

Abstract
Massive uterine bleeding occurring after delivery is in most cases unpredictable and can have fatal consequences. This article presents the technique of combining the twisting of uterus on a 90° rotation on its axis and positioning a sling around the cervix, allowing to decrease incoming blood flow from uterine and ovarian arteries. The aim of this easy-to-use procedure is to enable surgeons and anaesthesiologists to respectively ensure the presence of an experienced surgeon and to stabilise the haemodynamic of the patient. It is a modus operandi of particular interest in resources’ challenged environments.
Introduction
Caesarean section (c-section) is one of the most widely performed surgery procedures. Among the feared complications, massive bleeding may occur due to uterine atony, accreta spectrum or vascular lesions. Prompt reaction to bleeding during surgery will be lifesaving (Hawkins Citation2020). Although procedures have evolved (Wilson Citation1945), there is a wide disparity in access to advanced techniques. The simple procedure of cervical sling can be performed by any surgeon when massive uterine bleeding occurs. The purpose of the technique is to be an intermediate step in bleeding control by compression of uterine and descending cervical arteries, in order to provide enough time to both surgical team to call on an experienced surgeon for support and for the anaesthesiologists to stabilise the patient, within good conditions and minimal additional blood loss.
It can be performed under various conditions of uterine born bleedings from uterine origin, such as the whole placenta accreta spectrum, but also for myomectomies, vascular severing of uterine veins or arteries, major praevia localisation of the placenta and the like. This technique was performed on several patients in our institution, as stated in the video, with excellent clinical results.
Technique
Our proposed solution is a simple, reproducible manoeuvre that can be performed during c-section procedures. As demonstrated in the video (Supplemental online material: video of cervical sling and B-Lynch procedure), we proceed in four major steps.
Step 1: uterine twist + cervical sling
The surgeon proceeds to a uterine twist on its axis (). The direct anatomical effect is reduction of the blood flow issued from the uterine veins and arteries through their compression. Risk of uterine vessels’ laceration is regarded as low.
Figure 1. Uterus with 90° twist (arrow) and cervical sling (held in left hand) placed at cervix height, for blood supply blockage.
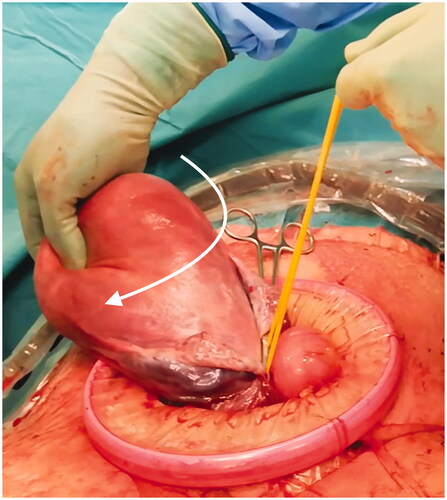
Second part of bleeding control is managed through strapping the utero-vaginal junction with a Foley catheter (elastic – soft and of upper diameter). This material is preferred in order to avoid tissues’ damage that may occur with other sling material such as suture thread or long surgical swab. A knot can be performed but clamping the two ends of the Foley with a Kocher clamp allows to adjust tension during intervention. First step is satisfactory when the uterus slightly changes colour to bluish due to venous congestion.
Step 2: stabilisation of haemodynamics and call for help
Stabilisation of haemodynamics by the anaesthesiologists, with an appropriate vascular access, then intra-vascular filling with crystalloids, blood, plasma and platelets transfusion. Concomitant call for senior or most experienced surgeons help is suggested. Infusion of utero-tonic medication such as oxytocin or sulprostone should be initiated.
Step 3: B-Lynch procedure
Adapted from the original procedure of B-Lynch et al. (Citation1997), we use Polyglactin 910 (Vicryl™ (Ethicon®) 1 or Mitsu™(Merillife®)) suture of min. Seventy centimetres length, with straight needle or Reverdin’s needle (Matsuzaki et al. Citation2019).
After de-twisting the uterus but maintaining the cervical sling, the first step is to exit threads from the cavity on the posterior wall from the uterus at A and B (video). The two strands of the suture are looped over the fundus, like suspenders, and then re-entered into the uterine cavity anteriorly at C and D, on the upper edge of the hysterorrhaphy. It is then exited from the lower edge of the hysterorrhaphy at E and F, which are directly below C and D, respectively. The uterus is rolled from the fundus, emptied and very tightly maintained. The two strands are tied together, ending the original B-Lynch procedure. Tying the two suspenders together allows them not to slip when the uterus will contract. Additional rolling up carpeting knots can be performed to lower even more the uterine volume.
Step 4: termination of procedure
Afterward, removal of Foley’s catheter, and termination of the c-section procedure are achieved.
Discussion
The present article highlights the importance of an easy-to-perform technique when massive uterine bleeding occurs. With only limited material at hand, it can be performed by junior surgeons. The two main goals are to provide enough time to the anaesthesiologist for fluids resuscitation, eventually induce general anaesthesia and more importantly call for the help of senior surgeons. The B-Lynch technique is a procedure that is not often taught, as it does usually happen in critical timing. The cervical sling allows to process with a quasi-blood-less uterus. Compared to other procedures for uterine atony and haemorrhage management (uterine artery ligation, intrauterine balloon, hysterectomy and radioembolisation), the cervical sling has the advantage to be faster, cheaper and not requiring specific training (fast learning curve).
The cervical sling is less pervasive and has been safely performed at our institute without any per and post-operative complications, but results may not be generalised as of today.
Conclusions
Uterine twist and cervical sling procedures can be easily performed by surgeons. It is safe and intuitive. It allows team to earn time to call for senior help and stabilise haemodynamic of the patient.
Ethics statement
The present study follows the principles of the Declaration of Helsinki.
Patient consent
Informed consent was obtained from all individual participants included in the study.
Supplemental Material
Download MP4 Video (42.8 MB)Acknowledgements
The authors would like to thank Sophie Pache for Video’s audio.
Disclosure statement
No potential competing interest was reported by the authors.
Related Research Data
References
- B-Lynch C, Coker A, Lawal AH, Abu J, Cowen MJ. 1997. The B-Lynch surgical technique for the control of massive postpartum haemorrhage: an alternative to hysterectomy? Five cases reported. British Journal of Obstetrics and Gynaecology 104:372–375.
- Hawkins JL. 2020. Obstetric hemorrhage. Anesthesiology Clinics 38:839–858.
- Matsuzaki S, Jitsumori M, Hara T, Matsuzaki S, Nakagawa S, Miyake T, et al. 2019. Systematic review on the needle and suture types for uterine compression sutures: a literature review. BMC Surgery 19:196.
- Wilson KM. 1945. The role of Porro cesarean section in modern obstetrics. American Journal of Obstetrics and Gynecology 50:761–764.