

Abstract
The aim of this review is to summarise the related characteristics of the natural history of female urinary incontinence (UI) using a narrative descriptive approach. PubMed, EMBASE and Web of Science were searched for articles published from 1 January 2010 to 1 January 2020 on the natural history of female UI, which including incidence, persistence, progression, remission, and regression of a single subtype of UI and the mutual influence of different UI subtypes. This literature review includes 15 articles published, indicates that UI is highly dynamic, with symptoms varying according to disease severity and subtype and influenced by multiple factors at different disease stages. Recent studies have increased our understanding of the natural history of UI. Future research should systematically analyse the progression of each subtype of UI and interactions between subtypes to prevent the progression of UI across females life course.
1. Introduction
The International Continence Society defines urinary incontinence (UI) as the involuntary leakage of urine (Abrams et al. Citation2002). There are three main subtypes of UI in women: stress urinary incontinence (SUI), in which there is the complaint of involuntary loss of urine on coughing or sneezing), urgency urinary incontinence (UUI), in which there is leakage of urine when there is a strong urge to urinate that cannot be controlled autonomously, and mixed urinary incontinence (MUI), which is the co-occurrence of SUI and UUI. UI has a complex aetiology: SUI and UUI have common epidemiologic features and clinical course as well as unique symptom evolution (Irwin et al. Citation2010).
Population-based epidemiologic studies have shown that UI is more frequent in women, with a prevalence rate of around 30%, although this varies considerably depending on the country and research methodology (Minassian et al. Citation2003, Cerruto et al. Citation2013, Zhang et al. Citation2015, Velázquez-Saornil et al. Citation2021). With the ageing of the global population, the prevalence of UI is likely to increase and it is already becoming a significant public health concern worldwide (Chai et al. Citation2017). UI has psychological effects such as embarrassment, depression, anxiety, and social isolation that reduce patients’ quality of life (Esparza et al. Citation2018, Pizzol et al. Citation2021), and also places a heavy economic burden on society, with hundreds of millions of dollars in medical expenditure (Milsom et al. Citation2014).
The natural history of a disease is the entire course of its occurrence, development, and outcome in the absence of any therapeutic interventions, which includes the biological pathogenesis, preclinical and clinical development, and outcome (Xiushan and Fang Citation2020). UI is a dynamic disease with a long progressive course, many factors contribute to its incidence, aggravation, or remission (Irwin et al. Citation2010, Komesu et al. Citation2016). Clarifying the evolution of symptoms in UI can help women develop optimal management of the disease to reduce medical expenses, excellent It is of great significance to improve medical services and patients’ life quality. However, the development of urinary incontinence in adult women is poorly understood. With the deepening of research, the understanding of the natural history of urinary incontinence has also undergone profound changes in recent years. The new findings about UI symptoms longitudinal change and associated factors are summarised and discussed in this review.
2. Methods
Three databases including PubMed, EMBASE and Web of Science were searched for our studies. The retrieval strategy was based on the combination of Mesh terms and text words, including Subject ‘Female/Women’, Subject ‘Urinary incontinence/Lower urinary tract symptoms’, then searching the results for ‘natural history’ or ‘course’ or ‘progress’, the retrieval time range is set from 1 January 2010 to 1 January 2020.
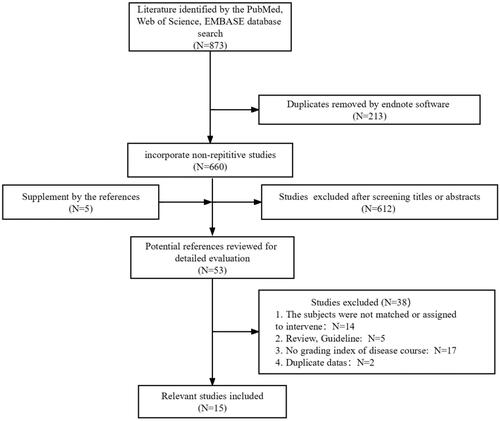
The inclusion criteria for this review were: (1) Sample size >100; (2) Study participants were adult women (≥18 years old); (3) Studies discussed incidence, persistence, progression, remission, and regression of UI and/or associated factors of UI; and (4) Course of disease measures used clearly definition. The exclusion criteria were (1) Studies on taking any interventions for study participants; and (2) narrative or systematic reviews, meta-analyses, or clinical guidelines; (3) studies that were not in English, and the full-text was not available. A systematic review was not attempted for this topic due to the small number of relevant studies and the diversity in the measurement of disease progression of UI in the literature. Two researchers independently screening titles, abstracts and full-text according to the inclusion criteria and extracted data from them, then their reference lists were scanned for further relevant articles. Flow diagram for the review process see .
Figure 1. Flow diagram for the review process.
3. Results
A total of 15 studies were used to examine advances in UI research in the past 10 years, see . The studies were summarised using a narrative descriptive approach with a focus on the natural history of female UI including single-subtype disease progression and interactions between different subtypes.
Table 1. Summary of studies on the natural history of female urinary incontinence in the last decade.
3.1. Research methods for the natural history of female UI
A longitudinal study design is used to examine symptom evolution during the progression of UI in females and identify the risk factors for disease in cross-sectional studies. Many large cohort studies have been carried out in many countries, including the Nurses’ Health Study (Hagan et al. Citation2018, Minassian et al. Citation2020), a longitudinal cohort study of overactive bladder (OAB) (Minassian et al. Citation2016, Citation2018), Norwegian Health Study (Ebbesen et al. Citation2013), and Mexican Health and Ageing Research (Giraldo-Rodríguez et al. Citation2019). UI is mostly evaluated using standardised self-report scales including the UI Severity Index, International Consultation on Incontinence Questionnaire (ICIQ) – Short Form, Urogenital Distress Inventory, Bristol Female Lower Urinary Tract Symptoms Questionnaire, Women’s Toileting Behaviour Scale, voiding diary, etc (Liqiong et al. Citation2017). These scales have been validated and have good sensitivity and specificity, and are easy to use to assess the frequency of UI, severity of leakage, and impact on quality of life; as such, they are also suitable for epidemiologic studies of UI. The natural progression from a single subtype of UI and the mutual influence of different subtypes are summarised in the following sections based on findings from the selected studies.
Most published studies have described the natural course of UI including incidence, persistence, progression, remission, and regression (Ebbesen et al. Citation2013, Erekson et al. Citation2016, Hagan et al. Citation2018, Giraldo-Rodríguez et al. Citation2019, Legendre et al. Citation2020). Disease severity is an important indicator of UI progression, but its assessment varies across studies. Pad weighing rests are used for evaluating the severity of incontinence as an objective measure, which are the best ‘gold standard’. Nevertheless, such an approach is time-and energy-consuming as well as omitting subjective feelings of patients. Multiple guidelines state that the self-report assessment tool can accurately and truly reflect the severity of urinary incontinence. In most cases the Incontinence Severity Index (ISI) (Sandvik et al. Citation1993) is used, this is created by multiplying the frequency (four levels) by the amount of urine leakage (two levels). The severity of urine leakage is categorised as no UI (0 points), slight UI (1–2 points), moderate UI (3–5 points), and severe UI (6–8 points). ISI has been well verified and widely used in different people, due to its brevity and credibility. However, the scale is too simple to distinguish the subtypes of urinary incontinence (Klovning et al. Citation2009). There have also been studies using the ICIQ, which is not just used to evaluate the symptoms of urinary incontinence, but also the severity of urinary incontinence based on the frequency, amount of urine leakage, and impact on the quality of life (Klovning et al. Citation2009) and is divided into the following 4 categories: mild (1–5 points), moderate (6–12 points), severe (13–18 points), and extremely severe (19–21 points). However, the current guidelines hold different opinions on the practicality and evidence level of ICIQ, and the division of severity among different people still needs further exploration (Sussman et al. Citation2020).
The optimal depiction of the natural history of UI requires better recognition of its subtypes due to their unique symptom evolution. Currently, there are many diagnostic tools and methods to differentiate between the types of UI, including questionnaires, ‘Q‐tip’ test, pad tests, the physical examination and the overall clinical assessment of which, a number of questionnaires exist to help differentiate these conditions in a more standardised way, such as Bristol Female Lower Urinary Tract Symptoms questionnaire (Khan et al. Citation2004), Michigan Incontinence Symptom Index (Bradley et al. Citation2005), etc. A systematic review (Holroyd-Leduc et al. Citation2008) reported that the most helpful component for diagnosing UUI is a history of urine loss associated with urgency, and a bladder stress test may be helpful for diagnosing SUI.
3.2. Natural history of a single subtype of UI and related factors
3.2.1. Stress UI
Stress UI is the main subtype of UI in young and middle-aged women. Data from the 2001 to 2002 National Health and Nutrition Examination Survey showed that the prevalence of SUI was 23.9% and was highest in women between 40 and 50 years of age, with the prevalence declining thereafter (Minassian et al. Citation2008). Among Japanese adult females, the prevalence of SUI was reported to be 19.3%, with the 40–49 and 50–59 years age groups accounting for 31.4% and 52.1%, respectively (Azuma et al. Citation2008). A few epidemiologic studies of female UI have been conducted in China, the largest survey was carried out in 2006 using the International Questionnaire Female Lower Urinary Tract Symptoms, and reported a prevalence of 18.9% for SUI—the most common subtype—in women >20 years old. The prevalence was highest in the 50–59 age group and the overall prevalence rate was lower than that of women in Western countries and other Asian countries (Zhang et al. Citation2015). In summary, SUI is the most prevalent subtype of UI worldwide, with the highest incidence observed in women in the age range of 50–59 years. SUI is caused by dysfunction of the internal urethral sphincter and pelvic floor muscles, fascia and ligament relaxation, and high urethral mobility (Aoki et al. Citation2017). A 10-year follow-up study of 2229 women found that the annual incidence of UI was 3.5%–4.5% in the 41–55 age group and that SUI was the main subtype, with most women experiencing mild symptoms that remained stable during the follow-up period (Jahanlu and Hunskaar Citation2010). In another study of 40–69 middle-aged and elderly women, 31% of subjects without UI at baseline reported new-onset SUI after 5 years, and the rate declined with age (Thom et al. Citation2010). There is evidence that SUI is the UI subtype most likely to enter symptomatic remission: in the French Women’s Health Cohort study, the annual remission rate of SUI was 4.7% (Legendre et al. Citation2020), and in a longitudinal study of 10,572 women in the United States conducted from 2004 to 2010, the annual remission rate of SUI in the 50–59 age group was 13.8%–17.7% and the overall prevalence of SUI did not increase significantly during this period (Komesu et al. Citation2016). In a study conducted in Norway, the annual remission rate of SUI for women >55 years of age was 14.8%, with milder symptoms being associated with a higher remission rate at the 11-year follow-up (Ebbesen et al. Citation2013). Thus, the severity of symptoms at onset affects the progression and remission of UI. Genetics, pregnancy, childbirth, depression, and obesity affect SUI onset and progression. The prevalence of SUI was 2 to 3 times higher among women with first-degree female relatives with SUI than among those with non-incontinent first-degree female relatives (Ertunc et al. Citation2004). Moreover, members of so-called UI families have a relatively young age of symptom onset, underscoring the contribution of genetics to UI aetiology. Pregnancy and childbirth also influence the clinical course of SUI. The incidence of UI was shown to increase gradually from prepregnancy to pregnancy, and was highest in the third trimester; in a prospective cohort study of 1535 pregnant women in Australia, the prevalence of UI was 10.8% in prepregnancy, 16% during early pregnancy, and 55.9% in the third trimester (Brown et al. Citation2010). Postpartum UI is also an important medical problem. In a survey of Chinese primiparas, the prevalence of UI at 6 weeks postpartum was 9.46% (955/10098) and the most common UI subtype was SUI (Lin Citation2010). Additionally, a meta-analysis of 15 cross-sectional studies (Tähtinen et al. Citation2016) showed that the long-term risk of SUI was nearly 2 times higher with vaginal delivery as compared to caesarean section and the absolute risk of moderate or severe SUI was increased by 8%, with the impact being greatest in young women and decreasing with age. A recent study of adult females with UI in Jiangsu Province, China showed that SUI was more prevalent in rural residents (44.0%) than in women in urban areas (28.9%), which could be attributed to the higher exposure to UI risk factors in the former group such as weight-bearing activities, physical labour, and multiple childbirths (95.6% of rural women had parity ≥2 as compared to 5.2% of urban women) (Sun et al. Citation2019). Depression is another risk factor for SUI. Findings from an 8-year prospective study of middle-aged French women suggested that the depression status of women at baseline was related to the incidence of new-onset SUI during follow-up, which confirmed that depression occurred before SUI onset (Legendre et al. Citation2020). Depression-associated changes in the level of the neurotransmitter serotonin can trigger UI, as serotonin is related to vesicle and urethral sphincter function. It has been proposed that depression-related autonomic nervous system dysfunction increases circulating cortisol and the level of catecholamine’s that induce changes in urethral sphincter function (Giraldo-Rodríguez et al. Citation2019). Obesity is closely linked to all subtypes of UI, long-term obesity has an effect similar to vaginal delivery in that it weakens the pelvic floor and urethral support structures, inducing the onset of SUI (Wesnes Citation2014). Body mass index (BMI) has been identified as an independent risk factor for SUI, but studies from China (Zhu et al. Citation2009), South Korea (Hunskaar et al. Citation2004), and the U.S. (Maserejian et al. Citation2014) have demonstrated that waist circumference is a better indicator of obesity and predictor of SUI. Other risk factors that can influence the occurrence of SUI such as ethnicity, menopause, and number of chronic diseases warrant more detailed investigation.
3.2.2. Urgency UI
Urgency UI is a symptom of and has similar epidemiology to OAB and other types of UI, but has not been well studied. According to a systematic review of 22 large population-based surveys, the estimated prevalence of UUI is 1.8%–30.5% in Europe, 1.7%–36.4% in the U.S., and 1.5%–15.2% in Asia (Milsom et al. Citation2014). The prevalence of UUI among Chinese women was reported to be 2.0%, and was lowest among 20-year-olds; the proportion increased with age, reaching a peak (8.1%) in women over the age of 70 years before gradually decreasing (Wang et al. Citation2011). Although UUI is the least common UI subtype among women, it has the most disruptive symptomatology (Agarwal et al. Citation2014), that is, the symptoms are more severe than those of SUI, are more likely to cause anxiety and depression, and have greater negative impact on patients’ quality of life (Hansson Vikström et al. Citation2021). UUI in females arises from abnormal bladder function; the main causes are detrusor muscle over activity, poor detrusor compliance, and bladder hyper responsiveness (Aoki et al. Citation2017). Among UI subtypes, UUI was associated with the oldest average age (60.0 years) at onset and the highest BMI (28.8 kg/m2), and was more likely to progress to severe UI (Minassian et al. Citation2020). Longitudinal data from 2004 to 2010 Health and Retirement Study of 10,572 women with UI over the age of 50 years showed that the incidence of UUI increased with age, and the odds ratio was about 9 times higher for women >90 years old than for those aged 50–60 years (Komesu et al. Citation2016). UUI severity has been classified into the following 4 stages based on symptoms: (1) no urinary symptoms, (2) urgency but no incontinence, (3) non-severe UUI (leakage frequency <1/day), and (4) severe UUI (leakage frequency ≥1/day) (Zhou et al. Citation2018). The progression from urgent symptoms to non-severe UUI occurs over 8–9 years, while the time interval of progression from non-severe to severe UUI may be shorter, although the underlying mechanisms are not fully understood. UUI also has the highest remission rate among UI subtypes (17%–45.5%) (Komesu et al. Citation2016, Giraldo-Rodríguez et al. Citation2019), remission is more common in young women with no comorbidities or functional limitations because they are more likely to have predisposing factors for UI such as urinary tract infection and intestinal disturbance that resolve even without treatment (Herzog et al. Citation1990). It was reported that professional women are at increased risk of UUI progression as a result of adopting unhealthy urination behaviours in order to adapt to their work rhythm such as delayed or premature voiding and straining to urinate (Zhou et al. Citation2018). One study showed that the physical activity level of older women with UUI was one-fifth that of women without UUI, providing evidence for a causal relationship between low physical activity and UUI/OAB (Jerez-Roig et al. Citation2020). UUI is associated with metabolic syndrome (Bunn et al. Citation2015), for which sedentary behaviour is an independent risk factor. Diabetes is closely related to UUI, elevated blood sugar may cause urine to become hypertonic, increasing the risk of frequent urination and urgency. Moreover, diabetic microvascular damage can lead to neurologic bladder dysfunction by affecting the stability of the detrusor muscle and integrity of the urethral sphincter. Interestingly, urgency can be improved by controlling blood sugar (Lawrence et al. Citation2007). Several other factors such as BMI, presence of >2 chronic diseases, a history of falls, and limited physical function may also contribute to the onset of UUI (Komesu et al. Citation2016, Giraldo-Rodríguez et al. Citation2019).
3.2.3. Mixed UI
Mixed UI is the most common subtype of UI in women aged >65 years (Minassian et al. Citation2003, Citation2017). In a study of 5204 American women, the prevalence of MUI was 34.4% overall and as high as 55.5% among 60-year-old women (Digesu et al. Citation2008). In a study of women >18 years of age in France, Germany, Spain, and the United Kingdom, the prevalence was 25%–40% (Komesu et al. Citation2016). A survey of lower urinary tract symptoms in 6 regions of China showed that the prevalence of MUI in the Chinese population was about 9.4%, which is similar to other Asian countries and lower than in Europe and the U.S. (Zhu et al. Citation2010). The prevalence of MUI increases with age, and it is the predominant subtype in later adulthood. Some studies have reported that MUI is more problematic for women than SUI or UUI and has a greater impact on quality of life (Luo et al. Citation2022). In MUI, SUI and UUI symptoms occur simultaneously and can have mutually aggravating effects. MUI mainly results from bladder and urethral dysfunction and has non-specific pathophysiologic characteristics. It has been proposed that MUI is a manifestations of severe UI symptoms rather than a combination of 2 UI subtypes (Bump et al. Citation2003). MUI can arise independently and may be asymptomatic, or may develop from simple UI (SUI or UUI). Most MUI symptoms are severe at the time of onset and may change (e.g. persist or worsen) during follow-up; on the contrary, MUI can revert to simple UI or enter remission. A study in Mexico that examined the relationship between sex and the different UI subtypes in community residents >50 years old found that in elderly females, MUI had the highest new incidence rate (8.7%), which increased with age from 6.9% in 50- to 59-year-olds to 11.8% in 90-year-olds (Giraldo-Rodríguez et al. Citation2019). A 10-year follow-up study of 50- to 70-year-old women found that MUI symptoms were mostly moderate to severe and were more likely to persist in the elderly, and were rarely relieved and unlikely to revert to simple UI (Erekson et al. Citation2016). Other studies have reported low remission rates for MUI: only 8% of women with mild and moderate MUI experienced complete remission after 4 years of follow-up, with an even lower rate for severe MUI (4%) (Giraldo-Rodríguez et al. Citation2019, Minassian et al. Citation2020). The presence of multiple chronic diseases (≥2 chronic diseases) can impact the incidence, type, and severity of UI. A study conducted in the U.S. showed that only 11% of elderly women with UI had no comorbidities; based on cluster analysis, 12 chronic diseases in women with UI were divided into 4 categories—cardiovascular disease (CVD) risk – younger, asthma-predominant, CVD risk – older, and multiple chronic conditions (MCC), with women in the MCC cluster showing the highest rates of MUI (43%) and moderate (40%) or severe (18%) symptoms (Markland et al. Citation2018). Obesity is an independent risk factor for each UI subtype and the severity of UI and MUI. A meta-analysis of 24 prospective studies revealed that for every 5-unit increase in BMI, the morbidity of MUI increased by 52%; even within the range of normal BMI values, the association was approximately linear (Aune et al. Citation2019). Other risk factors for MUI are advanced age, depression, poor health, and limitations in physical function.
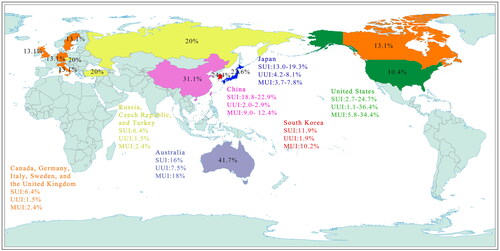
To sum up, we presented the result about the prevalence of three subtypes of UI throughout the world in the form of map for better visualisation, see .
Figure 2. Prevalence of three subtypes of urinary incontinence in female in parts of the world.
3.3. Interaction between the three subtypes of UI
3.3.1. Transition between the three UI subtypes
Most studies on the natural history of UI define progression as advancing from a mild to severe disease state; however, the transition from one UI subtype to another is another form of disease progression. Epidemiologic evidence has demonstrated that dynamic transitions occur between the three subtypes of UI: 1%–9% and 15%–27.4% of women with UUI develop SUI and MUI, respectively; among women with SUI, 1.5%–7% and 13%–34% transition to UUI and MUI, respectively; and among those with MUI, 8.6%–28% and 5.6%–25% revert to UUI and SUI, respectively (Komesu et al. Citation2016, Minassian et al. Citation2018, Citation2020). The relationship between SUI and UUI is not fully understood but assuming that they have independent onset, the prevalence of MUI is 17 times higher than would be expected from the effects of the 2 simple UIs (Minassian et al. Citation2008).
3.3.2. Interaction between SUI and UUI
A study conducted in the U.S. that analysed the characteristics of 950 episodes of urinary control disorder in 35 women with MUI over 30 consecutive days found that respiratory events such as coughing or sneezing preceded 52.5% of UUI episodes, meanwhile, 24 of the subjects reported that at least one episode of UUI was triggered by a respiratory event, which was the most common cause of urinary control disorder (Petros Citation2011). These results suggest that the presence of a UI subtype (e.g. SUI) increases the risk of developing another subtype (e.g. UUI). The transition of SUI to UUI may explain the decline in the prevalence of the former and the increase in that of MUI in women after the age of 50 years, which could represent the progression of UI. It can be difficult to distinguish SUI from UUI, given their pathologic similarities. SUI onset may be triggered by damage to the pelvic floor caused by physiologically stressful events such as childbirth or weight gain. Continuous exposure to stressors may increase the number of spontaneous SUI episodes, thereby increasing the sensitivity of the neuromuscular response and reducing the threshold of urinary urgency and leading to MUI.
3.3.3. Ui severity and transition
The severity of UI determines its progression and transition. According to the Sandvik Severity Index score, the incidence of severe UI is nearly 2 times higher in MUI than in SUI (Minassian et al. Citation2013). It was recently reported that mild-to-moderate simple UI (SUI or UUI) at symptom onset was relatively stable and that simple UI with severe symptoms at onset in obese individuals and SUI in women >70 years of age were more likely to progress to MUI (Minassian et al. Citation2020). A study of women over the age of 60 years showed that the frequency of severe UI and MUI did not change over the 2-year follow-up, The progression of UI from mild to severe is consistent with the progress from simple to mixed (Herzog et al. Citation1990). Compared to MUI, patients with SUI are more likely to have mild symptoms—that is, UI severity and subtype are interrelated, with changes in severity partly reflecting the transition between subtypes. The results of a 4-year longitudinal study showed that the probability of conversion from SUI (34%) and UUI (27%) to MUI was significantly higher than that from MUI to SUI (6%) and UUI (9%); moreover, MUI with milder symptoms was more likely to transform into simple UI during the follow-up period (Minassian et al. Citation2018). It has also been shown that women with MUI are less likely to enter remission, and those in remission are more likely to relapse than women with SUI or UUI (Komesu et al. Citation2016). Thus, while one UI subtype can transform into another, the general trend is one of progression to MUI, which is likely an advanced stage of UI.
4. Discussion
This review discusses the current state of knowledge regarding the characteristics and progression of different subtypes of UI in adult females. With the various study populations and study methodologies, comparisons between epidemiological reports are difficult to make. Moreover, evidence from studies indicates that the prevalence of the three subtypes of UI in women varies according to life stage, and their symptom evolution is also affected by different factors (Komesu et al. Citation2016, Giraldo-Rodríguez et al. Citation2019, Minassian et al. Citation2020). They differ in terms of incidence and progression, reflecting distinct pathophysiologic mechanisms, but also interact with each other during disease progression. Studies of female patients have shown that simple UI (SUI or UUI) can transform into MUI (SUI and UUI) and vice versa (Minassian et al. Citation2016, Citation2018). The findings can guide the development of interventions to prevent the progression of UI to MUI. Successful management should be multidimensional and dynamic by the fluctuating nature of the symptoms experienced by UI women. There is growing consensus that effective preventive measures should be taken earliest possible, perhaps the little or no UI stage, to be effective. There are some studies that Moderate exercise (de Mattos Lourenco et al. Citation2018), weight loss (Subak et al. Citation2015), glucose control (Wang et al. Citation2015) and smoking cessation (Kawahara et al. Citation2020) may reduce incidence of UI in Women residing in the community. In particular, incontinence is more likely to occur in certain time period’s in a women’s life, such as pregnancy, childbirth and warrant special consideration. A Cochrane review (Woodley et al. Citation2017) concluded that level 1 evidence for PFM exercises existed for continent pregnant women during pregnancy and up to 6 months after delivery. Few primary prevention interventions for UI exist for nonchildbearing adolescent and adult women. When women have severe symptoms or mixed urinary incontinence, a variety of treatment options are available including behavioural therapy, physical therapy, drugs and surgical treatment, but no single method is effective for every woman, and likely must be carefully matched to the individual women and their disease stages. It is proved to be effective to formulate comprehensive intervention therapy based on type of UI, patient preference and other factors (Visser et al. Citation2015). What’s more, research interest in foundational knowledge to explore innovative UI intervention programs and management approaches path is growing, which will may be a good breakthrough.
It is worth mentioning that, we discovered the causal relationships between psychological symptoms and urinary incontinence are very complicated when analysing the related factors of disease progression. In one longitudinal study anxiety was both a risk factor and a consequence of incontinence (Felde et al. Citation2017). In addition, recent studies have found that patients with psychiatric disorders (such as obsessive-compulsive disorders and eating disorders) appeared to have increased occurrence of functional urinary symptoms (Ng et al. Citation2021, Citation2022). Unfortunately, the current evidence base is very limited and its specific mechanism has yet to be conclusively determined.
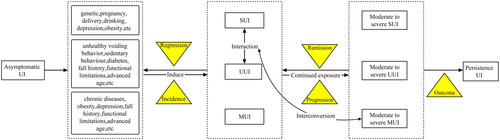
Although most of the mechanisms underlying the risk factors are unknown, we can still take preventive measures based on the identified factors of UI in different disease states, so as to improve the life quality of women across their lifecourse. In general, Future research should systematically analyse the progression of each subtype of UI and interactions between subtypes. Exploring these transitions and influencing factors can provide insight into the natural history of UI, which can in turn guide clinical evaluation and decision-making. The natural history of UI as well as risk factors and age-related changes thereof are summarised in .
Figure 3. The natural history of UI as well as risk factors and age-related changes.
The studies included in our review mostly adopts longitudinal follow-up research design. Longitudinal studies can reveal the temporal characteristics of UI symptoms, but most studies have a short follow-up time and a small sample size, making it difficult to establish the actual clinical course of UI. Zhou et al. (Citation2018) adopted a cross-sectional study design to compare the characteristics of two adjacent stages of SUI, thus providing significant insight into the factors that affect the dynamic progression of this disease.
Strengths of this review lies in distinguishing different UI subtypes to describe the epidemiological characteristics of the natural course of UI, Secondly, we presented an exhaustive list of factors related to the progress of UI, so our study provides important information about nature history on the three subtypes of UI. Although, we have not applied a systematic review of the literature, including comprehensive search strategy in all languages and thorough assessment of study quality, which is an important limitation for our study. We found there were limited available studies in this study field, while more number of studies were available with regard to transverse epidemiology of UI, Nevertheless, this detail mechanism and patterns of UI progression really deserves further study.
5. Conclusion
The severity of symptoms and conversion between different subtypes indicate that UI is a complex disease. Advanced age and obesity are risk factors for all UI subtypes, each of which also has distinct features. For example, pregnancy and childbirth are triggers for SUI; unhealthy voiding behaviour and low physical activity may contribute to UUI onset; and chronic diseases and poor health increase the risk of MUI. Despite the limitation that the evidence emerges from not systematically collected data, our review can provide a basis for developing effective prevention and treatment.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abrams, P., et al., 2002. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. American journal of Obstetrics and Gynecology, 187 (1), 116–126.
- Agarwal, A., et al., 2014. What is the most bothersome lower urinary tract symptom? Individual- and population-level perspectives for both men and women. European urology, 65 (6), 1211–1217.
- Aoki, Y., et al., 2017. Urinary incontinence in women. Nature Reviews, 3, 17042.
- Aune, D., et al., 2019. Body mass index, abdominal fatness, weight gain and the risk of urinary incontinence: a systematic review and dose-response meta-analysis of prospective studies. An International Journal of Obstetrics and Gynaecology, 126 (12), 1424–1433.
- Azuma, R., et al., 2008. Prevalence and risk factors of urinary incontinence and its influence on the quality of life of Japanese women. Nursing & Health Sciences, 10 (2), 151–158.
- Botlero, R., et al., 2011. Incidence and resolution rates of different types of urinary incontinence in women: findings from a cohort study. The Journal of Urology, 185 (4), 1331–1337.
- Bradley, C.S., et al., 2005. A new questionnaire for urinary incontinence diagnosis in women: development and testing. American Journal of Obstetrics and Gynecology, 192 (1), 66–73.
- Brown, S.J., et al., 2010. Urinary incontinence in nulliparous women before and during pregnancy: prevalence, incidence, and associated risk factors. International Urogynecology Journal, 21 (2), 193–202.
- Bump, R.C. et al., 2003. Mixed urinary incontinence symptoms: urodynamic findings, incontinence severity, and treatment response. Obstetrics and Gynecology, 102 (1), 76–83.
- Bunn, F., et al., 2015. Is there a link between overactive bladder and the metabolic syndrome in women? A systematic review of observational studies. International Journal of Clinical Practice, 69 (2), 199–217.
- Cerruto, M.A., et al., 2013. Prevalence, incidence and obstetric factors’ impact on female urinary incontinence in Europe: a systematic review. Urologia internationalis, 90 (1), 1–9.
- Chai, T.C., et al., 2017. Future directions of research and care for urinary incontinence: findings from the national institute of diabetes and digestive and kidney diseases summit on urinary incontinence clinical research in women. The Journal of Urology, 198 (1), 22–29.
- Daly, D., Clarke, M. and Begley, C., 2018. Urinary incontinence in nulliparous women before and during pregnancy: prevalence, incidence, type, and risk factors. International urogynecology Journal, 29 (3), 353–362.
- de Mattos Lourenco, T.R., et al., 2018. Urinary incontinence in female athletes: a systematic review. International urogynecology Journal, 29 (12), 1757–1763.
- Digesu, G.A., et al., 2008. Mixed urinary symptoms: what are the urodynamic findings? Neurourology and Urodynamics, 27 (5), 372–375.
- Ebbesen, M.H., et al., 2013. Prevalence, incidence and remission of urinary incontinence in women: longitudinal data from the Norwegian HUNT study (EPINCONT). BMC Urology, 13 (1), 2–10.
- Erekson, E.A., et al., 2016. Ten-year prevalence and incidence of urinary incontinence in older women: a longitudinal analysis of the health and retirement study. Journal of the American Geriatrics Society, 64 (6), 1274–1280.
- Ertunc, D., et al., 2004. Is stress urinary incontinence a familial condition? Acta obstetricia et gynecologica Scandinavica, 83 (10), 912–916.
- Esparza, A.O., Tomás, M.Á C. and Pina-Roche, F., 2018. Experiences of women and men living with urinary incontinence: a phenomenological study. Applied Nursing Research, 40, 68–75.
- Espuña-Pons, M. et al., 2017. Prevalence, incidence, and remission rates of urinary incontinence in women attended in gynecological practice. Neurourology and Urodynamics, 36 (4), 1081–1085.
- Felde, G., Ebbesen, M.H. and Hunskaar, S., 2017. Anxiety and depression associated with urinary incontinence. A 10-year follow-up study from the Norwegian HUNT study (EPINCONT). Neurourology and Urodynamics, 36 (2), 322–328.
- Giraldo-Rodríguez, L., et al., 2019. Epidemiology, progression, and predictive factors of urinary incontinence in older community-dwelling Mexican adults: longitudinal data from the Mexican Health and Aging Study. Neurourology and Urodynamics, 38 (7), 1932–1943.
- Hagan, K.A., et al., 2018. A prospective study of the natural history of urinary incontinence in women. American journal of Obstetrics and Gynecology, 218 (5), 502.e1-502–e8.
- Hansson Vikström, N., et al., 2021. Anxiety and depression in women with urinary incontinence using E-health. International Urogynecology Journal, 32 (1), 103–109.
- Herzog, A.R., et al., 1990. Two-year incidence, remission, and change patterns of urinary incontinence in noninstitutionalized older adults. Journal of Gerontology, 45 (2), M67–74.
- Holroyd-Leduc, J.M., et al., 2008. What type of urinary incontinence does this woman have? JAMA, 299 (12), 1446–1456.
- Hunskaar, S., et al., 2004. The prevalence of urinary incontinence in women in four European countries. BJU International, 93 (3), 324–330.
- Irwin, D.E., et al., 2010. Dynamic progression of overactive bladder and urinary incontinence symptoms: a systematic review. European Urology, 58 (4), 532–543.
- Jahanlu, D. and Hunskaar, S., 2010. The Hordaland Women’s Cohort: prevalence, incidence, and remission of urinary incontinence in middle-aged women. International Urogynecology Journal, 21 (10), 1223–1229.
- Jerez-Roig, J., et al., 2020. Is urinary incontinence associated with sedentary behaviour in older women? Analysis of data from the National Health and Nutrition Examination Survey. PLoS One, 15 (2), e0227195.
- Kawahara, T., et al., 2020. Impact of smoking habit on overactive bladder symptoms and incontinence in women. International Journal of Urology, 27 (12), 1078–1086.
- Khan, M.S., et al., 2004. The relationship between urinary symptom questionnaires and urodynamic diagnoses: an analysis of two methods of questionnaire administration. An International Journal of Obstetrics and Gynaecology, 111 (5), 468–474.
- Klovning, A., et al., 2009. Comparison of two questionnaires for assessing the severity of urinary incontinence: the ICIQ-UI SF versus the incontinence severity index. Neurourology and Urodynamics, 28 (5), 411–415.
- Komesu, Y.M., et al., 2016. Epidemiology of mixed, stress, and urgency urinary incontinence in middle-aged/older women: the importance of incontinence history. International Urogynecology Journal, 27 (5), 763–772.
- Lawrence, J.M., et al., 2007. Pelvic floor disorders, diabetes, and obesity in women: findings from the Kaiser Permanente Continence Associated Risk Epidemiology Study. Diabetes Care, 30 (10), 2536–2541.
- Legendre, G., et al., 2020. Incidence and remission of stress, urge, and mixed urinary incontinence in midlife and older women: a longitudinal cohort study. Neurourology and Urodynamics, 39 (2), 650–657.
- Lin, L., 2010. The epidemiologic study of primipara with urinary incontience in china–multicentric prospective cohort study. Doctor of Philosophy. Peking Union Medical College.
- Liqiong, S., et al., 2017. Research progress of urinary incontinence symptom assessment tools. Journal of Nursing Science, 32, 107–110.
- Luo, Y., et al., 2022. Prevalence and risk factors of urinary incontinence among elderly adults in Rural China: a cross-sectional survey. Journal of Wound, Ostomy, and Continence Nursing, 49 (1), 78–86.
- Markland, A.D., et al., 2018. Cluster analysis of multiple chronic conditions associated with urinary incontinence among women in the USA. BJU International, 122 (6), 1041–1048.
- Maserejian, N.N., et al., 2014. Treatment status and risk factors for incidence and persistence of urinary incontinence in women. International Urogynecology Journal, 25 (6), 775–782.
- Milsom, I., et al., 2014. Global prevalence and economic burden of urgency urinary incontinence: a systematic review. European Urology, 65 (1), 79–95.
- Minassian, V.A., Bazi, T. and Stewart, W.F., 2017. Clinical epidemiological insights into urinary incontinence. International Urogynecology Journal, 28 (5), 687–696.
- Minassian, V.A., et al., 2013. Severity of urinary incontinence and effect on quality of life in women by incontinence type. Obstetrics and Gynecology, 121 (5), 1083–1090.
- Minassian, V.A., Drutz, H.P. and Al-Badr, A., 2003. Urinary incontinence as a worldwide problem. International Journal of Gynaecology and Obstetrics, 82 (3), 327–338.
- Minassian, V.A., et al., 2020. The natural history of urinary incontinence subtypes in the Nurses’ Health Studies. American Journal of Obstetrics and Gynecology, 222 (2), 163.e1-163–e8.
- Minassian, V.A., Stewart, W.F. and Hirsch, A.G., 2008. Why do stress and urge incontinence co-occur much more often than expected? International Urogynecology Journal and Pelvic Floor Dysfunction, 19 (10), 1429–1440.
- Minassian, V.A., Stewart, W.F. and Wood, G.C., 2008. Urinary incontinence in women: variation in prevalence estimates and risk factors. Obstetrics and Gynecology, 111 (2 Pt 1), 324–331.
- Minassian, V.A., et al., 2018. Does transition of urinary incontinence from one subtype to another represent progression of the disease? International Urogynecology Journal, 29 (8), 1179–1185.
- Minassian, V.A., et al., 2016. Mixed incontinence masked as stress induced urgency urinary incontinence. The Journal of Urology, 196 (4), 1190–1195.
- Ng, Q.X., et al., 2022. Females with eating disorders and urinary incontinence: a psychoanalytic perspective. International Journal of Environmental Research and Public Health, 19 (8), 4874.
- Ng, Q.X., et al., 2021. Obsessive-compulsive disorders and functional urinary disorders: a fortuitous association? Behavioural Sciences, 11 (6), 89.
- Petros, P.E., 2011. Mixed urinary incontinence–time to uncouple urgency from stress? International Urogynecology Journal, 22 (8), 919–921.
- Pizzol, D., et al., 2021. Urinary incontinence and quality of life: a systematic review and meta-analysis. Aging Clinical and Experimental Research, 33 (1), 25–35.
- Sandvik, H., et al., 1993. Validation of a severity index in female urinary incontinence and its implementation in an epidemiological survey. Journal of Epidemiology and Community Health, 47 (6), 497–499.
- Subak, L.L., et al., 2015. Urinary incontinence before and after bariatric surgery. JAMA Internal Medicine, 175 (8), 1378–1387.
- Sun, Y.L., et al., 2019. Analysis of the prevalence of and factors associated with urinary incontinence among urban and rural adult women in Xuzhou, Jiangsu Province of China. Journal of Nurses Training, 34, 1881–1883.
- Sussman, R.D., Syan, R. and Brucker, B.M., 2020. Guideline of guidelines: urinary incontinence in women. BJU International, 125 (5), 638–655.
- Tähtinen, R.M., et al., 2016. Long-term impact of mode of delivery on stress urinary incontinence and urgency urinary incontinence: a systematic review and meta-analysis. European Urology, 70 (1), 148–158.
- Thom, D.H., et al., 2010. Incidence of and risk factors for change in urinary incontinence status in a prospective cohort of middle-aged and older women: the reproductive risk of incontinence study in Kaiser. The Journal of Urology, 184 (4), 1394–1401.
- Velázquez-Saornil, J., et al., 2021. Observational study on the prevalence of urinary incontinence in female athletes. International Journal of Environmental Research and Public Health, 18 (11), 5591.
- Visser, E., et al., 2015. Active encouragement of older women with urinary incontinence in primary care to undergo diagnosis and treatment: a matched-pair cluster randomized controlled trial. Maturitas, 80 (2), 212–219.
- Wang, R., et al., 2015. Diabetes, glycemic control, and urinary incontinence in women. Female Pelvic Medicine & Reconstructive Surgery, 21 (5), 293–297.
- Wang, Y., et al., 2011. Prevalence, risk factors, and impact on health related quality of life of overactive bladder in China. Neurourology and Urodynamics, 30 (8), 1448–1455.
- Wesnes, S.L., 2014. Weight and urinary incontinence: the missing links. International Urogynecology Journal, 25 (6), 725–729.
- Woodley, S.J., et al., 2017. Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database System Review, 12, CD007471.
- Xiushan, G. and Fang, S., 2020. Application of natural history research in spinal muscular atrophy. China Medical Herald, 17, 177–180.
- Zhang, L., et al., 2015. A population-based survey of the prevalence, potential risk factors, and symptom-specific bother of lower urinary tract symptoms in adult chinese women. European Urology, 68 (1), 97–112.
- Zhou, F., Newman, D.K. and Palmer, M.H., 2018. Urinary urgency in working women: what factors are associated with urinary urgency progression? Journal of Women’s Health, 27 (5), 575–583.
- Zhu, L., et al., 2009. The epidemiological study of women with urinary incontinence and risk factors for stress urinary incontinence in China. Menopause, 16 (4), 831–836.
- Zhu, L., et al., 2012. Prevalence and risk factors for peri- and postpartum urinary incontinence in primiparous women in China: a prospective longitudinal study. International Urogynecology Journal, 23 (5), 563–572.
- Zhu, L., et al., 2010. Epidemiology of mixed urinary incontinence in China. International journal of Gynaecology and Obstetrics, 109 (1), 55–58.