

Abstract
Total testosterone (TT), sex hormone-binding globulin (SHBG), dehydroepiandrosterone (DHEA) levels, and cervical length (CL) were investigated in pregnant Egyptian women with polycystic ovary syndrome (PCOS, n = 38), history of miscarriages (RM, n = 40) and without the conditions (HC, n = 40). At week 8, the RM had lower levels of TT (p = 0.000) and free androgen index (FAI) (p = 0.000) and higher SHBG (p = 0.000) and DHEA (p < 0.05) than the PCOS. Compared with the HC, they had elevated SHBG (p < 0.05) and DHEA (p = 0.001) and reduced CL (p = 0.000). TT (p = 0.001) and FAI (p = 0.000) were higher and SHBG (p = 0.000) and CL (p = 0.001) lower in the PCOS than in the HC group. At week 16, TT (p = 0.000) and FAI (p = 0.000) were higher, and SHBG (p = 0.000) and CL (p < 0.05) lower in PCOS than in RM and HC. The PCOS had elevated FAI than the RM (p = 0.000) and HC (p = 0.001) at week 20. The DHEA, SHBG and CL abnormalities in PCOS and RM may compromise pregnancy outcomes.
What is already known on this subject? Hyperandrogenaemia, low sex hormone-binding globulin (SHBG), shortened cervical length (CL) and polycystic ovary syndrome (PCOS) are the most cited risk factors for recurrent miscarriages (RM). However, the published data are inconsistent, perhaps because of the confounding effects of ethnicity and nutritional milieu.
What do the results of this study add? The study’s findings comprising ethnically and socially homogenous women demonstrate that PCOS and RM are characterised by elevated dehydroepiandrosterone (DHEA) and shortened CL, and PCOS by reduced SHBG. These abnormalities would be expected to have an adverse impact on pregnancy outcomes.
What are the implications of these findings for clinical practice and/or further research? Twenty-weeks DHEA and CL values have the potential to predict outcome risk in women with a history of RM and PCOS. Further research on other population groups is required to validate the current study’s findings.
IMPACT STATEMENT
Introduction
Recurrent miscarriage (RM), also known as recurrent pregnancy loss, is commonly defined as the loss of ≥2 (ESHRE – The European Society of Human Reproduction and Embryology Citation2017, Van Dijk et al. Citation2020, ASRM – The American Society for Reproductive Medicine Citation2020) or ≥ 3 ( RCOG – The Royal College of Obstetricians and Gynaecologists Citation2011, HSE – Health Service Executive, Ireland Citation2016, Huchon et al. Citation2016) consecutive pregnancies before 20 weeks of gestation. RM affects 1–2% (Hennessy et al. Citation2021), 2–4% (Stephenson and Kutteh Citation2007) and 7.46% (Patki and Chauhan Citation2016) of reproductive-age women. These prevalence variations could reflect the RM definition used, the ethnicity of the populations investigated (Patki and Chauhan Citation2016) and lifestyle factors (Ng et al. Citation2021). Besides, there is some evidence that the incidence of RM has increased over the last decades (Rossen et al. Citation2018). This increase may be due to the obesity epidemic since there is an association between body mass index and RM (Eapen et al. Citation2021, Ng et al. Citation2021)
The established risk factors of RM include chromosomal and genetic (Turki et al. Citation2016), uterine anatomical (Venetis et al. Citation2014, Gabbai et al. Citation2018), endocrine (Kaur and Gupta Citation2016, El Hachem et al. Citation2017) and immune system (Li et al. Citation2021, Vomstein et al. Citation2021) abnormalities, blood clotting disorders (Di Prima et al. Citation2011, Nassour-Mokhtari et al. Citation2020), infection (Nigro et al. Citation2011), obesity (Eapen et al. Citation2021, Ng et al. Citation2021), maternal age (Magnus et al. Citation2019) and lifestyle factors – smoking and alcohol consumption (Sharma et al. Citation2013, Ng et al. Citation2021). However, the cause of about 50% of RM (Diejomaoh Citation2015, Vomstein et al. Citation2021) remains unknown.
Although the reported incidence rates are variable (Cocksedge et al. Citation2009, Ashaq et al. Citation2017), polycystic ovary syndrome (PCOS) is thought to be associated with RM (Cocksedge et al. Citation2008, Mayrhofer et al. Citation2020). Hyperandrogenism and hyperinsulinemia (Tian et al. Citation2007, Maryam et al. Citation2012) and hyperhomocysteinemia (Chakraborty et al. Citation2013) have been implicated in PCOS-related pregnancy loss.
The pathological mechanism of the established risk factors of RM in women with and without PCOS is yet to be fully elucidated. However, there is evidence that a reduction of sex-hormone-binding globulin (SHBG) level and a concomitant hyperandrogenaemia (elevation of testosterone) (Dendana et al. Citation2018) shortens the endocervix (Papastefanou et al. Citation2016) and subsequently causes miscarriage. Perhaps paradoxically, dehydroepiandrosterone (DHEA), a precursor of steroid hormones including testosterone, supplementation has been shown to reduce miscarriage rates in women with diminished ovarian reserves (Gleicher and Barad Citation2011).
There is a scarcity of rigorous investigations that compared androgens and endocervix length in women with RM and PCOS.
Aim
This study investigated the changing pattern of testosterone, sex hormone-binding globulin, dehydroepiandrosterone levels, and cervical length during pregnancy in women with polycystic ovary syndrome, a history of RM, and women without the conditions.
Subjects, diagnosis and methods
Subject and diagnosis
Women aged 23 to 40 years, with PCOS (n = 38), history of RM (n = 40) and healthy control group (n = 40) were recruited during their first antenatal visit to Al-Agoza Hospital, Cairo, Egypt. The exclusion criteria were – age above 40, genetic (Sickle cell disease (SCD) and thalassaemia, etc.) or non-genetic chronic (diabetes, high blood pressure) diseases, thyroid issues, physical disability restricting access to food or eating, malnutrition and inability to provide informed consent for participation in the study. Detailed demographic, obstetric and medical history data were meticulously documented. Five ml of blood samples were collected at weeks 8, 16, and 20 of pregnancy. The study was approved by the Ethics Committee of Al-Agoza Hospital, Cairo, Egypt, and informed and signed consent was obtained from all participants. This study was conducted in line with the human experimentation guidelines of the Helsinki declaration (second revision, 1983).
Diagnosis and measurement
Pregnancy was diagnosed based on an immunometric analysis of serum beta-human chorionic gonadotropin and an ultrasound dating scan.
Hormonal evaluation (follicle-stimulating hormone, luteinising hormone, oestradiol, etc.), ultrasonography (enlarged ovaries with thickened sclerotic capsules and an abnormal number of follicles) and clinical presentation (menstrual dysfunction, anovulation, hirsutism, acne, androgenic alopecia, etc.) were used to diagnose polycystic ovary syndrome (Rotterdam Criteria – The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group) Citation2004).
Based on the Royal College of Obstetricians and Gynaecologists guidelines (RCOG Citation2011), women with a history of loss of three or more consecutive pregnancies before 24 weeks from the last menstrual period were diagnosed with RM.
Cervical length, the distance between the external and internal os along the endocervical canal (Berghella et al. Citation1997), was measured at eight, sixteen and twenty gestation weeks using a transvaginal ultrasound (Voluson™ E8 ultrasound system, USA).
Methods
Weight was measured with a Seca Electronic Scale 890 (UNISCALE, Seca, Birmingham, UK), and height was assessed using a height–length measuring board (Schorr, Weight and Measure, LLC, Olney, Maryland, USA).
Serum testosterone, dehydroepiandrosterone and sex hormone and binding globulin, and urine beta-human chorionic gonadotropin were measured by immunometric methods using an advanced automated immunoassay analyser (ADVIA Centaur® XPT Immunoassay System, Siemens Healthineers, Healthcare GmbH, Germany).
Data analyses
The data are expressed as mean ± standard deviation (±sd), and the level of statistical significance is set at p < 0.05. The demographic and obstetrics data were tested for normality and homogeneity of variance and analysed with a one-way analysis of variance (ANOVA). The post hoc test Fisher’s Least Significant Difference (LSD) was conducted when ANOVA indicates significance. Statistical analyses were performed using IBM SPSS, version 25 (International Business Machines Corporation, New York, USA).
Results
Demographic data of the women with a history of RM, PCOS and healthy control group (HC) are presented in . There was no difference in ages or body mass index between the three groups (p > 0.05). The PCOS women were lighter and shorter than the RM (p < 0.05). Similarly, the women with RM were shorter than their healthy counterparts (p < 0.001).
Table 1. Anthropometric data (mean ± sd) of women with a history of recurrent miscarriages (RM, n = 40), polycystic ovary syndrome (PCOS, n = 38) and healthy control group (HC, n = 40) at week eight of pregnancy.
Levels of total testosterone (TT), sex hormone-binding globulin (SHBG), dehydroepiandrosterone (DHEA), free androgen index (FAI) and cervical length (CL) of the HC women and women with RM and PCOS at week eight, sixteen and twenty are shown in .
Table 2. Mean (±sd) cervical length (CL, mm) and total testosterone (TT, mmol/L), sex hormone-binding globulin (SHBG, mmol/L) dehydroepiandrosterone (DHEA, mmol/L), free androgen index (FAI) levels of women with a history of recurrent miscarriages (RM, n = 40), polycystic ovary syndrome (PCOS, n = 38) and healthy controls (HC, n = 40) at three stages of pregnancy.
At week eight of pregnancy, the women with RM had lower levels of TT (p = 0.000) and FAI (p = 0.000) and higher SHBG (p = 0.000) and DHEA (p < 0.05) than those with PCOS. Besides, compared with their HC counterparts, they had elevated concentrations of SHBG (p < 0.05) and DHEA (p = 0.001) and reduced CL (p = 0.000). The values of TT (p = 0.001) and FAI (p = 0.000) were higher and SHBG (p = 0.000) and CL (p = 0.001) lower in the PCOS than in the HC group.
At week sixteen of pregnancy, the concentrations of TT (p = 0.000) and FAI (p = 0.000) were higher, and SHBG level (p = 0.000) and CL length (p < 0.05) lower in the PCOS than in the RM and HC women. DHEA (p = 0.000) and SHBG (p = 0.001) concentrations were elevated CL length (p = 0.000) reduced in the women with RM compared with the HC.
At week twenty of pregnancy, the HC women had higher TT (p = 0.000) and CL (p = 0.000) and lowered DHEA (p = 0.000) than the other two groups. The PCOS group had an elevated level of FAI compared with those of the RM (p = 0.000) and HC (p = 0.001) women.
depicts changes in levels of testosterone (TT), sex hormone-binding globulin (SHBG), dehydroepiandrosterone (DHEA), free androgen index (FAI) and cervical length (CL) of the three groups of women between pregnancy week eight and twenty.
Table 3. Mean (±sd) changes of cervical length (CL, mm) and total testosterone (TT, mmol/L), sex hormone-binding globulin (SHBG, mmol/L) dehydroepiandrosterone (DHEA, mmol/L), free androgen index (FAI) levels of women with a history of recurrent miscarriages (RM, n = 40), polycystic ovary syndrome (PCOS, n = 38) and healthy controls (HC, n = 40) with the progress of pregnancy.
The week eight TT, SHBG and DHEA levels of the PCOS group, respectively, were lower than that of weeks sixteen (p = 0.000, p = 0.000 & p = 0.000) and twenty (p = 0.000, p = 0.000 & p = 0.000). In contrast, the group had higher FAI and CL values in weeks sixteen (p = 0.000, p = 0.000) and twenty (p = 0.000 & p = 0.000) than in week eight.
The women with RM had reduced concentrations of TT, SHBG, DHEA and FAI in weeks sixteen (p = 0.000, p = 0.000 & p = 0.000, p > 0.05) and twenty (p = 0.000, p = 0.000, p = 0.000 & p = 0.001) than in week eight of pregnancy. Conversely, compared to week eight, they had higher CL levels in week sixteen (p < 0.05) and twenty (p = 0.000).
Compared with week eight of pregnancy, the TT, SHBG and DHEA values of the HC women were higher in week sixteen (p = 0.000, p = 0.000 & p = 0.000) and twenty (p = 0.000, p = 0.000 & p = 0.000). Besides, compared with week twenty, the HC group had a lower FAI concentration (p = 0.000) and higher CL length (p = 0.001) in week eight.
Twenty-eight (74%) of PCOS, thirty-four (85%) of RM, and none of the control groups miscarried. Nine (26%, mean gestation week 27.7 ± 2.3) of PCOS, five (15%, mean gestation week, 28.2 ± 2.1) of RM and four (10%, mean gestation week 34.3 ± 2.9) of the control women delivered before date (gestation week 37). One of the PCOS (gestation week 38), one of the RM (gestation week 37) and 36 of the control (gestation week 39.4 ± 2.9) women gave birth at term.
Discussion
Previous communications have reported that obesity is a common phenomenon in women with polycystic ovary syndrome (PCOS) both before (Vanky and Lovvik Citation2020, Liu et al. Citation2021) and during (Kakoly et al. Citation2017) pregnancy. However, in the current study, inconsistent with the reports mentioned above, the women with PCOS compared with the other two groups (RM and HC) had a lower mean body weight. This reflected the intensive dietary and lifestyle counselling given to women with PCOS Al-Agoza Hospital to help enhance their ability to conceive and prevent maternal and foetal morbidity ().
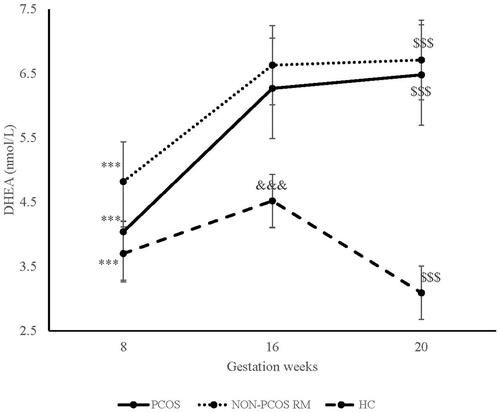
Figure 1. Changes in mean (±se) dehydroepiandrostrone (DHEA) concentration of women with recurrent miscarriages, polycystic ovary syndrome, and healthy control group between pergnancy week 8 and 20.
Notations – ap = 0.000(8 vs. 16 week); bp = 0.000 (8 vs. 20 week);cp = 0.000 (16 vs. 20 week).
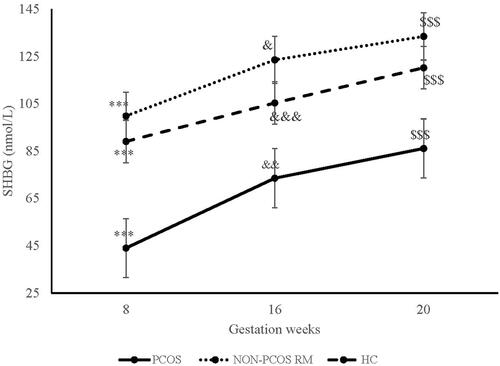
Hyperandrogenism (Ashraf et al. 2019, Valdimarsdottir et al. Citation2021) and lower blood SHBG concentrations (Deswal et al. Citation2018, Qu and Donnelly Citation2020) have been reported in women with PCOS. Consistent with these findings, the PCOS group in our study had higher TT (Supplementary Figure 1) and FAI (Supplementary Figure 2) and lowered SHBG () levels on weeks eight, sixteen and twenty. There is evidence that higher levels of TT and FAI in women with the disorder indicate enhanced production of ovarian androgen (Ashraf et al. Citation2019) and impaired synthesis and secretion of SHBG, which is the primary testosterone binder (Dunn et al. Citation1981), respectively. The reason for the reduced level of SHBG in women with PCOS is yet to be fully elucidated. However, obesity and body fat distribution (Zain and Norman Citation2008, Qu and Donnelly Citation2020), low levels of HDL-cholesterol (Chen et al. Citation2006), hyperinsulinemia (Lin et al. Citation2015, Tawfeek et al. Citation2017) and hepatic lipogenesis (Qu and Donnelly Citation2020) have been implicated.
Figure 2. Changes in mean (±se) sex hormone binding globulin (SHBG) concentration of women with recurrent miscarriages, polycystic ovary syndrome, and healthy control group between pergnancy week 8 and 20.
Notations – ap = 0.000(8 vs. 16 week); bp = 0.000 (8 vs. 20 week); cp < 0.05, dp < 0.001, ep < 0.000, (16 vs. 20 week).
It is postulated that a reduction in SHBG expression resulting from SHBG gene polymorphism increases the risk of RM by inducing hyperandrogenaemia (Dendana et al. Citation2018). Similarly, Hogeveen et al. (Citation2002) have suggested that a low plasma SHBG concentration resulting from variations of the SHBG gene is associated with recurrent pregnancy loss. Indeed, it has been reported that a low SHBG level and PCOS-related complications in women with the condition could be ameliorated with SHBG treatment (Deswal et al. Citation2018).
In this study, the Egyptian women with a history of RM did not have elevated TT and FAI or lower SHBG levels, unlike their counterparts with PCOS. In contrast, other investigators have reported hyperandrogenaemia (Cocksedge et al. Citation2008) and reduced SHBG (Spencer et al. Citation2005) in miscarrying women in Europe. The reason behind these contradictory findings is not evident. There is evidence that blood levels of sex hormones and sex hormone-binding globulin are influenced by dietary habits (Moran et al. Citation2016, Huang et al. Citation2018). Therefore, differences in dietary habits between the population studied (Egyptians and Europeans) might have contributed to the conflicting observations.
The levels of DHEA in the women with PCOS and RM compared with that of the control group were higher by 9 and 30% on week eight, 38 and 47% on week sixteen and 83 and 117% on week twenty (). Similarly, a meta-analysis of case-control studies undertaken by Benjamin et al. (Citation2021) revealed women with PCOS have elevated concentrations of DHEA. Excess adrenal precursor androgen production (DHEAS, DHEA) was also reported in women with PCOS (Goodarzi et al. Citation2015, Moran et al. Citation2015). Besides, reproductive abnormalities similar to that observed in women with PCOS was exhibited in rats treated with DHEA (Seow et al. Citation2018). Regardless, the aetiology of excess DHEA production and its obstetric and clinical implications are unclear and require further investigations.
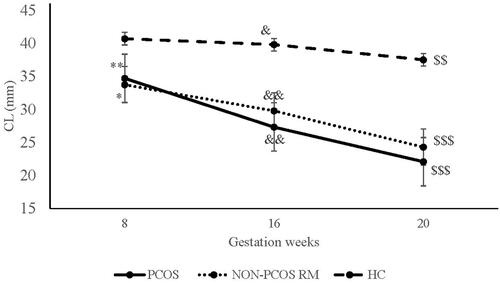
The cervix lengths (CL) of the PCOS and RM groups, respectively, were shorter than their healthy counterparts by 9 and 30% at eight, 38 and 47% at sixteen and 83 and 117% at twenty weeks of pregnancy (). At twenty weeks, the CL of the PCOS was 22.1 mm and the RM 24.3 mm. A short CL, conventionally defined as shorter than 25 mm, measured during the second trimester, predicts the risk of spontaneous delivery before the due date (Berghella et al. 1997, O’Hara et al. Citation2015). However, Bortoletto et al. (Citation2021) have questioned using a single cut-off point to diagnose cervical competence. They contend that it is necessary to identify different CL curves and cut-off values that reflect cervical length variations of varying population groups. Regardless, CL is an effective predictor of spontaneous preterm birth for singleton (Hernandez-Andrade et al. Citation2012, Wulff et al. Citation2018) and twin (Souka et al. Citation2011) pregnancies.
Figure 3. Changes in mean (±se) cervical length of women with recurrent miscarriages, polycystic ovary syndrome, and healthy control group between pergnancy week 8 and 20.
Notations – ap < 0.05, bp < 0.001 (8 vs. 16 week); cp = 0.001, cp = 0.000 (8 vs. 20 week); d p < 0.05 ep = 0.001 (16 vs. 20 week).
The conventionally accepted cut-off point of cervical competence suggests that the women with PCOS and RM who had a mean CL of 22.1 and 24.3 mm, respectively, were at higher risk of delivery before date or miscarrying. The question is, why was the CL of the two groups significantly shorter compared to that of the healthy control women. It is hypothesised that hyperandrogenism plays a role in the shortening (Lovvik et al. Citation2015) and remodelling and ripening of the cervix (Naver et al. Citation2014). The HC women had a higher total testosterone concentration than the other two groups at week twenty. Similarly, their FAI was higher than the RM group (2.59 vs 1.76). Hence, TT or FAI on its own would not have influenced the shortening or ripening of the cervix. However, the DHEA levels of the PCOS and RM groups which were almost 1.4 (week sixteen) and 2.0 (week twenty) times higher than that of the HC women, on its own or in concert with TT, may have been the driving factor behind cervical shortening. The elevated DHEA levels in the PCOS and RM groups without the concomitant increase in testosterone on weeks sixteen and twenty suggests its conversion to testosterone may be impaired.
The study’s findings comprising ethnically and socially homogenous women demonstrate that PCOS and RM are characterised by elevated DHEA and shortened cervical length and PCOS by reduced SHBG. These abnormalities would be expected to have an adverse effect on pregnancy outcomes. Also, the findings suggest that the twenty-week DHEA and cervical length values can potentially predict outcome risk in this population.
The outcome of pregnancy, blood lipid parameters, biomarkers of insulin resistance, dehydroepiandrosterone sulphate were not assessed because of financial and logistic constraints. These limitations will be addressed in the study that will be undertaken shortly.
Author contributions
EEM and NF conceptualised and conducted the study, and collected the laboratory data, KG, MA and EEM analysed the data, and KG and EEM wrote the manuscript.
Supplemental Material
Download Zip (165.3 KB)Acknowledgement
Very sincere thanks are due to the women who graciously consented to participate in the study, and the obstetrics and gynaecology team and the pathology laboratory technicians at Al-Agoza Hospital for their contributions to the data collection and collection and processing of blood specimens, respectively.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Ashaq, L., Al Mazer, Y. and Al Qahtani, N., 2017. Recurrent pregnancy loss in patients with polycystic ovary syndrome: a case control study. Open Journal of Obstetrics and Gynecology, 07 (11), 1073–1085. http://www.scirp.org/journal/ojog
- Ashraf, S., et al., 2019. Hyperandrogenism in polycystic ovarian syndrome and role of CYP gene variants: a review. Egyptian Journal of Medical Human Genetics, 20 (1), 25.
- ASRM – The American Society for Reproductive Medicine. 2020. Definitions of infertility and recurrent pregnancy loss: a committee opinion practice committee of the American Society for reproductive medicine. Fertility and Sterility, 113 (3), 533–534.
- Benjamin, J. J., et al., 2021. DHEA and polycystic ovarian syndrome: meta-analysis of case-control studies. PLoS One, 16 (12), e0261552.
- Berghella, V., et al., 1997. Cervical ultrasonography compared with manual examination as a predictor of 7; preterm delivery. American Journal of Obstetrics and Gynecology, 177 (4), 723–730.
- Bortoletto, T.G., et al., 2021. Cervical length varies considering different populations and gestational outcomes: results from a systematic review and meta-analysis. PLoS One, 16 (2), e0245746.
- Chakraborty, P., et al., 2013. Recurrent pregnancy loss in polycystic ovary syndrome: role of hyperhomocysteinemia and insulin resistance. PLoS One, 8 (5), e64446.
- Chen, M.J., et al., 2006. Low sex hormone-binding globulin is associated with low high-density lipoprotein cholesterol and metabolic syndrome in women with PCOS. Human Reproduction, 21 (9), 2266–2271.
- Cocksedge, K.A., et al., 2009. How common is polycystic ovary syndrome in recurrent miscarriage. Reproductive Biomedicine Online, 19 (4), 572–576.
- Cocksedge, K.A., et al., 2008. Does free androgen index predict subsequent pregnancy outcome in women with recurrent miscarriage? Human Reproduction, 23 (4), 797–802.
- Dendana, M., et al., 2018. Common genetic variants in the sex hormone-binding globulin (SHBG) gene in idiopathic recurrent pregnancy loss: a case-control study. Translational Medicine Communications, 3 (1), 5.
- Deswal, R., Yadav, A. and Dang, A.S., 2018. Sex hormone binding globulin – an important biomarker for predicting PCOS risk: a systematic review and meta-analysis. Systems Biology in Reproductive Medicine, 64 (1), 12–24.
- Di Prima, F.A.F., et al., 2011. Antiphospholipid Syndrome during pregnancy: the state of the art. Journal of Prenatal Medicine, 5 (2), 41–53.
- Diejomaoh, M.F.E., 2015. Recurrent spontaneous miscarriage, is still a challenging diagnostic and therapeutic quagmire. Medical Principles and Practice, 24 (suppl 1), 38–55.
- Dunn, J.F., Nisula, B.C. and Rodbard, D., 1981. Transport of steroid hormones: binding of 21 endogenous steroids to both testosterone-binding globulin and corticosteroid-binding globulin in human plasma. The Journal of Clinical Endocrinology and Metabolism, 53 (1), 58–68.
- Eapen, A., et al., 2021. Mean differences in maternal body mass index and recurrent pregnancy loss: a systematic review and meta-analysis of observational studies. Fertility and Sterility, 116 (5), 1341–1348.
- El Hachem, H., et al., 2017. Recurrent pregnancy loss: current perspectives. International Journal of Women’s Health, 9, 331–345.
- ESHRE – The European Society of Human Reproduction and Embryology. 2017. Early Pregnancy Guideline Development Group. Recurrent Pregnancy Loss, version 2.
- Gabbai, D., et al., 2018. Pregnancy outcomes among patients with recurrent pregnancy loss and uterine anatomic abnormalities. Journal of Perinatal Medicine, 46 (7), 728–734.
- Gleicher, N. and Barad, D.H., 2011. Dehydroepiandrosterone (DHEA) supplementation in diminished ovarian reserve (DOR). Reproductive Biology and Endocrinology, 9, 67.
- Goodarzi, M.O., Carmina, E. and Azziz, R., 2015. DHEA, DHEAS and PCOS. The Journal of Steroid Biochemistry and Molecular Biology, 145, 213–225.
- Hennessy, M., et al., 2021. Clinical practice guidelines for recurrent miscarriage in high-income countries: a systematic review. Reproductive Biomedicine Online, 42 (6), 1146–1171.
- Hernandez-Andrade, E., et al., 2012. Ransabdominal evaluation of uterine cervical length during pregnancy fails to identify a substantial number of women with a short cervix. The Journal of Maternal-Fetal & Neonatal Medicine, 25 (9), 1682–1689.
- Hogeveen, K.N., et al., 2002. Human sex hormone-binding globulin variants associated with hyperandrogenism and ovarian dysfunction. The Journal of Clinical Investigation, 109 (7), 973–981.
- HSE – Health Service Executive, Ireland. 2016. National standards for bereavement care following pregnancy loss and perinatal death. Version 1.15
- Huang, M., et al., 2018. Relationship between dietary carbohydrates intake and circulating sex hormone-binding globulin levels in postmenopausal women. Journal of Diabetes, 10 (6), 467–477.
- Huchon, C., et al., 2016. Pregnancy loss: French clinical practice guidelines. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 201, 18–26.
- Kakoly, N.S., et al., 2017. Group-based developmental BMI trajectories, polycystic ovary syndrome, and gestational diabetes: a community-based longitudinal study. BMC Medicine, 15 (1), 195.
- Kaur, R. and Gupta, K., 2016. Endocrine dysfunction and recurrent spontaneous abortion: an overview. International Journal of Applied & Basic Medical Research, 6 (2), 79–83.
- Li, D., et al., 2021. The role of immune cells in recurrent spontaneous abortion. Reproductive Sciences, 28 (12), 3303–3315.
- Lin, X.F., et al., 2015. Exploring the significance of sex hormone-binding globulin examination in the treatment of women with polycystic ovarian syndrome (PCOS). Clinical and Experimental Obstetrics & Gynecology, 42 (3), 315–320.
- Liu, X., et al., 2021. Women with PCOS with a history of early pregnancy loss show a higher risk of gestational diabetes mellitus. International Journal of General Medicine, 14, 6409–6416.
- Lovvik, T.S., et al., 2015. Pregnancy and perinatal outcomes in women with polycystic ovary syndrome and twin births: a population-based cohort study. An International Journal of Obstetrics and Gynaecology, 122 (10), 1295–1302.
- Magnus, M.C., et al., 2019. Role of maternal age and pregnancy history in risk of miscarriage: prospective register-based study. BMJ, 364, l869.
- Maryam, K., et al., 2012. The comparison of insulin resistance frequency in patients with recurrent early pregnancy loss to normal individuals. BMC Research Notes, 5, 133.
- Mayrhofer, D., et al., 2020. The prevalence and impact of polycystic ovary syndrome in recurrent miscarriage: a retrospective cohort study and meta-analysis. Journal of Clinical Medicine, 9 (9), 2700.
- Moran, C., et al., 2015. Adrenal androgen excess and body mass index in polycystic ovary syndrome. The Journal of Clinical Endocrinology and Metabolism, 100 (3), 942–950.
- Moran, L.J., et al., 2016. Long-term effects of a randomised controlled trial comparing high protein or high carbohydrate weight loss diets on testosterone, shbg, erectile and urinary function in overweight and obese men. PLoS One, 11 (9), e0161297.
- Nassour-Mokhtari, I., et al., 2020. Inherited thrombophilia and recurrent pregnancy loss: a single-center case-control study in North-Western Algeria. Egyptian Journal of Medical Human Genetics, 21 (1), 33.
- Naver, K.V., et al., 2014. Increased risk of preterm delivery and pre-eclampsia in women with polycystic ovary syndrome and hyperandrogenaemia. An International Journal of Obstetrics and Gynaecology, 121 (5), 575–581.
- Ng, K.Y.B., et al., 2021. Systematic review and meta‑analysis of female lifestyle factors and risk of recurrent pregnancy loss. Scientific Reports, 11 (1), 7081.
- Nigro, G., et al., 2011. Role of the infections in recurrent spontaneous abortion. The Journal of Maternal-Fetal & Neonatal Medicine, 24 (8), 983–989.
- O’Hara, S., et al., 2015. The maternal cervix: Why, when and how? Sonography, 2 (4), 74–83.
- Papastefanou, I., et al., 2016. First trimester cervical length is associated with mid-trimester loss. The Journal of Maternal-Fetal & Neonatal Medicine, 29 (1), 51–54.
- Patki, A. and Chauhan, N., 2016. An epidemiology study to determine the prevalence and risk factors associated with recurrent spontaneous miscarriage in India. Journal of Obstetrics and Gynaecology of India, 66 (5), 310–315.
- Qu, X. and Donnelly, R., 2020. Sex hormone-binding globulin (SHBG) as an early biomarker and therapeutic target in polycystic ovary syndrome. International Journal of Molecular Sciences, 21 (21), 8191.
- RCOG – The Royal College of Obstetricians and Gynaecologists., 2011. The Investigation and Treatment of Couples with Recurrent First-trimester and Second-trimester Miscarriage. Guideline No. 17.
- Rossen, L.M., Ahrens, K.A. and Branum, A.M., 2018. Trends in risk of pregnancy loss among us women, 1990–2011. Paediatric and Perinatal Epidemiology, 32 (1), 19–29.
- Rotterdam Criteria – The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group), 2004. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertility and Sterility, m81 (1), 19–25.
- Seow, M., et al., 2018. The use of dehydroepiandrosterone-treated rats is not a good animal model for the study of metabolic abnormalities in polycystic ovary syndrome. Taiwanese Journal of Obstetrics & Gynecology, 57 (5), 696–704.
- Sharma, R., et al., 2013. Lifestyle factors and reproductive health: taking control of your fertility. Reproductive Biology and Endocrinology, 11, 66. http://www.rbej.com/content/11/1/66.
- Souka, A.P., et al., 2011. Cervical length changes from the first to second trimester of pregnancy, and prediction of preterm birth by first-trimester sonographic cervical measurement. Journal of Ultrasound in Medicine, 30 (7), 997–1002.
- Spencer, K., et al., 2005. First trimester sex hormone-binding globulin and subsequent development of preeclampsia or other adverse pregnancy outcomes. Hypertension in Pregnancy, 24 (3), 303–311.
- Stephenson, M. and Kutteh, W., 2007. Evaluation and management of recurrent early pregnancy loss. Clinical Obstetrics and Gynecology, 50 (1), 132–145.
- Tawfeek, M.A., et al., 2017. Sex hormone binding globulin as a valuable biochemical marker in predicting gestational diabetes mellitus. BMC Women’s Health, 17 (1), 18.
- Tian, L., et al., 2007. Insulin resistance increases the risk of spontaneous abortion after assisted reproduction technology treatment. The Journal of Clinical Endocrinology and Metabolism, 92 (4), 1430–1433.
- Turki, R.F., et al., 2016. Associations of recurrent miscarriages with chromosomal abnormalities, thrombophilia allelic polymorphisms and/or consanguinity in Saudi Arabia. BMC Medical Genetics, 17 (S1), 69.
- Valdimarsdottir, R., et al., 2021. Pregnancy outcome in women with polycystic ovary syndrome in relation to second-trimester testosterone levels. Reproductive Biomedicine Online, 42 (1), 217–225.
- Van Dijk, M.M., et al., 2020. Recurrent pregnancy loss: diagnostic workup after two or three pregnancy losses? A systematic review of the literature and meta-analysis. Human Reproduction Update, 26 (3), 356–367.
- Vanky, T.S. and Lovvik, T.S., 2020. Polycystic ovary syndrome and pregnancy – from a clinical perspective. Current Opinion in Endocrine and Metabolic Research, 12, 8–13.
- Venetis, C.A., et al., 2014. Clinical implications of congenital uterine anomalies: a meta-analysis of comparative studies. Reproductive Biomedicine Online, 29 (6), 665–683.
- Vomstein, K., et al., 2021. Immunological risk factors in recurrent pregnancy loss: guidelines versus current state of the art. Journal of Clinical Medicine, 10 (4), 869.
- Wulff, C.B., et al., 2018. Transvaginal sonographic cervical length in first and second trimesters in a low-risk population: a prospective study. Ultrasound in Obstetrics & Gynecology, 51 (5), 604–613.
- Zain, M.M. and Norman, R.J., 2008. Impact of obesity on female fertility and fertility treatment. Women’s Health, 4 (2), 183–194.