

Abstract
At concentrations achieved following systemic administration, the primary effect of imidazoles and triazoles on fungi is inhibition of 14-α-sterol demethylase, a microsomal cytochrome P450 (CYP) enzyme. Imidazoles and triazoles impair the biosynthesis of ergosterol for the cytoplasmic membrane and lead to the accumulation of 14-α-methyl sterols. The synthetic imidazole miconazole is additionally able to increase intracellular reactive oxygen species, at least in part through inhibition of fungal catalase and peroxidase. This unique feature of miconazole is probably the basis for its fungicidal activity in C. albicans, in addition to the fungistatic mode of action. Studies show that miconazole is superior to nystatin treatment and demonstrate its impact as one of the best options in managing vulvovaginal candidiasis. Regarding recurrent vulvovaginal candidiasis, several new drugs are currently developed to ensure effective treatment also for this group of patients.
Introduction
Descriptions of Candida, especially the oral form, go back to the time of Hippocrates circa 460–370 BCE (Bennett et al. Citation2019). Vulvovaginal candidiasis was first described in 1849 by Wilkinson (Lynch Citation1994). In 1875, Haussmann demonstrated that both vulvovaginal and oral candidiasis are caused by the same organism (Lynch Citation1994). With the advent of antibiotics following World War II, the rates of candidiasis increased, before they decreased in the 1950s after the development of nystatin (Brunton Citation2011).
Genital candidiasis
Candidiasis’s signs and symptoms vary depending on the area affected (Bennett et al. Citation2019). Generally, most candida infections result in minimal-to-marked redness, itching and discomfort, though complications may be severe or fatal if left untreated in specific populations. In healthy (immunocompetent) persons, candidiasis is usually a localised infection of the skin, fingernails, or toenails (onychomycosis), or mucosal membranes, including the oral cavity and pharynx (thrush), oesophagus, and genitalia (vagina, glans penis, etc.) (Walsh et al. Citation1996, Patil et al. Citation2015, Hidalgo and Vazquez Citation2020). Less common sites of candida infection in healthy individuals are the gastrointestinal tract, urinary tract and respiratory tract (Martins et al. Citation2014, Wang et al. Citation2014, Erdogan and Rao Citation2015).
Infection of the vagina or vulva may cause severe itching, burning, soreness, irritation, and a whitish, greenish or yellowish cottage-cheese-like discharge. Symptoms of disease of the male genitalia (balanitis thrush) include redness, swelling, irritation, itchiness and soreness of the head of the penis, thick, lumpy discharge under the foreskin, unpleasant odour, difficulty retracting the foreskin (phimosis), and pain when passing urine or during sex (Doering and Santiago Citation1990).
Causes
Candida yeasts are generally present in healthy humans, frequently as a part of the human body’s normal oral, intestinal and vaginal flora, and particularly on the skin. However, their growth is generally limited by the human immune system and by competition of other microorganisms, such as bacteria occupying the same locations in the human body (Mulley and Goroll Citation2006). Candida requires moisture for growth, especially on the skin (Goehring Citation2008).
The majority of cases of candidiasis is caused by C. albicans (89%), followed by C. glabrata (7.9%), C. parapsilosis (1.7%) and C. tropicalis (1.4%). This distribution of Candida species is consistent among the different age groups, yet it could be demonstrated that infections caused by C. albicans decrease with the women’s age (Vermitsky et al. Citation2008).
Remarkably, the overall susceptibility to develop vaginal candidiasis declines with age. Reasons for this phenomenon are an elevated pH and lower glycogen levels in the vaginal epithelium in post-menopausal women which impairs pathological overgrowth of Candida yeasts (Hillier and Lau Citation1997).
Factors that increase the risk of candidiasis include HIV/AIDS, mononucleosis, cancer treatments, steroids, stress, use of antibiotics, diabetes and nutrient deficiency. Hormone replacement therapy and infertility treatment may also be predisposing factors (Nwokolo and Boag Citation2000). Treatment with antibiotics can eliminate the yeast’s natural competitors for resources in the oral, intestinal and vaginal flora, thereby promoting colonisation of Candida (Bassetti et al. Citation2010). A weakened or undeveloped immune system or metabolic illnesses are also significant predispositions for candidiasis (Odds Citation1987). Almost 15% of patients with a weakened immune system develop a systemic illness caused by Candida species (Choo et al. Citation2010). Diets which are high in carbohydrates have been found to affect the incidence of oral and vaginal candidiasis (Akpan and Morgan Citation2002, Rachapromma and Chayachinta Citation2022). External use of detergents or douches or internal disturbances (hormonal or physiological) can perturb the normal vaginal flora like Lactobacilli resulting in an overgrowth of Candida spp. (Mårdh et al. Citation2003). Pregnancy and oral contraceptives have been reported as risk factors as well (Schiefer Citation1997).
The causes of penile candidiasis include sexual intercourse with an infected individual, low immunity, antibiotics and diabetes. Male genital yeast infections are less common, and incidences of the disease are only a fraction of those in women; however, yeast infection on the penis from direct contact via sexual intercourse with an infected partner is not uncommon (David et al. Citation1997).
Dysbiosis of a vaginal ecosystem may lead to multiple concurrent diseases. Symptoms of vaginal candidiasis are also present in the more common bacterial vaginosis (Warren Citation2010). Aerobic vaginitis, an overgrowth of intravaginal aerobic flora causing severe inflammation, is distinct and should be excluded from the differential diagnosis (Donders et al. Citation2002). In a 2002 study, only 33% of women who self-medicated for a yeast infection had such an infection, while most had bacterial vaginosis or a mixed-type infection (Ferris et al. Citation2002).
Diagnosis
Since the presence of a fungal infection can only be suspected by clinical parameters and examination, the final diagnosis is made via microscopic examination, culture or molecular diagnosis. For identification by light microscopy, a scraping or swab of the affected area is placed on a microscope slide. A drop of 10% potassium hydroxide (KOH) solution is added to the specimen. The KOH dissolves epithelial cells and leukocytes but leaves the Candida cells intact, permitting visualisation of pseudohyphae and budding yeast cells typical of many Candida species.
To establish a fungal culture, a sterile swab is rubbed on the infected skin surface or collects vaginal discharge which is then plated on a suitable culture medium. The culture is incubated at 37 °C (98.6 °F) for several days to develop fungal colonies. The colonies’ characteristics (such as morphology and colour) allow an initial diagnosis of the organism causing disease symptoms (Srikumar and Nagaraja Citation2011).
Prevention
Since carbohydrates have been associated to vaginal and oral candidiasis, a diet that supports the immune system and is not high in simple carbohydrates contributes to a healthy balance of the oral and intestinal flora (Akpan and Morgan Citation2002, Mulley and Goroll Citation2006). Even if yeast infections are associated with diabetes, the level of blood sugar control may not affect the risk (Nyirjesy and Sobel Citation2013). Wearing cotton underwear may help reduce the risk of skin and vaginal yeast infections, along with not wearing wet clothes for extended periods (Goehring Citation2008).
For women who experience recurrent yeast infections, there is limited evidence that oral or intravaginal probiotics, including either pills or yogurt, help to prevent future infections (Falagas et al. Citation2006, Jurden et al. Citation2012).
Mechanism of action and treatment against Candidiasis
General aspects
Antifungal agents are discussed under two major headings: systemic and topical. However, this distinction is rather arbitrary since the imidazole, triazole and polyene antifungal agents can be used systemically or topically for treating many superficial mycoses. Over the last several decades, the number of antifungal agents has increased remarkably.
Azole antifungal agents have dominated antifungal drug development and clinical use because of their broad-spectrum, oral bioavailability and low toxicity (Brunton Citation2011).
Mechanism of action of amphotericin, imidazoles, triazoles and allylamines in fungi
Amphotericin B and other polyenes, such as nystatin, bind to ergosterol in fungal cell membranes and thus increase membrane permeability (). Imidazoles and triazoles, such as itraconazole and fluconazole, inhibit 14-α-sterol demethylase, prevent ergosterol synthesis, and lead to the accumulation of 14-α-methyl sterols. These methyl sterols may disrupt the close packing of acyl chains of phospholipids, impairing the functions of specific membrane-bound enzyme systems such as ATPase and enzymes of the electron transport system and thus inhibiting the growth of the fungi. Some azoles (e.g. clotrimazole) directly increase the permeability of the fungal cytoplasmic membrane, but the concentrations required are likely only obtained with topical use.
Figure 1. Mechanism of action of amphotericin, imidazoles, triazoles, allylamines and 5-fluorocytosine in fungi. Amphotericine B binds to ergosterol in fungal cell membranes, thereby increasing membrane permeability. Imidazoles and triazoles inhibit 14-α-sterol demethylase which prevents ergosterol synthesis on the one hand and causes the accumulation of 14-α-methyl sterols on the other hand. These methyl sterols finally impair fungal cell growth. Allylamines such as naftifine or terbinafine additionally impair the squalene epoxidase, thus inhibiting lanosterol synthesis. Caspofungin as an echinocandin inhibits glucan synthesis, which finally destabilises the fungal cell wall. 5-Fluorocytosine interferes with the nucleic acid synthesis.
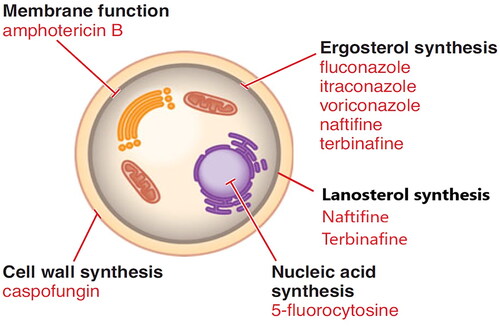
Allylamines, such as naftifine and terbinafine, inhibit squalene epoxidase and impair ergosterol synthesis. Echinocandins, such as caspofungin, inhibit the formation of glucans in the fungal cell wall (Brunton Citation2011).
Imidazoles and triazoles
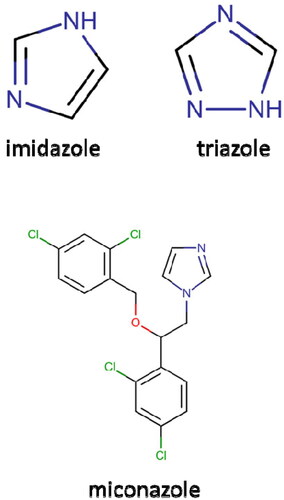
The azole antifungals include two broad classes, imidazoles and triazoles, which share the same antifungal spectrum and mechanism of action. The systemic triazoles are metabolised more slowly and have a more negligible effect on human sterol synthesis than the imidazoles. Due to these advantages, new congeners under development are primarily triazoles.
Of the drugs now on the market in the United States, clotrimazole, miconazole, ketoconazole, econazole, butoconazole, oxiconazole, sertaconazole and sulconazole are imidazoles while terconazole, itraconazole, fluconazole, voriconazole and posaconazole are triazoles (Brunton Citation2011).
depicts the structure of a triazole.
Figure 2. Structure of imidazole, triazole and miconazole.
Antifungal activity
Azoles have clinically helpful activity against Candida albicans, Candida tropicalis, Candida parapsilosis, Candida glabrata, Cryptococcus neoformans, Blastomyces dermatitidis, Histoplasma capsulatum, Coccidioides species, Paracoccidioides brasiliensis and ringworm fungi (dermatophytes). Aspergillus spp., Scedosporium apiospermum (Pseudallescheria boydii), Fusarium and Sporothrix schenckii are intermediate in susceptibility.
Candida krusei and mucormycosis-causing molds are partially resistant to treatment with azoles. In these cases, the drugs only have a limited antifungal activity. However, the investigational application of the azole posaconazole, has been shown to have some in vitro activity against mucormycosis (Brunton Citation2011).
Azole resistance has emerged gradually during prolonged azole therapy, causing clinical failure for example in patients with far advanced HIV infection and oropharyngeal or oesophageal candidiasis. The primary resistance mechanism in C. albicans is an accumulation of mutations in ERG11, the gene coding for the 14-α-sterol demethylase. These mutations protect the enzyme pocket from binding to azoles but allow access to the natural substrate for the enzyme, lanosterol. Cross-resistance affects all azoles. Increased azole efflux from the cytoplasm by ATP-binding cassette (ABC) and major facilitator superfamily transporters can add to fluconazole resistance in C. albicans and C. glabrata. Enhanced production of 14-α-sterol demethylase is another potential cause of resistance. Mutation of the C-5,6-sterol reductase gene ERG3 also increases azole resistance in some species (Brunton Citation2011).
Vaginal application
Vaginal creams, suppositories and tablets for vaginal candidiasis are used once a day for 1–7 days, preferably at bedtime, to facilitate retention. Most vaginal creams are administered in 5 g amounts. Three vaginal formulations – clotrimazole tablets, miconazole suppositories and terconazole cream – come in low- and high-dose preparations. These preparations are administered for 3–7 days. Approximately, 3–10% of the vaginally applied amount is absorbed. Although some imidazoles are teratogenic in rodents, no adverse effects on the human foetus have been attributed to the vaginal use of imidazoles or triazoles. The most common side effect is a mild vaginal burning or itching. A male sexual partner may experience mild penile irritation. Cross-allergenicity among these compounds is assumed to exist based on their structural similarities (Workowski and Bachmann Citation2022).
The US Centers for Disease Control and Prevention (CDC) and other clinicians generally recommend that uncomplicated vulvovaginal candidiasis (defined as vulvovaginal candidiasis that is mild to moderate, sporadic or infrequent, most likely caused by C. albicans, or occurring in immunocompetent women) should be treated with an intravaginal azole antifungal (e.g. butoconazole, clotrimazole, miconazole, terconazole and tioconazole) given in an appropriate single-dose or short-course regimens or oral fluconazole given in a single-dose regimen (Sobel Citation1994, Citation1997, Tobin Citation1995, Hay Citation1996, Sobel et al. Citation1998, Lansdorp et al. Citation1999, Workowski and Bachmann Citation2022).
These regimens have generally been associated with clinical and mycologic cure rates of 80–90% in otherwise healthy, nonpregnant women with uncomplicated infections. There is no clear evidence that any intravaginal azole antifungal regimen is superior to other intravaginal azole regimens available for treating these infections.
A longer duration of therapy (i.e. 7–14 days) with an intravaginal or oral azole antifungal is generally necessary to treat complicated vulvovaginal candidiasis, including recurrent and severe disease (Doering and Santiago Citation1990, Workowski and Bachmann Citation2022).
Vulvovaginal candidiasis is usually not acquired through sexual activity, and treatment of sexual partner(s) is not recommended but may be considered in women with recurrent infections.
Male sexual partners with symptomatic balanitis or penile dermatitis may benefit from treatment with a topical antifungal agent to relieve symptoms (Workowski and Bachmann Citation2022).
The antifungal miconazole
The first use of miconazole in medicine can be dated to the early 1970s, when several azole compounds were introduced to the market, primarily in topical forms, to treat superficial fungal infections. Miconazole is a synthetic imidazole derivative that has built a reputation for fast fungicidal action when being used topically against a wide variety of yeasts and dermatophytes (Sawyer et al. Citation1975, Ivanov et al. Citation2022).
Millions of patients have been treated with this compound in various formulations. Common indications for topical miconazole include vaginal and oral candidiasis, skin and nail infections due to Trichophyton, Epidermophyton, and Pityrosporon species, dermatomycosis, and onychomycosis (Zhang et al. Citation2019, Saxon et al. Citation2020, Kaur et al. Citation2021, Workowski et al. Citation2021). Miconazole antifungals are available most commonly in cream but also in gel, solution or spray formulations at a 1% (Jartarkar et al. Citation2021) or 2% concentration (Ridzuan et al. Citation2019), and most are indicated for use twice-daily for 2–4 weeks (Jartarkar et al. Citation2021) or occasionally for up to 6 weeks if required (Barasch and Griffin Citation2008). More potent miconazole-containing topical preparations are also used, such as in the USA, where several products that contain miconazole, typically a 2–4% cream, have been approved for over the counter (OTC) sale (Hay Citation2018). When using miconazole topically, particularly in the form of a cream, serious adverse effects are uncommon; reports of maceration, redness of the skin, and allergic or irritant contact dermatitis are sporadic and rare (Poojary Citation2017).
Interestingly, despite the wide availability and use of miconazole, fungal resistance to this drug remains relatively low (Fothergill Citation2006). The typical minimal inhibitory concentration (MIC) has a range of 1–10 µg/ml for most tested pathogens, including C. albicans (Casneuf et al. Citation1980, Redding et al. Citation1999). This fact becomes extremely important considering recurring opportunistic fungal disease.
Mechanisms of action of miconazole
Miconazole has multiple mechanisms of action. Azoles, the most common antimycotics in the pharmacopeia, damage fungal organisms by interfering with ergosterol biosynthesis, which results in toxic methylated sterol levels (Vanden Bossche et al. Citation1990). Kobayashi et al. described an additional antifungal mechanism for miconazole: accumulation of drug-induced reactive oxygen species (ROS) within the fungal organism results in oxidative damage and cell death (Kobayashi et al. Citation2002). This mechanism was confirmed in another publication by Thevissen et al. who studied the effects of miconazole in Saccharomyces cerevisiae and C. albicans demonstrated that the antifungal increases the stability of actin cables which corresponds to the model that an enhanced stability of actin filaments followed by clumping of actin triggers generation of ROS and induces apoptosis in yeast cells (Thevissen et al. Citation2007). In addition, miconazole increases intracellular ROS partly through inhibition of fungal catalase and peroxidase. It can be assumed that ROS-induced apoptosis is probably the basis for the fungicidal activity of miconazole, whereas other azoles are fungistatic. It could be further demonstrated that only miconazole but no other imidazole’s are able to induce ROS in C. albicans (Francois et al. Citation2006).
Miconazole readily penetrates the skin’s stratum corneum and persists for more than four days after application. Less than 1% is absorbed into the blood. Absorption is no more than 1.3% from the vagina (Brunton Citation2011).
Mild adverse effects from topical application to the vagina include burning, itching, irritation in about 7% of recipients, infrequently, pelvic cramps (0.2%), headache, hives or skin rash. Irritation, burning and maceration are rare after cutaneous application (Brunton Citation2011).
Miconazole is considered safe during pregnancy, although some authors recommend avoiding its vaginal use during the first trimester (Brunton Citation2011).
Uncomplicated vaginal candidiasis
The principal use of miconazole is in women with signs and symptoms of uncomplicated vulvovaginal candidiasis. The diagnosis should be confirmed either by demonstrating yeast or pseudohyphae with direct microscopic examination of vaginal discharge (saline, 10% KOHwet mount or Gram stain) or by culture. The identification of Candida by culture in the absence of symptoms is not an indication for antifungal treatment since approximately 10–20% of asymptomatic women harbour Candida or other yeasts in the vagina (Workowski and Bachmann Citation2022). Miconazole vaginal cream or vaginal suppositories may be used for self-medication of vulvovaginal candidiasis in otherwise healthy, nonpregnant women who have been previously diagnosed by a clinician and have a recurrence of similar symptoms. When an adequate response is not achieved following a course of miconazole nitrate therapy for vulvovaginal candidiasis or if symptoms recur within two months, appropriate microbiologic studies should be performed to confirm the diagnosis and identify unusual Candida species (e.g. C. glabrata).
Cure rates of 80–95% have been reported in patients receiving the once-daily intravaginal application of miconazole nitrate for two weeks. Randomised clinical trials using miconazole nitrate cream or suppositories have shown that treatment regimens of seven days or longer have cure rates equivalent to 14-day regimens. Clinical studies comparing a seven-day treatment regimen using the vaginal cream with a three-day treatment regimen using the 200 mg vaginal suppositories have shown that the cure rate with the suppository regimen was slightly lower but not statistically different from that with the cream regimen. A seven-day treatment regimen using vaginal cream effectively treats vulvovaginal candidiasis during pregnancy. An observation of using seven-day suppositories combing miconazole 200 mg and metronidazole 750 mg for treating 43 pregnant women at a tertiary hospital in Thailand showed high clinical and microscopic cure rates, at 84.6% and 73.1%, at 2-week follow-ups. Perinatal outcomes were not different from the local background data (Chayachinda Citation2022).
In two comparative studies, 2% miconazole nitrate cream applied intravaginally once daily for two weeks resulted in higher cure rates for vulvovaginal candidiasis than 100,000 units of nystatin inserted intravaginally as tablets once or twice daily for two weeks (Eliot et al. Citation1979, Hoppe Citation1997).
Complicated and recurrent vulvovaginal candidiasis
Up to 75% of women reportedly have at least one episode of vulvovaginal candidiasis, and 40–45% have two or more episodes during their lifetime (Kaur et al. Citation2021, Workowski and Bachmann Citation2022). Still, a small percentage of women (up to 5%) have recurrent vulvovaginal candidiasis (i.e. four or more episodes of symptomatic vulvovaginal candidiasis each year). While certain factors may precipitate a sporadic attack of vulvovaginal candidiasis and have been associated with an increased risk for recurrent vulvovaginal candidiasis (e.g. uncontrolled diabetes mellitus, pregnancy, oral contraceptive use, corticosteroid or other immunosuppressive therapy, immunodeficiency, use of intravaginal sponges or devices, repeated courses of topical or systemic antibacterial agents), these factors are not present in most women who have recurrent episodes (Workowski and Bachmann Citation2022).
Optimum regimens for treating recurrent vulvovaginal candidiasis have not been established yet (Brunton Citation2011). Although each episode caused by C. albicans may respond to usual short-term intravaginal antifungal regimens or a single-dose of oral fluconazole, a more extended initial therapy may be necessary to achieve mycologic remission and chronic maintenance therapy may be required to prevent relapse. The CDC recommends the use of an initial intensive regimen consisting of 7–14 days of an intravaginal azole antifungal or a three-dose regimen of oral fluconazole (100-, 150- or 200 mg dose given every third day for a total of three doses) followed by a maintenance antifungal regimen (issued for six months). The CDC recommends oral fluconazole (100, 150 or 200 mg doses once weekly) for the maintenance regimen. If this oral regimen cannot be used, some clinicians recommend intravaginal clotrimazole (200 mg twice weekly or 500 mg once weekly) or other intravaginal treatments used intermittently. These maintenance regimens can effectively reduce recurrent infections; however, 30–50% of women will have recurrent disease once maintenance therapy is discontinued (Workowski and Bachmann Citation2022).
The response rate to a single-dose antifungal regimen is lower in patients with severe vulvovaginal candidiasis (i.e. extensive vulvar erythema, oedema, excoriation and fissure formation). Either a two-dose regimen of oral fluconazole (150 mg repeated three days later) or 7–14 days of therapy with an intravaginal azole antifungal is recommended for these infections. These more prolonged regimens may also be necessary for treating vulvovaginal candidiasis in women with underlying debilitating medical conditions (e.g. those with uncontrolled diabetes or those receiving corticosteroid therapy) (Workowski and Bachmann Citation2022).
Furthermore, new therapy strategies are currently developed for the treatment of recurrent vulvovaginal candidiasis and tested in clinical trials. Oteseconazole, which is an orally administered, selective inhibitor of the fungal sterol 14-α-demethylase cytochrome P450 (CYP) has been approved by the US Food and Drug Administration (FDA) in 2022 and has been shown to be safe and efficient for the prevention of recurrent vulvovaginal candidiasis (Martens et al. Citation2022). Moreover, ibrexafungerp, the first triterpenoid could be proven to be safe and effective in clinical trials. It is an antifungal targeting the glucan synthase, resulting in a decline of (1,3)-β-glucan polymers, weakening the fungal cell wall which finally results in cell death. It has been demonstrated that ibrexafungerp shows activity against azole- or echinocandin-resistant Candida species, thus it provides a promising new therapy option which is already available on the US market (Schwebke et al. Citation2022). In 2018, a phase II clinical trial was conducted to evaluate the effectiveness of NDV-3A, a fungal immunotherapeutic vaccine regarding the treatment of recurrent vulvovaginal candidiasis. The study proved safety and high immunogenicity of the agent; however, further research in this field is still needed (Edwards et al. Citation2018).
Conclusions
Miconazole nitrate, an imidazole derivative, is a synthetic azole antifungal agent that is structurally related to other imidazole-derivative azole antifungal agents (e.g. butoconazole, clotrimazole, econazole, ketoconazole, oxiconazole, sulconazole and tioconazole).
It has been widely and successfully used for many candidal infections, including vaginal candidiasis with a clinical experience of more than 40 years. Miconazole is a unique option in managing vaginal candidiasis in acute situations for otherwise healthy women and special risk groups.
Besides, several new drugs which are either already on the market or currently investigated are a promising option for the future treatment of vulvovaginal candidiasis. There are lots of innovative agents in the pipeline which will provide a targeted treatment of this common disease. This variety of new treatment options can be combined to standard therapy strategies such as miconazole-treatment and can be used to target even fungal infections that have been resistant to common antifungals.
Ethical approval
Not applicable.
Consent form
Not applicable.
Disclosure statement
P.-A. Regidor is an employee of Exeltis Healthcare.
Santiago Palacios, Manopchai Thamkhantho and Chenchit Chayachinda declare no conflict of interest.
Data availability statement
Not applicable.
Additional information
Funding
References
- Akpan, A. and Morgan, R., 2002. Oral candidiasis. Postgraduate Medical Journal, 78 (922), 455–459.
- Barasch, A. and Griffin, A. V., 2008. Miconazole revisited: new evidence of antifungal efficacy from laboratory and clinical trials. Future Microbiology, 3 (3), 265–269.
- Bassetti, M., Mikulska, M., and Viscoli, C., 2010. Bench-to-bedside review: therapeutic management of invasive candidiasis in the intensive care unit. Critical Care, 14 (6), 244.
- Bennett, J.E., Dolin, R., and Blaser, M.J., 2019. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. 7th ed. Philadelphia: Churchill Livingstone/Elsevier.
- Brunton, L.L., 2011. Goodman & Gilman’s the pharmacological basis of therapeutics. 12th ed. The McGraw-Hill Companies, Inc.
- Casneuf, J., et al., 1980. Oral thrush in children treated with miconazole gel. Mykosen, 23 (2), 75–78.
- Chayachinda, C., 2022. Experience of using the vaginal suppository combining metronidazole and miconazole in Siriraj Hospital. In: Pattanachindakul B, et al., eds. OB-GYN in practice 2022, 303–306.
- Choo, Z.W., et al., 2010. A comparative histopathological study of systemic candidiasis in association with experimentally induced breast cancer. Oncology Letters, 1 (1), 215–222.
- David, L.M., Walzman, M., and Rajamanoharan, S., 1997. Genital colonisation and infection with candida in heterosexual and homosexual males. Genitourinary Medicine, 73 (5), 394–396.
- Doering, P.L. and Santiago, T.M., 1990. Drugs for treatment of vulvovaginal candidiasis: comparative efficacy of agents and regimens. DICP, 24 (11), 1078–1083.
- Donders, G.G., et al., 2002. Definition of a type of abnormal vaginal flora that is distinct from bacterial vaginosis: aerobic vaginitis. British Journal of Gynecology, 109 (1), 34–43.
- Edwards, J.E., Jr., et al., 2018. A fungal immunotherapeutic vaccine (NDV-3A) for treatment of recurrent vulvovaginal candidiasis—a phase 2 randomized, double-blind, placebo-controlled trial. Clinical Infectious Diseases, 66 (12), 1928–1936.
- Eliot, B.W., Howat, R.C., and Mack, A.E., 1979. A comparison between the effects of nystatin, clotrimazole and miconazole on vaginal candidiasis. British Journal of Obstetrics and Gynaecology, 86 (7), 572–577.
- Erdogan, A. and Rao, S.S., 2015. Small intestinal fungal overgrowth. Current Gastroenterology Reports, 17 (4), 16.
- Falagas, M.E., Betsi, G.I., and Athanasiou, S., 2006. Probiotics for prevention of recurrent vulvovaginal candidiasis: a review. Journal of Antimicrobial Chemotherapy, 58 (2), 266–272.
- Ferris, D.G., et al., 2002. Over-the-counter antifungal drug misuse associated with patient-diagnosed vulvovaginal candidiasis. Obstetrics and Gynecology, 99 (3), 419–425.
- Fothergill, A.W., 2006. Miconazole: a historical perspective. Expert Review of anti-Infective Therapy, 4 (2), 171–175.
- Francois, I.E.J.A., et al., 2006. Azoles: mode of antifungal action and resistance development. Effect of miconazole on endogenous reactive oxygen species production in Candida albicans. Anti-Infective Agents in Medicinal Chemistry, 5, 3–13.
- Goehring, R.V., 2008. Mims’ medical microbiology. 4th ed. Mosby Elsevier.
- Hay, R.J., 1996. Yeast infections. Dermatologic Clinics, 14 (1), 113–124.
- Hay, R., 2018. Therapy of skin, hair and nail fungal infections. Journal of Fungi, 4 (3), 99.
- Hidalgo, J.A. and Vazquez, J.A., 2020. Candidiasis: clinical presentation. Medscape. Available from: https://emedicine.medscape.com/article/213853-clinical.
- Hillier, S.L. and Lau, R.J., 1997. Vaginal microflora in postmenopausal women who have not received estrogen replacement therapy. Clinical Infectious Diseases, 25 (Suppl. 2), S123–S126.
- Hoppe, J.E., 1997. Treatment of oropharyngeal candidiasis in immunocompetent infants: a randomized multicenter study of miconazole gel vs. nystatin suspension. The Antifungals Study Group. Pediatric Infectious Disease Journal, 16, 288–293.
- Ivanov, M., Ćirić, A., and Stojković, D., 2022. Emerging antifungal targets and strategies. International Journal of Molecular Sciences, 23 (5), 2756.
- Jartarkar, S.R., et al., 2021. Pathogenesis, immunology and management of dermatophytosis. Journal of Fungi, 8 (1), 39.
- Jurden, L., et al., 2012. Clinical inquiries. Can probiotics safely prevent recurrent vaginitis? Journal of Family Practice, 61 (6), 357, 368.
- Kaur, N., et al., 2021. A review on antifungal efficiency of plant extracts entrenched polysaccharide-based nanohydrogels. Nutrients, 13 (6), 2055.
- Kobayashi, D., et al., 2002. Endogenous reactive oxygen species is an important mediator of miconazole antifungal effect. Antimicrobial Agents and Chemotherapy, 46 (10), 3113–3117.
- Lansdorp, D., et al., 1999. Potentiation of acenocoumarol during vaginal administration of miconazole. British Journal of Clinical Pharmacology, 47 (2), 225–226.
- Lynch, D.P., 1994. Oral candidiasis. History, classification, and clinical presentation. Oral Surgery, Oral Medicine, and Oral Pathology, 78 (2), 189–193.
- Mårdh, P.A., Novikova, N., and Stukalova, E., 2003. Colonisation of extragenital sites by Candida in women with recurrent vulvovaginal candidosis. British Journal of Gynecology, 110 (10), 934–937.
- Martens, M.G., et al., 2022. Phase 3 study evaluating the safety and efficacy of oteseconazole in the treatment of recurrent vulvovaginal candidiasis and acute vulvovaginal candidiasis infections. American Journal of Obstetrics and Gynecology, 227 (6), 880.e1–880.e11.
- Martins, N., et al., 2014. Candidiasis: predisposing factors, prevention, diagnosis and alternative treatment. Mycopathologia, 177 (5–6), 223–240.
- Mulley, A.G. and Goroll, A.H., 2006. Primary care medicine: office evaluation and management of the adult patient. Wolters Kluwer Health.
- Nwokolo, N.C. and Boag, F.C., 2000. Chronic vaginal candidiasis. Management in the postmenopausal patient. Drugs & Aging, 16 (5), 335–339.
- Nyirjesy, P. and Sobel, J.D., 2013. Genital mycotic infections in patients with diabetes. Postgraduate Medicine, 125 (3), 33–46.
- Odds, F.C., 1987. Candida infections: an overview. Critical Reviews in Microbiology, 15 (1), 1–5.
- Patil, S., et al., 2015. Clinical appearance of oral candida infection and therapeutic strategies. Frontiers in Microbiology, 6, 1391.
- Poojary, S.A., 2017. Topical antifungals: a review and their role in current management of dermatophytoses. Clinical Dermatology Review, 1, S24–S29.
- Rachapromma, P. and Chayachinta, C., 2022. Care for women with acute vaginal candidiasis. Siriraj Medical Bulletin, 15 (2), 107–113.
- Redding, S.W., et al., 1999. Epidemiology of oropharyngeal Candida colonization and infection in patients receiving radiation for head and neck cancer. Journal of Clinical Microbiology, 37 (12), 3896–3900.
- Ridzuan, P.M., et al., 2019. Mini review on dermatomycosis. Journal of Science and Mathematics Letters, 8, 6–15.
- Sawyer, P.R., et al., 1975. Miconazole: a review of its antifungal activity and therapeutic efficacy. Drugs, 9 (6), 406–423.
- Saxon, C., et al., 2020. British Association for Sexual Health and HIV national guideline for the management of vulvovaginal candidiasis (2019). International Journal of STD & AIDS, 31 (12), 1124–1144.
- Schiefer, H.G., 1997. Mycoses of the urogenital tract. Mycoses, 40 (Suppl. 2), 33–36.
- Schwebke, J.R., et al., 2022. Ibrexafungerp versus placebo for vulvovaginal candidiasis treatment: a phase 3, randomized, controlled superiority trial (VANISH 303). Clinical Infectious Diseases, 74 (11), 1979–1985.
- Sobel, J.D., 1994. Controversial aspects in the management of vulvovaginal candidiasis. Journal of the American Academy of Dermatology, 31 (3 Pt 2), S10–S13.
- Sobel, J.D., 1997. Vaginitis. New England Journal of Medicine, 337 (26), 1896–1903.
- Sobel, J.D., et al., 1998. Vulvovaginal candidiasis: epidemiologic, diagnostic, and therapeutic considerations. American Journal of Obstetrics and Gynecology, 178 (2), 203–211.
- Srikumar, C. and Nagaraja, H., 2011. A comprehensive review of the occurrence and management of systemic candidiasis as an opportunistic infection. Microbiology Journal, 1, 1–7.
- Thevissen, K., et al., 2007. Miconazole induces changes in actin cytoskeleton prior to reactive oxygen species induction in yeast. Journal of Biological Chemistry, 282 (30), 21592–21597.
- Tobin, M.J., 1995. Vulvovaginal candidiasis: topical vs. oral therapy. American Family Physician, 51 (7), 1715–1720, 1723–1724.
- Vanden Bossche, H., et al., 1990. Saperconazole: a selective inhibitor of the cytochrome P-450-dependent ergosterol synthesis in Candida albicans, Aspergillus fumigatus and Trichophyton mentagrophytes. Mycoses, 33 (7–8), 335–352.
- Vermitsky, J.P., et al., 2008. Survey of vaginal-flora Candida species isolates from women of different age groups by use of species-specific PCR detection. Journal of Clinical Microbiology, 46 (4), 1501–1503.
- Walsh, T.J., et al., 1996. Deep mycoses. In: Baron S, ed. Baron’s medical microbiology. 4th ed. University of Texas Medical Branch.
- Wang, Z.K., et al., 2014. Review article: fungal microbiota and digestive diseases. Alimentary Pharmacology & Therapeutics, 39 (8), 751–766.
- Warren, T.R.N., 2010. Is it a yeast infection? WebMD. Available from: https://www.webmd.com/women/features/is-it-yeast-infection.
- Workowski, K.A. and Bachmann, L.H., 2022. Centers for disease control and prevention’s sexually transmitted diseases infection guidelines. Clinical Infectious Diseases, 74 (74 Suppl. 2), S89–S94.
- Workowski, K.A., et al., 2021. Sexually transmitted infections treatment guidelines, 2021. Morbidity and Mortality Weekly Report. Recommendations and Reports, 70 (4), 1–187.
- Zhang, X., Yin, M., and Zhang, L.J., 2019. Keratin 6, 16 and 17-critical barrier alarmin molecules in skin wounds and psoriasis. Cells, 8 (8), 807.