

Abstract
A random-effects meta-analysis was performed in English and Chinese databases since its inception to August 2020 to assess the incidence, causes and severity of acute pancreatitis (AP) at various stages of pregnancy, maternal and foetal mortality. A total of 154 articles representing 4034 patients with AP during pregnancy in China were included for the analysis. The incidence of AP during pregnancy was 0.0469 (95% confidence interval [CI], 0.0349; 0.0627) in the first trimester, whereas it was 0.2518 (95% CI, 0.2210; 0.2854) and 0.6323 (95% CI, 0.5870; 0.6753) in the second and third trimester, respectively. The major causes of AP were hypertriglyceridaemia (0.351 [95% CI, 0.3202; 0.3834]) and biliary pancreatitis (0.424 [95% CI, 0.4094; 0.5002]). The severity of AP was mild in majority of the patients. The incidence of AP at maternal mortality was 0.0184 (95% CI, 0.0126; 0.0269) and foetal mortality was 0.1018 (95% CI, 0.0867; 0.1192). Our meta-analysis revealed that hypertriglyceridaemia and biliary pancreatitis remain the major causes of AP during pregnancy. Foetal mortality requires further investigation.
What is already known on this subject? Acute pancreatitis (AP) in pregnant women is characterised by acute onset and delay in understanding the interaction of the metabolic changes with pancreatic pathophysiology, and thus becomes difficult to diagnose the disease and provide timely treatment to the patients. This poses a greater health risk among women and their foetus by increasing their chances of mortality.
What the results of this study add? We performed an exhaustive, random-effects meta-analysis involving 154 articles representing 4034 patients to assess the incidence of AP at various stages of pregnancy, the causes of AP and the severity of AP during pregnancy, maternal and foetal mortality.
What are the implications of these findings for clinical practice and/or further research? Our meta-analysis revealed that hypertriglyceridaemia and biliary pancreatitis remain the major causes of AP during pregnancy. Although the rates of maternal mortality have decreased in the recent years, foetal mortality still remains high and requires further investigation.
IMPACT STATEMENT
Introduction
Pregnancy is associated with physiological changes that alter the presenting symptoms and signs of many disease processes (Hernandez et al. Citation2007). Acute pancreatitis (AP) during pregnancy though rare is associated with incidence rate of 1 per 1000–10,000 pregnancies (Eddy et al. Citation2008; Pitchumoni and Yegneswaran Citation2009; Igbinosa et al. Citation2013). AP during pregnancy is more frequent in multiparous women (Ramin et al. Citation19952011; Igbinosa et al. Citation2013). Also, it is more common in East Asian countries, with an incidence rate of 0.227–4.25% (Sun et al. Citation2011; Zhang et al. Citation2013). In Asian countries, cholelithiasis is more common than in the Western world, which may explain the differences in morbidity to AP (Tazuma Citation2006). A study reported that AP was more common in Asian women, and they are more likely to die of AP than their Caucasian counterparts (McNabb-Baltar et al. Citation2014).
Nevertheless, AP in pregnant women is characterised by acute onset and delay in understanding the interaction of the metabolic changes with pancreatic pathophysiology, and thus becomes difficult to diagnose the disease and provide timely treatment to the patients (Pitchumoni and Yegneswaran Citation2009). This poses a greater health risk among women and their foetus by increasing their chances of mortality (Pitchumoni and Yegneswaran Citation2009). Earlier, the maternal-foetal mortality rate was high (37% and 60%, respectively), which has decreased in the recent years to 1% and 0–18%, respectively (Papadakis et al. Citation2011). This can be attributed to earlier diagnosis and dynamic improvement in maternal and neonatal intensive care (Ducarme et al. Citation2014). Besides, the causes of AP during pregnancy can be different similar to the causes that are in non-pregnant women (Ducarme et al. Citation2014). The common identified causes of AP during pregnancy include gallstones (66%), alcohol abuse (12%), hyperlipidaemia (4%), idiopathic (17%), obesity and occasionally trauma, hyperparathyroidism, medication and fatty liver of pregnancy (Eddy et al. Citation2008; Pitchumoni and Yegneswaran Citation2009; Papadakis et al. Citation2011; Igbinosa et al. Citation2013).
Given the low incidence rate and limited clinical data in China regarding the disease, there remains an uncertainty regarding diagnosis and treatment of AP during pregnancy. A study from 36 cases of AP during pregnancy reported that hypertriglyceridaemia was associated with poor outcomes of the disease (Xu et al. Citation2015). The most recent study identified an association between foetal distress and foetal loss with severity of AP during pregnancy (Tang et al. Citation2018). These findings reiterate the significance of precise diagnosis and care for AP during pregnancy in reducing maternal and foetal mortality. Furthermore, in China, there are no standardised guidelines for the management of AP during pregnancy, probably due to low incidence rate. To date, there are no meta-analysis evaluating the incidence and mortality rate of AP during pregnancy in China to the best of our knowledge. We therefore aimed at evaluating the incidence of AP during pregnancy at various stages and identifying the potential risk factors for AP during pregnancy along with their implications on maternal mortality and foetal loss in Chinese women.
Methods
Protocol and registration
This meta-analysis was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the number CRD42020220316.
Data search strategy and selection
A systematic literature search was performed in EMBASE and PubMed databases since inception to August 2020. Relevant Chinese articles were searched in CNKI and Wanfang literature databases. The following search string was used with minor variations to suit the database ‘acute pancreatitis’ AND ‘pregnancy’. The corresponding Chinese search string was used for screening articles from respective databases.
Study eligibility criteria
The studies were selected for review based on the following criteria: (1) pregnant women with AP (2) patients belonging to geographical region of China (3) studies reporting outcomes such as incidence of maternal mortality, incidence of foetal loss or infant mortality, causes of AP during pregnancy and incidence of AP at any stage of pregnancy (4) prospective and retrospective observational study (5) eligible studies limited to those published in English and Chinese. The studies were excluded if they are in the following criteria (1) case reports, reviews, meta-analysis, randomised controlled trial (RCTs) or other than observational studies (2) duplicate publications from the same patient population (3) studies reporting outcomes other than stated above (4) studies published in language other than Chinese and English.
Data and quality assessment
Two independent investigators initially reviewed articles through the titles and abstracts to assess whether they met the inclusion criteria. Studies satisfying the inclusion criteria and those with abstracts were retrieved for full-text evaluations. Data from included studies regarding author, year of publication, title, study design, demographics of the study population and outcomes of interest were extracted into standardised MS Office Excel. In addition, the data extraction sheet included the number of patients, percentages and p-value reported for each outcome. The Newcastle-Ottawa scale was used to assess the methodological quality of observational studies. A higher score represented better methodological quality. The quality assessment of each article is available as supplements (Supplementary Table 1).
One of the constraints of a meta-analysis of observational studies is that there are no appropriate tools available for assessing publication bias. We therefore performed a thorough research of the available literature to assess publication bias in observational studies.
Data synthesis and statistical analysis
Heterogeneity (I2) is expected among studies with different populations. To incorporate part of the heterogeneity, a random-effects meta-analysis was used, and a series of subgroup analysis was performed concerning publication year, severity of the disease and aetiology of the disease. Heterogeneity among the results of different studies was examined using Cochran’s Q and I2 statistics. A fixed effects model was used to calculate the pooled effect if I2 was <50% (insignificant heterogeneity), whereas the random effects model was used if I2 was >50% (significant heterogeneity). Baseline characteristics were presented using descriptive statistics. A p value of ≤ .05 was considered statistically significant, wherever applicable. All the inferences at each level of analysis were validated, and the limitations were identified. On the basis of the limitations, the generalised inferences are presented in this study.
Results
Study selection and population characteristics
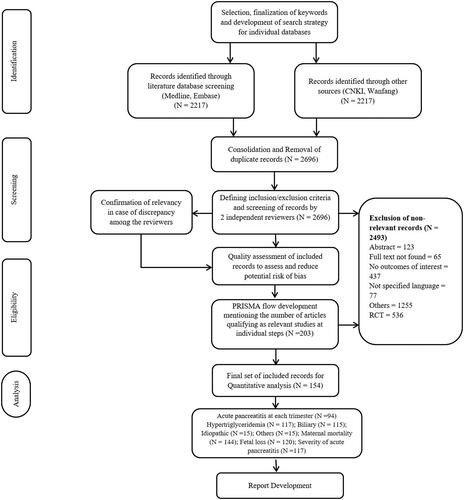
A total of 3643 articles were retrieved from literature search. After removing duplicates and screening for inclusion/exclusion criteria, a total of 155 articles were identified and included in the analysis. represents the PRISMA flowchart for the studies evaluation. The summary characteristics of included studies are presented in Supplementary Table 1.
Figure 1. PRISMA flowchart for selection of studies.
AP during pregnancy in each trimester
The overall incidence of AP in this population was reported in very few studies (19 studies), and it was found to be 0.0009 (95% confidence interval [CI], 0.0001; 0.0145). Of 154 studies, 94 studies (9 English and 85 Chinese) were included for the analysis of the incidence of AP during pregnancy for each trimester. Among these studies, the incidence of AP during pregnancy was found to be 0.0469 (95% CI, 0.0349; 0.0627) in the first trimester, whereas the incidence of AP during pregnancy in the second trimester was 0.2518 (95% CI, 0.2210; 0.2854) and the third trimester was 0.6323 (95% CI, 0.5870; 0.6753; ).
Table 1. Incidences of acute pancreatitis in pregnancy in different subgroups.
AP during pregnancy based on publication year
We divided the included articles based on the publication year as follows: before 2010 and after 2010. Thirty-five articles were found before 2010, whereas 60 articles were included after 2010 for each trimester. The incidence rate of AP during pregnancy before 2010 was 0.0459 (95% CI, 0.0256; 0.0810) in the first trimester, whereas after 2010, it was 0.0469 (95% CI, 0.0334; 0.0655). Similar results were obtained for AP during pregnancy in the second and third trimester ().
Causes of AP during pregnancy
One hundred seventeen articles were included for the analysis of hypertriglyceridaemia as a risk factor. The number of articles analysing biliary pancreatitis, idiopathic and other causes were 115, 15 and 15, respectively. The rate of hypertriglyceridaemia was found to be 0.351 (95% CI, 0.3202; 0.3834), whereas the cause of AP during pregnancy was idiopathic in 0.168 of patients (95% CI, 0.1014; 0.2654) and biliary in 0.424 (95% CI, 0.4094; 0.5002) of patients ().
Severity of AP during pregnancy
Mild and severe forms of AP during pregnancy were reported in 117 articles. For the number of years, the incidence rate of mild AP among women was 0.6494 (95% CI, 0.6124; 0.6848) and severe AP was 0.2988 (95% CI, 0.2678; 0.3317) ().
Mortality outcomes
Maternal mortality was reported in 144 studies, whereas foetal loss was reported in 120 studies. The incidence of maternal mortality was found to be 0.0184 (95% CI, 0.0126; 0.0269), whereas foetal loss was found to be 0.1018 (95% CI, 0.0867; 0.1192; ).
Discussion
To our knowledge, this is the first meta-analysis reporting the incidence of AP in terms of severity, aetiology as well as maternal and foetal mortality outcomes in Chinese pregnant women. Our analysis included articles reporting AP during pregnancy for a period of 40 years. The incidence of AP during pregnancy was found to be the highest (63.23%) in the third trimester. This proportion was similar to the previous studies reporting that most AP during pregnancy occurred in the third trimester (Ducarme et al. Citation2014; Vilallonga et al. Citation2014; Luo et al. Citation2018; Yang et al. Citation2020). This might be attributed to the increased compression to the pancreas and gallbladder by the enlarging uterus as the trimester advances, as well as change in steroids that directly affects gallbladder function (Braverman et al. Citation1980). In later stages of pregnancy, incomplete emptying of the gallbladder may lead to the retention of cholesterol crystals, a precursor of cholesterol-gallstone formation (Braverman et al. Citation1980). Increase in serum triglyceride levels due to oestrogen produces hyper viscosity, which leads to ischaemia and acidosis in pancreatic capillaries (Swisher et al. Citation1994). This results in change in bile composition, which may induce the formation of gallstones and sludge (Ducarme et al. Citation2014).
Hypertriglyceridaemia (35%) and biliary pancreatitis (45%) remain the leading causes of AP during pregnancy among women to date. Similar findings were reported by Luo et al. stating that gallstone and hypertriglyceridaemia were the common causes of AP among pregnant Chinese women (Luo et al. Citation2018). One probable reasons for this consistent rise may include a 2-fold to 4-fold increase in plasma triglycerides, particularly in the third trimester of pregnancy (Takaishi et al. Citation2009). A blood triglyceride level >1000 mg/dL is considered as a high risk factor for AP during pregnancy (Athyros et al. Citation2002; Okura et al. Citation2004), although they never reach levels above 300 mg/dL (3.42 mmol/L) (Saharia et al. Citation1977). Nevertheless, patients with abnormal lipid metabolism may experience severe elevations in circulating triglycerides and chylomicrons, which may cause pancreatic circulation-related ischaemic lesions (Saharia et al. Citation1977). A literature reports that lipoprotein lipase mutation is associated with extreme hypertriglyceridaemia during pregnancy (McGladdery and Frohlich Citation2001). Besides, abnormal lipid and glucose metabolism due to high-fat diet is reported to be an important inducer of AP during pregnancy (Gürsoy et al. Citation2006). Contrary to these findings, various studies from the United States indicate that gallstones is the most common cause of AP during pregnancy (>50%) (Pitchumoni and Yegneswaran Citation2009; Tang et al. Citation2010; Mali Citation2016). This may reflect regional differences between Chinese and other populations, and more studies are needed to clarify these findings.
In China, reports from 1980 to 1990 revealed that the incidence of AP during pregnancy was 12.5% (Xiuhai and Yushan Citation1993). Gradually, in recent years, the incidence of AP during pregnancy has improved with articles reporting the incidence rate around 0.1% (Xu et al. Citation2015; Ding and Chou Citation2017; He Fang et al. Citation2017; Tang et al. Citation2018; Wang Xiaowei et al. Citation2018). Similarly, the rate of maternal mortality was very low among this population of patients, indicating an improvement in laboratory tests and imaging techniques leading to early diagnosis (Ramin et al. Citation1995). However, the foetal mortality rate was quite high (10%). A study predicted that gestational trimesters, delayed diagnosis, hypertriglyceridaemia, multiple organ failure, gestational diabetes mellitus and pre-eclampsia are significant predictors of foetal loss (Yang et al. Citation2020). Sun et al. predicted that miscarriages and pre-term infants contributed to foetal loss in the mild group, whereas foetal death and stillbirth contributed to foetal loss in the severe group (Sun et al. Citation2011). The deficit in foetal state monitoring, lack of assessment and management of pregnant women might be the main cause of increased foetal loss of AP during pregnancy (Tang et al. Citation2018). Owing to lack of studies reporting data between severity of AP during pregnancy and maternal and foetal outcomes, a relationship could not be established. However, a study reported that severe AP (44%) was associated with a higher risk of foetal death (Luo et al. Citation2018). Systematic inflammation cytokine explosion is a characteristic of tissue damage in severe AP (Luo et al. Citation2018). A previous study by Sun et al. also indicated that the increased intra-abdominal pressure during severe AP was also associated with a higher risk of foetal death (Sun et al. Citation2015). Furthermore, severe AP during early pregnancy is particularly threatening to foetal life due to the severe onset of the disease (Abdullah et al. Citation2015). Thus, the severity of AP during pregnancy ascertains the risk for neonatal health and maternal and foetal death.
One of the major strengths of this meta-analysis is the inclusion of English and Chinese articles, which gave us an insight to a wider range of studies reporting AP during pregnancy in Chinese population. Secondly, a random effects model was used to pool the data to provide a more conservative estimate. However, there are certain limitations that warranted mention. Owing to the inclusion of limited number of articles that are published in English, a possible bias cannot be eliminated. Also, a limited number of studies assessed the incidences of AP during pregnancy, which could create bias in the analysis and interpretation of results. Occurrence of publication bias cannot be eliminated despite thorough literature search. The pharmacological management of AP during pregnancy could not be assessed because of heterogeneity of treatment reported in various studies. Lastly, limited number of studies reported severity of AP at various trimesters, and thus this parameter could not be assessed.
Conclusion
In conclusion, our study results indicate the lower incidence of AP among Chinese women in the recent years. Analysis reported that hypertriglyceridaemia and biliary pancreatitis still remain the major causes of AP during pregnancy. Moreover, although the rates of maternal mortality have improved with increasing years, AP during pregnancy poses serious threats to the safety of foetus compared with the mother.
Author contributions
Study conception and design: Zhao Haiyan, Peng Na, Gao Yong, Bai Xiumei and Bai Jianying. Acquisition of data: Zhao Haiyan and Peng Na. Analysis and interpretation of data: Zhao Haiyan, Peng Na, Bai Xiumei and Bai Jianying. Drafting of manuscript: Zhao Haiyan and Peng Na. Critical revision: Zhao Haiyan, Peng Na, Gao Yong, Bai Xiumei and Bai Jianying
Supplemental Material
Download MS Word (158.3 KB)Disclosure statement
The authors declare that they have no competing interests.
Data availability statement
Data are available from the author upon request.
Additional information
Funding
References
- Abdullah B, Kathiresan Pillai T, Cheen LH, Ryan RJ. 2015. Severe acute pancreatitis in pregnancy. Case Reports in Obstetrics and Gynecology 2015:1–4.
- Aixia W, Xueqing B. 2011. Clinical nursing of late pregnancy complicated with acute pancreatitis. Journal of Wenzhou Medical College 41:295–296.
- Aiyun S, Honghua L. 2010. Nursing care of 12 pregnant women with severe acute pancreatitis. Chinese Journal of Misdiagnosis 10:4238–4238.
- Anyuan WL, Kai Y, Chunfang X. 2018. Analysis of clinical features of 36 cases of pregnancy complicated with acute pancreatitis. Jiangsu Medicine 44:702–704.
- Athyros VG, Giouleme OI, Nikolaidis NL, Vasiliadis TV, Bouloukos VI, Kontopoulos AG, Eugenidis NP. 2002. Long-term follow-up of patients with acute hypertriglyceridemia-induced pancreatitis. Journal of Clinical Gastroenterology 34:472–475.
- Bangying L. 2013. Nursing experience of pregnancy complicated with pancreatitis. Chinese Folk Medicine 22:132.
- Baochuan Z. 2015. Clinical study of acute pancreatitis in different pregnancy. Mother and Baby World 147–148.
- Beibei Y. 2013. Clinical analysis of 17 cases of acute pancreatitis in late pregnancy. China Health and Nutrition 508–509.
- Bi XD. 2012. Reduce misdiagnosis and pay attention to the diagnosis and treatment of acute pancreatitis during pregnancy. Chinese Journal of Modern Medicine 22:65–68.
- Binbin L, Huahong W. 2017. Analysis of diagnosis and treatment of 12 cases of acute pancreatitis during pregnancy. Chinese Journal of Digestion 37:41–43.
- Bing H, Weiwen Y. 2006. Clinical analysis of 30 cases of pregnancy complicated with acute pancreatitis. In: The 3rd Yangtze River Delta Perinatal Medicine Academic Forum and 2006 Zhejiang Perinatal Medicine Academic Annual Conference Paper Collection. Hangzhou, Zhejiang, China: Zhejiang Medical Association.
- Braverman DZ, Johnson ML, Kern F. 1980. Effects of pregnancy and contraceptive steroids on gallbladder function. The New England Journal of Medicine 302:362–364.
- Changwei Z, Jiayao Z, Yong Z, Jinmei L. 2012. Clinical analysis of 15 cases of acute pancreatitis in late pregnancy. Chinese Medicine Guide 10:496–497.
- Chaoyang W, Hui X, Maimtim D, Samusak T. 2008. Clinical analysis of 20 cases of acute pancreatitis during pregnancy. Xinjiang Medicine 38:14–16.
- Chen H, Haiduo L, Hongfei T, Long C, Zhiqiang Z. 2010. Analysis of diagnosis and treatment of 12 cases of pregnancy complicated with acute pancreatitis. Journal of Hepatobiliary and Pancreatic Surgery 22:314–316.
- Chenmin Y, Zongrong T. 2013. Analysis of clinical diagnosis and treatment of 36 cases of acute pancreatitis during pregnancy. Chinese Medical Science 3:17–19.
- Chensong H, Wei C, Kunsong Z, Jiaming L, Lijian L, Xiaoyu Y. 2018. Analysis of clinical diagnosis and treatment of acute pancreatitis in pregnancy. Chinese General Surgery Literature 12:192–195.
- Chunli Y, Yuquan Z, Xiaobin Z, Lihua P, Guojun C, Wen L. 2015. Analysis of clinical features of acute pancreatitis in pregnancy. Journal of PLA Medical College 36:1022–1024.
- Chunyan H. 2018. Analysis of the effects of prevention and treatment of severe complications of acute pancreatitis in pregnancy. Electronic Journal of Clinical Medicine Literature 5:54.
- Cuiping F, Zheng Z, Xiaoyu P. 2018. Analysis of clinical diagnosis and treatment of 16 cases of pregnancy complicated with acute pancreatitis. Journal of China-Japan Friendship Hospital 32:135–138.
- Ding W, Chou X-W, and Wang, Z. 2017. Clinical analysis of 34 cases of pregnancy complicated with acute pancreatitis. Chinese Obstetric Emergency Electronic Journal 6:112–117.
- Dongmei X, Jianling L, Yingmei X, Shaohua L. 2014. Experience in diagnosis and treatment of 16 cases of pregnancy complicated with acute pancreatitis. Lingnan Modern Clinical Surgery 14:642–645.
- Ducarme G, Maire F, Chatel P, Luton D, Hammel P. 2014. Acute pancreatitis during pregnancy: a review. Journal of Perinatology 34:87–94.
- Eddy JJ, Gideonsen MD, Song JY, Grobman WA, O'Halloran P. 2008. Pancreatitis in pregnancy. Obstetrics and Gynecology 112:1075–1081.
- Fang H, Xiaolin T, Jingjin G, Chunhong S, Yuguo P, Dunjin C. 2017. Analysis of 40 cases of clinical features of pregnancy complicated with pancreatitis. Chinese Journal of Practical Gynecology and Obstetrics 33:1174–1177.
- Feng Z, Baowei H, Chunyou W, Jiongxin X, Chidan W. 2005. Diagnosis and treatment of acute pancreatitis in pregnancy. Journal of Clinical Surgery 411–412.
- Fu H, Hu G, Wu H, Cheng YS. 2018. Analysis of 20 cases of pregnancy complicated with acute pancreatitis. Jilin Medicine 39:528–529.
- Fuming M. 2014. Discussion on clinical diagnosis and treatment of 32 cases of acute pancreatitis during pregnancy. China’s Health Industry 7:132–134.
- Gang W, Bei S, Jun X, Chang L, Zunqiang Li Jun Z, Jinpeng Z, et al. 2004. Clinical analysis of 12 cases of acute pancreatitis during pregnancy. Journal of Harbin Medical University 570–572.
- Gang Z, Jie Y, Li Y, Zhou L, Jianhuan T, Xun Y, Xiaohui Z, Jian W. 2007. Clinical features, diagnosis and treatment strategies of acute pancreatitis in pregnancy (a report of 31 cases). In: 2007’ International General Surgery Forum and the 14th National General Surgery Basic and Clinical Progress Academic Exchange Conference Paper Collection. 成都: Chinese Medical Association, Editorial Department of Chinese Medical Journal. p. 204–207.
- Geng Y, Li W, Sun L, Tong Z, Li N, Li J. 2011. Severe acute pancreatitis during pregnancy: eleven years experience from a surgical intensive care unit. Digestive Diseases and Sciences 56:3672–3677.
- Guixiang L, Qian Z, Benhui C. 2007. Nursing care of acute pancreatitis during pregnancy. West China Medicine 391–392.
- Gürsoy A, Kulaksizoglu M, Sahin M, Ertugrul DT, Ozer F, Tutuncu NB, Demirag NG. 2006. Severe hypertriglyceridemia-induced pancreatitis during pregnancy. Journal of the National Medical Association 98:655–657.
- Haiping X, Bin X, Wei L. 2008. Nursing care of 12 cases of pregnancy complicated with acute pancreatitis. Chinese Journal of Coal Industry Medicine 1603.
- Haiyan L, Weiqin L, Wenkui Y. 2006. Analysis of clinical characteristics of pancreatitis of pregnancy. In: Paper compilation of the 11th National Pancreatic Surgery Symposium of Chinese Medical Association. p. 1.
- Hernandez A, Petrov MS, Brooks DC, Banks PA, Ashley SW, Tavakkolizadeh A. 2007. Acute pancreatitis and pregnancy: a 10-year single center experience. Journal of Gastrointestinal Surgery 11:1623–1627.
- Hong Y. 2013. Nursing experience of patients with acute pancreatitis during perinatal period. Chinese Medicine 8:867–868.
- Hongqiong D, Xiangying Z. 2012. Clinical nursing of 14 cases of severe acute pancreatitis in late pregnancy. Qilu Nursing Journal 18:83–85.
- Hongzhen L, Weili L, Yun Z. 2006. Nursing experience of pregnancy complicated with acute pancreatitis. National Surgery. Neurosurgery Nursing Academic Exchange and Special Lecture Conference Paper Collection 2.
- Huang L, Min H. 2012. Clinical analysis of 61 cases of acute pancreatitis during pregnancy. Chinese Journal of Obstetrics and Gynecology 13:458–459.
- Huang Q, Minhua L, Jinxiu D, Xiande Y, Jinshun Z. 2010. Analysis of diagnosis and treatment of 24 cases of pregnancy complicated with acute pancreatitis. Zhejiang Practical Medicine 15:383–384 + 394.
- Huang J, Yan H. 2009. Clinical analysis of 12 cases of pregnancy complicated with acute pancreatitis. Modern Chinese Doctor 47:66–71.
- Huang C, Liu J, Lu Y, Fan J, Wang X, Liu J, et al. 2016. Clinical features and treatment of hypertriglyceridemia-induced acute pancreatitis during pregnancy: a retrospective study. Journal of Clinical Apheresis 31:571–578.
- Huáng Gao L. 2013. Clinical diagnosis and treatment of 21 cases of pregnancy complicated with acute pancreatitis. China’s Health Industry 10:93–94.
- Huánghǎi QZ, Qín’ān c, wěi fēng Q. 2013. Analysis of clinical diagnosis and treatment of 32 cases of pregnancy complicated with acute pancreatitis. Journal of Clinical Surgery 21:943–944.
- Huaping L, Yajuan H. 2012. Retrospective analysis of 19 cases of pregnancy complicated with acute pancreatitis. Chinese Journal of Practical Gynecology and Obstetrics 28:131–133.
- Huilan S, Hanqing W, Weixiang O. 2010. Analysis of diagnosis and treatment of 36 cases of pregnancy complicated with acute pancreatitis. Chinese Journal of Critical Care Medicine 3:109–112.
- Igbinosa O, Poddar S, Pitchumoni C. 2013. Pregnancy associated pancreatitis revisited. Clinics and Research in Hepatology and Gastroenterology 37:177–181.
- Jiakui Y, Gang Y. 2014. Analysis and treatment of characteristics of acute pancreatitis in pregnancy. Chinese Community Physician 30:50–51.
- Jian P, Ping Z, Xiaohong X, Xiong H. 2009. Diagnosis and treatment of acute pancreatitis during pregnancy: a report of 48 cases. Chinese Journal of General Surgery 18:212–214.
- Jiancheng W, Xiao Z, Jianfeng Y. 2009. Clinical features, diagnosis and treatment of acute pancreatitis in pregnancy. Zhejiang Medicine 31:1654–1656.
- Jiangliu X, Chen L, Wenjie L, Hongxia Z, Yang Z. 2016. Analysis of clinical diagnosis and treatment of acute pancreatitis in pregnancy. China Practical Medicine 11:10–12.
- Jiangping H, Ming D. 2017. Analysis of clinical diagnosis and treatment of 40 cases of pregnancy complicated with acute pancreatitis. Diet Health 4:126–127.
- Jiayuan H. 2009. Nursing experience of 15 cases of pregnancy complicated with pancreatitis. Modern Journal of Integrated Traditional Chinese and Western Medicine 18:1797–1799.
- Jiming M, Junhong H. 2006. Diagnosis and treatment of 12 cases of acute pancreatitis during pregnancy. Journal of the Fourth Military Medical University 798.
- Jin X, Xianmin B. 2018. Clinical characteristics and treatment experience of acute pancreatitis in the middle and late pregnancy. Chinese Journal of General Surgery 17:2–209.
- Jing Y, Fei M, Xiaowei T, Xia C, Yan P. 2019. Analysis of clinical features and prognosis of acute pancreatitis in pregnancy. Journal of Clinical Hepatobiliary Disease 35:138–142.
- Jin X, Xianmin B, Xianwei D. 2008. Treatment of 23 cases of acute pancreatitis in middle and late pregnancy. World Chinese Journal of Digestion 548–550.
- Jin J, Yu Y, Zhong M, Zhang G. 2015. Analyzing and identifying risk factors for acute pancreatitis with different etiologies in pregnancy. The Journal of Maternal-Fetal & Neonatal Medicine 28:267–271.
- Ju X, Yan Z, Rong Z. 2009. Clinical characteristics and outcome analysis of 62 cases of pregnancy complicated with acute pancreatitis in different periods. Journal of Practical Obstetrics and Gynecology 25:352–354.
- Jú X. 2011. Experience in the treatment of 10 cases of pregnancy complicated with pancreatitis. Chinese and Foreign Health Digest 08:46–47.
- Jun W. 2011. Analysis of diagnosis and treatment of 19 cases of acute pancreatitis during pregnancy. Journal of Bengbu Medical College 36:813–814 + 817.
- Junxu L, Yi S. 2009. Analysis of diagnosis and treatment of 20 cases of acute pancreatitis during pregnancy. Chinese Medicine and Clinic 9:1232–1233.
- Kongdi J, Xuefeng W, Bin G, Huisen Y. 2015. Analysis of the influence of pregnancy complicated with acute pancreatitis on pregnancy outcome. Huaihai Medicine 33:558–559.
- Li L. 2015. Clinical analysis and treatment of acute pancreatitis in pregnancy. China Rural Health 27.
- Lianwu Z, Honggang Y, Lei S. 2011. 20 cases of acute pancreatitis during pregnancy. World Chinese Journal of Digestion 19:1311–1313.
- Lianying Z, Shumin L. 2010. Imaging and clinical exploration of 68 cases of acute pancreatitis during pregnancy. China Maternal and Child Health 25:4648.
- Liheng C, Xiaozhong J, Yong Z, Yiping D, Lunan Y, Guang G, et al. 2008. Analysis of clinical diagnosis and treatment of acute pancreatitis during pregnancy. Chinese Journal of Basic and Clinical Medicine 58–60.
- Li W, Hongqiong D, Xiaoyan Z. 2006. Nursing care of patients with acute pancreatitis during pregnancy. Journal of Nursing 32–33.
- Li H, Huang Y, Chen X. 2011. Acute pancreatitis in pregnancy: a 6-year single center clinical experience. Chinese Medical Journal 124:2771–2775.
- Lihui Zhang Ai J, Li Hejiang L. 2003. Acute pancreatitis in pregnancy. Journal of Physician Training 36–37.
- Li H-l, Jiang Y-h, Wei Y, Zhao Y-y, Zhu X, Yao G-q. 2014. Clinical analysis of acute pancreatitis during pregnancy and postpartum. Beijing da Xue Xue Bao. Yi Xue Ban = Journal of Peking University. Health Sciences 46:125–129.
- Li W, Limin D, Tao S, Xiangzhen G. 2004. Analysis of 14 cases of pregnancy complicated with acute pancreatitis. Chinese Journal of Practical Gynecology and Obstetrics 60–61.
- Liping S, Jinfeng S. 2007. Clinical analysis of 31 cases of pregnancy complicated with acute pancreatitis. Zhejiang Clinical Medicine 881–882.
- Liping Z, Hong W, Xiao WYW. 2015. Experience in diagnosis and treatment of 14 cases of pregnancy complicated with acute pancreatitis. Chinese Medical Science 5:78–81.
- Liu C. 2009. Diagnosis and treatment of acute pancreatitis during pregnancy. Modern Practical Medicine 21:950–951.
- Liwei H, Hang Y, Jingbo Z, Fei W. 2004. Clinical analysis of 12 cases of acute pancreatitis during pregnancy. Chinese Journal of Modern Medicine 106–108.
- Luo L, Zen H, Xu H, Zhu Y, Liu P, Xia L, et al. 2018. Clinical characteristics of acute pancreatitis in pregnancy: experience based on 121 cases. Archives of Gynecology and Obstetrics 297:333–339.
- Mali P. 2016. Pancreatitis in pregnancy: etiology, diagnosis, treatment, and outcomes. Hepatobiliary & Pancreatic Diseases International 15:434–438.
- McGladdery SH, Frohlich JJ. 2001. Lipoprotein lipase and apoE polymorphisms: relationship to hypertriglyceridemia during pregnancy. Journal of Lipid Research 42:1905–1912.
- McNabb-Baltar J, Lee L, Banks P, Conwell D. 2014. Acute pancreatitis in pregnancy: a report from the nationwide inpatient sample: 285. American Journal of Gastroenterology 109:S88.
- Mei L, Rong Y. 2017. Diagnosis and treatment of acute pancreatitis during pregnancy. Medical Theory and Practice 30:3378–3379.
- Meifeng Z, Sixin L. 2009. Report of 10 cases of acute pancreatitis during pregnancy. Practical Clinical Medicine 10:79–79.
- Min P, Daomiao X, Yuhang A, Shuangping Z. 2012. Analysis of diagnosis and treatment of 30 cases of pregnancy complicated with acute pancreatitis. Progress in Modern Obstetrics and Gynecology 21:413–414 + 416.
- Mingyin L, Meng Z, yuǎn J. z, Min Z, Ping Z, Haoming L. 2012. Treatment and prognosis of 25 cases of acute pancreatitis during pregnancy. Abdominal Surgery 25:164–165.
- Mingyin L, Meng Z, zhì yuǎn J, Min Z, Ping Z. 2010. Treatment and prognosis of 25 cases of pregnancy complicated with pancreatitis. In: Proceedings of the 4th Cross-Strait General Surgery Symposium and China Clinical General Surgery Frontiers and Debate Summit Forum. Zhǎngchūn: Tongji Hospital. p. 213–214.
- Nóng guān l. 2019. Analysis of clinical features of acute pancreatitis in pregnancy. Mǔ Yīng Shìjiè 106.
- Nong Y. 2005. Nursing experience of 16 cases of pregnancy complicated with acute pancreatitis. She Zhi 211–212.
- Okura Y, Hayashi K, Shingu T, Kajiyama G, Nakashima Y, Saku K. 2004. Diagnostic evaluation of acute pancreatitis in two patients with hypertriglyceridemia. World Journal of Gastroenterology 10:3691–3695.
- Papadakis EP, Sarigianni M, Mikhailidis DP, Mamopoulos A, Karagiannis V. 2011. Acute pancreatitis in pregnancy: an overview. European Journal of Obstetrics, Gynecology, and Reproductive Biology 159:261–266.
- Pingming G, Xin Z, Chengli Y, Naidong H. 2012. Diagnosis and treatment of pancreatitis in pregnancy. Chinese and Foreign Medical 31:37–38.
- Pitchumoni CS, Yegneswaran B. 2009. Acute pancreatitis in pregnancy. World Journal of Gastroenterology 15:5641–5646.
- Qian X, Jingtong W. 2013. Analysis of clinical features of acute pancreatitis during pregnancy. China Comprehensive Clinic 29:1182–1185.
- Qihui C, Xiping Z, Xianfeng D. 2012. Clinical study on acute pancreatitis in pregnancy in 26 cases. Gastroenterology Research and Practice 2012:271925.
- Ramin KD, Ramin SM, Richey SD, Cunningham FG. 1995. Acute pancreatitis in pregnancy. American Journal of Obstetrics and Gynecology 173:187–191.
- Renmei X, Yongming B, Wuhua T. 2019. Influence of pregnancy with acute pancreatitis on maternal and infant outcome. Chinese Primary Medicine 2976–2979.
- Rong Z, Yan C, Ning L, Aiyun X. 2009. Clinical analysis of 41 cases of acute pancreatitis during pregnancy. Progress in Modern Obstetrics and Gynecology 18:216–218.
- Ruying W. 2006. Clinical analysis of 19 cases of acute pancreatitis in late pregnancy. Anhui Medicine 10:360–361.
- Saharia P, Margolis S, Zuidema GD, Cameron JL. 1977. Acute pancreatitis with hyperlipemia: studies with an isolated perfused canine pancreas. Surgery 82:60–67.
- Shaobing H. 2013. Nursing experience of patients with acute pancreatitis during pregnancy. China Health and Nutrition 283–284.
- Shi C, Qingjun Z, Jindong L, Rong L, Xuejun G, Huihuan T, Zhiming W. 2010. Clinical diagnosis and treatment of pancreatitis in pregnancy. Chinese Journal of General Surgery 19:805–808.
- Shiyu L, Yan Z, Xianlan Z. 2019. Clinical analysis of acute pancreatitis in pregnancy. Henan Journal of Surgery 25:54–56.
- Shuanghong H, Yajuan H, Xin T, Hui T. 2016. Traditional Chinese and Western Nursing Care of Pregnant Women Complicated with Acute Pancreatitis. West China Medicine 31:560–563.
- Shuhong G, Peng S. 2008. Analysis of clinical data of 29 cases of pregnancy complicated with acute pancreatitis. Modern Health Care and Medical Innovation Research 5:99–100.
- Shujuan F, Junxi X, Mi X, Fanghui W, Xiaojie L, Xihui Z, et al. 2018. The influence of pregnancy complicated with acute pancreatitis on pregnancy outcome and newborn. Chinese Journal of Contemporary Pediatrics 20:274–278.
- Sumei W, Zhenyu Z. 2008. Report of 14 cases of pregnancy complicated with acute pancreatitis. Progress in Modern Obstetrics and Gynecology 778–780.
- Sun Y, Fan C, Wang S. 2013. Clinical analysis of 16 patients with acute pancreatitis in the third trimester of pregnancy. International Journal of Clinical and Experimental Pathology 6:1696–1701.
- Sun L, Li W, Geng Y, Shen B, Li J. 2011. Acute pancreatitis in pregnancy. Acta Obstetricia et Gynecologica Scandinavica 90:671–676.
- Sun L, Li W, Sun F, Geng Y, Tong Z, Li J. 2015. Intra-abdominal pressure in third trimester pregnancy complicated by acute pancreatitis: an observational study. BMC Pregnancy and Childbirth 15.
- Suxu Y, Jing W. 2003. Clinical analysis of 17 cases of pregnancy complicated with acute pancreatitis. Journal of Practical Medicine 54–55.
- Suxu Y, Yanlang C. 2000. Clinical analysis of acute pancreatitis during pregnancy. Chinese Journal of Digestion 50–52.
- Suyu C, Yujie L. 2018. Analysis of 16 cases of pregnancy complicated with acute pancreatitis. Journal of Chongqing Medical University 43:931–934.
- Swisher SG, Hunt KK, Schmit PJ, Hiyama DT, Bennion RS, Thompson JE. 1994. Management of pancreatitis complicating pregnancy. The American Surgeon 60:759–762.
- Takaishi K, Miyoshi J, Matsumura T, Honda R, Ohba T, Katabuchi H. 2009. Hypertriglyceridemic acute pancreatitis during pregnancy: prevention with diet therapy and ω-3 fatty acids in the following pregnancy. Nutrition 25:1094–1097.
- Tang S-J, Rodriguez-Frias E, Singh S, Mayo MJ, Jazrawi SF, Sreenarasimhaiah J, et al. 2010. Acute pancreatitis during pregnancy. Clinical Gastroenterology and Hepatology 8:85–90.
- Tang M, Xu J-M, Song S-S, Mei Q, Zhang L-J. 2018. What may cause fetus loss from acute pancreatitis in pregnancy. Medicine 97:e9755.
- Tazuma S. 2006. Gallstone disease: epidemiology, pathogenesis, and classification of biliary stones (common bile duct and intrahepatic). Best Practice & Research. Clinical Gastroenterology 20:1075–1083.
- Tian L, Suhua C, Haodong C, Ning L. 2013. Analysis of diagnosis and treatment of 23 cases of pregnancy complicated with acute pancreatitis. Chinese Obstetric Emergency Electronic Journal 2:132–135.
- Vilallonga R, Calero-Lillo A, Charco R, Balsells J. 2014. Acute pancreatitis during pregnancy, 7-year experience of a tertiary referral center. Cirugia Espanola 92:468–471.
- Weinan W, Zhen H. 2018. Clinical analysis of acute pancreatitis in pregnancy. Journal of Wannan Medical College 37:557–559.
- Wenxiang W. 2012. Early diagnosis and treatment of pancreatitis in pregnancy. Chinese and Foreign Medical 31:93.
- Wenying X. 2011. Significance of diagnosis and treatment of 15 cases of pregnancy complicated with acute pancreatitis. Modern Chinese Doctor 49:153–154.
- Xia C, Hongxian Z, Zhongqiong W, Changping L. 2015. Analysis of clinical characteristics of 32 cases of acute pancreatitis during pregnancy. Journal of Luzhou Medical College 38:485–487.
- Xiaomin F, Yanqing G. 2009. Clinical analysis of 15 cases of pregnancy complicated with acute pancreatitis. China Maternal and Child Health 24:2166–2167.
- Xiaoshan L, Bin S. 2015. Analysis of the etiology, clinical features, treatment and prognosis of acute pancreatitis during pregnancy. Electronic Journal of Clinical Medicine Literature 5656:5653–5653.
- Xiaowei W, Xiang Y, Pinjie Z, Yun S. 2018. Analysis of clinical and prognostic factors influencing acute pancreatitis during pregnancy. Journal of Hepatobiliary Surgery 26:335–340.
- Xiaoxiao X, Xiangfei M, Zhiying G. 2013. Diagnosis and treatment of 12 cases of acute pancreatitis during pregnancy in a single center. Chinese Journal of Healthcare and Medicine 15:149–151.
- Xiaoyan W, Meng Z, Yingxia L, Hongtao W. 2017. Analysis of clinical characteristics of acute pancreatitis in pregnancy. Henan Medical Research 26:3679–3680.
- Xiaoyan Z, Yuhuan Q, Ruixia G. 2011. Experience in diagnosis and treatment of 16 cases of pregnancy complicated with acute pancreatitis. Journal of Practical Medicine 27:2480–2481.
- Xiaozheng L, Xiangdong Z. 2010. Analysis of 18 cases of pregnancy complicated with acute pancreatitis. China Practical Medicine 5:179–180.
- Xin Z, Zhihua W. 2014. The influence of pregnancy with acute pancreatitis on perinatal outcome. Modern Practical Medicine 26:1425–1426.
- Xingrui L, Wen C, Jilin Y. 2006. Diagnosis and treatment of acute pancreatitis in pregnancy. China Maternal and Child Health 1185–1186.
- Xinzhi Y, Dongmei LT. 2006. Diagnosis and treatment of acute pancreatitis in pregnancy. Journal of Practical Diagnosis and Treatment 227–228.
- Xiufeng D, Bin L, Ying W. 2005. Analysis of 15 cases of pregnancy complicated with acute pancreatitis. Chinese Journal of Practical Gynecology and Obstetrics 445.
- Xiuhai H, Yushan Q. 1993. Analysis of 45 cases of acute pancreatitis in middle and late pregnancy. Hunan Medicine 233.
- Xu K. 2012. Retrospective analysis of 19 cases of pregnancy complicated with acute pancreatitis. Medical Theory and Practice 25:2280–2281.
- Xue Longyan B. 2019. Analysis of 15 cases of pregnancy complicated with acute pancreatitis. Chinese Journal of Reproductive Health 30:444–448.
- Xuefeng L, Baoquan L. 2017. Clinical analysis of 15 cases of pregnancy complicated with acute pancreatitis. Medical Theory and Practice 30:1425–1427.
- Xuehong C. 2007. Observation, analysis and preventive measures of acute pancreatitis during pregnancy. China Practical Medicine 67–68.
- Xueqin W, Yufang L. 2009. Analysis of diagnosis and treatment of 18 cases of pregnancy complicated with acute pancreatitis. Chinese Journal of Practical Diagnosis and Therapy 23:234–236.
- Xu Q, Wang S, Zhang Z. 2015. A 23-year, single-center, retrospective analysis of 36 cases of acute pancreatitis in pregnancy. International Journal of Gynecology & Obstetrics 130:123–126.
- Yan L, Yuanyuan C, Jianchun Z. 2015. Clinical analysis of acute pancreatitis in pregnancy. Clinical Medicine Practice 24:589–592.
- Yanfeng G, Jianwei T. 2007. Analysis of diagnosis and treatment of 12 cases of acute pancreatitis during pregnancy. Community Medicine Journal 34–35.
- Yang Z, Guo G, Li H. 2020. Predicting fetal loss in severe acute pancreatitis during pregnancy: a 5-year single-tertiary-center retrospective analysis. Postgraduate Medicine 132:473–478.
- Yanlan W, Bin H, Danfang Y. 2012. Clinical analysis of 10 cases of pregnancy complicated with acute pancreatitis. Journal of Qiqihar Medical College 33:1872–1873.
- Yanwei G, Yanju Z. 2014. Retrospective analysis of 14 cases of acute pancreatitis during pregnancy. International Journal of Obstetrics and Gynecology 41:272–273.
- Yi X, Senlin L, Peihua L, Tao X. 2009. Analysis of 15 cases of pregnancy complicated with acute pancreatitis. China Practical Medicine 4:179.
- Yifeng Y. 2013. Analysis of clinical diagnosis and treatment of 34 cases of pregnancy complicated with acute pancreatitis. China Health & Nutrition 23:3688–3689.
- Yinfeng L, Wuhua T, Kangyuan Z. 2017. Clinical analysis of 62 cases of pregnancy complicated with acute pancreatitis. Frontiers of Medicine 7:199–200.
- Yinghao, Z, Zonggang, J, Chunying, Z, Thunder Yi R. 2009. 36 cases of acute pancreatitis with pregnancy. 2009 Zhejiang Surgery Annual Conference Paper Collection. p. 1.
- Yongliang X, Yajun P, Li X. 2015. Clinical analysis of 23 cases of pregnancy complicated with acute pancreatitis. Zhejiang Clinical Medicine 1572–1573.
- Yongmei X, Dali C, Baoquan L. 2014. Clinical analysis of 14 cases of pregnancy complicated with acute pancreatitis. Shandong Medicine 54:44–46.
- Yongyue Y, Yan Z. 2014. Clinical analysis of acute pancreatitis during pregnancy. Modern Health B 118–118.
- Yu G, Wei W, Yan L, Ruilian Z. 2014. Analysis of 13 cases of pregnancy complicated with acute pancreatitis. Jilin Medicine 35:3281–3282.
- Yue G, Baolian L, Xiaohong Z. 2009. Observation and nursing care of pregnant patients with severe acute pancreatitis. Chinese Journal of Practical Nursing 25:57–58.
- Yueqin S, Guoying C. 2013. Clinical nursing of 15 cases of pregnancy complicated with acute pancreatitis. Chinese Primary Medicine 20:1590–1591.
- Yun Z. 2018. Analysis of 24 cases of pregnancy complicated with acute pancreatitis. Frontiers of Medicine 8:98.
- Yun Z, Jinwen S, Yuqin F. 2013. Nursing care of acute pancreatitis during pregnancy. Zhejiang Practical Medicine 18:225–226.
- Yunli L, Qin Z. 2012. Diagnosis and treatment of 26 pregnant women with acute pancreatitis. Journal of Medical Postgraduates 25:496–498.
- Zhang 2016. Analysis of risk factors and clinical diagnosis and treatment of acute pancreatitis in pregnancy. Air Force Medical Journal 32:189–191 + 195.
- Zhang GP. 2012. Analysis of diagnosis and treatment of 16 cases of pregnancy complicated with acute pancreatitis. Chinese Community Physician 14:139–140.
- Zhang D-L, Huang Y, Yan L, Phu A, Ran X, Li S-S. 2013. Thirty-eight cases of acute pancreatitis in pregnancy: a 6-year single center retrospective analysis. Journal of Huazhong University of Science and Technology. Medical Sciences = Hua Zhong ke ji da Xue Xue Bao. Yi Xue Ying De Wen Ban = Huazhong Keji Daxue Xuebao. Yixue Yingdewen Ban 33:361–367.
- Zhang C, Ma Q, Yang J, Hong N, Fen A. 2012. Clinical features, diagnosis and treatment of acute pancreatitis in pregnancy. China Practical Medical Journal 59–60.
- Zhaoxia L, Yi G, Xiaoping L. 2006. Clinical analysis of hyperlipidemia pancreatitis in pregnancy. Journal of Jiangxi Medical College 164–165.
- Zheng T, Axing Q, Guihua G. 2004. Diagnosis and treatment of acute pancreatitis in pregnancy. Shandong Medicine 30–31.
- Zhengli D, Zonghai L, Fan Y. 2016. Clinical analysis of 10 cases of pregnancy complicated with acute pancreatitis. Anhui Medicine 37:562–565.
- Zhigang Z, Xin W. 2007. Analysis of 17 cases of pregnancy complicated with acute pancreatitis. Chinese Journal of Misdiagnosis 5911–5912.
- Zhijin L, Chunchi H, Yinli T. 2002. Analysis of 13 cases of pregnancy complicated with acute pancreatitis. Guangdong Medicine 1180–1181.
- Zhilian W, Min H, Yuqi Z, Jingfang R, Yonghong W. 2011. Clinical analysis of 12 cases of pregnancy complicated with acute pancreatitis. Chinese Medicine and Clinic 11:1323–1325.
- Zhiying W, Sea Y, Zhiming Q. 2014. Analysis of the treatment and nursing of 32 cases of pregnancy complicated with acute pancreatitis. Henan Journal of Surgery 20:41–42.
- Zhiyong G, Dan Z, Bingqiang Z, Qing G. 2020. Analysis of clinical features and prognosis of 46 cases of acute pancreatitis in the middle and late stages of pregnancy. Chongqing Medicine 49:973–976.
- Zhiyuan S, Xianfeng Zhou Ping Zhou Meng S, Min Z, Mingyin L. 2012. Analysis of diagnosis and treatment of 18 cases of acute pancreatitis in late pregnancy. Advances in Modern General Surgery in China 15:576–577. +585.
- Zhong J, Lunan Y, Guang G, Fugui L, Yujian Z. 2008. Analysis of clinical diagnosis and treatment of acute pancreatitis in pregnancy. Chinese Journal of Hepatobiliary Surgery 759–762.
- Zhongchao W. 2008. Clinical study on acute pancreatitis during pregnancy. Tibet Medical Journal 10–13.
- Zhu L. 2009. Clinical analysis and nursing of 32 cases of pregnancy complicated with acute pancreatitis. Nursing Practice and Research 6:73–74.
- Ziyang DL, Haipeng Haoqi WC, Kang XC. 2020. Analysis of clinical features of acute pancreatitis in pregnancy. Zhejiang Medicine 42:1653–1654 + 1658.
- Zongwen H, Guangyuan C, Junming J, Qing X, Gang W. 1997. Analysis of 19 cases of pregnancy complicated with acute pancreatitis. West China Medicine 35–36.