

Abstract
Background
This study aimed to evaluate the value of non-invasive prenatal testing (NIPT) in the prenatal screening of foetal aneuploidy-associated diseases at different gestational ages.
Methods
Briefly, cell-free foetal DNAs were extracted from plasma first, followed by DNA sequencing and bioinformatics analyses for chromosome aneuploidy (T21, T18, and T13), sex chromosome aneuploidy (SCA), and microdeletion/microduplication. Subsequently, the positive results were subject to karyotype analyses.
Results
The pregnant women included in this study were divided into six groups, and the results, such as chromosome diagnoses, and clinical phenotypes, were collected for data analyses. According to the results of the data analysis, the positivity rates of foetal chromosomal abnormalities in pregnant women under 20, 20–24, 25–29, 30–34, 35–39, and >40 years old were 0%, 0.17%, 0.25%, 0.27%, 0.60%, and 1.66%, respectively. The positive predictive value (PPV) in the 20–24 years group was 41.67%, that in the 25–29 years group was 62.5%, that in the 30–34 years group was 66.67%, that in the 35–39 years group was 90.74%, and that in the >40 years group was 90.32%.
Conclusion
Overall, NIPT detection in elderly pregnant women has excellent clinical application value in reducing the incidence of either birth defects or abortion caused by invasive chromosome examination.
PLAIN LANGUAGE SUMMARY
It is critical to diagnose foetal chromosome aneuploidy in time through prenatal screening to prevent birth defects. This study aimed to evaluate the value of non-invasive prenatal testing (NIPT) in prenatal screening of foetal aneuploidy-associated diseases at different gestational ages. A retrospective analysis based on NIPT screening data at a medical laboratory was performed. The results showed that the total positivity rate and total positive predictive value of trisomy 21, trisomy 18, and trisomy 13 in older pregnant women (≥35 years old) were significantly higher than those in younger pregnant women, and there was an increasing trend with increasing maternal ages. This study indicated that NIPT detection in elderly pregnant women has an excellent application value in clinical practice to reduce the incidence of birth defects and abortion caused by invasive chromosome examination.
Introduction
Birth defects constitute a major health problem worldwide, and they are the leading cause of infant mortality. Unfortunately, the incidence of birth defects in China (about 4.6%) is relatively high (Guo et al. Citation2022, Zhang et al. Citation2022), accounting for about 20% of the total number of birth defects in the world. Chromosomal abnormalities, which represent the leading cause of birth defects, may affect 1/200–1/150 births. The most typical chromosomal aneuploidies consist of trisomy 13 (T13) syndrome, trisomy 18 (T18) syndrome, and trisomy 21 (T21) syndrome (Chen et al. Citation2011, He et al. Citation2014). Additional chromosomal abnormalities include sex chromosome abnormalities (SCAs) (Mizia et al. Citation2016, Samango-Sprouse et al. Citation2020) and chromosomal microdeletions and multiplication (microduplication) syndrome (Yuanyuan et al. Citation2020, Yang et al. Citation2021). Several previous studies have confirmed that the probability of foetal chromosomal abnormalities increases as maternal age increases (Ping et al. Citation2021) mainly because as the latter increases, the ovarian function, and egg quality of pregnant women decrease, while the probability of germ cell abnormalities and egg fertilisation increases. Therefore, in China, elderly pregnant women (≥35 years old) are the recommended population for prenatal diagnostic testing. Karyotype analysis is the gold standard for diagnostic testing performed using amniocentesis extracted amniotic fluid aseptically under B-ultrasound guidance (Simons et al. Citation2013). Timely prenatal screening of foetal chromosome aneuploidy is critical to the prevention of birth defects.
Non-invasive prenatal testing (NIPT) is a DNA sequencing-based method. Generally, NIPT is employed to detect the overall quantitative difference of cell-free foetal DNA fragments in maternal peripheral blood plasma to identify common forms of autosomal trisomy. Moreover, due to the ability to reflect the copy number difference of chromosomes, NIPT can be applied in the screening of chromosome aneuploidies (Lo et al. Citation1999, Lo et al. Citation2010, Demko et al. Citation2022). Through bioinformatics analyses of sequencing results, foetal genetic information was identified. Compared with invasive chromosome karyotype analyses of amniocentesis fluid, NIPT is less harmful to pregnant women and can effectively avoid an increase in the risk of surgical infection and abortion.
We conducted a retrospective analysis was performed on the data of NIPT screening at a medical laboratory to evaluate the value of NIPT in the prenatal screening of foetal aneuploidy-associated diseases at different gestational ages.
Materials and methods
Study design and setting
Pregnant women of different ages who voluntarily underwent NIPT screening at a medical laboratory from January 2017 to December 2021 were included in this study. All NPT-positive pregnant women were subjected to invasive karyotype analyses in prenatal diagnostic institutions. All pregnant women received prenatal counselling, and the pregnancy outcome was followed up for one year. This study was approved by the Ethics Committee of Guangzhou KingMed Diagnostics Ltd (2022144). All design, analysis, interpretation of data, drafting, and revisions in this study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies, available through the Enhancing the Quality and Transparency of Health Research network.
Participants
Our inclusion criteria were as follows: (1) normal pregnancy evolving for more than 12 weeks; (2) the couple’s chromosomes were normal; (3) the age ranged from 18 years to 45 years. We excluded individuals who (1) once received an allogeneic blood transfusion; (2) underwent transplant surgery; (3) received stem cell therapy within one year; (4) provided incomplete information. The pregnant women enrolled in this study were divided into six groups; namely, <20 years old, 20–24 years old, 25–29 years old, 30–34 years old, 35–39 years old, and ≥40 years old groups.
DNA sequencing and bioinformatics analysis
Firstly, 5–10 mL peripheral blood samples were collected from pregnant women, placed in the cell-free DNA storage tubes, and then transported to a laboratory in cold storage. Plasma separation of all samples did not exceed 72 h. To be specific, the plasma was separated via two centrifugations performed at a speed of 1600 R/min that lasted for 10 min. After extracting the cell-free foetal DNA (cffDNA) from the separated plasma, the library was constructed per the instructions of foetal chromosome aneuploidy (T21, T18, and T13) testing kits (Capitalbio Corporation, Beijing, China). Briefly, the fragmented cffDNA was subject to end repairing, followed by ligation with the tag and the sequencing primer. Subsequently, the amplicon was generated through polymerase chain reaction (PCR), and library quantification was performed using PCR based on the standard curve method. Then, the pooling library was denatured and the loading library (with a concentration of 25 pM) was generated for sequencing with a BES 4000 sequencing system (CapitalBio Corporation, Beijing, China, CFDA Registration Permit NO. 20153400309). The metric included the effective sequencing data size of a single library >3.5 M, ISP loading >75%, polyclonal <30%, and low quality <10%. Non-invasive Prenatal Data Analysis Management System V3.0 (CapitalBio Corporation, Beijing) was used for bioinformatics analyses. The results of the detection were expressed as the Z-value risk score; −3 < Z < 3 was the low-risk reference range of T13/18/21, and Z ≥ 3 or Z ≤ −3 was the elevated-risk reference range for T13/T18/T21. By the way, a Z-score of ≥3 or ≤-3 was associated with migrations/microduplications and SCA (Han et al. Citation2015). The quality control requirement for the foetal DNA concentration was >4%. All experiments were assessed by trained PCR technicians in our laboratory.
Karyotype analysis
Briefly, a 15-mL aliquot of amniotic fluid was collected and centrifuged at 2000 rmp for 7 min, after which the cell pellet was collected and re-suspended for culture. Once more than eight cell clones were formed, the cell samples were transferred into the tube for the preparation of a cell suspension. The results were analysed and quality-controlled per the standards of the American College of Pathologists which required nuclear fission phases >20 and resolution >320 bands.
Data analysis
Data were collected and processed as described previously (Demko et al. Citation2022, Guo et al. Citation2022, Zhang et al. Citation2022). Among the cases that tested positive, the affected ones were the true positives, while the unaffected ones were the false positives (FPs). The negative predictive value (NPV) and positive predictive value (PPV) were calculated to assess test performance. SPSS 23.0 was used for statistical analyses of all data, and p < 0.05 was statistically significant.
Results
Study procedures and test results
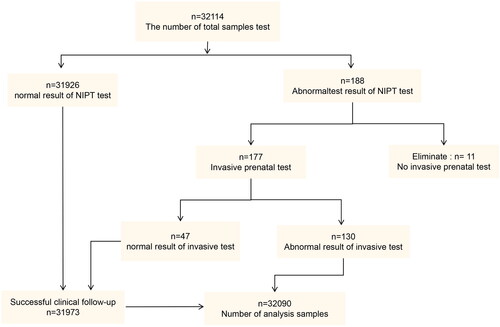
A total of 32,114 subjects were first analysed by NIPT. As shown in , 177 out of the 188 abnormal NIPT test results were then examined by invasive prenatal karyotype analysis. Besides, 130 samples were found to have abnormal chromosomal appearances, including the number, arrangement, size, and structure of the chromosomes. All subjects with either normal NIPT or accepted abnormal karyotype analyses were confirmed by regular follow-up.
Figure 1. Inclusion and exclusion of patients and samples in this study. NIPT: non-invasive prenatal testing.
The verification of non-invasive prenatal testing (NIPT) results by invasive prenatal karyotype analysis
We found a total of 188 abnormal NIPT results, indicating a high risk of SCA, and the probability of chromosomal abnormalities was 0.59%. Among the 188 subjects, a total of 177 pregnant women underwent invasive chromosome karyotype examinations. As a result, there were 130 cases of confirmed chromosomal abnormalities, and the PPV was 73.45%; 47 cases were FP, giving an FP rate of 25%. The other 11 pregnant women did not undergo prenatal diagnostic testing.
There were 103 cases of T21 aneuploidy screened by NIPT, of which 96 were confirmed by karyotype examination, giving a PPV of 93.20% for T21. Besides, the 30 cases of T18 in NIPT were further examined by karyotype examination, of which 19 cases were confirmed, and the PPV of T18 was 63.33%. Ten out of 28 cases of T13 in NIPT were confirmed by karyotype examinations, and the PPV was 35.71%. The 10 cases with SCA in NIPT further underwent karyotype examinations, and the examination revealed three positive results, giving a PPV of 30%. The seven other subjects were FP SCA in NIPT. In addition, two out of six subjects with other autosomal microdeletions and microduplications were also confirmed by karyotype examination, giving a PPV of 33.33% (). Obviously, NIPT had the highest clinical predictive value for foetal T21 syndrome.
Table 1. The results of prenatal diagnosis and clinical outcome.
Age distribution of pregnant women with chromosomal abnormalities
As shown in , the results of NIPT, and invasive prenatal diagnosis in different age groups showed different positivity rates of foetal chromosomal abnormalities. Specifically, the positivity rate in pregnant women aged under 20 years was 0%, that in pregnant women aged 20–24 years was 0.17%, that in pregnant women aged 25–29 years was 0.25%, that in pregnant women aged 30–34 years was 0.27%, that in pregnant women aged 35–39 years was 0.60%, and that in pregnant women aged >40 years was 1.66%. Overall, the probability of foetal chromosomal abnormalities increased with the age of pregnant women. Moreover, the positivity rate of foetal chromosome abnormality differed significantly among pregnant women of different age groups (χ2 = 87.028, p ˂ 0.01).
Table 2. The results of NIPT and invasive prenatal detection in pregnant women.
In comparison with invasive karyotype examination results, the consistency of the positive results of NIPT in the 20–24 years age group was 41.67%, that in the 25–29 years age group was 62.5%, that in the 30–34 years age group was 66.67%, that in the 35–39 years age group was 90.74%, while that in the >40 years age group was 90.32%. The results showed that the PPV of NIPT screening was significantly higher in people aged above 35 years (χ2 = 38.328, p ˂ 0.01; ).
Discussion
With the development and application of high-throughput sequencing technology, the prenatal screening, and diagnosis project of pregnant women with advanced maternal age has greatly improved. In 2001, the American Association of Obstetricians and Gynaecologists (AAOG) and the Maternal and Child Protection Act of China (MCPAA) definitely proposed the necessity of interventional prenatal diagnosis for elderly pregnant women. However, due to the characteristic detection cycle delay and trauma of interventional prenatal diagnostic procedures, the compliance of pregnant women is poor. NIPT, a non-invasive technique that is developed and applied earlier and faster, has become a candidate for older pregnant women (Teder et al. Citation2019, LeFevre and Sundermeyer Citation2020). Okmen et al. found that the number of invasive prenatal diagnostic procedures decreased significantly in their study on the changes in prenatal diagnosis populations before and after NIPT application (Firat et al. Citation2020). In 2015, the AAOG and the Maternal-Foetal Medicine Association suggested that NIPT could be applied in the interventional prenatal diagnosis of high-risk patients as a first-line screening method.
NIPT is not considered a diagnostic test because it has the possibility to acquire FP or false negative (FN) results, even if the possibility is small. The main reason for the inconsistent results is that the circulating cffDNA is mainly derived from the cytotrophoblasts of the chorionic villi in the placenta, which is not always representative of the foetus (Flori et al. Citation2004). Moreover, differences in placental and foetal karyotype and the extent of chimerism can influence NIPT outcomes (Srebniak et al. Citation2014). Therefore, the outcomes of amniocentesis positivity were applied in this study to confirm the results of NIPT. In this paper, the NPV of T13/T18/T21 was 100% in a total of 32,103 NIPT subjects; the PPVs of T21, T18, and T13 were 93.20%, 63.33%, and 35.71%, respectively. It is consistent with the results of 65%–94% for T21, 47%–85% for T18, and 12%–62% for T13 reported in the literature (Norton et al. Citation2015, Yuval et al. Citation2015, Liu et al. Citation2017). Therefore, NIPT showed the highest accuracy in the detection of T21, followed by T18, and T13 in the above three common chromosomal aneuploidy abnormalities. Gu et al. also demonstrated that NIPT had the highest diagnostic coincidence rate for T21 (90.00%) and the lowest diagnostic coincidence rate for other chromosomal abnormalities (Gu et al. Citation2022). Maternal age ≥35 years is considered a cautious indicator of NIPT in technical regulations for prenatal screening and the detection of foetal free DNA in maternal peripheral blood published by the National Health and Family Planning Commission of the People’s Republic of China. On the one hand, the high incidence of chromosomal abnormalities in elderly pregnant women requires that this condition be diagnosed as early as possible, and on the other hand, the limited range of NIPT detection makes it difficult to detect additional chromosomal abnormalities.
This study also showed that the total PPV of older pregnant women (≥35 years old) was more than 90%. The positivity rate of foetal chromosomal abnormalities in older pregnant women (>35 years old) was 0.78%, which was about two times higher than that in younger pregnant women (0.24% in women aged ≤35 years old). Among them, the incidence of foetal chromosomal abnormalities in the group of women aged over 40 years reached 1.66%, which was about 6.9 times higher than that in the group of women aged below 35 years (0.24%); besides, the incidence increased with the ages of the pregnant women. There were 461 pregnant women aged below 20 years, and no abnormal NIPT positivity was observed. In addition, there were only six cases of NIPT true positives in the population of women aged 20–24 years, accounting for 0.17% of the total number of 3438, containing five cases of T21 and one case of T18. The risk of foetal T21, T18, and T13 is extremely low in these groups. Therefore, NIPT has a higher detection rate and PPV of foetal chromosomal abnormalities in older pregnant women. Another study also showed that the diagnostic rate of foetal chromosomal abnormalities in pregnant women under 40 years is 0.39%–0.79%; however, the risk in those aged >40 years is relatively high; i.e. 1.32%–4.44% (Gu et al. Citation2022). Thus, it is recommended to use NIPT as the first line of chromosome aneuploidy screening in older pregnant women, followed by invasive chromosome examination for the clinical diagnosis of women with positive screening results.
In addition, one subject of HFW04252 was found to be T13-positive in NIPT in this study; however, it was 46, XN, 1qh+, dup (13) (q14.3q21.1) instead in the followed foetal chromosome karyotype analysis. Such a result demonstrated a certain value of NIPT screening possessed for the microduplication of large fragments in chromosome 13. In this paper, 11 pregnant women with positive NIPT results did not undergo foetal karyotyping. Moreover, nine out of eleven subjects terminated their pregnancies directly, and the other two subjects chose to continue with their pregnancies. One of these two subjects was at high risk of 1q31-proximal telomere duplication syndrome combined with an elevated risk of sex chromosome aneuploidy XO/XY (sample number: NP01551) and another was an elevated risk of 22q11.2 deletion (DiGeorge) syndrome (sample number: NB13053). The follow-up results revealed that the neonate from subject NP01551 had a normal phenotype, while the foetus from subject NB13053 was found to have 22q11.2 microdeletion syndrome by chromosome karyotyping, alongside the clinical phenotype. Therefore, genetic counselling should be performed for pregnant women after NIPT screening. Also, further prenatal karyotyping is recommended to avoid either the NIPT FP result-caused pregnancy termination, or the lack of understanding of NIPT led to birth defects.
Furthermore, this study demonstrated that the PPVs of NIPT results were 30% in SCA and 33.3% in chromosomal microdeletions and microduplications, which were low and consistent with the findings of previous studies (Bianchi Citation2019, Jiexia et al. Citation2021). Notably, all the above SCA, and chromosomal microdeletions and microduplications occurred in pregnant women aged above 35 years. However, due to the limited number of positives, the findings of the study cannot be generalised. A systematic review of FP and FN NIPT cases indicated that confined placental mosaicism, true foetal mosaicism, maternal CNV, or mosaicism, maternal malignancy, vanishing twin, and technical or human errors could be determinants of discordance between NIPT results and foetal karyotypes (Hartwig et al. Citation2017).
The application of NIPT in screening sex chromosomes and other chromosomal microdeletions and microduplicates in pregnant women of different ages remains a major challenge. A previous study pointed out that the elimination of the background maternal age risk from the algorithm absolute risk ameliorated the detection rate for aneuploidy, while such a conclusion needs to be further verified by a prospective study with a larger sample size (Padula et al. Citation2017). The accuracy of NIPT gives it a high clinical value in screening chromosome aneuploidy, and the insurance for a healthy baby is mainly based on the NPV of the test. In general, a subject with a negative NIPT result is not going to undergo invasive karyotyping without birth defect insurance. Thus, the life of a subject with FN NIPT results could be threatened in the absence of insurance claims. Therefore, the accuracy of NIPT is highly significant for the clinical diagnosis of birth defects during pregnancy.
This is a cross-sectional study conducted with retrospective data, and the predictability is therefore insufficient. In addition, the real challenge in the era of molecular medicine is to find a biomarker or a panel of biomarkers for the early diagnosis of preeclampsia, intrauterine growth restriction, and stillbirth. For example, decreased numbers of endothelial progenitor cells and increased numbers of natural killer cells in peripheral blood may be early markers of preeclampsia (Laganà et al. Citation2017). Specific values of pregnancy-associated plasma protein-A (PAPP-A) and free beta-hCG could identify the risk of low birth weight or high birth weight since the first trimester of pregnancy (Cignini et al. Citation2016). Therefore, the relevant molecular biomarkers can be explored as a supplement to NIPT in future studies.
Conclusion
In this article, the positivity rate of foetal chromosomes in pregnant women at different age groups has been compared based on the NIPT method. In brief, the total positivity rates, and total PPV of T21, T18, and T13 in elderly pregnant women (≥35 years old) are not only significantly higher than those in younger pregnant women but also show an increasing trend with increasing maternal age. However, the results of prenatal diagnoses have revealed some FP cases. Still, positive NIPT results need to be further verified by karyotype analyses or chromosome microarray analyses (Yibo et al. Citation2019, Yuanyuan et al. Citation2020).
The NPV of NIPT in different age groups is 100%, which plays a significant role in the screening of foetal T21, T18, and T13 syndromes. In terms of sex chromosomes and other chromosomal microdeletions and microduplicates, the NIPT detection results of elderly pregnant women also have a higher detection rate. However, more research is still required due to the limited available statistical positive data. Overall, NIPT detection in elderly pregnant women has excellent clinical application value to reduce the incidence of birth defects and abortion caused by invasive chromosome examination.
Ethics statement
This study was approved by the Ethics Committee of Guangzhou KingMed Diagnostics Ltd (2022144).
Authors’ contributions
ZQL and XHL contributed to conception and design; ZQL and XHL were involved in drafting the manuscript and revising it critically for important intellectual content; WLK, SJT, YM, TF, JJF and XHL made substantial contributions to the acquisition of data; WLK, SJT, YM, TF, JJF and XHL analysis and interpretation of data; and all authors have given final approval of the version to be published.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Additional information
Funding
References
- Cignini, P., et al., 2016. Predictive value of pregnancy-associated plasma protein-A (PAPP-A) and free beta-hCG on fetal growth restriction: results of a prospective study. Archives of Gynecology and Obstetrics, 293 (6), 1227–1233.
- Bianchi, D.W., 2019. Turner syndrome: new insights from prenatal genomics and transcriptomics. American Journal of Medical Genetics Part C, Seminars in Medical Genetics, 181 (1), 29–33.
- Chen, E.Z., et al., 2011. Noninvasive prenatal diagnosis of fetal trisomy 18 and trisomy 13 by maternal plasma DNA sequencing. PloS One, 6 (7), e21791.
- Demko, Z., Prigmore, B. and Benn, P., 2022. A critical evaluation of validation and clinical experience studies in non-invasive prenatal testing for trisomies 21, 18, and 13 and monosomy X. Journal of Clinical Medicine, 11 (16), 4760.
- Firat, O., et al., 2020. Comparison of indications and results of prenatal invasive diagnostic tests before and after the implementation of the use of cell-free fetal DNA: a tertiary referral center experience. Journal of Assisted Reproduction and Genetics, 37 (8), 2019–2024.
- Flori, E., et al., 2004. Circulating cell-free fetal DNA in maternal serum appears to originate from cyto- and syncytio-trophoblastic cells. Case report. Human Reproduction, 19, 723–724.
- Gu, Z., et al., 2022. Study on the clinical value of noninvasive prenatal testing in screening the chromosomal abnormalities of the fetus in the elderly pregnant women. Computational and Mathematical Methods in Medicine, 2022, 2977128.
- Guo, N., et al., 2022. Positive predictive value of noninvasive prenatal testing for sex chromosome abnormalities. Molecular Biology Reports, 49 (10), 9251–9256.
- Han, Z., et al., 2015. Statistical approach to decreasing the error rate of noninvasive prenatal aneuploid detection caused by maternal copy number variation. Scientific Reports, 5 (1), 16106.
- Hartwig, T.S., et al., 2017. Discordant non-invasive prenatal testing (NIPT) - a systematic review. Prenatal Diagnosis, 37 (6), 527–539.
- He, F., et al., 2014. Directed Bmp4 expression in neural crest cells generates a genetic model for the rare human bony syngnathia birth defect. Developmental Biology, 391 (2), 170–181.
- Jiexia, Y., et al., 2021. Performances of NIPT for copy number variations at different sequencing depths using the semiconductor sequencing platform. Human Genomics, 15 (1), 41.
- Laganà, A.S., et al., 2017. Decreased endothelial progenitor cells (EPCs) and increased natural killer (NK) cells in peripheral blood as possible early markers of preeclampsia: a case-control analysis. Archives of Gynecology and Obstetrics, 295 (4), 867–872.
- LeFevre, N.M. and Sundermeyer, R.L., 2020. Fetal aneuploidy: screening and diagnostic testing. American Family Physician, 101 (8), 481–488.
- Liu, C., et al., 2017. Effects of Lactobacillus casei and Enterococcus faecalis on growth performance, immune function and gut microbiota of suckling piglets. Archives of Animal Nutrition., 71 (2), 120–133.
- Lo, Y.M., et al., 1999. Quantitative abnormalities of fetal DNA in maternal serum in preeclampsia. Clinical Chemistry, 45 (2), 184–188.
- Lo, Y.M., et al., 2010. Maternal plasma DNA sequencing reveals the genome-wide genetic and mutational profile of the fetus. Science Translational Medicine., 2 (61), 61ra91.
- Mizia, K., Townsend, L. and Karatas, J., 2016. Sex chromosome aneuploidy screening in a general population. Australasian Journal of Ultrasound in Medicine, 19 (3), 105–108.
- Norton, M.E., et al., 2015. Cell-free DNA analysis for noninvasive examination of trisomy. Obstetrical & Gynecological Survey, 70 (8), 483–484.
- Padula, F., et al., 2017. The introduction of the absolute risk for the detection of fetal aneuploidies in the first-trimester screening. The Journal of Maternal-Fetal & Neonatal Medicine, 30 (10), 1249–1253.
- Ping, C.L., et al., 2021. Predictive value of aberrant right subclavian artery for fetal chromosome aneuploidy in women of advanced maternal age. BMC Pregnancy and Childbirth, 21 (1), 148.
- Samango-Sprouse, C.A., et al., 2020. Impact of early diagnosis and noninvasive prenatal testing (NIPT): knowledge, attitudes, and experiences of parents of children with sex chromosome aneuploidies (SCAs). Prenatal Diagnosis, 40 (4), 470–480.
- Simons, A., Shaffer, G. and Hasting, J., 2013. Cytogenetic nomenclature: changes in the ISCN 2013 compared to the 2009 edition. Cytogenetic and Genome Research, 141 (1), 1–6.
- Srebniak, M.I., et al., 2014. Abnormal non-invasive prenatal test results concordant with karyotype of cytotrophoblast but not reflecting abnormal fetal karyotype. Ultrasound in Obstetrics & Gynecology, 44, 109–111.
- Teder, H., et al., 2019. Computational framework for targeted high-coverage sequencing based NIPT. PLoS One, 14 (7), e0209139.
- Yang, J., et al., 2021. A cross-sectional survey of pregnant women’s knowledge of chromosomal aneuploidy and microdeletion and microduplication syndromes. European Journal of Obstetrics & Gynecology and Reproductive Biology, 256, 82–90.
- Yibo, C., et al., 2019. Noninvasive prenatal testing for chromosome aneuploidies and subchromosomal microdeletions/microduplications in a cohort of 42,910 single pregnancies with different clinical features. Human Genomics, 13 (1), 60.
- Yuanyuan, P., et al., 2020. Efficiency of noninvasive prenatal testing for the detection of fetal microdeletions and microduplications in autosomal chromosomes. Molecular Genetics & Genomic Medicine, 8 (8), e1339.
- Yuval, Y., et al., 2015. Current status of testing for microdeletion syndromes and rare autosomal trisomies using cell-free DNA technology. Obstetrics and Gynecology, 126 (5), 1095–1099.
- Zhang, Y., et al., 2022. Non-invasive prenatal testing for the detection of trisomy 13, 18, and 21 and sex chromosome aneuploidies in 68,763 cases. Frontiers in Genetics, 13, 864076.