

Abstract
This nested case-control study aimed to investigate the determinants of low birth weight among newborn babies delivered in Shenzhen, Guangdong, China. We recorded socio-demographic data, health status before pregnancy, pregnancy outcomes and complications in a Shenzhen mother and infant cohort. Among 8951 cases, 401 (4.48%) had low birth weight and 1.65% were full-term with LBW. Maternal body mass index, family income, history of pregnancy, hypertension before pregnancy, vaginal bleeding in 1st trimester, pregnancy-related diabetes, hypertension, placenta previa, placental abruption, premature rupture of membrane, oligohydramnios, and placental types were significantly associated with low birth weight (P < 0.05). In this study, high-risk and mainly preventable factors were linked to low birth weight. Adequate antenatal care, proper maternal nutrition and implementation of proven strategies to prevent high-risk factors may be effective ways to reduce the incidence of low birth weight.
IMPACT STATEMENT
What is already known on this subject? Low birth weight (LBW) is associated with adverse perinatal outcomes and neonatal disease and death. The aim of this study was to investigate the factors affecting low birth weight infants in a developed region in China.
What the results of this study add? According to this study, the incidence of LBW in Shenzhen of China was 4.48%. Maternal body mass index, family income, history of pregnancy, hypertension before pregnancy, vaginal bleeding in 1st trimester, pregnancy-related diabetes, hypertension, placenta previa, placental abruption, premature rupture of membrane, oligohydramnios, and placental types were significantly associated with LBW.
What the implications are of these findings for clinical practice and/or further research? This study suggests that good prenatal care, maternal nutrition and implementation of proven strategies to manage high-risk factors are needed to prevent and reduce the incidence of LBW. Health care providers could use our findings to identify good antenatal care and provide individualised interventions targeting women with risk factors.
Introduction
Extensive research has connected prenatal and postnatal environments to the risk of disease later in adult life (Waterland and Michels Citation2007). Low birth weight (LBW) is defined as less than 2500 g and is associated with a 20-fold increased chance of neonatal mortality (McCormick Citation1985). It is also associated with some types of cancer, disorders in mental health and long-term neurodevelopment (Schieve et al. Citation2016) and increased risk of noncommunicable diseases such as diabetes, hypertension and cardiovascular disease (Grillo et al. Citation2021).
Globally, more than 20 million babies are born each year with LBW, although incidence varies widely between nations and regions (Moradi et al. Citation2021). For most developing countries in Asia, the incidence is between 15% and 20%, and in developed countries, it is 5–7% (https://www.cdc.gov/mmwr/preview/mmwrhtml/00000389.htm). Therefore, the World Health Organisation (WHO) has established a global target to reduce the incidence of LBW by 30% by 2025. As a WHO Member State, China is responsible for meeting this goal.
The health of children has increasingly been a key concern in China since the establishment of the family planning policy in the 1970s, both for individual families as well as the entire society. LBW causes high rates of mortality and morbidity, putting a huge strain on health resources, social services, and families (Petrou Citation2003). As a result, reducing the LBW rate is a critical public health concern in order to avoid immediate negative effects on children.
The purpose of the current study was to identify factors contributing to LBW in China as a basis for the development of sustainable preventive measures to reduce the cost to the health sector. This study, therefore, assessed the socio-demographic, maternal, and obstetric factors associated with LBW babies delivered in Shenzhen, Guangdong, China.
Materials and methods
Sample
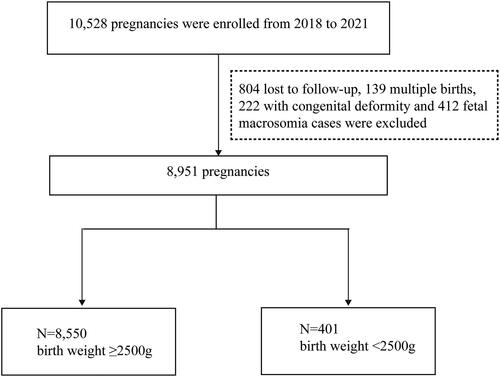
This nested case-control study was conducted in a Shenzhen mother and infant cohort. The first pregnant woman was recruited in Shenzhen centre on April 17th, 2018 and by 31 December, 2021, 10,528 pregnant women had been recruited. We extracted data from the cohort that met the inclusion criteria and excluded 804 lost-to-follow-up, 139 multiple births, 222 with a congenital deformity, and 412 foetal macrosomia cases. As shown in , 8951 cases were finally included, 401 (4.48%) with infant birth weight <2500 g and 8,550 (95.52%) with birth weight ≥2500 g, the latter being allocated to the control group.
Figure 1. Study profile. After pregnancies with loss follow up, multiple births, congenital deformity and foetal macrosomia cases were excluded, a total of 8951 pregnancies with single-term births were analysed in the present study.
Data collection and procedure
Data were collected using a pre-piloted questionnaire which asked mothers about socio-demographic and maternal factors at their first antenatal care visit. Socio-demographic characteristics included information about the mother’s age, ethnicity, maternal education (secondary education or lower, post-secondary education, short-cycle tertiary education, bachelor’s level and master’s or doctoral level), body mass index (BMI), personal income, family income, and place of birth. Maternal variables included the history of pregnancy, history of miscarriage, type of pregnancy (natural or by assisted reproductive technology), age at menarche, regularity of menstrual cycle, health status before pregnancy (hypertension, diabetes, thyroid dysfunction, reproductive tract infection, periodontal disease or fever) and behaviour before pregnancy (history of smoking and intake of alcohol and folic acid). Pregnancy-related symptoms which occurred in the first trimester, including vaginal bleeding, low abdominal pain, morning sickness, or threatened abortion, were also recorded. During the pregnancy, relevant outcomes and complications were extracted from the hospital information system. These included the history of specific diseases during pregnancy (hypertension, diabetes, thyroid dysfunction), polyhydramnios or oligohydramnios, placental abruption, premature rupture of membrane, uterine inertia and cord entanglement. Patients’ diagnoses were made by qualified doctors under strict quality control.
Eligibility criteria
Infants with normal birth weight (NBW; at least 2500 g and less than 4000 g) and gestational age 37–42 weeks were included in the study as controls. Those with birth weights less than 2500 g were allocated to the LBW group. Since LBW does not account for gestational weeks, we included full-term LBW (birth weight <2500 g and gestational age 37–42 weeks).
Exclusion criteria
Newborns of twin or multiple births, and those with congenital deformity or foetal macrosomia were excluded from this study.
Ethical approval and consent to participate
This study was approved by the Medical Ethics Committee of Shenzhen Maternity and Child Healthcare Hospital ([2017]86) and was conducted in accordance with the Declaration of Helsinki. The patients/participants provided their written informed consent to participate in this study.
Data analysis
We used descriptive analysis for the socio-demographic characteristics of the LBW, full-term LBW and NBW (normal birth weight) groups. Continuous variables are described by mean ± standard deviation and median values, and groups were compared using t tests if data were normally distributed, and using Mann–Whitney U tests if not. Categorical variables are reported as numbers and percentages, and Pearson’s Chi-squared test was performed to compare groups. Binary logistic regression analysis was performed to test the association between possible risk factors and LBW. The association between predictor variables and the outcome variable is expressed as crude odds ratio (cOR) with a 95% confidence interval (CI). Subsequently, predictor variables that P < 0.05 in the binary logistic analysis were selected for multivariable logistic analysis. The association between exposure and outcome is expressed as an adjusted odds ratio (aOR) with a 95% confidence interval (CI). A value of P < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 25.0 (SPSS, Chicago, IL, USA).
Results
As shown by , 8951 deliveries were included in our study, of which 401 were cases with LBW, resulting in an incidence rate of 4.48%. Of all cases, 148 (36.9%) were full-term LBW (≥37 weeks).
Maternal socio-demographic characteristics
The incidence rates of LBW associated with maternal socio-demographic characteristics are shown in . BMI, family income and the mother’s birthplace may be regarded as potential risk factors. Almost all mothers (96%) in the LBW and NBW groups were of Han nationality. The average age of pregnant women was 30.9 ± 4.4 years in LBW and 30.8 ± 4.1 in NBW. Almost half (44.2%) in each group were educated to Bachelor’s level. No statistically significant difference was found in maternal age, ethnicity or education level between groups. BMI was 21.2 ± 3.4 in LBW and 21.1 ± 2.8 in NBW, which was statistically significant (P < 0.001) as a categorical variable. However, BMI was 20.5 ± 3.1 in the full-term LBW group, significantly lower than that of the other two groups (P = 0.001). As defined by pre-pregnancy BMI, 1362 (15.2%) women were underweight, 6347 (71.2%) were normal-weight, 1007 (11.3%) were overweight, and 208 (2.3%) were obese. The underweight and obese groups were more likely to have LBW babies and the normal-weight group was more likely to have NBW babies. Family income was significantly different between NBW and both LBW and full-term LBW (P = 0.028 in LBW, P = 0.039 in full-term LBW). Birthplace differed between groups, with 40.6% of mothers of NBW and 51.9% of LBW born in Southern China, and 37.1% of mothers of NBW and 31.9% of LBW in Central China. Mothers born in Southern China were at higher risk of having LBW babies than other groups while those born in Central China were at lower risk (P = 0.001).
Table 1. Socio-demographic characteristics of the mothers delivered at Shenzhen.
Analysis of pre- and during pregnancy maternal variables associated with low birth weight
The results of the univariate and multivariable analysis are presented in . Univariate analysis showed that history of pregnancy, hypertension before pregnancy, vaginal bleeding in 1st trimester, pregnancy-related diabetes and hypertension, placental types, placenta previa, premature rupture of membrane, oligohydramnios and placental abruption may be regarded as possible risk factors of LBW.
Table 2. Results of univariate and multivariate logistic regression analysis of LBW newborns born in Shenzhen.
Multivariable logistic regression analysis showed that the risk of LBW in mothers with a history of pregnancy was about 1.5 times higher than that in mothers without such history [aOR = 1.375, CI 95% (1.115, 1.696)]. The odds of LBW were 1.6 times higher among mothers with vaginal bleeding in their first trimester than those without [aOR = 1.561, CI 95% (1.255, 1.942)]. The risk of LBW was significantly higher in mothers with than without pre-pregnancy hypertension [aOR = 3.704, CI 95% (1.238, 11.083)], while its risk in mothers with pregnancy-induced hypertension was almost 3 times higher [aOR = 2.491, CI 95% (1.454, 4.270)]. Furthermore, regarding gestational complications, mothers who had pregnancy-related diabetes had an increased risk of having LBW babies [aOR = 1.368, CI 95% (1.055, 1.773)]. The incidence of LBW among mothers with adverse perinatal outcomes was increased by about 2 to 8 times (placenta previa aOR = 7.795, CI 95% (4.153, 14.634); placental abruption aOR = 7.486, CI 95% (4.909, 11.415); premature rupture of membrane aOR = 1.841, CI 95% (1.479, 2.293); and oligohydramnios aOR = 4.094, CI 95% (2.311, 7.250)). Further, mothers with abnormal placenta were 4 times more likely to deliver an infant with LBW [aOR = 3.748, CI 95% (2.351, 5.973)].
Analysis of risk factors associated with full-term low birth weight
shows the results of the analysis of data from the full-term LBW group to explore whether the risk factors were associated with gestational age. After excluding skewed data on “diabetes before pregnancy” and “polyhydramnios”, maternal smoking, history of pregnancy, hypertension during pregnancy, placental types, placenta previa, oligohydramnios and placental abruption were associated with a significantly increased risk of full-term LBW (P < 0.05).
Table 3. Results of univariate and multivariate logistic regression analysis of full-term LBW newborns born in Shenzhen.
Discussion
This study based in Shenzhen, China, reveals a significant relationship between LBW and maternal BMI, family income, history of pregnancy, hypertension before pregnancy, vaginal bleeding in 1st trimester, pregnancy-related diabetes and hypertension, placenta previa, placental abruption, premature rupture of membrane, oligohydramnios, and placental types.
Our findings on BMI and LBW are consistent with those of previous studies (Liu et al. Citation2012, Zhao et al. Citation2018, Xie et al. Citation2021, Waits et al. Citation2021) including systematic reviews (Liu et al. Citation2019) based in China and other countries (Nakanishi et al. Citation2022, Khazaei et al. Citation2021). The present study found that underweight women accounted for 15.2% of LBW in Shenzhen, somewhat higher than China’s average of 11.0%. A significant association was also found between LBW and mothers born in Southern China. The staple food in these regions is rice, which is a lower-energy food compared with wheat, and a negative association has been found between a rice-based dietary pattern and BMI (Shi et al. Citation2011), people who eat rice tend to have reduced obesity (Zhang et al. Citation2008). Shenzhen is a highly urbanised city with an immigrant population. Most of Shenzhen’s young women are white-collar workers, highly educated and employed. Exercise and a rice-based dietary pattern are the key reasons for underweight among young Chinese women (Xie et al. Citation2021). Underweight women may have a smaller uterus and reduced blood flow, which limits the growth of the uterus, placenta and foetus directly (Xie et al. Citation2021).
The present study revealed that family income is a risk factor associated with LBW. However, it has been suggested that since low-income women live in adverse social circumstances their socioeconomic status and lifestyle may lead to the birth of LBW infants (Starfield et al. Citation1991). Dadi et al. (Citation2020) argued that antenatal depression is a risk factor for low birth weight, while economic factors such as financial difficulties increase the probability of depression during pregnancy.
This study also found that mothers with a history of pregnancy had higher odds of having LBW babies, consistent with the results of Indian studies in which the prevalence of LBW declined among subsequent pregnancies (Starfield et al. Citation1991, Weiss et al. Citation2004). While most mothers had a history of pregnancy, they may have a higher incidence of labour complications due to advanced maternal age increasing the likelihood of delivering a baby with LBW.
The likelihood of LBW was also increased with vaginal bleeding in the first trimester, a common complication of pregnancy, with a frequency of 16 to 25% (Bondick et al., Citation2022). Despite its frequency, the risk of adverse outcomes in pregnancies with first-trimester vaginal bleeding remains unclear. Weiss et al. (Citation2004) found that first-trimester vaginal bleeding was an independent risk factor for adverse obstetric outcomes in a population-based screening study of 16,506 patients. Some previous studies have shown a connection between vaginal bleeding during early pregnancy and preterm delivery (Liu et al. Citation2021a, Hackney and Glantz Citation2011). Vaginal bleeding can cause maternal stress and anxiety, which is linked to a poor pregnancy outcome, and may suggest underlying placental dysfunction, such as altered trophoblast invasion and angiogenesis (Şükür et al. Citation2014). In addition, underlying placental dysfunction may present as preeclampsia, placental abruption, and premature rupture of membranes (PROM).
The present results show that hypertensive disorders may lead to the birth of LBW newborns, consistent with the results of other studies (Velentgas et al. Citation1994, Liu et al. Citation2021c). Reduction in utero-placental perfusion is the most typical pathophysiologic mechanism of LBW (Jung et al. Citation2022). Hypertensive disorders are characterised by both endothelial dysfunction and reduced blood placental perfusion (Agrawal and Wenger Citation2020). It has generally been observed that women with chronic hypertension have a high risk of preeclampsia compared to those without hypertension (Bartsch et al. Citation2016, Ogunwole et al. Citation2021). Impaired uteroplacental perfusion results in foetal growth restriction due to reduced oxygen and nutrition transport to the embryo. Uteroplacental ischaemia via maternal syncytiotrophoblast stress may be the aetiology of preeclampsia (Jung et al. Citation2022). More attention should be paid to the intrauterine growth of the foetus and the development of anomalies in mothers with hypertensive disorders or preeclampsia.
The present study found a relationship between gestational diabetes mellitus (GDM) and LBW, but not full-term LBW. GDM has been linked to an increased risk of adverse outcomes such as preterm delivery, caesarean‐section (C‐section) delivery, preeclampsia, macrosomia and intrauterine growth retardation (Damm et al. Citation2016) but its correlation with LBW is contentious. A prospective cohort study including 3,126 women found a positive correlation between GDM and adverse outcomes, but insufficient gestational weight gain in GDM women did not increase the risk of LBW (Zheng et al. Citation2021). Considering the present results in full-term LBW, GDM may influence birth weight by increasing the incidence of iatrogenic preterm birth. These findings suggest that GDM may operate as a risk enhancer rather than being a direct risk factor.
Our results showed that an abnormal placenta significantly increased the probability of LBW. This condition includes bilobed, succenturiate, circumvallate, membranous, ring-shaped, and marginate placentas (Rathbun and Hildebrand Citation2022). Changes in placental shape with reduced placental efficiency may be more common in pregnancies with adverse outcomes such as LBW births (Salafia et al. Citation2010, Cotter et al. Citation2014, Nigam et al. Citation2014). Placental histopathology suggests that maldevelopment of the placenta, placental under-perfusion, and epigenetic modulation lead to placental dysfunction and LBW (Longtine and Nelson Citation2011, Nigam et al. Citation2014). The clinically, placental abnormality may be associated with vaginal bleeding; preterm delivery, PROM, placenta previa and placenta accrete.
In the present study, the frequency of LBW was significantly increased in mothers with a diagnosis of placenta previa, consistent with some previous findings (Moeini et al. Citation2021) in which placenta previa with abnormal placentation occurs more frequency in LBW than in controls. Antepartum haemorrhage is attributed to placenta previa (Crane et al. Citation2000) and leads to maternal anaemia, which has been linked with an increased risk of delivering LBW babies (Figueiredo et al. Citation2019) due to reduced oxygen-carrying capacity (Savaliya et al. Citation2021). Furthermore, placenta previa is an independent risk factor for the placenta accreta spectrum (Liu et al. Citation2021b). The abnormal attachment of the placenta causes dysfunction of maternal vascular remodelling and may result in LBW. Placenta previa is therefore also an important independent risk factor for preterm infant birth (Huang et al. Citation2021). The routine strategy for high-risk pregnancies such as women with placenta previa and other maternal comorbidities is iatrogenic preterm birth, however preterm delivery such as emergency caesarean delivery is linked with LBW. Consistent with this, the present results suggest an overall higher rate of LBW for women with placenta previa.
In the present study, a correlation was found between placental abruption and both LBW and full-term LBW. To the best of our knowledge, placental abruption is a major cause of neonatal outcomes such as perinatal asphyxia, stillbirth, prematurity, and maternal complications including risk for haemorrhage, disseminated intravascular coagulation, and even death (Schmidt et al. Citation2022). However, few studies have focussed on placental abruption and LBW directly. Mavedatnia et al. (Mavedatnia et al. Citation2021) found no direct interaction between birthweight and placental abruption but concluded that prematurity and birthweight were the main mediators of lower Apgar scores and intensive care admission (Kramer et al. Citation1997). Moreover, pregnancy-induced hypertension is regarded as an important risk factor for placental abruption (Kramer et al. Citation1997, Khan et al. Citation2022). Placental calcification leads to preeclampsia, which eventually accounts for decreased uteroplacental blood flow and LBW (Khan et al. Citation2022, Dash et al. Citation2021).
Previous results have shown a doubling of LBW incidence in PROM, with an increased risk of prematurity (Miller and Jekel Citation1989). In the present study, no association was found between PROM and full-term LBW, suggesting that PROM affected LBW indirectly via prematurity.
Oligohydramnios was a risk factor for LBW in the present study, consistent with a prior study (Chen et al. Citation2013) in which a low amniotic fluid index was a significant independent predictor of low birth weight. Although the mechanism of oligohydramnios is unclear, it has been considered a symptom of placental dysfunction, which may cause foetal anoxia and result in LBW. We also found that maternal smoking was associated with full-term LBW, and this is a well-known maternal and foetal health risk (2020), reducing placental transmission of blood, oxygen, and nutrients, resulting in foetal hypoxia and LBW.
The incidence of LBW in the present study was lower than the average level in China but similar to that in developed countries. This may be explained by the fact that Shenzhen is an economic zone of China with high urbanisation and an immigrant city with large population mobility, where the population is very young with high education and is attentive to prenatal care and enjoys advanced health care facilities (Ma et al. Citation2020). Besides, to reduce the morbidity of LBW, good prenatal care, proper maternal nutrition and implementation of proven strategies to prevent high-risk factors are essential.
This study identified several factors associated with LBW, even in an economically developed city in China. In view of the prognosis and long-term complications of LBW, good prenatal care, maternal nutrition and implementation of proven strategies to manage high-risk factors are needed to prevent and reduce the incidence of LBW. Our findings provide new insights into preventative strategies to reduce the morbidity of LBW and achieve the WHO global health target by 2025. Healthcare providers could use these findings to identify good antenatal care and provide individualised interventions targeting women with risk factors.
Strengths and limitations
A strength of this study is its setting in the Shenzhen Maternity and Child Healthcare Hospital, a maternal and neonatal intensive care unit which serves over 1.8 million people annually and with access to detailed birth data. Thus, the results in this study may accurately reflect the situation in the Shenzhen population. The prospective nature of the study allowed risk factors to be accurately recorded and recall bias to be minimised.
As well as being a strength, the location of the study is a limitation, since Shenzhen differs from other regions in terms of cultural and socio‑economic factors. Therefore, the findings of this study may have limited generalisability beyond Shenzhen.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Not applicable.
Additional information
Funding
References
- 2020. Tobacco and nicotine cessation during pregnancy: ACOG committee opinion summary, number 807. Obstet Gynecol, 135, 1244–1246.
- Agrawal, A. and Wenger, N. K., 2020. Hypertension during pregnancy. Current Hypertension Reports, 22 (9), 64.
- Bartsch, E., et al., 2016. Clinical risk factors for pre-eclampsia determined in early pregnancy: systematic review and meta-analysis of large cohort studies. BMJ, 353, i1753.
- Bondick, C. P., Das, J. M., and Fertel, H., 2022. Subchorionic hemorrhage. StatPearls. Treasure Island (FL): StatPearls Publishing, 2.
- chen, Y., et al., 2013. An epidemiological survey on low birth weight infants in China and analysis of outcomes of full-term low birth weight infants. BMC Pregnancy and Childbirth, 13 (1), 242.
- Cotter, S. L., et al., 2014. A stochastic model for early placental development. Journal of the Royal Society Interface, 11 (97), 20140149.
- Crane, J. M., et al., 2000. Maternal complications with placenta previa. American Journal of Perinatology, Volume 17 (Number 02), 101–106.
- Dadi, A. F., et al., 2020. Global burden of antenatal depression and its association with adverse birth outcomes: an umbrella review. BMC Public Health, 20 (1), 173.
- Damm, P., et al., 2016. Gestational diabetes mellitus and long-term consequences for mother and offspring: a view from Denmark. Diabetologia, 59 (7), 1396–1399.
- Dash, S., et al., 2021. Perinatal outcomes in premature placental calcification and the association of a color doppler study: report from a tertiary care hospital in eastern India. Clinics and Practice, 11 (4), 841–849.
- Figueiredo, A., et al., 2019. Maternal anemia and birth weight: A prospective cohort study. PLoS One, 14 (3), e0212817.
- Grillo, M. A., Mariani, G. and Ferraris, J. R., 2021. Prematurity and low birth weight in neonates as a risk factor for obesity, hypertension, and chronic kidney disease in pediatric and adult age. Frontiers in Medicine, 8, 769734.
- Hackney, D. N. and Glantz, J. C., 2011. Vaginal bleeding in early pregnancy and preterm birth: systemic review and analysis of heterogeneity. The Journal of Maternal-Fetal & Neonatal Medicine, 24 (6), 778–786.
- Huang, L., et al., 2021. Iatrogenic factors contributed to the high rate of preterm birth in a community hospital. Translational Pediatrics, 10 (10), 2602–2613.
- Jung, E., et al., 2022. The etiology of preeclampsia. American Journal of Obstetrics and Gynecology, 226 (2S), S844–s866.
- Khan, S., et al., 2022. Frequency of abruption placenta in women with pregnancy-induced hypertension. Cureus, 14 (1), e21524.
- Khazaei, Z., et al., 2021. Risk factors associated with low birth weight among infants: a nested case-control study in southeastern Iran. International Journal of Preventive Medicine, 12, 159.
- Kramer, M. S., et al., 1997. Etiologic determinants of abruptio placentae. Obstetrics and Gynecology, 89 (2), 221–226.
- Liu, L., et al., 2019. Maternal body mass index and risk of neonatal adverse outcomes in China: a systematic review and meta-analysis. BMC Pregnancy and Childbirth, 19 (1), 105.
- Liu, S., et al., 2021a. Study on the correlation between vaginal bleeding in first trimester and preterm birth: A birth cohort study in Lanzhou, China. Journal of Obstetrics and Gynaecology Research, 47 (6), 1997–2004.
- Liu, X., et al., 2021b. What we know about placenta accreta spectrum (PAS). European Journal of Obstetrics, Gynecology, and Reproductive Biology, 259, 81–89.
- Liu, Y., et al., 2012. Prepregnancy body mass index and gestational weight gain with the outcome of pregnancy: a 13-year study of 292,568 cases in China. Archives of Gynecology and Obstetrics, 286 (4), 905–911.
- Liu, Y., et al., 2021c. Impact of gestational hypertension and preeclampsia on low birthweight and small-for-gestational-age infants in China: A large prospective cohort study. Journal of Clinical Hypertension (Greenwich, Conn.), 23 (4), 835–842.
- Longtine, M. S. and Nelson, D. M., 2011. Placental dysfunction and fetal programming: the importance of placental size, shape, histopathology, and molecular composition. Seminars in Reproductive Medicine, 29 (3), 187–196.
- Ma, R., et al., 2020. Ten-year time trends in preterm birth during a sociodemographic transition period: a retrospective cohort study in Shenzhen, China. BMJ Open, 10 (10), e037266.
- Mavedatnia, D., et al., 2021. Impact of co-existing placental pathologies in pregnancies complicated by placental abruption and acute neonatal outcomes. J Clin Med, 10 (23), 5693.
- Mccormick, M. C., 1985. The contribution of low birth weight to infant mortality and childhood morbidity. New England Journal of Medicine, 312 (2), 82–90.
- Miller, H. C. and Jekel, J. F., 1989. Epidemiology of spontaneous premature rupture of membranes: factors in pre-term births. Yale Journal of Biology and Medicine, 62 (3), 241–251.
- Moeini, R., et al., 2021. Maternal and neonatal outcomes of abnormal placentation: a case-control study. The Journal of Maternal-Fetal & Neonatal Medicine, 34 (19), 3097–3103.
- Moradi, G., et al., 2021. Maternal risk factors for low birth weight infants: A nested case-control study of rural areas in Kurdistan (western of Iran). Journal of Preventive Medicine and Hygiene, 62 (2), E399–e406.
- Nakanishi, K., et al., 2022. Severity of low pre-pregnancy body mass index and perinatal outcomes: the Japan environment and Children’s Study. BMC Pregnancy and Childbirth, 22 (1), 121.
- Nigam, J., et al., 2014. Histopathological study of placentae in low birth weight babies in India. Annals of Medical and Health Sciences Research, 4 (Suppl 2), S79–S83.
- Ogunwole, S. M., et al., 2021. preeclampsia across pregnancies and associated risk factors: findings from a high-risk US Birth Cohort. Journal of the American Heart Association., 10, e019612.
- Petrou, S., 2003. Economic consequences of preterm birth and low birthweight. Bjog: An International Journal of Obstetrics and Gynaecology, 110 (Suppl 20), 17–23.
- Rathbun, K. M. and Hildebrand, J. P., 2022. Placenta abnormalities. StatPearls. Treasure Island (FL): StatPearls Publishing, 4–7.
- Salafia, C. M., et al., 2010. Placental surface shape, function, and effects of maternal and fetal vascular pathology. Placenta, 31 (11), 958–962.
- Savaliya, K., et al., 2021. Multigravida women with moderate to severe anaemia in third trimester: fetomaternal outcomes. Cureus, 13 (12), e20493.
- Schieve, L. A., et al., 2016. Population impact of preterm birth and low birth weight on developmental disabilities in US children. Annals of Epidemiology, 26 (4), 267–274.
- Schmidt, P., Skelly, C. L. and Raines, D. A., 2022. Placental abruption. StatPearls. Treasure Island (FL): StatPearls Publishing, 12–14.
- shi, Z., et al., 2011. Dietary pattern and weight change in a 5-year follow-up among Chinese adults: results from the Jiangsu Nutrition Study. British Journal of Nutrition, 105 (7), 1047–1054.
- Starfield, B., et al., 1991. Race, family income, and low birth weight. American Journal of Epidemiology, 134 (10), 1167–1174.
- ŞüKüR, Y. E., et al., 2014. The effects of subchorionic hematoma on pregnancy outcome in patients with threatened abortion. Journal of the Turkish German Gynecological Association, 15 (4), 239–242.
- Velentgas, P., Benga-DE, E. and Williams, M. A., 1994. Chronic hypertension, pregnancy-induced hypertension, and low birthweight. Epidemiology, 5 (3), 345–348.
- Waits, A., Guo, C. Y. and Chien, L. Y., 2021. Inadequate gestational weight gain contributes to increasing rates of low birth weight in Taiwan: 2011–2016 nationwide surveys. Taiwanese Journal of Obstetrics & Gynecology, 60 (5), 857–862.
- Waterland, R. A. and Michels, K. B., 2007. Epigenetic epidemiology of the developmental origins hypothesis. Annual Review of Nutrition, 27, 363–388.
- Weiss, J. L., et al., 2004. Threatened abortion: A risk factor for poor pregnancy outcome, a population-based screening study. American Journal of Obstetrics and Gynecology, 190 (3), 745–750.
- Xie, D., et al., 2021. Effects of pre-pregnancy body mass index on pregnancy and perinatal outcomes in women based on a retrospective cohort. Scientific Reports, 11 (1), 19863.
- Zhang, X., et al., 2008. Consumption and corpulence in China: A consumer segmentation study based on the food perspective. Food Policy., 33 (1), 37–47.
- Zhao, R., et al., 2018. Maternal pre-pregnancy body mass index, gestational weight gain influence birth weight. Women and Birth: journal of the Australian College of Midwives, 31 (1), e20–e25.
- Zheng, W., et al., 2021. Weight gain after diagnosis of gestational diabetes mellitus and its association with adverse pregnancy outcomes: a cohort study. BMC Pregnancy and Childbirth, 21 (1), 216.