

Abstract
Severe pre-eclampsia is a leading cause of maternal and perinatal morbidity and mortality. This retrospective study explored pregnancy outcome predictive values of umbilical artery Doppler with serum adiponectin in severe pre-eclampsia. Fasting elbow venous blood was collected from 118 severe pre-eclampsia patients [maternal systolic pressure ≥ 160 mmHg and/or diastolic pressure ≥ 110 mmHg + minimal proteinuria, 56; mild hypertension + heavy proteinuria (≥2 g/24 h or random urinary protein ≥ 2+), 42; no proteinuria but new-onset hypertension + diseases of heart/lung/liver/kidney/other organs or abnormalities in blood/digestive/nervous systems, placental foetus involved, 20] and 90 controls (18.5-24.9 kg/m2) in the first morning of admission. Serum adiponectin and resistance/pulsatility indexes were separately measured and correlatively analysed by Pearson’s coefficient analysis. Adverse outcomes included maternal primary postpartum haemorrhage and placental abruption, neonatal asphyxia, low birth weight, foetal distress, foetal growth restriction. In severe pre-eclampsia, serum adiponectin (downregulated) was negatively-correlated with resistance/pulsatility indexes (upregulated). The area under the curve of umbilical artery Doppler with serum adiponectin for predicting adverse outcomes of severe pre-eclampsia was 0.6545 (specificity 60.27%, sensitivity 60.00%). In conclusion, umbilical artery Doppler with serum adiponectin predicts adverse pregnancy outcomes in severe pre-eclampsia.
What is already known on this subject? Sad levels were lowered in sPE patients. UA ultrasound hemodynamic parameters can predict adverse pregnancy outcomes.
What do the results of this study add? Our study revealed that ultrasonic hemodynamic indexes of UA combined with Sad levels had better efficacy in predicting pregnancy outcomes in patients with sPE, and our study is expected to improve the accuracy of clinical prediction of adverse outcomes in sPE patients.
What are the implications of these findings for clinical practice and/or further research? Through the combined detection of multiple indicators of the foetus in the mother, our study expects to be able to monitor and predict the growth of the foetus in the mother more accurately in clinical practice, avoid excessive intervention or untimely intervention, and reduce the incidence of perinatal adverse pregnancy outcomes.
Impact statement
Introduction
Pre-eclampsia (PE) was defined according to the guidelines of American College of Obstetricians and Gynecologists as gestational hypertension (systolic blood pressure > 140 mmHg and/or diastolic blood pressure > 90 mmHg on at least two occasions after gestational week 20), with the accompaniment of proteinuria (> 0.3 g/24 h), and severe pre-eclampsia (sPE) was defined as blood pressure above 160 mmHg systolic and/or 110 mmHg diastolic or proteinuria > 5 g/24 h or oliguria (< 500 ml urine/24 h) (Azizi et al. Citation2017). As a gestational hypertension, sPE affects 2% to 8% of pregnancies worldwide and causes significant maternal and perinatal morbidity and mortality (Ives et al. Citation2020, Mirkovic et al. Citation2020). Nevertheless, the pathogenesis of sPE is unknown, and there is no effective intrauterine therapy to treat it so far (Wang et al. Citation2022). Consequently, finding effective methods to predict adverse pregnancy outcomes of sPE, identify high-risk populations, and conduct targeted prenatal monitoring, is an effective means to reduce the prevalence of sPE (Poon et al. Citation2019).
Considerable hemodynamic changes can occur during the course of gestation and the maternal hemodynamic profile is of great importance to the treatment of hypertension in PE (Masini et al. Citation2022). As one of the key factors to protect the intrauterine environment, maternal uterine arterial blood flow is essential for the maintenance of normal placental function and foetal growth and development, and hemodynamic ultrasound can predict pregnancy outcomes in PE patients and provide theoretical support to reduce adverse pregnancy outcomes (Ridder et al. Citation2019, Zhu et al. Citation2022). With the continuous development of imaging technology, colour Doppler ultrasound has been widely used in prenatal diagnosis and hemodynamic examination as a non-invasive method (Rossi and Prefumo Citation2017). Colour Doppler ultrasound can distinguish the hemodynamic changes in the maternal umbilical artery (UA), uterine artery, middle cerebral artery, and venous catheter (Cornette et al. Citation2016). Pregnant women with early sPE often experience reduced blood flow to UA, and increased blood flow resistance (Hosapatna Basavarajappa et al. Citation2020, Melchiorre et al. Citation2020, Perdios et al. Citation2021). Fortunately, colour Doppler ultrasound can detect elevated UA-systolic/diastolic blood pressure values, which affect normal foetal development (Wang et al. Citation2022). Additionally, the clinical value of UA Doppler has demonstrated clinical values and is one of the few interventions to reduce perinatal mortality in high-risk pregnancies (Alfirevic et al. Citation2015, 2017). More importantly, foetal UA Doppler is a preferential indicator for adverse birth outcomes in severe late-onset PE (Moawad et al. Citation2022). Nevertheless, given that the ultrasound imaging effect and subjective diagnosis of foetal ultrasound images by different medical personnel in clinical diagnosis (different measurements can be made on the same object) remain unsatisfying, it is very crucial to find a more efficient way to diagnose sPE.
Adiponectin is the most abundant peptide secreted by fat cells, whose reduction plays an essential role in obesity-related diseases such as insulin resistance, type 2 diabetes, and cardiovascular disease (Achari and Jain Citation2017). In addition, adiponectin is considered a protective factor for insulin resistance and vascular disease, and abnormal fluctuations of serum adiponectin (Sad) are observed in patients with PE (Dong et al. Citation2018). Meanwhile, adiponectin regulates placentation and proteinuria in PE and affects the foetal-maternal interface, and its level decreases physiologically with pregnancy progression (Adu-Gyamfi et al. Citation2020). Thagaard et al. (Citation2019) pointed out that the risk of pre-eclampsia in obese pregnant women is significantly higher than that in normal pregnant women, and the Sad content in severely obese pregnant women is the lowest, while Sad has good diagnostic values in moderately and severely obese pregnant women. Besides, a recent study has revealed the predictive and diagnostic value of Sad in intrahepatic cholestasis during pregnancy (Yurtcu et al. Citation2022). Notably, maternal Sad levels are shown to be potential biomarkers for PE (Rao et al. Citation2021). In a diabetic model of hypertensive rats, researchers have identified certain association between adiponectin and renal haemodynamics (Afzal et al. Citation2020). Yet, the correlation of UA Doppler parameters with Sad levels in sPE patients has not been reported.
In the present study, adverse pregnancy outcomes were defined as maternal primary postpartum haemorrhage and placental abruption, neonatal asphyxia, low birth weight, foetal distress, and foetal growth restriction (FGR) (Gottardi et al. Citation2021, Takahashi et al. Citation2018). Specifically, placental abruption refers to uterine bleeding greater than usual in the absence of placenta previa or trauma (related to contractions, non-reassuring foetal heart tones and/or clinical diagnosis of abruption) resulting in delivery (Tita et al. Citation2022). FGR represents a birth weight measuring under the 10th percentile for gestational age and infant sex according to the Duryea population standard and a small-for-gestational-age birth weight measuring under the 5th percentile (Duryea et al. Citation2014, Tita et al. Citation2022). Hence, this study recruited 118 sPE patients and 90 normal pregnant women and collected their clinical information and blood samples to analyse the expression of Sad and its correlation with Doppler parameters, in anticipation of predicting pregnancy outcomes in sPE patients.
Materials and methods
Ethics statement
The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Nanchang University (Approval number: 20191022, Date: 2019.11.08). All participants voluntarily signed the informed consent.
Study subjects
All 525 PE patients underwent antepartum examination, were diagnosed with sPE and gave birth in the First Affiliated Hospital of Nanchang University from January 2020 to June 2021, including 341 non-sPE patients and 184 sPE patients. Finally, 118 sPE patients were recruited according to the inclusion and exclusion criteria and patients with other pregnancy complications were excluded by clinical examination. Meanwhile, 90 normal pregnant women undergoing physical examination in the same period were randomly selected as controls.
Inclusion criteria: (1) all patients fell within the normal body mass index (BMI) range (18.5-24.9 kg/m2) (Thagaard et al. Citation2019); (2) all patients accorded with the diagnosis criteria of PE; (3) all patients were in singleton pregnancies; (4) all patients had no history of essential hypertension, kidney disease, and diabetes; (5) all patients had complete information, including test results of proteinuria. Exclusion criteria: (1) patients were in multiple pregnancies; (2) patients had essential hypertension, kidney disease, and diabetes; (3) patients had spontaneous discharge or were lost to follow-up and had no record of delivery; (4) patients had incomplete laboratory and auxiliary examination data.
The diagnostic criteria of sPE were as follows: maternal systolic blood pressure was ≥ 160 mmHg and (or) diastolic blood pressure was ≥110 mmHg and accompanied by mild proteinuria, or mild hypertension was accompanied by severe proteinuria (≥ 2 g/24 h or random urine protein ≥ 2+), or new-onset hypertension in the absence of proteinuria was accompanied by any of the diseases and abnormalities involving the following vital organs or system: heart, lung, liver, and kidney, or blood system, digestive system, nervous system, and placental involvement.
Among the enrolled sPE patients, 56 cases were with maternal systolic pressure ≥160 mmHg and/or diastolic pressure ≥110 mmHg accompanied by minimal proteinuria, 42 cases were with mild hypertension accompanied by heavy proteinuria (≥2 g/24 h or random urinary protein ≥2+), and 20 cases were with no proteinuria but new-onset hypertension accompanied by any diseases of heart, lung, liver, kidney and other organs or abnormalities in the blood, digestive or nervous systems, placental foetus involved. The elbow venous blood was collected from pregnant women (after 8-10 h of continuous fasting) on the morning of the first day of admission and centrifuged at 2000 g for 10 minutes at 4 °C. Then, the supernatants were transferred to eppendorf tubes and stored at −80 °C. Prior to this study, the sample had not undergone any freeze-thaw cycle. The adverse pregnancy outcomes were recorded.
Enzyme-linked immunosorbent assay (ELISA)
According to the manufacturer’s instructions, Sad concentrations were determined using an ELISA kit (DRG International, Marburg, Germany). The detection limit of Sad was 0.026 µg/mL with intra- and inter-assay coefficient of variation (CV) < 7.0%.
Colour Doppler ultrasonography
Doppler examinations were carried out with the patients placed in a recumbent or semirecumbent position. Toshiba Eccocee SSA-340 (Toshiba, Otaware, Japan), Acuson 128 XP, and Acuson Sequoia (Acuson, CA, USA) ultrasound machines, equipped with pulsed and colour Doppler options were used. The high-pass filter was set at 100 Hz and the pulsed Doppler gate was selected according to the diameter of the vessel examined
Statistical analysis
Data were subjected to analysis and plotting utilising SPSS21.0 statistical software (IBM Corp., Armonk, NY, USA) and GraphPad Prism 6.0 software (GraphPad Software Inc., San Diego, CA, USA). Normal distribution was verified by Shapiro-Wilk test. Normally distributed measurement data were depicted in the form of mean ± standard deviation (SD). The independent sample t-test was adopted for pairwise comparisons, and Mann-Whitney U test was used for data comparison between two groups. Counting data were represented as the number of cases, and the chi-square test was used for data comparison between two groups. sPE adverse pregnancy outcomes were analysed using receiver operating characteristic (ROC) curves. The P value was derived from two-sided tests. The difference was regarded as statistically significant when p < 0.05.
Results
Clinical baseline characteristics
A total of 118 sPE patients and 90 healthy subjects were recruited. The age of sPE patients was 29.19 ± 1.61 years, and gestational age at delivery was 33.98 ± 2.79 weeks. The age of healthy controls was 29.53 ± 1.65 years and gestational age at delivery was 34.17 ± 3.94 weeks. Their basic information is shown in . The results showed that there were no significant differences in age, BMI, gestational age, and placental weight between the two groups (all P > 0.05); there were significant differences in mean arterial pressure, serum calcium level, platelet, urinary protein, BMI at delivery, and infant birth weight (all P < 0.01). Meanwhile, relative to the control group, pulsatility index (PI), and resistance index (RI) values in the sPE group were visibly increased (all P < 0.001).
Table 1. Comparative analysis of baseline clinical data from sPE patients and healthy subjects.
Sad was poorly expressed in sPE patients
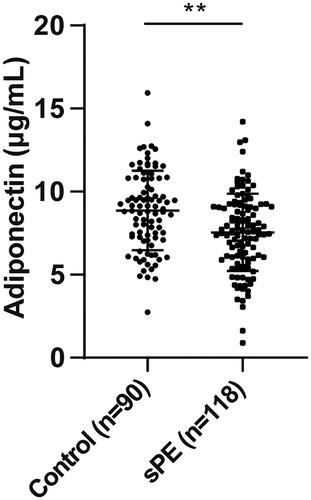
Subsequently, the Sad levels in sPE patients and control subjects were determined by ELISA. The results displayed that the Sad level in sPE patients (7.55 ± 2.32 μg/mL) was markedly lower than that in healthy controls (8.86 ± 2.38 μg/mL) (P < 0.01) ().
Figure 1. Sad levels were reduced in sPE patients. The Sad levels in sPE patients and control subjects were determined by ELISA. Data were described as mean ± SD. The independent sample t test was used to compare difference between groups. ** P < 0.01.
Correlation analysis of ultrasonic hemodynamic parameters of umbilical artery and Sad level in sPE patients
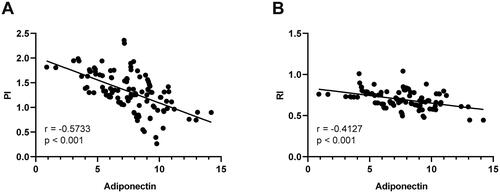
Furthermore, Pearson’s coefficient analysis was adopted to evaluate the correlation between ultrasonic hemodynamic parameters of umbilical artery (PI and RI) and Sad levels in sPE patients. It was discovered that the Sad level in sPE patients was negatively correlated with PI (r = −0.5733, p < 0.001) and RI (r = −0.4127, p < 0.001) ().
Figure 2. Correlation analysis of ultrasonic hemodynamic parameters of UA (PI and RI) and Sad level in sPE patients. Pearson method was used to analyse (A) the correlation between PI and Sad level in sPE patients, and (B) the correlation between RI and Sad level.
Ultrasonic hemodynamic parameters of umbilical artery combined with Sad level in sPE patients were utilised to evaluate adverse pregnancy outcomes
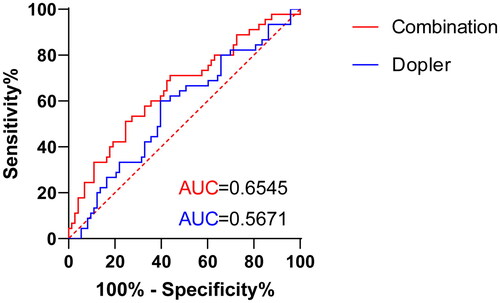
Next, we used the ROC curve to analyse the prognostic value of ultrasonic hemodynamic parameters of umbilical artery (PI and RI) and ultrasonic hemodynamic parameters of umbilical artery combined with Sad for adverse pregnancy outcomes in sPE patients. The area under the ROC curve (AUC) of ultrasonic hemodynamic parameters of umbilical artery for predicting adverse pregnancy outcomes in sPE patients was 0.5671, with a cut-off value of 0.4822 and 56.16% specificity and 71.11% sensitivity. The AUC of ultrasonic hemodynamic parameters of umbilical artery combined with Sad in identifying adverse pregnancy outcomes in sPE patients was 0.6545, with 60.27% specificity and 60.00% sensitivity (). In short, ultrasonic hemodynamic parameters of umbilical artery combined with Sad levels had better efficacy in evaluating adverse pregnancy outcomes in sPE patients.
Figure 3. Ultrasonic hemodynamic parameters of UA combined with Sad levels in sPE patients were utilised to evaluate adverse pregnancy outcomes. ROC curve analysis of ultrasonic hemodynamic parameters combined with Sad level in identifying adverse pregnancy outcomes in sPE patients.
Discussion
PE is a unique pregnancy disorder that occurs in pregnant women after 20 weeks of pregnancy (Machado et al. Citation2014). Globally, approximately 76,000 women and 500,000 infants die from the disease each year (Poon et al. Citation2019). Since the introduction of obstetric colour Doppler flow, foetal UA and other blood flow velocity waveforms measured by colour Doppler technology provide an effective method for monitoring foetal intrauterine safety (Ambrozic et al. Citation2017). Furthermore, adiponectin may be used as a biomarker and therapeutic target of PE in the clinical application because it protects the body against hypertension and proteinuria and dysregulated levels of adiponectin can trigger abnormal placentation and PE (Adu-Gyamfi et al. Citation2020). Our findings demonstrated that the combined use of UA Doppler and Sad levels can be used to assist in the prediction of adverse pregnancy outcomes in sPE patients.
Previously, parameters associated with the development of PE, such as blood pressure and urinary protein, have been identified as influencing factors for the prediction of PE (Jhee et al. Citation2019). Meanwhile, serum calcium levels and platelet counts are likewise strongly associated with the development of PE, and low serum calcium levels and platelet counts have been noted in PE patients during the prenatal period (Gabbay et al. Citation2014, Udenze et al. Citation2014). Moreover, PE is significantly associated with the risk of low birth weight (Akiyama et al. Citation2022). Unsurprisingly, sPE patients in our present study differed from healthy subjects in terms of mean arterial pressure, serum calcium levels, urinary protein, platelets, BMI at delivery, and infant birth weight. For PE, foetal hemodynamic changes can be found 2-3 weeks earlier and can be used to predict perinatal outcomes (Rani et al. Citation2016). Specifically, the features of high resistance flow in very advanced placental diseases can be detected by UA Doppler (Babic et al. Citation2015). As a whole, ultrasound Doppler (PI in particular) is unquestionably a preferred informational and prognostic tool for the management of high-risk pregnancies (Moawad et al. Citation2022). A study has identified significantly elevated UA markers (PI and RI) in women of childbearing age with severe late-onset PE (Moawad et al. Citation2022). Consistently, our present study manifested observably elevated values of PI and RI in sPE patients. Clearly, this reconfirms the findings of an earlier study that the UA Doppler index has important values in evaluating PE (Wang et al. Citation2022).
It has been reported that decreased adiponectin expression in placental tissues of patients with PE may be related to the development of PE (Garces et al. Citation2014). The BMI of pregnant women can lead to significant changes in Sad, and Sad in moderately and severely obese pregnant women is significantly poorly expressed and has a significant correlation with PE (Thagaard et al. Citation2019). As expected, our study documented an obvious decrease in Sad levels in sPE patients. Past research has looked into the correlation between adiponectin and uterine artery Doppler indexes in early- or late-onset PE (Tobinaga et al. Citation2014), while few studies have considered the relationship between Sad concentration and PI and RI. Notably, the existing research insufficiency highlighted the innovation of our study to highlight a significant negative correlation between Sad levels and PI/RI in sPE patients. In separate forms, UA Doppler has significant values in the antepartum foetal surveillance for FGR and PE (Gravett et al. Citation2016), and adiponectin acts as a biomarker of pregnancy complications (Pheiffer et al. Citation2021, Rao et al. Citation2021). A practice guideline points out that Doppler ultrasound not only has its unique value in diagnosing PE, but also plays an equally important role in detecting foetal status in patients with PE (Sotiriadis et al. Citation2019). More importantly, the AUC of ultrasonic hemodynamic parameters combined with Sad levels in diagnosing adverse pregnancy outcomes in sPE patients was 0.6545, which was higher than that of ultrasonic hemodynamic parameters of umbilical artery alone (AUC = 0.5671). Thus, we assumed that the diagnostic values may be even higher in obese patients. Taken together, our study emphasised for the first time that ultrasonic hemodynamic parameters combined with Sad had good diagnostic efficacy for adverse pregnancy outcomes in patients with sPE. Additionally, we observed decreased sensitivity in the curve of Sad combined with Doppler parameters. Youden index was used to determine the optimal critical value of variables including PI, RI and Sad, and regression model based tests were used to evaluate the prognostic performance of biomarker combinations (Yao et al. Citation2021). In the process of comparing the joint curve between different groups, the UA ultrasonic hemodynamic parameters in patients were increased significantly, while Sad expression was decreased significantly. The weight of the joint curve combined with PI/RI/SAD was different. Although FGR and abruption have no intervention or prevention, we observed increased diagnostic values in the combination of Sad and Doppler parameters, which might be even higher when obese pregnant women were enrolled. Thus, it could be inferred that UA ultrasound haemodynamics combined with Sad measurement could improve the predictive values on the adverse pregnancy outcomes of sPE patients.
In conclusion, this retrospective study analysed the correlation between ultrasonic hemodynamic parameters of umbilical artery (PI and RI) and Sad levels in sPE patients and evaluated the diagnostic efficacy of combined factors in the adverse pregnancy outcomes of sPE patients, which provided a new idea for predicting adverse pregnancy outcomes in sPE. Even if the possible pregnancy outcomes of sPE patients can’t be intervened so far, this paper can at least attract the attention of doctors or pregnant women to some extent, and for them to monitor the pregnant women promptly and prepare for possible accidents. For those that can be prevented, we hope that the results of Sad with Doppler parameters would also attract attention from doctors and pregnant women to adjust the state of women in preparation for pregnancy in time through diet, medical care, and other aspects to avoid possible adverse outcomes in advance. It is recommended that the monitoring of Sad levels in PE patients, especially sPE patients, and the management of daily diet and body weight be strengthened, which is of great significance to avoid accidents and improve medical quality. However, there are several limitations to this study. First, the sample size selected in this study was small, the BMI was normal, and the selection of ultrasonic hemodynamic parameters of umbilical artery was relatively simple (only PI and RI). In addition, the number of cases included in this study was small, so the sensitivity decreased. In the future, we need to carry out multi-center prospective studies to expand the sample size with precise classifications and to observe the diagnostic efficacy of Sad combined with Doppler parameters from the perspective of obese degree, with the expectation of providing new ideas for the diagnosis and prediction of adverse outcomes of PE in clinical practice.
Disclosure statement
The authors declare that they have no competing interests.
Availability of data and materials
All the data generated or analysed during this study are included in this published article.
Additional information
Funding
References
- Achari, A. E. and Jain, S. K., 2017. Adiponectin, a therapeutic target for obesity, diabetes, and endothelial dysfunction. International Journal of Molecular Sciences, 18(6), 1321.
- Adu-Gyamfi, E. A., et al., 2020. The role of adiponectin in placentation and preeclampsia. Cell Biochemistry and Function, 38 (1), 106–117.
- Afzal, S., et al., 2020. Renoprotective and haemodynamic effects of adiponectin and peroxisome proliferator-activated receptor agonist, pioglitazone, in renal vasculature of diabetic spontaneously hypertensive rats. PLoS One, 15 (11), e0229803.
- Akiyama, S., et al., 2022. Pregnancy and neonatal outcomes in women receiving calcineurin inhibitors: a systematic review and meta-analysis. British Journal of Clinical Pharmacology, 88 (9), 3950–3961.
- Alfirevic, Z., Stampalija, T., and Dowswell, T., 2017. Fetal and umbilical Doppler ultrasound in high-risk pregnancies. Cochrane Database Systematic Review, 6 (6), CD007529.
- Alfirevic, Z., Stampalija, T. and Medley, N., 2015. Fetal and umbilical Doppler ultrasound in normal pregnancy. Cochrane Database Systematic Review, 2015 (4), CD001450.
- Ambrozic, J., et al., 2017. Lung and cardiac ultrasound for hemodynamic monitoring of patients with severe pre-eclampsia. Ultrasound in Obstetrics & Gynecology, 49 (1), 104–109.
- Azizi, F., et al., 2017. Evaluation of placental mir-155-5p and long non-coding RNA sONE expression in patients with severe pre-eclampsia. International Journal of Molecular and Cellular Medicine, 6 (1), 22–30.
- Babic, I., et al., 2015. Intraplacental villous artery resistance indices and identification of placenta-mediated diseases. Journal of Perinatology, 35 (10), 793–798.
- Cornette, J., et al., 2016. Hemodynamic effects of intravenous nicardipine in severely pre-eclamptic women with a hypertensive crisis. Ultrasound in Obstetrics & Gynecology, 47 (1), 89–95.
- Dong, G., Tian, Y., and Li, X., 2018. Adiponectin participates in preeclampsia by regulating the biological function of placental trophoblasts through P38 MAPK-STAT5 pathway. Iranian Journal of Public Health, 47 (12), 1838–1844.
- Duryea, E. L., et al., 2014. A revised birth weight reference for the United States. Obstetrics & Gynecology, 124 (1), 16–22.
- Gabbay, A., et al., 2014. Calcium level during the first trimester of pregnancy as a predictor of preeclampsia. Hypertension in Pregnancy, 33 (3), 311–321.
- Garces, M. F., et al., 2014. Irisin levels during pregnancy and changes associated with the development of preeclampsia. Journal of Clinical Endocrinology and Metabolism, 99 (6), 2113–2119.
- Gottardi, E., et al., 2021. Preeclampsia before 26 weeks of gestation: Obstetrical prognosis for the subsequent pregnancy. Journal of Gynecology Obstetrics and Human Reproduction, 50 (3), 102000.
- Gravett, C., et al., Brighton Collaboration Non-reassuring Fetal Status Working Group, 2016. Non-reassuring fetal status: case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine, 34 (49), 6084–6092.
- Hosapatna Basavarajappa, D., et al., 2020. Neuroradiological perspectives of severe preeclampsia and eclampsia spectrum – correlation from posterior reversible encephalopathy syndrome. Pregnancy Hypertension, 20, 119–123.
- Ives, C. W., et al., 2020. Preeclampsia-pathophysiology and clinical presentations: JACC state-of-the-art review. Journal of the American College of Cardiology, 76 (14), 1690–1702.
- Jhee, J. H., et al., 2019. Prediction model development of late-onset preeclampsia using machine learning-based methods. PLoS One, 14 (8), e0221202.
- Machado, J. S., et al., 2014. Polymorphisms of the adiponectin gene in gestational hypertension and pre-eclampsia. Journal of Human Hypertension, 28 (2), 128–132.
- Masini, G., et al., 2022. Preeclampsia has two phenotypes which require different treatment strategies. American Journal of Obstetrics and Gynecology, 226 (2), S1006–S1018.
- Melchiorre, K., et al., 2020. Hypertensive disorders of pregnancy and future cardiovascular health. Frontiers in Cardiovascular Medicine, 7, 59.
- Mirkovic, L., et al., 2020. Prediction of adverse maternal outcomes of early severe preeclampsia. Pregnancy Hypertension, 22, 144–150.
- Moawad, E. M. I., et al., 2022. Evaluating the predictive value of fetal Doppler indices and neonatal outcome in late-onset preeclampsia with severe features: a cross-sectional study in a resource-limited setting. BMC Pregnancy and Childbirth, 22 (1), 377.
- Perdios, D., et al., 2021. CNN-based ultrasound image reconstruction for ultrafast displacement tracking. IEEE Transactions on Medical Imaging, 40 (3), 1078–1089.
- Pheiffer, C., et al., 2021. Adiponectin as a potential biomarker for pregnancy disorders. International Journal of Molecular Sciences, 22 (3), 1326.
- Poon, L. C., et al., 2019. The International Federation of Gynecology and Obstetrics (FIGO) initiative on pre-eclampsia: a pragmatic guide for first-trimester screening and prevention. International Journal of Gynecology & Obstetrics, 145 (S1), 1–33.
- Rani, S., Huria, A. and Kaur, R., 2016. Prediction of perinatal outcome in preeclampsia using middle cerebral artery and umbilical artery pulsatility and resistance indices. Hypertension in Pregnancy, 35 (2), 210–216.
- Rao, S., et al., 2021. Predicting maternal serum adiponectin and leptin level as biomarkers of pre-eclampsia: a prospective study. Journal of Obstetrics and Gynecology of India, 71 (1), 58–65.
- Ridder, A., et al., 2019. Preeclampsia: the relationship between uterine artery blood flow and trophoblast function. International Journal of Molecular Sciences, 20 (13), 3263.
- Rossi, A. C. and Prefumo, F., 2017. Correlation between fetal autopsy and prenatal diagnosis by ultrasound: a systematic review. European Journal of Obstetrics & Gynecology and Reproductive Biology, 210, 201–206.
- Sotiriadis, A., et al., 2019. ISUOG Practice Guidelines: role of ultrasound in screening for and follow-up of pre-eclampsia. Ultrasound in Obstetrics & Gynecology, 53 (1), 7–22.
- Takahashi, N., et al., 2018. Vitamin B(3) nicotinamide: a promising candidate for treating preeclampsia and improving fetal growth. The Tohoku Journal of Experimental Medicine, 244 (3), 243–248.
- Thagaard, I. N., et al., 2019. Leptin and adiponectin as markers for preeclampsia in obese pregnant women, a cohort study. Pregnancy Hypertension, 15, 78–83.
- Tita, A. T., et al., 2022. Treatment for mild chronic hypertension during pregnancy. New England Journal of Medicine, 386 (19), 1781–1792.
- Tobinaga, C. M., et al., 2014. Angiogenic factors and uterine Doppler velocimetry in early- and late-onset preeclampsia. Acta Obstetricia et Gynecologica Scandinavica, 93 (5), 469–476.
- Udenze, I. C., et al., 2014. Calcium and magnesium metabolism in pre-eclampsia. West African Journal of Medicine, 33 (3), 178–182.
- Wang, Q., Liu, D., and Liu, G., 2022. Value of ultrasonic image features in diagnosis of perinatal outcomes of severe preeclampsia on account of deep learning algorithm. Computational and Mathematical Methods in Medicine, 2022, 4010339.
- Yao, C., et al., 2021. Optimized combination of circulating biomarkers as predictors of prognosis in AECOPD patients complicated with heart failure. International Journal of Medical Sciences, 18 (7), 1592–1599.
- Yurtcu, N., et al., 2022. Predictive and diagnostic value of serum adipokines in pregnant women with intrahepatic cholestasis. International Journal of Environmental Research and Public Health, 19 (4), 2254.
- Zhu, D., et al., 2022. Fetal cerebral hemodynamic changes in preeclampsia patients by ultrasonic imaging under intelligent algorithm. Computational Intelligence and Neuroscience, 2022, 4269308.