

Abstract
This study was to investigate the incidence, survival and prognostic factors of cervical cancer with distant organ metastasis, and to develop a nomogram to predict the prognosis of cervical cancer. We used the Surveillance, Epidemiology and End Results (SEER) database to screen patients diagnosed with cervical cancer from 2010 to 2014. The chi-squared test was used to analyse the differences in clinical characteristics, and we used Kaplan–Meier methods to perform survival analysis. Univariate and multivariate Cox proportional hazard regression models were used to estimate prognostic factors, and we developed a visual nomogram to judge the prognosis. We found that lung metastasis was the most common in cervical cancer patients with distant organ metastasis. Age, race, characteristics of the tumour, and therapy should be considered when analysing the prognosis of cervical cancer patients. The findings of this study may help clinicians to formulate individualised treatment strategies.
What is already known on this subject? Distant organ metastasis of cervical cancer mainly involves lung, bone, liver and brain. Once it occurs, the survival and prognosis will be threatened seriously.
What the results of this study add? 4176 patients were included, and lung metastasis was the most common in cervical cancer with distant organ metastasis (3.5%). Additionally, age, race, tumour grade, histological type, T-stage, N-stage, lung, liver and bone metastasis and the treatment mode are significantly related to the outcomes of cervical cancer patients. Furthermore, we developed a nomogram that could predict the probability of three-year and five-year OS.
What the implications are of these findings for clinical practice and/or further research? The findings of this study may drive more and more studies focussing on the comprehensive prognostic assessment, diagnosis, and treatment of distant metastasis of cervical cancer. Besides, clinicians can utilise these findings to formulate individualised treatment strategies.
Impact Statement
Introduction
Cervical cancer is the fourth leading cause of cancer-related death in women around the world (Sung et al. Citation2021). Besides, it is one of the most frequently diagnosed cancers among women, and there were more than 600,000 new cases of cervical cancer, of which about 342,000 died of this cancer in 2020 worldwide (Small et al. Citation2017, Sung et al. Citation2021). Most patients diagnosed with cervical cancer are infected with high-risk human papillomavirus (HPV) that can be prevented by carrageenan (CG) (Crosbie et al. Citation2013, Calagna et al. Citation2020). And it has been shown that about 10–15% of high-grade squamous intraepithelial lesion (HSIL) patients are negative for high-risk HPV and have a lower recurrence rate comparing to those who are positive for high-risk HPV (Bogani Citation2021). Although efforts are being made around the world to reduce the incidence and mortality of cervical cancer by improving HPV vaccination rate, popularising cervical cancer screening, and treating HSIL in time, there are still a number of cervical cancer patients with advanced stage and even metastasis at initial diagnosis, which greatly reduces the survival of them (Li et al. Citation2016). Therefore, advanced cervical cancer, especially with metastasis, remains a major concern for public health (Mountzios et al. Citation2013). The main metastatic pathways of cervical cancer include direct spread, lymphatic metastasis and haematogenous metastasis. The first two modes of metastasis are relatively common, yet the distant organ metastasis caused by haematogenous dissemination is unusual, mainly involving the lung (4.16%–7.7%), bone (0.8%–29%), liver (1.2%–2.2%) and brain (0.5%–1.2%) (Carlson et al. Citation1967, Raggio and Kaplan Citation1982, Abdul-Karim et al. Citation1990, Cormio et al. Citation1996, Fulcher et al. Citation1999, Agarwal et al. Citation2002, Babar et al. Citation2007, Disibio and French Citation2008, Thanapprapasr Citation2010, Ishikawa Citation2012, Li et al. Citation2016). Once metastasis occurs in a distant organ, the risk of death will be 5.3 times higher than that of lymphatic metastasis (Carlson et al. Citation1967, Kim et al. Citation2010).
Although there have been some studies on cervical cancer with distant organ metastasis, the epidemiology and signatures of these patients are still unclear (Li et al. Citation2016). Therefore, we used the Surveillance, Epidemiology and End Results (SEER) database to comprehensively explore the epidemiological characteristics, analyse the possible prognostic factors, and predict the survival time of cervical cancer with distant organ metastasis.
Materials and methods
Our manuscript conforms to the Enhancing the QUAlity and Transparency Of health Research (EQUATOR) network guidelines.
The SEER database covers about 30% of the American population and is one of the largest registry databases of cancer information supported by the National Cancer Institute of the United States currently (Mao et al. Citation2019, Zheng Citation2019). It includes basic demographic information and cancer characteristics, such as diagnosis age, year of diagnosis, race, TNM stage, treatment modality and survival time (Martin et al. Citation2017, Mao et al. Citation2020). Additionally, the SEER database has started to record the metastasis information of lung, liver, bone and brain since 2010. We used the National Cancer Institute’s SEER*Stat 8.4.0 software (1975-2019 SEER Research Plus Data, 8 Registries, November 2021 submission) to access the SEER database and the registration code was 11003-Nov2021.
Analysis of the de-identified data from the SEER database is exempt from medical ethics review, and informed consent is not required because the SEER database does not contain personal information. All procedures performed in this study involving human participants were in accordance with the declaration of Helsinki 1964, its amendments, and subsequent clarification or comparable ethical standards.
Study population selection
In order to select cases diagnosed with malignant cervical cancer from 2010 to 2014, we limited the site code ICD-O-3 (International Classification of Diseases for Oncology-3)/World Health Organisation (WHO) 2008 to ‘cervix uteri’, the behaviour code ICD-O-3 to ‘malignant’ and the year of diagnosis to ‘2010–2014’. Patients who met any of the following criteria were excluded: younger than 18 years, unknown survival time, unknown lung metastasis, unknown liver metastasis, unknown bone metastasis, and unknown brain metastasis.
Data elements
The following patient demographic and clinical characteristics were included: year of diagnosis, age, race, marital status, tumour grade, histological type, T-stage, N-stage, lung metastasis, liver metastasis, bone metastasis, brain metastasis, surgery, radiotherapy, chemotherapy and survival time (months). Overall survival (OS) was the primary study end point. Besides, median OS, three-year OS and five-year OS were also other interest outcomes in our study.
After submitting a request for access and signing the SEER research data agreement, we downloaded all the raw data from the SEER website (https://seer.cancer.gov/data/) via the SEER*Stat 8.4.0 software in client-server mode in our study.
Statistical analysis
We used chi-squared test to analyse the differences in the clinical characteristics with distant organ metastasis. Then Kaplan–Meier methods were used to analyse the OS. The log-rank test was used to compare the differences between them.
Prognostic nomogram for overall survival
Univariate and multivariate Cox proportional hazard regression models were used to estimate the hazard ratios (HR) and 95% confidence intervals (CI) in order to determine the relationship between independent prognostic factors and OS. Then we developed a novel visual nomogram based on the results of Cox proportional hazards regression. Finally, we tested the nomogram by using the area under receiver operating characteristic (ROC) curves (AUC) and calibration curves. A p value of <.05 was considered significant in all statistical analyses. The SPSS software (version 25; IBM Corp., USA) and R software (version 4.2.0; http://www.r-project.org/) were used for all statistical analyses.
Results
We found 4407 patients with cervical cancer between 2010 and 2014 in the database totally. According to the inclusion and exclusion criteria, 4176 cases were eventually included in our study.
The demographic data and clinical characteristics are shown in . There were 147 (3.5%) cervical cancer patients with lung metastasis, 84 (2.0%) and 81 (1.9%) patients with liver metastasis and bone metastasis respectively, besides, the number of patients with brain metastasis was the least, only 8 (0.2%) patients.
Table 1. Characteristics of patients with cervical cancer in our study.
Incidence
The incidence of lung metastasis (147, 3.5%) was the highest. With the increase of age, tumour grade, T-stage and N-stage, the incidence of lung metastasis also gradually increased (p < .001). Besides, black people were more likely to have lung metastasis (6.1%, p = .005) than white people. Compared with adenocarcinoma, squamous cell carcinoma had a higher rate of lung metastasis (p < .001). However, the differences in year of diagnosis and marital status were not significantly (p ≥ .05).
Similar to lung metastasis, patients over 80 years old (3.9%, p = .01), black patients (4.8%, p < .001) and patients with grade IV (9.2%, p < .001) or T4-stage (7.7%, p < .001) or N1-stage (3.7%, p < .001) had a higher rate of liver metastasis. Unlike lung metastasis, the incidence of liver metastasis in squamous cell carcinoma is lower than that in adenocarcinoma (1.5%, p < .001). However, there was no statistical significance in year of diagnosis and marital status (p ≥ .05).
Bone metastasis was not statistically significant in race, in addition to the year of diagnosis. Unlike lung and liver metastasis, married patients had a lower rate of bone metastasis compared with unmarried patients (2.5%, p = .043), and patients between 60 years and 80 years had the highest rate of bone metastasis (3.5%, p < .001). Adenocarcinoma was less likely to develop bone metastasis than squamous cell carcinoma (1.7%, p < .001). Similarly, bone metastasis was more easily to occur in the patients with grade IV (3.4%, p = .001), T4-stage (9.2%, p < .001) and N1-stage (5.0%, p < .001).
The number of patients with brain metastasis (8, 0.2%) were the lowest. There was no statistical significance in year of diagnosis, age at diagnosis, race, tumour grade and marital status (All p ≥ .05). Besides, patients with squamous cell carcinoma (0.2%, p = .049), T4-stage (1.4%, p = .049) and N1-stage (0.6%, p = .049) were more likely to have brain metastasis.
The most common single metastasis site was lung metastasis (81, 1.9%), followed by bone metastasis (42, 1%) and liver metastasis (33, 0.8%), brain metastasis (4, 0.1%) accounted for the lowest proportion. In the two sites of metastasis, the proportion of lung and liver metastasis (32, 0.8%) were the highest, followed by lung and bone metastasis (22, 0.5%), liver and bone metastasis (8, 0.2%), lung and brain metastasis (2, 0.0%), liver and brain metastasis (1, 0.0%) and finally bone and brain metastasis (0, 0.0%). Among the three-site metastasis, lung, liver and bone were the most common (9, 0.2%), followed by lung, liver and brain (1, 0.0%). In addition, there was no simultaneous metastasis of four sites in these screened patients with cervical cancer (Supplementary Table 2).
Table 2. Kaplan–Meier analysis OS, three-year and five-year OS for cervical cancer patients.
Survival analysis
The related factors on OS of cervical cancer patients are shown in . According to the Kaplan–Meier analysis we found that age, race, marital status, tumour grade, histological type, T-stage, N-stage, organ metastasis, and the mode of treatment were possible prognostic factors. The five-year OS of cervical cancer patients with these four organ metastases was not optimistic, the worst was liver metastasis (5.0%), followed by lung metastasis (11.7%) and brain metastasis (12.5%), and the best prognosis was bone metastasis (13.1%).
Patients treated with surgery only had the highest three-year OS (97.5%) and five-year OS (96.3%), in contrast to patients treated with chemotherapy only, who had the lowest three-year OS (24.2%) and five-year OS (9.1%). In addition, we also found that the three-year OS (89.5%) and five-year OS (86.7%) of patients with surgery combined with radiotherapy were considerable (Supplementary Table 1).
We found for single-site metastasis, the median OS from high to low was bone (23 months), liver (9 months), lung (7 months) and brain (4 months) metastasis. In cervical cancer patients with two and three metastatic sites, due to the limitation of the number of patients, only lung and bone metastasis could completely calculate the median OS (seven months), three-year OS (9.1%) and five-year OS (4.6%) (Supplementary Table 2).
Prognostic factors of OS
We used univariate and multivariate Cox proportional hazard regression to calculate the prognostic factors of OS and the detailed information is shown in . From the results of multivariate Cox regression analysis, we found that age at diagnosis, race, tumour grade, histological type, T-stage, N-stage, lung metastasis, liver metastasis, bone metastasis, and the mode of treatment were independent prognostic factors. Additionally, marital status and brain metastasis were not significant factors.
Table 3. Univariate and multivariable Cox regression analysis of OS.
Nomogram
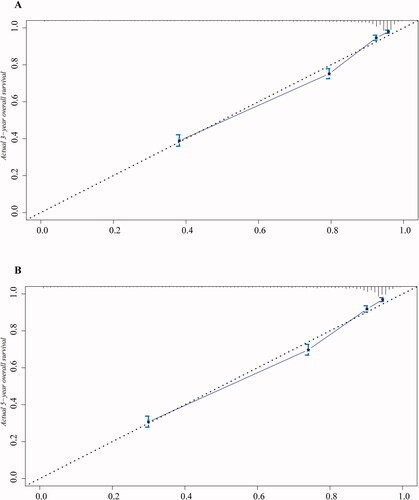
We built and interpreted a visualised nomogram for predicting the survival rate based on the Cox regressions results (). An individual patient’s value is located on different variable axes, and a vertical line is drawn upward to determine the points received for each variable value. Final total score is located on the total points axis and a vertical line is drawn downward to the survival axes to determine the possibility of five-year OS and three-year OS. In this nomogram, the blue boxes represent the sample size of demographic statistics and the yellow colour block on the total points axis represent the population distribution of the prognosis. Finally, in order to evaluate the discriminative ability of nomogram, we drew the , which included two receiver operating characteristic (ROC) curves of three-year OS (AUC = 0.881) and five-year OS (AUC = 0.879). And the concordance of the nomogram is shown by the calibration curves (). In , dotted line represents location of the ideal nomogram in which predicted and actual probabilities are identical, and solid line indicates expected performance on future data. In summary, this visualised nomogram had considerable discriminative and calibrating abilities.
Figure 1. Nomogram for predicting three-year and five-year OS of cervical cancer patients.
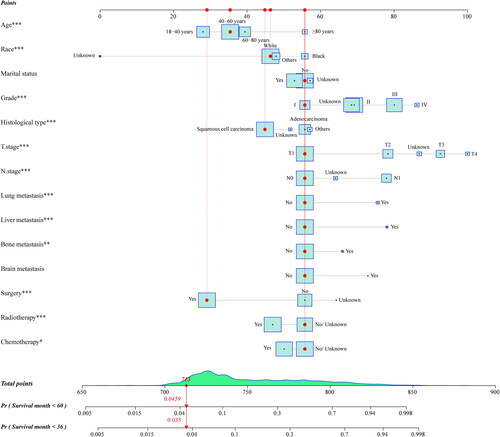
Figure 2. ROC curves of nomogram for predicting the OS of cervical cancer patients. (A) Three-year OS and (B) five-year OS.
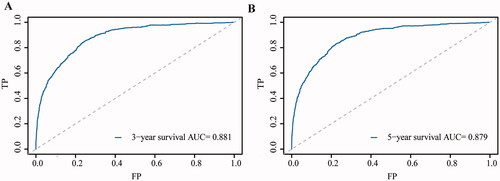
Figure 3. The calibration curves for predicting three-year and five-year OS of cervical cancer patients between the nomogram and the actual observation. (A) Three-year OS and (B) five-year OS.
For example, a white unmarried cervical cancer patient aged between 40 and 60 without lung, liver, bone or brain metastasis, her tumour grade is grade I and histological type is squamous cell carcinoma, besides, she belongs to T1N0 and she received surgery, but she had no radiotherapy or chemotherapy, or whether she received radiotherapy or chemotherapy is unknown. Her total point is 713, and the probability of her survival of less than five years and three years are .0459 and .035, respectively.
Discussion
Distant organ metastasis of cervical cancer is very rare, but it has a critical impact on the prognosis of patients. However, there are few studies on cervical cancer with distant organ metastasis, and most of them focus on a specific metastasis site or stage (Blythe Citation1975, Cormio et al. Citation1996, Thanapprapasr Citation2010, Yoon et al. Citation2013). Therefore, we conducted this comprehensive study to cover as much of the population as possible, rather than just focussing on specific parts in order to achieve the widest applicability under existing conditions. In our study, we found that the incidence of lung metastasis was the highest among all cervical cancer with distant metastasis, while brain metastasis was the lowest, liver metastasis and bone metastasis were in the middle. Besides, age at diagnosis, race, tumour grade, histological type, T-stage, N-stage, lung metastasis, liver metastasis, bone metastasis and the mode of treatment have been proved to be independent prognostic factors for cervical cancer. In addition, our nomogram is a useful tool for risk assessment and survival prediction in cervical cancer patients. It can provide effective prognostic assessment for patients with cervical cancer, which is helpful for doctors to provide individualised treatment.
Our study showed that in cervical cancer patients, lung metastasis was more common in distant organ metastasis, followed by liver metastasis and bone metastasis, and brain metastasis was rare, which is consistent with previous retrospective studies (Li et al. Citation2016). The reason for more lung metastasis and less brain metastasis may be the lung is often the first filter and the brain has its unique cell types, anatomical structures and immune environment (Boire et al. Citation2020, Mao et al. Citation2020). In the study, we found that the incidence of distant organ metastasis of cervical cancer didn’t change significantly every year, which may be due to little change in the annual detection rate of advanced cervical cancer. Besides, our study found that lung, bone and liver metastasis were more likely to occur in cervical cancer patients over 80 years old, but there was no age difference in brain metastasis. In addition to their own physical function factors, this may also be due to delayed diagnosis or inadequate treatment of elderly patients (Berkman Citation1994, Yoon et al. Citation2013, Darlin Citation2014, Kissel et al. Citation2020). As for race, we found that blacks were more likely to have lung and liver metastasis and less likely to have brain metastasis than whites, while there was no racial difference in bone metastasis, which is roughly consistent with previous studies (Alimena et al. Citation2021). The reason why unmarried patients were more prone to bone metastasis may be spouses can provide social support and encourage patients to seek medical help (Mao et al. Citation2020). In addition, patients with high tumour grade and high TNM stage were more likely to develop lung, bone, liver and brain metastasis. The reason could be that the higher the tumour grade and TNM stage, the higher the degree of malignancy (Lee Citation2019). Although there was little difference, squamous cell carcinoma was more likely to have organ metastasis than adenocarcinoma. The occurrence of this condition may be related not only to the common occurrence of squamous cell carcinoma in cervical cancer, but also to the different biological characteristics of the two histological types (Levi et al. Citation1994).
Through survival analysis, we found that the more metastatic sites, the more threatened the OS of patients, which is precise because more metastatic sites mean higher cancer progression. Although lung metastasis accounted for the highest proportion of single organ metastasis, its median OS was not the shortest. On the contrary, although the proportion of brain metastasis was the lowest, its median OS was the shortest. This shows that compared with the common lung metastasis, due to the particularity of the part of the brain and the importance of function, once rare brain metastasis occurs, it will seriously endanger the survival of patients with cervical cancer. Of the two metastatic sites, our analysis found the shortest median OS in the lung and brain metastasis and the longest in the liver and brain metastasis. Yet due to the limitations of the number of patients in these two groups, it is reasonable to assume that this conclusion is not accurate enough. And there were fewer patients with three metastasis sites who can be used to analyse accurately. Patients with lung metastasis of cervical cancer had relatively long median OS, which may be related to the following factors: (1) the metastasis can be found easily by roentgenography or CT; (2) The treatment methods are diverse and effective, for example, surgery, chemotherapy and radiotherapy can improve the prognosis (Saijo Citation1982, González Casaurrán Citation2011, Shu Citation2014). However, brain metastasis of cervical cancer often occurs in the supratentorial area of the brain and is not easy to find, and there is still no satisfactory treatment, which leads to the fact that brain metastasis of cervical cancer is often regarded as an incurable disease (Cormio et al. Citation1996, Ikeda et al. Citation1998, Erdis Citation2014). This may explain why there were great differences in median OS between different metastatic sites.
Similar to other solid tumours, age at diagnosis, race, tumour grade, histological type, T-stage, N-stage, lung metastasis, liver metastasis, bone metastasis and the mode of treatment were independent prognostic factors (Leone et al. Citation2017, Luo et al. Citation2018). We found that the age, tumour grade and TNM stage at the time of diagnosis were negatively correlated with the OS of patients with cervical cancer, and the occurrence of lung, liver or bone metastasis would shorten the OS of patients, and surgery, chemotherapy or radiotherapy were beneficial to improve the prognosis of patients. In addition, whites with histological type of squamous cell carcinoma had a better prognosis than blacks with histological type of adenocarcinoma. Interestingly, we found that marital status and brain metastasis have no effect on predicting the prognosis of cervical cancer patients, which is contrary to some other studies (Li et al. Citation2016). In our opinion, this may be related to the small number of patients with brain metastases included in this study, and the fact that most of these patients have died, making this conclusion inaccurate.
In order to better predict the prognosis of cervical cancer patients, we used the results of Cox regression analysis and chose the age at diagnosis, race, marital status, tumour grade, histological type, T-stage, N-stage, lung metastasis, liver metastasis, bone metastasis, brain metastasis and the mode of treatment for our nomogram, although some of these factors showed no significant difference in our Cox proportional hazard regression analysis. At present, there are few articles on nomogram predicting survival in cervical cancer patients. However, it is undeniable that the use of nomogram to predict survival in patients with cervical cancer was found to be very intuitive and comprehensive. It not only incorporates TNM staging, but also takes into account individual patient differences. At some point its predictive role may be better than existing prediction systems, but more in-depth studies are needed to confirm this. Additionally, recent studies have found that some biomarkers are important for diagnosing early cervical cancer and assessing its progression, metastasis and prognosis, for example, P16INK4a and ki-67 immunocytochemistry have been proposed as biomarkers panel to detect pre‑invasive to invasive lesions shift, HPV E6/E7 mRNA may serve as a predictor of disease persistence or relapse in women, DNA aneuploidy and ProExC immunocytochemistry combined with cytological results is a marker for HSIL and can determine which lesions are likely to progress, the gain of chromosome arm 3q by fluorescent in situ hybridisation (FISH) may be used to identify women who do not require close monitoring, biomarkers related to DNA methylation and peritoneal HPV positivity are important for treatment and prognosis (Valenti et al. Citation2017, Bizzarri et al. Citation2021).
Several limitations should be taken into consideration in our study. Firstly, there is no International Federation of Gynaecology and Obstetrics (FIGO) staging system in the SEER database. Secondly, the records in the database didn’t cover some key indicators, such as surgical methods, cycles and doses of radiotherapy and chemotherapy, and patient complications. Finally, our nomogram cannot be externally verified, and only internal verification is possible because of a lack of data support.
Our study may contribute to the development of treatment and prognosis of cervical cancer patients in the future, especially those with distant organ metastasis. The comprehensive individualised evaluation of cervical cancer patients through nomogram is beneficial to the individualised and precise treatment of cervical cancer patients in the future, so as to improve their prognosis and maximise their benefits. In order to further evaluate the clinical application value of nomogram, this study may attract more and more researchers to devote themselves to relevant research, so as to construct a new diagnosis and treatment system for patients with cervical cancer.
Supplemental Material
Download Zip (16.8 KB)Acknowledgements
We would like to thank everyone who helped with this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abdul-Karim, F. W., et al., 1990. Bone metastasis from gynecologic carcinomas: a clinicopathologic study. Gynecologic Oncology, 39 (2), 108–114.
- Agarwal, U., et al., 2002. Scalp metastasis in carcinoma of the uterine cervix–a rare entity. Gynecologic Oncology, 87 (3), 310–312.
- Alimena, S., et al., 2021. Race- and age-related disparities in cervical cancer mortality. Journal of the National Comprehensive Cancer Network: JNCCN, 19 (7), 789–795.
- Babar, S., et al., 2007. Magnetic resonance imaging appearances of recurrent cervical carcinoma. International Journal of Gynecological Cancer: Official Journal of the International Gynecological Cancer Society, 17 (3), 637–645.
- Berkman, B., 1994. Myths and biases related to cancer in the elderly. Cancer, 74 (7 Suppl), 2004–2008.
- Bizzarri, N., et al., 2021. Peritoneal HPV-DNA test in cervical cancer (PIONEER study): a proof of concept. International Journal of Cancer, 148 (5), 1197–1207.
- Blythe, J. G., 1975. Bony metastases from carcinoma of cervix. Occurrence, diagnosis, and treatment. Cancer, 36 (2), 475–484.
- Bogani, G., 2021. High-risk HPV-positive and -negative high-grade cervical dysplasia: analysis of 5-year outcomes. Gynecologic Oncology, 161 (1), 173–178.
- Boire, A., et al., 2020. Brain metastasis. Nature Reviews. Cancer, 20 (1), 4–11.
- Calagna, G., et al., 2020. Secondary prevention’ against female HPV infection: literature review of the role of carrageenan. Expert Review of anti-Infective Therapy, 18 (9), 865–874.
- Carlson, V., Delclos, L., and Fletcher, G. H., 1967. Distant metastases in squamous-cell carcinoma of the uterine cervix. Radiology, 88 (5), 961–966.
- Cormio, G., et al., 1996. Brain metastases from cervical carcinoma. Tumori, 82 (4), 394–396.
- Crosbie, E. J., et al., 2013. Human papillomavirus and cervical cancer. Lancet, 382 (9895), 889–899.
- Darlin, L., 2014. Elderly women above screening age diagnosed with cervical cancer have a worse prognosis. Anticancer Research., 34 (9), 5147–5151.
- Disibio, G. and French, S. W., 2008. Metastatic patterns of cancers: results from a large autopsy study. Archives of Pathology & Laboratory Medicine, 132 (6), 931–939.
- Erdis, E., 2014. A rare metastatic region of cervix cancer; the brain. Journal of Pakistan Medical Association, 64 (1), 89–90.
- Fulcher, A. S., et al., 1999. Recurrent cervical carcinoma: typical and atypical manifestations. Radiographics: A Review Publication of the Radiological Society of North America, Inc, 19, S103–S116; quiz S264–S265.
- González Casaurrán, G., 2011. Surgery of female genital tract tumour lung metastases. Arch Bronconeumol, 47 (3), 134–137.
- Ikeda, S., et al., 1998. Cerebral metastasis in patients with uterine cervical cancer. Japanese Journal of Clinical Oncology, 28 (1), 27–29.
- Ishikawa, M., 2012. A case of stage IVb cervical carcinoma in which survival was prolonged by two different chemotherapies and CCRT. Gan to Kagaku Ryoho, 39 (3), 451–455.
- Kim, K., et al., 2010. The type of metastasis is a prognostic factor in disseminated cervical cancer. Journal of Gynecologic Oncology, 21 (3), 186–190.
- Kissel, M., et al., 2020. Challenges and advances in cervix cancer treatment in elder women. Cancer Treatment Reviews, 84, 101976.
- Lee, S. I., 2019. 2018 FIGO staging system for uterine cervical cancer: enter cross-sectional imaging. Radiology, 292 (1), 15–24.
- Leone, B. A., et al., 2017. Prognostic impact of metastatic pattern in stage IV breast cancer at initial diagnosis. Breast Cancer Research and Treatment, 161 (3), 537–548.
- Levi, F., et al., 1994. Incidence, mortality and survival from invasive cervical cancer in Vaud, Switzerland, 1974-1991. Annals of Oncology: Official Journal of the European Society for Medical Oncology, 5 (8), 747–752.
- Li, H., Wu, X., and Cheng, X., 2016. Advances in diagnosis and treatment of metastatic cervical cancer. Journal of Gynecologic Oncology, 27 (4), e43.
- Luo, D., et al., 2018. Prognostic value of distant metastasis sites and surgery in stage IV colorectal cancer: a population-based study. International Journal of Colorectal Disease, 33 (9), 1241–1249.
- Mao, W., et al., 2019. More lymph node dissection improves survival in patients with newly diagnosed lymph node-positive penile cancer. International Urology and Nephrology, 51 (4), 641–654.
- Mao, W., et al., 2020. Clinicopathological study of organ metastasis in endometrial cancer. Future Oncology, 16 (10), 525–540.
- Martin, A. M., et al., 2017. Brain metastases in newly diagnosed breast cancer: a population-based study. JAMA Oncology, 3 (8), 1069–1077.
- Mountzios, G., et al., 2013. Developments in the systemic treatment of metastatic cervical cancer. Cancer Treatment Reviews, 39 (5), 430–443.
- Raggio, M. and Kaplan, A. L., 1982. Carcinoma of the cervix metastatic to the liver presenting with obstructive jaundice. Gynecologic Oncology, 13 (2), 269–270.
- Saijo, N., 1982. Chemotherapy against pulmonary metastasis from uterine cervical carcinoma. Gan to Kagaku Ryoho, 9 (6), 992–997.
- Shu, T., 2014. Clinical analysis and prognostic factors in 106 patients with stage Ia-IIb cervical cancer with pulmonary metastasis. Zhonghua Zhong Liu Za Zhi, 36 (9), 703–707.
- Small, W. Jr, et al., 2017. Cervical cancer: a global health crisis. Cancer, 123 (13), 2404–2412.
- Sung, H., et al., 2021. global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians, 71 (3), 209–249.
- Thanapprapasr, D., 2010. Bone metastasis in cervical cancer patients over a 10-year period. Int J Gynecol Cancer, 20 (3), 373–378.
- Valenti, G., et al., 2017. Tumor markers of uterine cervical cancer: a new scenario to guide surgical practice? Updates in Surgery, 69 (4), 441–449.
- Yoon, A., et al., 2013. Contributing factors for bone metastasis in uterine cervical cancer. International Journal of Gynecological Cancer: Official Journal of the International Gynecological Cancer Society, 23 (7), 1311–1317.
- Zheng, X. Q., 2019. Incidence, prognostic factors, and a nomogram of lung cancer with bone metastasis at initial diagnosis: a population-based study. Translational Lung Cancer Research, 8 (4), 367–379.