

Abstract
Peripartum hypoxic neonatal brain injury cannot be accurately predicted with current foetal monitoring techniques. Neonatal brain monitoring through amplitude-integrated electroencephalography (aEEG) is utilised when brain injury is suspected. Intrapartum aEEG assessment may improve detection of foetal hypoxia, facilitating earlier intervention. Using different engineered configurations in adult volunteers (n = 18), we monitored aEEG through application of two foetal scalp electrodes (FSEs). This aided development of a novel signal splitter, our Foetal heart rate and aEEG Monitoring System (FEMS) to monitor aEEG intrapartum. We then compared FEMS with gold-standard EEG monitoring simultaneously in two adults. Average percentage of interpretable aEEG signal was 61.3%, with the FEMS obtaining 72.15%. EEG signal on the aEEG device consistently showed a similar trace to gold standard EEG. This study demonstrates feasibility of aEEG monitoring in adults with FEMS utilising FSE inputs. An intrapartum foetal study utilising FEMS is due to commence shortly.
What is already known on this subject? Cardiotography, the current gold standard in foetal monitoring, is not associated with a reduction in cerebral palsy or infant mortality rates. Neonatal amplitude-integrated electroencephalography (aEEG) is an established method of monitoring brain function to guide commencing cooling therapy in suspected hypoxic brain injury. Intrapartum animal studies have illustrated foetal EEG changes reflecting evolving hypoxia.
What do the results of this study add? This study demonstrates aEEG monitoring in human adult volunteers through application of foetal scalp electrodes and use of a novel signal splitter. This Foetal heart rate and aEEG Monitoring System (FEMS) provided a good overall percentage of aEEG signal, consistently showing a similar trace to gold standard EEG.
What the implications are of these findings for clinical practice and/or further research? This proof of principle study provides the first step in developing a novel intrapartum foetal monitoring technique to monitor foetal aEEG in labour. This provides an exciting prospect of transferring well established neonatal monitoring techniques to facilitate accurate brain function assessment intrapartum and early intervention to reduce hypoxic brain injury. An intrapartum foetal study of this technology is due to begin in the near future.
IMPACT STATEMENT
Introduction
Each year, data consistently shows that brain injury occurred in around 3.4/1000 live births at or soon after the time of birth in the UK (Gale et al. Citation2018). Around three quarters of these are secondary to hypoxic ischaemic encephalopathy (HIE) caused by hypoxia in the peripartum period. The Department of Health in 2015 committed to significantly reducing such injuries (Department of Health and Social Care Citation2015).
Continuous electronic foetal monitoring in labour is recommended for all pregnant women with antepartum or intrapartum risk factors such as diabetes, hypertensive disorders or antepartum haemorrhage. The mainstay of intrapartum monitoring involves cardiotocography (CTG) which records changes in the foetal heart rate (FHR) and their temporal relationship to uterine contractions. This is performed transabdominally or through attachment of an electrode to the foetal scalp (FSE). If CTG abnormality is present, foetal blood sampling (FBS) from the foetal scalp is often used to assess for foetal acidosis (National Institute for Health and Care Excellence Citation2017). FHR variations are poorly correlated with neonatal hypoxia and brain injuries. Despite being routine practice, when compared to intermittent auscultation of the foetal heart, CTG is not associated with reduction in cerebral palsy or infant mortality rates or an improvement in other standard measures of neonatal wellbeing (Alfirevic et al. Citation2017). CTG is associated with increased rates of caesarean section and instrumental vaginal births contributing to maternal morbidity and mortality in current and future pregnancies (Alfirevic et al. Citation2017). Some obstetric units apply FSEs routinely to all high-risk women in labour as it permits ST-analysis of the foetal electrocardiogram (ECG). ST-analysis is an adjunct aiming to improve the performance of foetal heart rate monitoring. However meta-analysis of randomised trials has not shown a reduction in neonatal adverse outcomes or severe metabolic acidosis (Neilson Citation2015). As such it is clear that a robust method for detecting intrapartum foetal hypoxia leading to brain dysfunction is urgently needed to avoid poor foetal and neonatal outcomes, with current foetal monitoring modalities being sub-optimal.
Amplitude-integrated electroencephalography (aEEG) is a means of assessing brain function, providing prognostic evidence for morbidity and mortality in neonates. Its role is well established in the neurological assessment of neonates, particularly those at risk of developing encephalopathy secondary to intrapartum hypoxia. Neonatal Intensive Care Units (NICUs) incorporate its use into selecting infants with encephalopathy for therapeutic cooling and identifying neonatal seizures (Toet and Lemmers Citation2009). Therapeutic hypothermia or ‘cooling’ is the current standard treatment for hypoxic perinatal brain injury, significantly reducing morbidity and mortality. However, death or severe neurodevelopmental disability is still evident in up to one-third of cooled infants with impact on cognitive skills by early school age (National Institute for Health and Care Excellence Citation2010; Liu et al. Citation2017; Lee-Kelland et al. Citation2020).
Animal studies have shown that simultaneous EEG and FHR monitoring can be achieved intrapartum through FSE application. EEG amplitude decreases consistently with occlusion of the umbilical artery, consistent with developing foetal hypoxia. As such, foetal EEG changes that occur in response to cerebral hypoxia have already been established in animals (Chakkarapani and Thoresen Citation2015; Frasch et al. Citation2015, Citation2017). Historic proof of principle study utilising a tripolar suction device on the foetal scalp in labour has demonstrated the feasibility of monitoring EEG and FHR in labour (Maynard et al. Citation1979). However, significant advancements in aEEG applications and technology have occurred over the past 40 years.
We sought to develop a novel technique for the simultaneous monitoring of foetal heart rate and aEEG through the use of two FSEs. In stage one, we aimed to show proof of principle of successful aEEG monitoring with two FSEs in adult volunteers through different engineered designs. We then aimed to develop a signal splitter that could be used intrapartum for simultaneous foetal aEEG and heart rate monitoring. Finally, in stage two we aimed to compare monitoring via our FSE aEEG monitoring system to gold standard EEG monitoring. This will act as proof of principle for aEEG monitoring in humans and the first step in working towards feasibility of human foetal aEEG monitoring.
Materials and methods
The study was approved by University of Bristol Faculty of Health Sciences Research Ethics Committee [reference 6687] and conducted at the University of Bristol. All volunteers received verbal and written information to consent in writing to participation in the study. Volunteers were 8 female and 10 male healthy adults.
Development of aEEG monitors and signal splitters
For stage one of the study, FSE probes (Rocket Copeland Foetal Scalp Electrode, Rocketmedical, England) were adapted to EEG plugs. FSE probes are two-pin devices with a subdermal electrode (the ‘hook’) connection which attaches to the foetus and a floating ‘sheath’ connection which may come in contact with the mother and shields the FHR signal from external noise. aEEG monitors require three single-pin plugs: two differential signals attached on either side of the scalp and one ground connection, usually attached to the scalp or the upper back of the subject. We explored all possible configurations of connections for the probe and sheath to determine which would produce the best signal to noise ratio (SNR).
Four probe designs () were built. The probe configurations were: (a) separate connections for the sheath and hook, where the sheath is connected to the aEEG monitor’s ground; (b) the sheath and hook merged into a single signal, and the aEEG ground connected to a different location on the body; (c) the sheath not connected and the aEEG ground connected to a different location on the body; and (d) a dual probe with two hook connections and a single shared sheath connection (shown connected to the aEEG monitor in , with the sheath connected to ground and the two hooks connected to the two signal channels). (a)–(c) would require two probes to function, while (d) requires only one dual probe.
Figure 1. ( A) Schematic diagram of the four different FSE connections (A, B, C and D) tested in stage one of the experiment. (B) Connector D connected to input of Olympic CFM6000. (C) The final signal splitter (foetal heart rate and aEEG monitoring system – FEMS) developed to permit the simultaneous monitoring of foetal aEEG and foetal heart rate (CTG) via two foetal scalp electrodes. (D) Block diagram showing the operation of the foetal heart rate and aEEG monitoring system (FEMS).
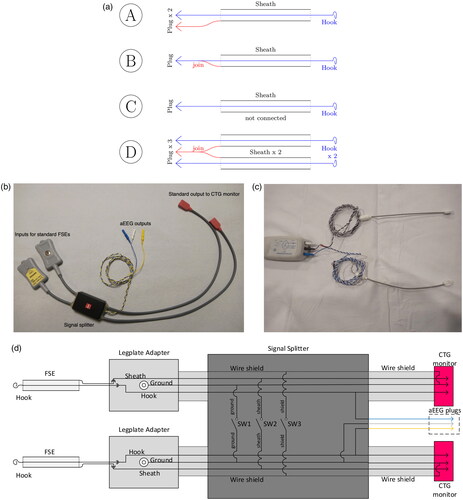
It was expected that configurations (a) and (d) would give the best performance, as the sheath would be connected to ground, which would allow the aEEG monitor to accurately determine the difference between environmental noise and the desired signal due to the nearby reference. It was expected that configuration (b) would be inferior, as the sheath and probe are joined, resulting in environmental noise being introduced to the desired signal. Configuration (b) effectively served as a test to determine whether the probe configuration had a significant effect on the SNR and that a good signal could not be obtained by mere proximity. Configuration (c) most closely mimics other aEEG setups, but does not effectively shield the signal from environmental noise due to the ungrounded sheath. Therefore, we expect it to be worse than (a) and (d) but better than (b).
The probe connections were then re-designed for use in labour. The FSE probes must remain in a sterile environment until use. Thus, we modified the reusable, non-sterile legplate adapter cable (Philips, UK). The goal was to continue to supply the FHR signal while also providing three aEEG plug connections for an aEEG monitor. Therefore, we developed a foetal heart rate and aEEG monitoring system (FEMS).
The Philips legplate adapter provides a reliable ground connection via an adhesive ECG pad on the mother’s thigh and a two-pin connection to a Foetal Scalp Electrode (FSE). The hook and sheath FSE connections, along with the ground connection, are then provided to the CTG monitor, with the adapter cable’s electromagnetic (EM) shielding and the ground connection merged inside the CTG monitor plug.
To provide these connections to both aEEG and CTG monitors simultaneously, a FEMS splitter box, , was built. On the left side, two Philips legplate adapters feed into the splitter box, with the intention to connect one hook to either side of the foetus’ scalp. On the right, two FHR plugs (corresponding to the two legplate adapters) are provided for connection to CTG monitors. In addition, three aEEG plugs are available, with the blue and yellow plugs connected to the subdermal hooks, and the white plug connected to a legplate ground.
The FEMS splitter contains a three-pole switch for configuration, see . Pin one connects the grounds of the two legplate adapters, pin two connects the probe sheaths, and pin three connects the EM shielding. As the ground and EM shielding are merged at the plug, pins one and three perform the same function at lower frequencies, although higher frequencies (megahertz) will experience differences. This configuration allows flexibility in the trade-off between shielding (protection from external noise) and capacitance (reduction of signal amplitude with increasing frequency due to a larger load).
Stage 1
In stage 1 of the study, adult volunteers (n = 15) were recruited. Two stick on electrodes (Ambu BlueSensor N, Ambu Sdn Bhd, Penang Malaysia) were applied to either side of the adult scalp. The adapted FSEs were clipped on to the stick-on electrodes and connected to the aEEG monitor. The adapted FSEs were distributed into 5 groups with 3 adults monitored in each group. The groups used designs A, B, C, D and the FEMS signal splitter as outlined above. Between 16 and 41 minutes of aEEG recording was collected for each adult volunteer on Olympic CFM6000.
Stage 2
In stage 2 of the study, adult volunteers (n = 3) underwent direct application of 2 FSEs to the adult scalp, connected to the FEMS signal splitter. Between 20 and 43 min of aEEG recording were collected for each adult volunteer on Olympic CFM6000. In 2 of the volunteers, gold standard EEG monitoring was performed simultaneously using 19 sensors placed on the scalp and recorded on a portable video EEG system (Micromed, Micromed Electronics Ltd, Surrey, UK). 1 FSE was placed between O1-P3 and the other between O2-P4 with recording on an Olympic CFM6000. This was to ensure the EEG signal acquired through the foetal scalp electrodes recording an aEEG was comparable to the EEG signal acquired through the gold standard recording. Volunteers performed movements including opening eyes, closing eyes and tapping aEEG leads during recordings to more closely represent a clinical environment. Adult heart rate cannot be recorded through placement of FSEs on the scalp. Therefore, as a surrogate, an FSE was placed non-invasively in contact with the skin over the radial pulse of an adult volunteer to monitor heart rate when attached to the signal splitter as proof of principle.
Data analysis
Analysis of the amplitude integrated EEG recordings was performed offline by 2 researchers, who were blinded to the data acquisition and the conduct of the study. The total duration of the aEEG was recorded. One of the researchers removed the artefact from the recording. Artefact was defined as impedance greater than 10k ohms as shown on the CFM device with a red marker. An independent researcher (DO) read the raw EEG trace to quantify the real EEG signal. This was then quantified as percentage of interpretable signal from aEEG recording. aEEG traces and gold standard EEG traces were directly compared.
Results
Stage 1
The average percentage of interpretable aEEG signal for each engineered design was: (A) 60.3%, (B) 29.7%, (C) 77.6%, (D) 67.9% and FEMS signal splitter 60.3%. demonstrates the percentage of interpretable aEEG signal from the total aEEG recording for each adult volunteer stratified by engineered design. A poor aEEG signal was seen in two of the three group B volunteers.
Figure 2. Graph showing percentage of good signal in total aEEG recording for each connector design (A, B, C, D), the foetal heart rate and aEEG monitoring system (FEMS) signal splitter and direct FSE application with FEMS. Data for each individual volunteer and the mean.
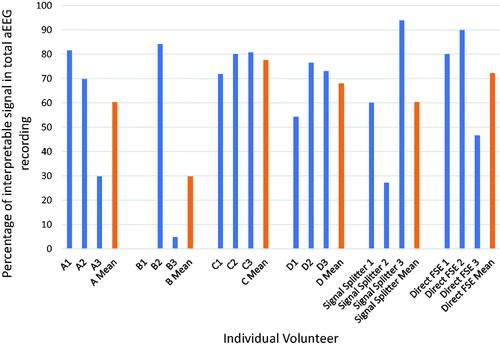
These results confirm that probe design is an essential component to achieving a usable aEEG signal. The poor SNR exhibited by probe B resulted in very little usable signal, as was expected. Surprisingly, probe C performed better than probes A and D. From this, we can deduce that having a ground with some distance from the measurement sites is beneficial, as some of the aEEG signal may be present in the vicinity of the measurement site, thereby inducing the same signal in the ground (reference) connection and weakening the overall SNR.
Stage 2
Direct FSE application with the FEMS signal splitter resulted in an average percentage of interpretable aEEG signal of 72.2% as seen in . FEMS further facilitated adult heart rate monitoring when an FSE hook was placed in contact with the skin over the radial pulse of an adult volunteer.
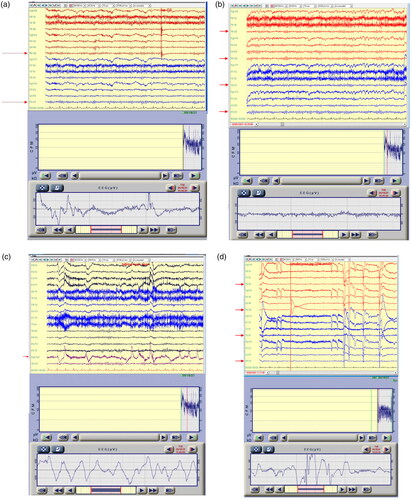
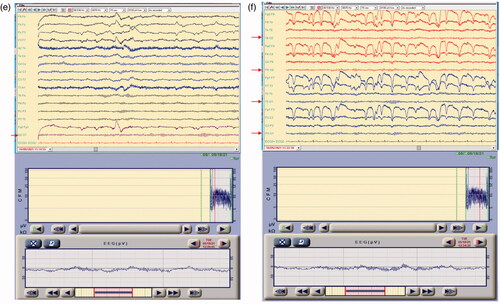
As is demonstrated in , the EEG signal on the aEEG device showed a similar trace to that recorded through the gold standard EEG at the commencement of the recording. demonstrates similarity between EEG signal obtained through multichannel gold standard EEG and single channel FSE acquired EEG in similar locations. further illustrates similarity between single channel FSE acquired EEG and signal obtained through gold standard EEG from multiple channels. These findings were further represented while opening eyes, closing of eyes, talking and tapping the aEEG electrode (). demonstrates the signal arising from single channel EEG is capable of summarising EEG data from multiple channels of multichannel EEG across locations.
Figure 3. Top of each subfigure demonstrates gold standard multichannel EEG recording over 15 s; bottom of each subfigure represents simultaneous single channel raw EEG obtained through FSE application over 15 s. (A) EEG signal on the aEEG device recorded using FSE showing trace similar to that seen in the EEG recording acquired using 19 scalp sensors at the commencement of the recording. Red arrows indicates the approximate location of the foetal scalp electrodes. (B and C): EEG and aEEG recording showing similar EEG signal during no movement (3B) and whilst talking and opening eyes (3C). Red arrows indicates the approximate location of the foetal scalp electrodes. (D and E) Simultaneous EEG and aEEG recording showing the signal changes captured during tapping the aEEG electrode and P4 EEG electrode (3D) and during no movement (3E). Red arrows in the EEG recording indicates the signal acquired around the sites of the foetal scalp electrode. (F) Simultaneous EEG and aEEG recording showing the summary EEG signal on the aEEG device that is capturing the predominant signal on EEG recording from the brain regions that was closer to the foetal scalp electrode sites. Red arrows in the EEG recording indicates the signal acquired around the sites of the foetal scalp electrode.
Discussion
Here we demonstrate proof of principle for human aEEG monitoring through the development of FEMS. The authors believe this is the first demonstration of the feasibility of this approach in human volunteers utilising FSEs from routine clinical practice. Overall, this represents an exciting prospect for a novel method of foetal monitoring in the future through simultaneous foetal aEEG and FHR monitoring in labour.
Through direct application of FSEs to the adult scalp, a good EEG signal was obtained for over 70% of recording time on average. Furthermore, the signal achieved through this method was similar to gold standard EEG monitoring, evidencing accurate measurement of the EEG signal. This was maintained despite eye movements, talking and tapping of the electrode, mimicking the movements of the clinical scenario of labour. As such, aEEG monitoring through FEMS is a feasible and representative method of EEG monitoring in humans. We also demonstrated heart rate recording via FEMS allowing simultaneous foetal aEEG and heart rate monitoring in labour. This will allow concomitant CTG and aEEG recording, essential for technological development and comparisons to current gold standard foetal monitoring techniques. FSE attachment to the adult scalp does not reliably detect heart rate. However, placement of the electrode over the radial pulse remedies this and as such was used as a surrogate in this study.
aEEG is a routinely used technique to monitor the electrocortical activity of both term and preterm infants in neonatal intensive care units worldwide. It not only allows for information predicting future neurological outcomes, but is also used to aid selection of infants for therapeutic cooling (Azzopardi et al. Citation2009; Bruns et al. Citation2017). Its use is firmly established in the neonatal period, with a wealth of experience of use. The ability to extrapolate this technology to intrapartum foetal monitoring would be invaluable with the potential of monitoring brain function directly in labour as opposed to surrogate markers. Evidence from animal studies illustrates that the intrapartum aEEG signal reflects evolving hypoxia and asphyxia (Frasch et al. Citation2015; Frasch et al. Citation2017). Previously, proof of principle study utilising a suction device on the scalp of foetuses satisfactorily monitored EEG and FHR in labour in 15 foetuses (Maynard et al. Citation1979). The technologies and evidence presented in this study offer a unique method of translating aEEG monitoring to clinical practice utilising FSEs, a well-established routine foetal monitoring modality.
Whilst this approach to foetal monitoring has several benefits, there are some limitations. The requirement to attach 2 FSEs to the foetal scalp is necessary to facilitate signal capture. Whilst the application of FSEs in labour is commonplace, and is accepted for other forms of foetal monitoring such as ST-analysis, it is an invasive procedure that not all patients accept. Furthermore, it limits use of such technologies to labour with amniorrhexis as opposed to antenatal applications. The risk of serious injury from foetal scalp electrode application is rare, with the frequency of minor complications such as cephalohaematoma or scalp injury low. A recent study looking at over 130,000 vaginal births, suggested that there was a 1.0% risk of cephalohaematoma, and 1.2% risk of scalp injury with FSE. However, the risk of both was 0.9% when an FSE was not used (Kawakita et al. Citation2016). In current practice, the benefits of accurate foetal monitoring with a foetal scalp electrode far outweigh the risks of the application if the abdominal monitoring is inadequate. We believe the same judgement will be made in the future with foetal EEG as a monitoring modality, where the risks of an additional foetal scalp electrode will be far outweighed by the benefits of accurate intrapartum foetal monitoring. It will be necessary to establish a pre-threshold change in aEEG signal prior to neurological injury to facilitate its use as a practical tool in labour. The current study has been performed in adults where potential variables such as amniotic fluid, blood and maternal tissues are not present. The addition of these factors in the environment could influence the aEEG waveforms. This requires further investigation in clinical study.
Further optimisation of the technology will be required to improve the percentage of good EEG signal in recordings, with further validation in foetuses in a proof of principle study. This will be achieved through use of FEMS to achieve simultaneous aEEG and FHR signal in foetuses of labouring women. Through this approach we hope to develop a robust method for detecting evolving intrapartum foetal hypoxia leading to brain dysfunction.
Acknowledgements
Mr Philip Blackwell and Ms Lydia Staniaszek, clinical neurophysiology, University Hospitals Bristol & Weston NHS Trust for acquiring the EEG from the volunteers.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Alfirevic Z, Devane D, Gyte GM, Cuthbert A. 2017. Continuous cardiotocography (CTG) as a form of electronic fetal monitoring (EFM) for fetal assessment during labour. The Cochrane Database of Systematic Reviews 2:Cd006066.
- Azzopardi DV, Strohm B, Edwards AD, Dyet L, Halliday HL, Juszczak E, et al. 2009. Moderate hypothermia to treat perinatal asphyxial encephalopathy. The New England Journal of Medicine 361:1349–1358.
- Bruns N, Blumenthal S, Meyer I, Klose-Verschuur S, Felderhoff-Müser U, Müller H. 2017. Application of an amplitude-integrated EEG monitor (cerebral function monitor) to neonates. Journal of Visualized Experiments (127):55985.
- Chakkarapani E, Thoresen M. 2015. The newborn pig global hypoxic-ischemic model of perinatal brain and organ injury. In: Yager JY, editor. Animal models of the developmental disabilities. New York, NY: Humana Press/Springer.
- Department of Health and Social Care. 2015. New ambition to halve rate of stillbirths and infant death [online]. [cited 2021 Nov 2]. Available from: https://www.gov.uk/government/news/new-ambition-to-halve-rate-of-stillbirths-and-infant-deaths
- Frasch MG, Boylan GB, Wu HT, Devane D. 2017. Commentary: computerised interpretation of fetal heart rate during labour (INFANT): a randomised controlled trial. Frontiers in Physiology 8:721.
- Frasch MG, Durosier LD, Gold N, Cao M, Matushewski B, Keenliside L, et al. 2015. Adaptive shut-down of EEG activity predicts critical acidemia in the near-term ovine fetus. Physiological Reports 3:e12435.
- Gale C, Statnikov Y, Jawad S, Uthaya SN, Modi N, Modi N, et al. 2018. Neonatal brain injuries in England: population-based incidence derived from routinely recorded clinical data held in the National Neonatal Research Database. Archives of Disease in Childhood. Fetal and Neonatal Edition 103:F301–F306.
- Kawakita T, Reddy UM, Landy HJ, Iqbal SN, Huang CC, Grantz KL. 2016. Neonatal complications associated with use of fetal scalp electrode: a retrospective study. BJOG : An International Journal of Obstetrics and Gynaecology 123:1797–1803.
- Lee-Kelland R, Jary S, Tonks J, Cowan FM, Thoresen M, Chakkarapani E. 2020. School-age outcomes of children without cerebral palsy cooled for neonatal hypoxic-ischaemic encephalopathy in 2008-2010. Archives of Disease in Childhood. Fetal and Neonatal Edition 105:8–13.
- Liu X, Jary S, Cowan F, Thoresen M. 2017. Reduced infancy and childhood epilepsy following hypothermia-treated neonatal encephalopathy. Epilepsia 58:1902–1911.
- Maynard DE, Cohen RJ, Viniker DA. 1979. Intrapartum fetal monitoring with the cerebral function monitor. British Journal of Obstetrics and Gynaecology 86:941–947.
- National Institute for Health and Care Excellence. 2010. Therapeutic hypothermia with intracorporal temperature monitoring for hypoxic perinatal brain injury. Interventional Procedures Guidance [IPG347] [online]. [cited 2021 Nov 2]. Available from: https://www.nice.org.uk/guidance/ipg347
- National Institute for Health and Care Excellence. 2017. Intrapartum care for healthy women and babies [online]. [cited 2021 Nov 2]. Available from: https://www.nice.org.uk/guidance/cg190/chapter/Recommendations#monitoring-during-labour
- Neilson JP. 2015. Fetal electrocardiogram (ECG) for fetal monitoring during labour. The Cochrane Database of Systematic Reviews 5:Cd000116.
- Toet MC, Lemmers PM. 2009. Brain monitoring in neonates. Early Human Development 85:77–84.