

Abstract
We aimed to investigate the blood pressure (BP) patterns of hypertensive disorders of pregnancy (HDP) in the first and second trimesters and its contributing factors, which may help us understand its pathogenesis and identify this group of diseases in a timely manner. SPSS 21.0 was used to describe the BP patterns of 688 HDP as well as 2050 normotensive pregnancies respectively before 28 gestational weeks, and the repeated measurements and two-way ANOVA was used to decide the significant difference of blood pressure in the same period. The results revealed blood pressure in HDP underwent a mid-pregnancy drop as normal while the drop was unremarkable in advanced-age or obesity pregnancies. Besides, we found blood pressure was significantly higher in patients during first and second trimesters, not just after 20 weeks. In conclusion, our study indicated a significant elevation of blood pressure had appeared before 20 weeks in HDP pregnancies, we should pay more attention to monitoring blood pressure before 20 weeks, especially for advanced age and obese women.
What is already known on this subject? Gestational hypertension, preeclampsia as well as eclampsia were supposed to have the similar pathogenesis and their time of onset was strictly defined after 20 gestational weeks, while the reason for the time point was not clear. On the other hand, higher blood pressure in the first trimester was associated with increasing risk of developing HDP, while the blood pressure(BP) pattern of normal as well as HDP pregnancy was still controversial, especially for the existence of mid-trimester drop.
What do the results of this study add? Firstly, we found blood pressure in HDP underwent a mid-pregnancy drop as normal while the BP drop was unremarkable in advanced-age or obesity pregnancies. Secondly, we noticed the blood pressure in HDP was significantly higher than the normal before 20 weeks, which had not been proved before.
What are the implications of these findings for clinical practice and/or further research? On one hand, both the abnormal elevation of BP and the development of the placenta happened in the first trimester suggested toxic substances caused by the defective placenta played a vital role in the onset and aggravation of HDP, which guides us to pay more attention to monitor blood pressure before 20 weeks, especially for advanced age and obesity pregnancies. On the other hand, our results about BP patterns in HDP help us identify this group of diseases in time which can contribute to a better outcome.
IMPACT STATEMENT
Introduction
Hypertensive disorders of pregnancy (HDP) is a gestation-specific syndrome whose prime clinical manifestation is significant elevation of blood pressure and the essential pathophysiologic of which is generalised vasospasm throughout the body (Kobayashi et al. Citation2001). It endangers about 10% of pregnant women around the world and is one of the leading reasons for maternal mortality (Robert Citation2013). Simultaneously, it has a bad effect on the quality of life seriously for its higher prevalence of caesarean section (Rotem et al. Citation2018) as well as foetal complications such as foetal growth restriction (FGR), preterm delivery even foetal death (Rasmussen and Irgens Citation2003, Hutcheon et al. Citation2011, Spiegler et al. Citation2013). What’s more, the mother who has experienced this disease is more likely to suffer from cardiovascular risks in the following years (Riise et al. Citation2019) and their offspring may get the same experience during pregnancy as well (Kajantie et al. Citation2009). Currently, the defective placenta in the early stage has been proved that played a vital role in the onset and progression of hypertensive disorders of pregnancy, while it is confused to explain the occurrence of postpartum preeclampsia even eclampsia in this way (Matthys et al. Citation2004). There is no effective cure for HDP but termination of pregnancy, as a result, predicting as well as recognizing this group of diseases timely has extraordinary importance for appropriate treatment and better outcomes for both mothers and newborns. Oftentimes, we take into consideration clinical materials, ultrasonographic indexes as well as laboratory parameters during prenatal cares for evaluating the placenta function, predicting the risks of developing preeclampsia, and providing protective drugs such as aspirin (Magee et al. Citation2022). But the study about blood pressure patterns in the first and second trimesters among HDP patients is limited, which can help us identify this disease in the aspect of measurement of blood pressure and understand the pathogenesis from hemodynamic change.
Blood pressure usually means arterial blood pressure, is a vital sign of the body and can be measured in a convenient and non-invasive approach. It is mainly decided by the cardiac output, heart rate, peripheral vascular resistance as well as flexibility of arteries, meanwhile, impressed by heredity factors, lifestyle and weight (Xin et al. Citation2001, Halperin et al. Citation2008, Wang et al. Citation2015). In the body of pregnancy, systemic organs, especially in the cardiovascular system, undergo a successional and adaptive variation of anatomy and physiology to create a high-volume, low-resistance state for foetus growth. And this process is also influenced by gestational hormones, placenta function, prostaglandins as well as the heat produced by the foetus. As a consequence, a regular blood pressure pattern exists throughout the whole pregnancy in normotensive and has a profound effect, especially on the pregnancies underlying cardiovascular disorders. While the blood pressure patterns are still controversial. On one hand, some opinions supported blood pressure, including systolic blood pressure (SBP) and diastolic blood pressure (DBP), experienced a minor decrease in mid-pregnancy (from 18 to 24 weeks) (Landt and Benjamin Citation1936, Page and Christianson Citation1976, Stone et al. Citation1995, Ochsenbein-Kolble et al. Citation2004, Grindheim et al. Citation2012). On the other hand, some scholars held SBP changed little during the pregnancy, while DBP first decreased by 5–10 mmHg from 12 to 26 gestational weeks, afterwards, it returned to the same level as the progestation at 36 weeks (Ayala et al. Citation2000), in other words, some women without a mid-trimester SBP drop still undergone a DBP drop (Salles et al. Citation2015). Although abnormal manifestations like proteinuria, thrombocytopenia and hyperuricaemia could be the first manifestation of HDP and used for assessing the severity, unexpected high blood pressure (SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg) is still the prior diagnostic basis during the pregnancy. More importantly, there is likely to be an obvious difference caused by the toxic substances from the defective placenta between the blood pressure patterns of HDP and normotensive pregnancies, which may help us recognise this disease and assess its progression. Twenty gestational weeks is a critical timing point for diagnosis and classification of HDP as essential or gestational hypertension. The latter further covers gestational hypertension, preeclampsia and eclampsia, which is thought to have a consistent pathogenesis and has a different medical guide during the pregnancy as well as after the delivery compared to the essential hypertension. What is strikingly noticeable is higher blood pressure in the first trimester is associated with an increased risk of developing HDP even preterm birth (Rang et al. Citation2004, Zhang et al. Citation2006, Magnussen et al. Citation2007, Cnossen et al. Citation2008, Akolekar et al. Citation2011, Poon et al. Citation2011). Besides, a case of HDP that developed at 9 weeks attracted our attention (Hayashi et al. Citation2021). In this study, we attempt to differentiate blood pressure patterns in the first and second trimesters of HDP from the normal, which can help us to identify it timely. In addition, we want to investigate whether 20 weeks is the original time when the significant high blood pressure appears, or high blood pressure has happened before 20 weeks but has not been noticed because the value does not reach the standard. That may help us understand development of HDP and guide us to monitor the blood pressure during pregnancy more effectively.
Materials and methods
Objects and data collection
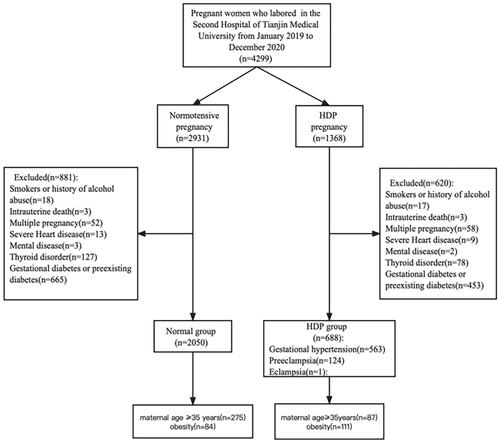
This study included the 4299 pregnancies who laboured in the Second Hospital of Tianjin Medical University from January 2019 to December 2020. In Tianjin, pregnancies usually got their prenatal cares in the local community health service centre before 28 weeks of gestation and the materials such as gestational age, weight and blood pressure values were uploaded and recorded in the website: Tianjin Maternal and Child Health Care Information System (60.29.92.68:82/Site/NewTjsfezxSite/Default.aspx), and into the third trimester, they chose their preferred hospital to continue their visits until delivery. In-hospital materials including maternal age, blood pressure values of delivery, gender, length and weight of offspring were recorded in the In-patient Management Information System. Considering that most mothers experienced the first prenatal care and created the pregnancy file during 8 + 0 weeks to 10 + 6 weeks and the last care they got in the local centre is around 28 + 0 weeks. So we chose seven average time periods (8 + 0 weeks to 10 + 6 weeks, 11 + 0 weeks to 13 + 6 weeks, 14 + 0 weeks to 16 + 6 weeks, 17 + 0 weeks to 19 + 6 weeks, 20 + 0 weeks to 22 + 6 weeks, 23 + 0 weeks to 25 + 6 weeks, 26 + 0 weeks to 28 + 6 weeks) to represent the first and second trimester. The electronic sphygmomanometer (arm or wrist) was used for measuring blood pressure. Pregnancies were in a sitting position and asked to rest for 5–10 min before measurement. Our data came from the two systems and this study had been reviewed and approved by the Ethics Committee.
Inclusion and exclusion criteria
The diagnosis of HDP depended on the guide of ISSHP (Brown et al. Citation2018). Pregnancies with multiple pregnancies, gestational diabetes mellitus or pregestational diabetes mellitus, thyroid dysfunction, severe cardiovascular disease, smoking and drinking story, or stillbirth were excluded from our study. We further excluded chronic hypertension and preeclampsia superimposed upon chronic hypertension for their influence on blood pressure in the first and the second trimesters. 35 years old was the definition for advanced-age women. BMI (body mass index) ≥28 kg/m2 was regarded as obesity in our study (Zhou Citation2002). The flow chart of the study is shown in .
Figure 1. Flow chart of the study.
Statistical analyses
SPSS 21.0 was used for data processing. Measurement data were expressed as mean ± standard deviation and enumeration data was expressed as a percentage. For measurement data which was in accord with normal distribution and homoscedasticity, T-test was used for analysing; For heterogeneity of variance, we used an approximate T-test. For data against normal distribution, we chose the Rank sum test. The repeated measurements and 2-way ANOVA was used to observe the blood pressure variation as the gestational age increased and decided the significant difference in the same period between the normal and HDP group. For the date which was not meet the Sphericity assumption, we used Greenhouse-Geisser test. Finally, we used Chi-square test for the analysis of categorical variable data. P < 0.05 is the standard for a significant difference.
Results
Comparison of baseline and delivery characteristics between HDP and the normal group
Compared with the normotensive pregnancy, the maternal age, BMI, rate of unipara, education level, Apgar 5 min score, gestational weight gain as well as the rate of caesarean section in HDP group had a significant difference, while Apgar 1 min as well as 10 min, rate of a baby boy, weight and height of infants from HDP had no significant difference (Shown in ).
Table 1. Baseline and delivery characteristics of normal and HDP group.
Blood pressure patterns of HDP and the normal
The results were shown in and , and . Mauchly’s W = 0.56, p < .05 in SBP and Mauchly’s W = 0.45, p < .05 in DBP.
Figure 2. Blood pressure patterns during the pregnancy.
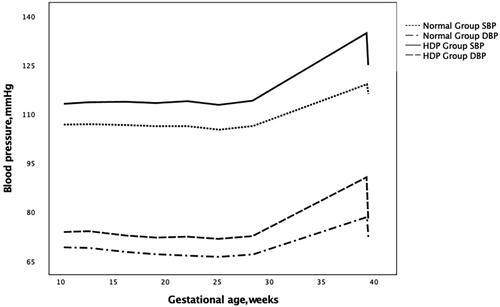
Table 2. Blood pressure in different gestational age.
Table 3. Blood pressure patterns during the pregnancy.
Comparison of blood pressure value in the same period of pregnancy
The compared gestational age had no significant difference between and HDP group (p>.05), while blood pressure was always higher in HDP group throughout the pregnancy (shown in ).
Influence on blood pressure patterns from advance age and obesity
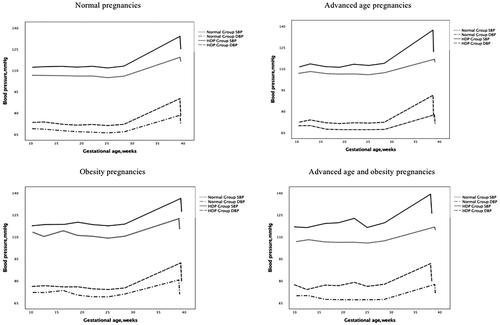
The results are shown in .
Figure 3. Influences from advanced age and obesity on blood pressure patterns.
Discussion
During pregnancy, every organ, especially the cardiovascular system, experiences a successional variation to adapt to the growing uterus and provide enough blood supply and nutrition to the foetal. This process is affected by the hormones from the placenta as well as the foetus at the same time. As a vital parameter of the cardiovascular system, blood pressure also shows its characteristic changing pattern as the gestational age increases. While in the body of hypertensive disorders of pregnancy, influenced by the toxic substances which result from the hypoxic-ischaemic placenta and promote the abnormal elevation of blood pressure, the blood pressure pattern can be different. Now many maternal blood proteins like PLGF, sFlt-1, sEng, PPAP-A can help us predict the risks of HDP effectively (Maynard et al. Citation2003, Chaiworapongsa et al. Citation2004, Venkatesha et al. Citation2006, Tarca et al. Citation2022), but the study about blood pressure pattern in patients is limited. So we aim to find out the pattern which can help us recognise this disease in the aspect of monitoring blood pressure.
Firstly, irrespective of the influence of age and BMI, the normal pregnancies and the patients experienced a similar blood pressure pattern in the first and second trimesters. The systolic blood pressure changed little from 8 + 0 weeks to 22 + 6 weeks, after which it decreased slightly and got the bottom from 23 + 0 to 25 + 6 weeks, then it increased progressively until the admission. Similarly, three types of research have proved that both normal and hypertensive pregnancies experienced SBP drop during the second trimester (Hare Citation1929, Landt and Benjamin Citation1936, Macdonald-Wallis et al. Citation2012). This pattern was decided by a combination of many factors. Specifically speaking, stroke volume, which is mainly influenced by the blood volume, and heart rate average increase by 35% and 15–17% respectively, accordingly, systemic vascular resistance decreases by 15–21% as the gestational age increases. At the same time, the process is affected by some hormones from the placenta and foetal like progestin and prostaglandins which can promote the metabolism of water and sodium (Solano and Arck Citation2019). As a result, the SBP decreases slightly at the end of the second trimester as a sign of normal compensation for the cardiovascular system (Abbas et al. Citation2005). Our results about DBP pattern in normal were consistent with a previous study which included 1112 pregnancies and described the relationship between gestational weight gain (GWG) and blood pressure patterns in normal (Lei et al. Citation2017). However, when we compared the DBP patterns between normal and HDP, what attracted us most is that the period when the DBP decreased before 20 weeks in HDP was shorter than normal. The reason we support this is the spasm condition of vessels in patients. It not only increases vascular resistance but also damages its resilience, expansivity as well as endocrine function, which mainly influences the DBP. This difference can help us identify the patients timely by describing the patterns of blood pressure.
Secondly, we wanted to examine the influence of advanced age and obesity on blood pressure patterns. As a consequence, we noticed there is no obvious drop in blood pressure presenting in the second trimester of advanced age or obesity pregnancies. Some scholars thought the absence of blood pressure drop may be associated with endothelial dysfunction (Silva et al. Citation2008), and this dysfunction can be aggravated by increasing age as well as overweight. Concretely speaking, the macrophage in adipose tissue of obesity is more than the ordinary, then activatory macrophage can release some inflammatory factors like IF-1β, IF-6, and TNF-α as well as chemokines which can exacerbate the endothelial dysfunction (Lumeng et al. Citation2007). On the other hand, in advance-age pregnancy, worse vessel elasticity and hypoperfusion (Lowe Citation2008) combined with excessive inflammation and insulin resistance which is relevant to dysfunctional endothelium as well as increasing endothelin-1(Walsh Citation2007, Mutter and Karumanchi Citation2008), jointly aggravate the progression of the disease. Therefore we should pay more attention to monitoring blood pressure of advanced age and obesity pregnancies.
Besides the findings about blood pressure patterns during pregnancy, another important result we got in this study was the time when the abnormal elevation of blood pressure occurred in patients. As we all know, for mothers who do not have risk factors for potential hypertension and record their blood pressure values at home, monitoring the blood pressure during each prenatal care is a very vital method to learn their blood pressure level. While the frequency of prenatal care that a mother gets in the first and second trimesters is far less than in the third trimester. Moreover, the definition of HDP makes us pay more attention to the blood pressure after 20 gestational weeks. While our findings indicated that abnormal elevation of blood pressure had existed before 20 weeks. We speculate this phenomenon is related to the dysfunctional placenta, an affiliated structure which derived as early as the embryo. Placenta, as the largest and the first foetal organ to develop, plays a central role in maternal and foetal health. It originates from the trophectoderm, which forms at ∼5 days post fertilisation (dsf). After the process of the primary villi, second villi (14 dsf) and third villi(21 dsf), the blueprint of the placenta has been finished by the end of the first trimester (Turco and Moffett Citation2019). With the help of sufficient remodelling, the vessel lumen of the uterine spiral artery enlarges to supply enough blood for the foetus's growth. While in the body of HDP, superficial implantation and incomplete remodelling make the placenta in a condition of hypoxic and ischaemic. Then abnormal placenta releases a large number of toxic substances into maternal serum, generalised vasospasm and high resistance of peripheral vascular results in elevation of blood pressure as well as other clinical manifestations like proteinuria and blurred vision (Romero Citation2008, Chaiworapongsa et al. Citation2014). Blood pressure decreases quickly after delivery of the placenta further proves this as well. In short, we should monitor the blood pressure more frequently in the first and second trimesters.
There are several deficiencies in our study. Firstly, we lack the blood pressure values during the third trimester which can help us describe the complete blood pressure pattern of pregnancy. Secondly, we should also take into consideration some factors which may affect the blood pressure value like the use of antihypertensive drugs or GWG. Thirdly, more experiments about serum indices are needed to perform in the future in order to fix why the extra rise of blood pressure appears in the second trimester for advanced age and obesity pregnancy.
Above all, blood pressure patterns in the first and second trimesters of HDP had a similar character as the normal, they both underwent a first decrease during the mid-pregnancy and then increased progressively until delivery. On the other hand, the blood pressure was always significantly higher in HDP throughout the pregnancy, not just after 20 weeks, which proved the unreasonable spasm condition of vessels had developed in the early stage, so it was very important for us to monitor the blood pressure more frequently before 20 weeks.
Acknowledgments
We gratefully acknowledge all the staff of Community Health Centers who provided us with the materials as well as the technicians who worked for the Tianjin Maternal and Child Health Care Information System.
Disclosure statement
All authors declare they have no financial or competing interests.
Additional information
Funding
References
- Abbas, A.E., Lester, S.J. and Connolly, H., 2005. Pregnancy and the cardiovascular system. International Journal of Cardiology, 98 (2), 179–189.
- Akolekar, R., et al., 2011. Prediction of early, intermediate and late pre-eclampsia from maternal factors, biophysical and biochemical markers at 11-13 weeks. Prenatal Diagnosis, 31 (8), 832–832.
- Ayala, D.E., et al., 2000. Blood pressure patterns in normal pregnancy, gestational hypertension, and preeclampsia. Journal of Hypertension, 18, S53–S54.
- Brown, M.A., et al., 2018. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis, and management recommendations for international practice. Pregnancy Hypertension, 13, 291–310.,
- Chaiworapongsa, T., et al., 2004. Evidence supporting a role for blockade of the vascular endothelial growth factor system in the pathophysiology of preeclampsia-Young Investigator Award. American Journal of Obstetrics and Gynecology, 190 (6), 1541–1547.
- Chaiworapongsa, T., et al., 2014. Pre-eclampsia part 1: current understanding of its pathophysiology. Nature Reviews Nephrology, 10 (8), 466–480.
- Cnossen, J.S., et al., 2008. Accuracy of mean arterial pressure and blood pressure measurements in predicting pre-eclampsia: systematic review and meta-analysis. BMJ (Clinical Research ed.), 336 (7653), 1117–1120.
- Grindheim, G., et al., 2012. Changes in blood pressure during healthy pregnancy: a longitudinal cohort study. Journal of Hypertension, 30 (2), 342–350.
- Halperin, R.O., Gaziano, J.M. and Sesso, H.D., 2008. Smoking and the risk of incident hypertension in middle-aged and older men. American Journal of Hypertension, 21 (2), 148–152.
- Hare, D.C., 1929. An investigation of blood pressure, pulse rate and the response to exercise during normal pregnancy and some observations during confinement. Quarterly Journal of Medicine, 22 (1929), 381–404.
- Hayashi, S., et al., 2021. A case of hypertensive disorders of pregnancy that developed at 9weeks of gestation. CEN Case Reports, 10 (4), 476–482.
- Hutcheon, J.A., Lisonkova, S. and Joseph, K.S., 2011. Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Best Practice & Research. Clinical Obstetrics & Gynaecology, 25 (4), 391–403.
- Kajantie, E., et al., 2009. Pre-eclampsia is associated with increased risk of stroke in the adult offspring the Helsinki Birth Cohort Study. Stroke, 40 (4), 1176–1180.
- Kobayashi, T., et al., 2001. Vasospasms are characteristic in cases with eclampsia/preeclampsia and HELLP syndrome: Proposal of an angiospastic syndrome of pregnancy. Seminars in Thrombosis and Hemostasis, 27 (2), 131–135.
- Landt, H. and Benjamin, J.E., 1936. Cardiodynamic and electrocardiographic changes in normal pregnancy. American Heart Journal, 12 (5), 592–607.
- Lei, Q., et al., 2017. Trimester-specific weight gain and mid pregnancy diastolic blood pressure rebound during normotensive pregnancy. Hypertension, 70 (4), 804–812.
- Lowe, S., 2008. Guidelines for the management of hypertensive disorders of pregnancy 2008: the Australian and New Zealand perspective. Hypertension in Pregnancy, 27 (4), 543–543.
- Lumeng, C.N., Bodzin, J.L. and Saltiel, A.R., 2007. Obesity induces a phenotypic switch in adipose tissue macrophage polarization. The Journal of Clinical Investigation, 117 (1), 175–184.
- macdonald-Wallis, C., et al., 2012. Blood pressure change in normotensive, gestational hypertensive, preeclamptic, and essential hypertensive pregnancies. Hypertension, 59 (6), 1241–1248.
- Magee, L.A., Nicolaides, K.H. and von Dadelszen, P., 2022. Preeclampsia. Obstetrical & Gynecological Survey, 77 (11), 641–643.
- Magnussen, E.B., et al., 2007. Prepregnancy cardiovascular risk factors as predictors of pre-eclampsia: population based cohort study. BMJ, 335 (7627), 978–981.
- Matthys, L.A., et al., 2004. Delayed postpartum preeclampsia: an experience of 151 cases. American journal of Obstetrics and Gynecology, 190 (5), 1464–1466.
- Maynard, S.E., et al., 2003. Excess placental soluble FMS-like tyrosine kinase 1(sFlt1) may contribute to endothelial dysfunction, hypertension, and proteinuria in preeclampsia. The Journal of Clinical Investigation, 111 (5), 649–658.
- Mutter, W.P. and Karumanchi, S.A., 2008. Molecular mechanisms of preeclampsia. Microvascular Research, 75 (1), 1–8.
- Ochsenbein-Kolble, N., et al., 2004. Cross sectional study of automated blood pressure measurements throughout pregnancy. BJOG: An International Journal of Obstetrics and Gynaecology, 111 (4), 319–325.
- Page, E.W. and Christianson, R., 1976. Impact of mean arterial-pressure in middle trimester upon the outcome of pregnancy. American Journal of Obstetrics and Gynecology, 125 (6), 740–745.
- Poon, L.C.Y., et al., 2011. Hypertensive disorders in pregnancy: screening by systolic diastolic and mean arterial pressure at 11–13 weeks. Hypertension in Pregnancy, 30 (1), 93–107.
- Rang, S., et al., 2004. Serial assessment of cardiovascular control shows early signs of developing pre-eclampsia. Journal of Hypertension, 22 (2), 369–376.
- Rasmussen, S. and Irgens, L.M., 2003. Fetal growth and body proportion in preeclampsia. Obstetrics and Gynecology, 101 (3), 575–583.
- Riise, H.K.R., et al., 2019. Hypertensive pregnancy disorders increase the risk of maternal cardiovascular disease after adjustment for cardiovascular risk factors. International journal of Cardiology, 282, 81–87.
- Robert, J.M., 2013. Hypertension in pregnancy of the American College of Obstetricians and Gynecologists’ task force on hypertension in pregnancy. Obstetrics and Gynecology, 122 (5), 1122–1131.
- Romero, R., 2008. A longitudinal study of angiogenic (placental growth factor) and anti-angiogenic (soluble endoglin and soluble vascular endothelial growth factor receptor-1) factors in normal pregnancy and patients destined to develop preeclampsia and deliver a small for gestational age neonate. Journal of Maternal-Fetal & Neonatal Medicine, 21 (1), 9–U3.
- Rotem, R., et al., 2018. Association between hypertensive disorders of pregnancy and third stage of labor placental complications. Pregnancy hypertension, 13, 166–170.
- Salles, G.F., et al., 2015. Blood pressure in healthy pregnancy and factors associated with no mid-trimester blood pressure drop: a prospective cohort study. American Journal of Hypertension, 28 (5), 680–689.
- Silva, L.M., et al., 2008. No mid pregnancy fall in diastolic blood pressure in women with a low educational level: the generation R study. Hypertension, 52 (4), 645–651.
- Solano, M.E. and Arck, P.C., 2019. Steroids, pregnancy and fetal development. Frontiers in Immunology, 10 (3017), 3017.
- Spiegler, J., et al., 2013. Pregnancy risk factors for very premature delivery: what role do hypertension, obesity and diabetes play? Archives of Gynecology and Obstetrics, 288 (1), 57–64.
- Stone, P., et al., 1995. Measurements of blood pressure, edema and proteinuria in a pregnant population of New Zealand. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 35 (1), 32–37.
- Tarca, A.L., et al., 2022. Prediction of preeclampsia throughout gestation with maternal characteristics and biophysical and biochemical markers: a longitudinal study. American Journal of Obstetrics and Gynecology, 226 (1), 126.e1-126–e22.
- Turco, M.Y. and Moffett, A., 2019. Development of the human placenta. Development, 146 (22), dev163428.
- Venkatesha, S., et al., 2006. Soluble endoglin contributes to the pathogenesis of preeclampsia. Nature Medicine, 12 (7), 862–862.
- Walsh, S.W., 2007. Obesity: a risk factor for preeclampsia. Trends in Endocrinology and Metabolism, 18 (10), 365–370.
- Wang, Z., et al., 2015. Association of visceral and total body fat with hypertension and prehypertension in a middle-aged Chinese population. Journal of Hypertension, 33 (8), 1555–1562.
- Xin, X., et al., 2001. Effects of alcohol reduction on blood pressure – a meta-analysis of randomized controlled trials. Hypertension, 38 (5), 1112–1117.
- Zhang, J., et al., 2006. Blood pressure dynamics during pregnancy and spontaneous preterm birth. American Journal of Obstetrics and Gynecology, 195 (6), S79.
- Zhou, B.F., 2002. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese Adults: study on optimal cut-off points of body mass index and waist circumference in Chinese Adults. Asia Pacific Journal of Clinical Nutrition, 11, S685–S693.