

Abstract
The aim was to assess the achievement by self-determined goals in pelvic organ prolapse (POP) participants receiving pelvic floor muscle training (PFMT) compared to vaginal pessary. Forty participants with POP stage II to III were randomly allocated to pessary or PFMT. Participants were asked to list up 3 goals they expected from treatment. Thai version of Prolapse Quality of Life Questionnaire (P-QOL) and Pelvic Organ Prolapse Incontinence Sexual Questionnaire, IUGA-revised (PISQ-IR) were completed at 0 and 6-week period. At 6-week post-treatment, they were asked if their goals had been achieved. The totally achieved goals in the vaginal pessary group were 70% (14/20) significantly higher than PFMT group at 30% (6/20) (p = 0.01). The mean ± SD of the post-treatment P-QOL score in the vaginal pessary group was significantly lower than the PFMT group (13.90 ± 10.83 vs 22.04 ± 5.93, p = 0.01), but not different in all PISQ-IR subscales. Pessary treatment for POP yielded better total goal achievements and better quality of life than PFMT for POP treatment at a 6-week follow-up.
What is already known on this subject? Pelvic organ prolapse (POP) can severely affect the quality of life, causing physical, social, psychological, occupational, and/or sexual dysfunction. Individual patient goal setting and goal achievement scaling (GAS) offers a new method of patient-reported outcome measurement (PRO) in therapeutic success such as pessary or surgery in patient with POP. But there is no randomised controlled trial comparing pessary vs pelvic floor muscle training (PFMT) using GAS as the outcome measurement.
What do the results of this study add? The results showed that women with POP stage II to III who received vaginal pessary had higher totally goal achievements and better quality of life than the women received the PFMT at 6-week follow up.
What are the implications of these findings for clinical practice and/or further research? The information about the better goal achievements by using pessary can be used as the tools for counselling for patients with POP for selecting the choices for the treatment in the clinical setting.
Impact statement
Brief summary
POP stage II to III patients treatedwith vaginal pessary had higher totally goal achievements and better quality of life than treated by PFMT.
Introduction
Pelvic organ prolapse (POP) is a common, non-life-threatening and major distressing condition affecting up to 30% of the women (Aytan et al Citation2014). The incidence of urogenital prolapse increases with advancing age and can severely affect the quality of life, causing physical, social, psychological, occupational, and/or sexual dysfunction There was evidence that sexual functions that deteriorated by pelvic organ prolapse improved after prolapse treatment (Obut et al. 2018). Nowadays there are trends of fertility sparing surgery treatment or uterus transplantation which can increase the incidence of POP (Giampaolino et al., Citation2022; Gullo et al., Citation2022; Tanos, et al. Citation2022). It has been reported that 50% of parous women lose pelvic floor support leading to development of prolapse, However, only about 20% are presented with symptoms (Barber et al. Citation2009; Barber and Maher, Citation2013). The paradigm of outcomes measurement in pelvic organ prolapse treatment has shifted from solely relying upon anatomical and functional outcomes to a more patient-oriented measurement (Hullfish, et al, Citation2002).
Individual patient goal setting and goal achievement scaling (GAS) offers a new method of patient-reported outcome measurement (PRO) in therapeutic success. The role of this method to assess treatment outcomes is gradually evolving. GAS has been extensively used widely in other fields of treatment such as rehabilitation services and geriatric medicine, supporting the assertion that goals are best defined according to patients’ unique problems which might be overlooked by standardised instruments (Turner-Stokes, Citation2009; Turner-Stokes et al., Citation2020; Witjes et al., Citation2019).
Studies with both short and long-term follow-ups have investigated the use of GAS to evaluate the success of pelvic floor treatment. Based on previously published work, GAS is well suited to evaluate pelvic organ prolapses treatment such as vaginal pessary treatment and surgical treatment in the urogynecology field (Elkadry et al. Citation2003; Komesu et al. Citation2008). Women who attain self-determined goals are likely to continue pessary use (Komesu et al. Citation2008). Nevertheless, a direct comparison of patient-reported goal achievement between pelvic floor muscle training (PFMT) and vaginal pessary in a randomised controlled trial study is still lacking. As a result, the aim of the study was to assess the achievement of patient-reported goal achievements in POP participants receiving pelvic floor muscle training compared to vaginal pessary as a treatment of POP, to understand what patients genuinely hoped to achieve from both treatments. The patient-reported goal achievement results from this study might be useful for patient counselling and contribute additional information to the current literature.
Materials and methods
Design and setting
This was a randomised controlled trial performed in the urogynecology clinic at King Chulalongkorn Memorial Hospital, Bangkok, Thailand. Study was conducted between May 2020 and April 2021. The trial was registered in the Thai Clinical Trials Registry (http://www.thaiclinicaltrials.org, identifier TCTR20191229002) and was approved by the Research Ethics Committee of the Faculty of Medicine, Chulalongkorn University on 23 April 2020, (COA No.482/2020). All participants gave written informed consent.
Study protocol
Participants with pelvic organ prolapse stage II to III according to the Pelvic Organ Prolapse Quantification System (POP-Q) were recruited. Participants were excluded if they had a history of silicone allergy, unable to perform pelvic floor muscle training, unable to take care or seek assistance in vaginal pessary care, cognitive impairment, or inability to understand research protocol. The degree of prolapse was measured prior to randomisation using the Pelvic Organ Prolapse Quantification (POP-Q) system. All participants were evaluated if theyare able to correctly perform PFMT and were able to be fitted by vaginal pessary prior to allocation. Participants who were candidates for both treatments were considered eligible for the trial.
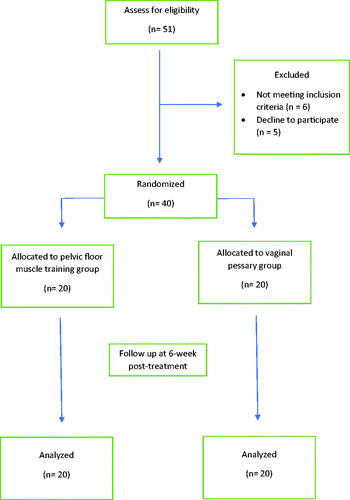
Eligible participants were randomised according to the CONSORT guideline (Schulz et al. Citation2010) with the flowchart (). They were randomly allocated to pessary treatment or PFMT in a 1:1 ratio using an external computer system. Block of 4 randomisation was used. Allocation concealment of the codes was kept in opaque, sealed envelopes and was opened by the research assistance prior to initiating treatment. It was not possible to blind participants to the treatment because of the nature of the intervention.
Figure 1. CONSORT Diagram.
Demographic data and medical history of all participants including age, parity, age at menopause, type of delivery, history of hormonal treatment and sexual activity were collected.
Eligible participants were asked to list 3 goals they expected from POP treatment and ranked them in order of importance. Goals were divided into ten categories; bladder, bowel, prolapse, pain-related, sexual, physical function, social relationships, emotional, combined goal and other goals. Two investigators categorised patients 'goals. When there was disagreement in categorisation, the two investigators reached a consensus. Thai version of Prolapse Quality of Life Questionnaire (P-QOL) (Manchana and Bunyavejchevin, Citation2010) and Pelvic Organ Prolapse Incontinence Sexual Questionnaire, IUGA-revised (PISQ-IR) (Bunyavejchevin and Ruanphoo Citation2022) were provided at first visit for the participants to complete before initiating treatment and at 6-week after. History taking and physical examination on POP patients were conducted by a research physician. All participants were scheduled for 2 visits with a 2-week and 6-week after initiating treatment.
The list of goals was provided to patients at 6-week post-treatment and they were asked to respond whether each pre-treatment goal had been achieved. Subjects who answered ‘yes’ to the statement, ‘My expectation has been met’, in all 3 goals, were classified as ‘Totally achieved goals’ while subjects who answered ‘no’ in 1 or 2 of the goals were classified ‘Partially achieved goals’ and subjected who answered ‘no’ to all goals were classified as ‘No goals achieved’ Degree of achievement was also evaluated by the patient on the VAS scale from 0 to 10, which 10 represented completely achieved the goals and 0 represented not achieved the goals at all. Also, Thai version of P-QOL (Manchana and Bunyavejchevin Citation2010) and PISQ-IR (Bunyavejchevin and Ruanphoo Citation2022) were provided at 6-week post-treatment.
Outcome measurement
Primary outcome was the proportion of the participants who totally achieved all 3 goals in the vaginal pessary group versus PFMT group. Secondary outcomes were to compare the proportion of partially achieved goals and no goals achieved participants between both groups, degree of achievement measured by Visual Analogue Scale (VAS) and the difference in post-treatment P-QOL and PISQ-IR score in both groups.
Pelvic floor muscle training
Participants allocated to PFMT started with an explanation of the function of the pelvic floor, given and supervised by the first author (W.L.). the pelvic floor muscle function and the ability to contract and relax the pelvic floor muscles correctly was examined using digital palpation. Participants who were unable to contract their pelvic floor muscles were instructed. They received comments as they correctly performed the PFMT using the digital examination. As soon as they were able to control their pelvic floor, they started the training by doing exercises at home and during each visit (at least 2 times a week). The protocol of PFMT followed the International urogynecology association (IUGA) recommendation (Association I.U Citation2022) consisted of practicing the exercises twice a week, 3 sets of 8-12 maximal contractions, 3 times a day. Number of sessions was recorded for each participant. All participants were scheduled at a 2-week and 6-week after initiating treatment. The digital examination was done at each follow up visit to check whether the participants can contract the muscle correctly and re-educated and remind them for the PFMT technique.
Pessary treatment
Pessaries were fitted by the first author (W.L.). All pessaries were made of silicone (MedGyn, Addison, IL). The type of vaginal pessary consisted of ring pessary with or without support and Gellhorn pessary.
Vaginal pessary was considered to have the correct size when the physician could place a finger between the pessary and the vaginal wall, the prolapse was reduced to above the hymen, the patient felt comfortable, and the pessary was retained during a Valsalva manoeuvre and coughing in both supine and standing positions. Pessary treatment was evaluated after 2 weeks. Participants in whom the pessary fell out or who experienced discomfort within the first 2 weeks were refitted with a different type or size of pessary and reviewed again after 2 weeks. If a pessary was not fitted successfully, pessary fitting was regarded as unsuccessful. All participants were scheduled at 6-week to evaluate the treatment and monitor side effects and completed the questionnaires.
Prolapse Quality of Life questionnaire (P-QOL)
The P-QOL questionnaire includes 20 questions in nine domains: general health perceptions, prolapse impact, role limitations, physical limitations, social limitations, personal relationships, emotional problem, sleep or energy disturbance, and measurement of symptom severity. A four-point grading system for each item is used except for the first question about general health which has five points. The total score in each domain is transformed into a range between 0 and 100. A higher score indicates a greater impairment on the quality of life, but a lower score indicates a better quality of life. P-QOL questionnaire has been validated and translated to Thai version (Manchana and Bunyavejchevin Citation2010).
Pelvic Organ prolapse Incontinence Sexual questionnaire, IUGA-revised (PISQ-IR)
The PISQ-IR is designed as a condition-specific measure of sexual function in women with pelvic floor dysfunction, including urinary and anal incontinence and pelvic organ prolapse
PISQ-IR scale is composed of six sub-scales in sexually active women and four in women who are not sexually active. Each sub-scale measures a different dimension of sexual function, consisting of
Not sexually active: partner-related (NSA-PR) dimension
Not sexually active: condition-specific (NSA- CS) dimension
Not sexually active: global quality rating of sexual quality (NSA-GQ) dimension
Not sexually active: condition impact on sexual quality (NSA-CI) dimension
Sexually active: assessment of arousal, orgasm (SA-AO) dimension
Sexually active: assessment of partner-related impacts (SA-PR) dimension
Sexually active: assessment of condition-specific impactson activity (SA-CS) dimension
Sexually active: assessment of sexual desire (SA-D)
Sexually active: global quality rating of sexual quality (SA-GQ) dimension
Sexually active: condition-specific impact on sexual quality (SA-CI) dimension
PISQ-IR questionnaire also has been validated and translated to Thai version (Bunyavejchevin and Ruanphoo Citation2022).
For scoring system, we used transformed summation method which is the most common conversion of scores to a ‘normed metric,’ generally ranging from 0 to 100. (0 = worst, 50 = middle and 100 = best). We presented the transformed summation in sub-scale due to the consideration of the underlying principles of multi-dimensional scaling used to develop the PISQ-IR score so that the PISQ-IR overall summation was not to be calculated (Rockwood et al. Citation2013).
Statistical analysis
For statistical analysis, baseline characteristics, categorical data were presented as number and percentage. Continuous data were presented as mean and standard deviation or median and interquartile range as appropriate. Intention-to-treat (ITT) analysis was used for primary outcome. To compare pre and post treatment outcome, paired t-test or Wilcoxson sign rank test was used for continuous data. To compare outcome between groups, continuous data were analysed using unpaired t-test or Mann-Whitney U test and categorical data were analysed using chi-square, Statistical analysis was performed using SPSS version 25.
The previous survey of totally goal achievement in POP patients undergoing PFMT at King Chulalongkorn Memorial Hospital showed totally achieved goals at 30%, while totally goal achievement in the vaginal pessary group is approximately 85% (n = 15), consistent with the study by Sung et al ( et al. Citation2016). With alpha level equal to 0.05, and a 30% lost to follow-up rate, forty patients were required.
Results
Forty participants were randomised and allocated to vaginal pessary and pelvic floor muscle training groups. The mean ± SD of age of the participants in the vaginal pessary group and the pelvic floor muscle training group was 68.80 ± 6.40 and 65.70 ± 9.89 years. Patient characteristics in the vaginal pessary and pelvic floor muscle training groups did not differ in age, age at menopause, body mass index (BMI), parity, menopausal status, stage of POP, history of hormonal use, sexual activity or pre-treatment P-QOL and PISQ-IR score ().
Table 1. Demographic data and baseline characteristics (N = 40).
There was no difference in the pre-treatment goals between the vaginal pessary group and PFMT (). The totally achieved goals in vaginal pessary group were 70% (14/20) significantly higher than the pelvic floor muscle training group at 30% (6/20) (). The mean ± SD of the degree of achievement by VAS in vaginal pessary group was significantly higher than the PFMT group (6.60 ± 3.09 vs 3.10 ± 2.09, p < 0.01).
Table 2. Distribution of the 3-ranked pre-treatment goals and the numbers of goals achieved in vaginal pessary group and PFMT group (N = 40).
The post-treatment P-QOL score in the vaginal pessary group was significantly lower than the PFMT group, representing improvement in quality of life. There was no statistically significant difference in all PISQ-IR subscales between the groups ().
Table 3. P-QOL and PISQ-IR score at 6 weeks after treatment (N = 40).
Discussion
The Self-Assessment Goal Achievement (SAGA) has been developed as a novel method in many disciplines to evaluate the successful of the treatment from the patients’perspective (Elkadry et al. Citation2003; Hullfish et al. Citation2002; Komesu et al. Citation2008). In our study, we found that participants who totally achieved their goals in the vaginal pessary group were significantly higher than the PFMT group. Our findings were consistent with Komesu et al (Komesu et al. Citation2008) finding which overall goal achievement in vaginal pessary users were as high as 74%. This may be explained by the vaginal pessary offers prompt reduction of the pelvic organ prolapse and restoration of normal anatomy which found to be significantly correlated with quality of life improvement and goal achievement by Srikrishna et al Citation2008). P-QOL score in the vaginal pessary group were also improved significantly. On the contrary, the patients who received PFMT as the treatment usually required longer time for the PFMT to reach its maximal potential. There were reports in improvements of urinary and POP symptoms beginning as early as 3 to 6 weeks after PFMT (Association I U, Citation2022; García-Sánchez et al. Citation2019). In addition, there are several factors that might have influenced the outcome of PFMT, such as age of the participants, baseline pelvic floor muscle strength, and body mass index (BMI)(García-Sánchez et al. Citation2019) which may vary between individuals and affect the outcome of the PFMT. Milne et al ( 2009) reported low rate of overall goal achievement at 20% by the patients with urinary incontinence undergoing PFMT. We also found that P-QOL score were not significantly improved in the PFMT group. Regarding the PISQ-IR, we found no difference in the PISQ-IR score in all subscales between groups. This may be due to low incidence of sexually active women in our study. Only 15% in the PFMT group and 10% in the vaginal pessary group were sexually active.
The information about the better goal achievements by using pessary can be used as the tools for counselling for patients with POP for selecting the choices for the treatment in the clinical setting.
Strength of the study
To our knowledge, this is the first randomised controlled trial comparing the two treatments (Vaginal pessary vs PFMT) using the SAGA as an outcome measurement in pelvic organ prolapse patients. We controlled and recruited only the women who were eligible for a vaginal pessary and able to correctly perform PFMT. Also, the standardised questionnaires such as P-QOL and PISQ-IR were used in the study. Lastly, we followed the standard protocol of PFMT suggested by IUGA(Association I U Citation2022).
Limitation of the study
We follow the patients at 6-week after treatment. Thus, the study with long term follow up are advocated. Blinding the participants to their treatment groups were not possible due to the nature of the intervention.
Conclusion
The patients with POP stage II to III who received vaginal pessary treatment showed higher totally goal achievements and better quality of life than the women who received the PFMT at 6 weeks follow up.
Author’s contributions
Limbutara W: Project development, Data collection, manuscript preparation and writing
Bunyavejchevin S: Project development, manuscript preparation and writing
Ruanphoo P: Project development, Data collection, and data analysis
Chiengthong K: Project development, Data collection, and data analysis
Disclosure statement
The authors declared no conflict of interest.
Additional information
Funding
References
- Association, I. U. 2022. Pelvic floor exercise. A guide for women. Retrieved from https://www.yourpelvicfloor.org/media/Pelvic_Floor_Exercises_RV2-1.pdf
- Aytan, H., et al., 2014. Prevalence of pelvic organ prolapse and related factors in a general female population. Turkish Journal of Obstetrics and Gynecology, 11 (3), 176–180.
- Barber, M. D., et al., 2009. Defining success after surgery for pelvic organ prolapse. Obstetrics and Gynecology, 114 (3), 600–609.
- Barber, M. D. and Maher, C., 2013. Epidemiology and outcome assessment of pelvic organ prolapse. International Urogynecology Journal, 24 (11), 1783–1790.
- Bunyavejchevin, S. and Ruanphoo, P., 2022. Thai translation and validation of the pelvic organ prolapse/urinary incontinence sexual questionnaire, IUGA-Revised (PISQ-IR) and pelvic floor distress inventory (PFDI-20). International Urogynecology Journal, 33 (11), 3137–3142.
- Elkadry, E. A., et al., 2003. Patient-selected goals: a new perspective on surgical outcome. American Journal of Obstetrics and Gynecology, 189 (6), 1551–1557. discussion 1557–1558.
- García-Sánchez, E., et al., 2019. What pelvic floor muscle training load is optimal in minimizing urine loss in women with stress urinary incontinence? A systematic review and meta-analysis. International Journal of Environmental Research and Public Health, 16 (22), 4358–4372.
- Giampaolino, P., et al., 2022. Fertility-sparing approach in patients with endometrioid endometrial cancer grade 2 stage IA (FIGO): a qualitative systematic review. BioMed Research International, 2022, 4070368.
- Gullo, G., et al., 2022. The reproductive potential of uterus transplantation: future prospects. Acta Bio-Medica : Atenei Parmensis, 93 (2), e2022138.
- Hullfish, K. L., et al., 2002. Patient-centered goals for pelvic floor dysfunction surgery: what is success, and is it achieved? American Journal of Obstetrics and Gynecology, 187 (1), 88–92.
- Komesu, Y. M., et al., 2008. Patient-selected goal attainment for pessary wearers: what is the clinical relevance? Am J Obstet Gynecol, 198 (5), 577.e571–575.
- Manchana, T. and Bunyavejchevin, S., 2010. Validation of the prolapse quality of life (P-QOL) questionnaire in Thai version. International Urogynecology Journal, 21 (8), 985–993.
- Milne, J. L., et al., 2009. Goal achievement as a patient-generated outcome measure for stress urinary incontinence. Health Expectations : an International Journal of Public Participation in Health Care and Health Policy, 12 (3), 288–300.
- Obut, M., Oğlak, S. C. and Akgöl, S., 2021. Comparison of the quality of life and female sexual function following laparoscopic pectopexy and laparoscopic sacrohysteropexy in apical prolapse patients. Gynecology and Minimally Invasive Therapy, 10 (2), 96–103.
- Rockwood, T. H., et al., 2013. The PISQ-IR: considerations in scale scoring and development. International Urogynecology Journal, 24 (7), 1105–1122.
- Schulz, K. F., Altman, D. G. and Moher, D, 2010. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. PLOS Medicine, 7 (3), e1000251.
- Srikrishna, S., et al., 2008. Is there a difference in patient and physician quality of life evaluation in pelvic organ prolapse? International Urogynecology Journal and Pelvic Floor Dysfunction, 19 (4), 517–520.
- Sung, V. W., et al., 2016. Patient-reported goal attainment and comprehensive functioning outcomes after surgery compared with pessary for pelvic organ prolapse. Am J Obstet Gynecol, 215 (5), 659.e651–659.e657.
- Tanos, P., et al., 2022. Biomolecular and genetic prognostic factors that can facilitate fertility-sparing treatment (FST) decision making in early stage endometrial cancer (ES-EC): a systematic review. International Journal of Molecular Sciences., 23 (5), 2653–2672.
- Turner-Stokes, L., 2009. Goal attainment scaling (GAS) in rehabilitation: a practical guide. Clinical Rehabilitation, 23 (4), 362–370.
- Turner-Stokes, L., et al., 2020. Goal-setting and attainment in prolonged disorders of consciousness - development of a structured approach. Brain Injury, 34 (1), 78–88.
- Vitale, S. G., et al., 2018. Transvaginal bilateral sacrospinous fixation after second recurrence of vaginal vault prolapse: efficacy and impact on quality of life and sexuality. BioMed Research International, 2018 (28), 5727165.
- Witjes, S., et al., 2019. Goal setting and achievement in individualized rehabilitation of younger total and unicondylar knee arthroplasty patients: a cohort study. Archives of Physical Medicine and Rehabilitation, 100 (8), 1434–1441.