the time of SAMM, which means results cannot be extrapolated to the male partners who are not together. It could well be that men who left or were left by their female partner were less concerned about their wife’s health and well-being. Unfortunately, the three male partners in a polygamous relation (out of 21 together with the same partner) were not available for interview, and only monogamous male partners were interviewed.
In conclusion, we found that male partners play an essential role in maternal well-being in terms of decision-making in healthcare-seeking and family planning and in finances. They can support their female partners during their recovery, physically as well as emotionally. Their role starts during pregnancy and extends in the long term. Up to two years after SAMM, some men are seen to take over their female partner’s duties, with financial repercussions to the household. Men expressed a sense of responsibility for their female partner’s health after SAMM. Because of the risk of recurring complications in subsequent pregnancies and the motivation of these men, we recommend strategies to improve maternal health by increasing birth preparedness and complication readiness to pay specific attention to involving male partners of women who have experienced SAMM. Programmes and interventions must however be gender transformative, to avoid reproducing or even aggravating existing gender-based power differentials.
Acknowledgments
The authors would like to thank Jessica A. Kofi for her contributions to the fieldwork and critical review of the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Data are available from the author upon request.
Additional information
Funding
References
- Aborigo RA, Reidpath DD, Oduro AR, Allotey P. 2018. Male involvement in maternal health: perspectives of opinion leaders. BMC Pregnancy and Childbirth 18:3.
- Anon. 2007. Engaging men and boys in changing gender-based inequity in health: evidence from programme interventions. Geneva: Anon.
- Anon. 2016. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015–2016. Maryland: Dar es Salaam, Tanzania and Calverton.
- Assarag B, Dujardin B, Essolbi A, Cherkaoui I, De Brouwere V. 2015. Consequences of severe obstetric complications on women’s health in Morocco: please, listen to me!. Tropical Medicine & International Health 20:1406–1414.
- August F, Pembe AB, Mpembeni R, Axemo P, Darj E. 2015. Men’s knowledge of obstetric danger signs, birth preparedness and complication readiness in Rural Tanzania. PLoS One 10:e0125978.
- Comrie-Thomson L, Tokhi M, Ampt F, Portela A, Chersich M, Khanna R, et al. 2015. Challenging gender inequity through male involvement in maternal and newborn health: critical assessment of an emerging evidence base. Culture, Health & Sexuality 17:S177–S189.
- de Kok BC, Hussein J, Jeffery P. 2010. Joining-up thinking: loss in childbearing from inter-disciplinary perspectives introduction. Social Science & Medicine 71:1703–1710.
- Duley L. 2009. The global impact of pre-eclampsia and eclampsia. Seminars in Perinatology 33:130–137.
- Filippi V, Goufodji S, Sismanidis C, Kanhonou L, Fottrell E, Ronsmans C, et al. 2010. Effects of severe obstetric complications on women’s health and infant mortality in Benin. Tropical Medicine & International Health 15:733–742.
- Geller SE, Koch AR, Garland CE, Macdonald EJ, Storey F, Lawton B. 2018. A global view of severe maternal morbidity: moving beyond maternal mortality. Reproductive Health 15:98.
- Haverkamp, G.W.M., Hulsbergen, M.H., Mooij, R. (eds.) (2014) 50 years of Ndala Hospital, Tanzania. Amsterdam: Stichting Tabora.
- Kabanga E, Chibwae A, Basinda N, Morona D. 2019. Prevalence of male partners involvement in antenatal care visits – in Kyela district, Mbeya. BMC Pregnancy and Childbirth 19:321.
- Kaye DK, Kakaire O, Nakimuli A, Osinde MO, Mbalinda SN, Kakande N. 2014. Lived experiences of women who developed uterine rupture following severe obstructed labor in Mulago hospital, Uganda. Reproductive Health 11:31.
- Koblinsky M, Chowdhury ME, Moran A, Ronsmans C. 2012. Maternal morbidity and disability and their consequences: neglected agenda in maternal health. Journal of Health, Population, and Nutrition 30:124–130.
- Kruk ME, Mbaruku G, Rockers PC, Galea S. 2008. User fee exemptions are not enough: out-of-pocket payments for ‘free’ delivery services in rural Tanzania. Tropical Medicine & International Health 13:1442–1451.
- Litorp H, Kidanto HL, Roost M, Abeid M, Nystrom L, Essen B. 2014. Maternal near-miss and death and their association with caesarean section complications: a cross-sectional study at a university hospital and a regional hospital in Tanzania. BMC Pregnancy and Childbirth 14:244.
- Mbalinda SN, Nakimuli A, Nakubulwa S, Kakaire O, Osinde MO, Kakande N, et al. 2015. Male partners’ perceptions of maternal near miss obstetric morbidity experienced by their spouses. Reproductive Health 12:23.
- Mbarak B, Kilewo C, Kuganda S, Sunguya BF. 2019. Postpartum depression among women with pre-eclampsia and eclampsia in Tanzania; a call for integrative intervention. BMC Pregnancy and Childbirth 19:270.
- Mooij R, Kapanga RR, Mwampagatwa IH, Mgalega GC, Dillen J, Stekelenburg J, et al. 2021. Beyond severe acute maternal morbidity: a mixed-methods study on the long-term consequences of (severe pre-)eclampsia in rural Tanzania. Tropical Medicine & International Health 26:33–44.
- Mooij R, Lugumila J, Mwashambwa MY, Mwampagatwa IH, Van Dillen J, Stekelenburg J. 2015. Characteristics and outcomes of patients with eclampsia and severe pre-eclampsia in a rural hospital in Western Tanzania: a retrospective medical record study. BMC Pregnancy and Childbirth 15:213.
- Moser CON. 1989. Gender planning in the third world: meeting practical and strategic gender needs. World Development 17:1799–1825.
- Mosha I, Ruben R, Kakoko D. 2013. Family planning decisions, perceptions and gender dynamics among couples in Mwanza, Tanzania: a qualitative study. BMC Public Health 13:523.
- Moshi FV, Ernest A, Fabian F, Kibusi SM. 2018. Knowledge on birth preparedness and complication readiness among expecting couples in rural Tanzania: differences by sex cross-sectional study. PLoS One 13:e0209070.
- Munguambe K, Boene H, Vidler M, Bique C, Sawchuck D, Firoz T, et al. 2016. Barriers and facilitators to health care seeking behaviours in pregnancy in rural communities of southern Mozambique. Reproductive Health 13:31.
- Nelissen EJ, Mduma E, Ersdal HL, Evjen-Olsen B, Van Roosmalen JJ, Stekelenburg J. 2013. Maternal near miss and mortality in a rural referral hospital in northern Tanzania: a cross-sectional study. BMC Pregnancy and Childbirth 13:141.
- Ronsmans C. 2009. Severe acute maternal morbidity in low-income countries. Best Practice & Research. Clinical Obstetrics & Gynaecology 23:305–316.
- Singh D, Lample M, Earnest J. 2014. The involvement of men in maternal health care: cross-sectional, pilot case studies from Maligita and Kibibi, Uganda. Reproductive Health 11:68.
- Sk MIK, Paswan B, Anand A, Mondal NA. 2019. Praying until death: revisiting three delays model to contextualize the socio-cultural factors associated with maternal deaths in a region with high prevalence of eclampsia in India. BMC Pregnancy and Childbirth 19:314.
- Storeng KT, Akoum MS, Murray SF. 2013. ‘This year I will not put her to work’: the production/reproduction nexus in Burkina Faso. Anthropology & Medicine 20:85–97.
- Storeng KT, Baggaley RF, Ganaba R, Ouattara F, Akoum MS, Filippi V. 2008. Paying the price: the cost and consequences of emergency obstetric care in Burkina Faso. Social Science & Medicine 66:545–557.
- Storeng KT, Murray SF, Akoum MS, Ouattara F, Filippi V. 2010. Beyond body counts: a qualitative study of lives and loss in Burkina Faso after ‘near-miss’ obstetric complications. Social Science & Medicine 71:1749–1756.
- Thaddeus S, Maine D. 1994. Too far to walk: maternal mortality in context. Social Science & Medicine 38:1091–1110.
- Van Vuuren JA. 2003. Women striving for self-reliance. Diversity of female-headed households in Tanzania and the livelihood strategies they employ. Amsterdam: University of Amsterdam.
- Vermeiden T, Stekelenburg J. 2017. Maternity waiting homes as part of an integrated program for maternal and neonatal health improvements: women’s lives are worth saving. Journal of Midwifery & Women’s Health 62:151–154.