

 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Vaginal bleeding during pregnancy has been recognised as a significant risk factor for adverse pregnancy outcomes. This study aimed to investigate the association between vaginal bleeding during the first trimester of pregnancy and clinical adverse effects using a systematic review and meta-analysis.
Methods
Databases of Scopus, Web of Science, PubMed (including Medline), Cochrane Library and Science Direct were searched until June of 2023. Data analysis using statistical test fixed- and random-effects models in the meta-analysis, Cochran and meta-regression. The quality of the eligible studies was assessed by using the Newcastle–Ottawa Scale checklist (NOS).
Results
A total of 46 relevant studies, with a sample size of 1,554,141 were entered into the meta-analysis. Vaginal bleeding during the first trimester of pregnancy increases the risk of preterm birth (OR: 1.8, CI 95%: 1.6–2.0), low birth weight (LBW; OR: 2.0, CI 95%: 1.5–2.6), premature rupture of membranes (PROMs; OR: 2.3, CI 95%: 1.8–3.0), abortion (OR: 4.3, CI 95%: 2.0–9.0), stillbirth (OR: 2.5, CI 95%: 1.2–5.0), placental abruption (OR: 2.2, CI 95%: 1.4–3.3) and placenta previa (OR: 1.9, CI 95%: 1.5–2.4).
Conclusions
Vaginal bleeding in the first trimester of pregnancy is associated with preterm birth, LBW, PROMs, miscarriage, stillbirth, placental abruption and placenta previa. Therefore, physicians or midwives need to be aware of the possibility of these consequences and manage them when they occur.
PLAIN LANGUAGE SUMMARY
Vaginal bleeding in the first trimester of pregnancy increases the relative risk of preterm birth, low birth weight, premature rupture of membranes, abortion, stillbirth, placental abruption and placenta previa.
Introduction
Vaginal bleeding during pregnancy, especially during the first trimester, can lead to adverse maternal and infant outcomes including placental abruption, premature rupture of membranes (PROMs), preterm delivery, intrauterine growth restriction (IUGR) and admission to the neonatal intensive care unit (NICU) (Madan et al. Citation2010, Sutter et al. Citation2006). Spotting and vaginal bleeding are common during pregnancy, but they have not been attributed to any specific cause (Hasan et al. Citation2010). It has that a quarter of pregnancies are associated with mild to severe vaginal bleeding during the first trimester. The prevalence of vaginal bleeding during the first trimester of pregnancy ranges from 7 to 25% (Hasan et al. Citation2010). It has been reported that about 50% of pregnant women with vaginal bleeding experienced abortion (Dongol et al. Citation2011). Generally, vaginal bleeding during the first trimester of pregnancy can predict adverse outcomes for the mother and infant and the risk of foetal, and infant mortality is quadrupled (Mustafa et al. Citation2009). These adverse outcomes can increase the rate of hospitalisation for newborns and their mothers, hinder infants’ development, lead to neonatal death and impose enormous costs on the healthcare system (Dolatian et al. Citation2013, Morisaki et al. Citation2014, Nour Citation2012).
There is a diversity of reports regarding the association between bleeding during pregnancy and adverse neonatal outcomes, but none of them suggests a causal relationship (Dee Zhen Citation2017, Kayode et al. Citation2016, Yang et al. Citation2004). Differences in access to health services during pregnancy, severity and duration of bleeding, urinary tract infection, education level, causes of bleeding, history of abortion, unwanted pregnancy, infertility, multiple pregnancies and smoking cessation also influence the above-mentioned association and can lead to discrepancies in the results of studies. Therefore, identifying the appropriate and accurate association between bleeding during pregnancy and adverse pregnancy outcomes requires pooling studies’ results and drawing a more complete picture of factors affecting pregnancy outcomes (Hasan et al. Citation2010, Nour Citation2012, Yang et al. Citation2004).
This systematic review and meta-analysis aimed to probe the pooled estimate of associations between vaginal bleeding during the first trimester of pregnancy and adverse clinical outcomes in the mother and infant to improve our understanding of appropriate health measures for preventing adverse pregnancy outcomes.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standard guideline was used to follow up the review process and report findings (Liberati et al. Citation2009).
Protocol and registration
The study protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO) under the code CRD42020167710.
Search strategy and selection criteria
This review focused on retrospective and prospective case-control and cohort studies of vaginal bleeding during pregnancy (other than spotting) and associated adverse clinical outcomes published in English-language articles (Articles with abstract or full text in English) by the June of 2023. The databases of Scopus, Web of Science, PubMed (including Medline), Cochrane Library and Science Direct were searched medical subject headings (MeSH) keywords: Uterine Haemorrhage, Pregnancy Complications, Pregnancy, stillbirth, Foetal Growth Retardation, Placenta Previa, Abruptio Placentae, Foetal Membranes Premature Rupture, abortion Premature Birth, Abortion Threatened, Premature Birth, Infant, low birth weight (LBW), Pre-Eclampsia and Apgar Score. And other relevant keywords: vaginal bleeding, adverse birth outcomes, intrauterine growth retardation, placental abruption, PROM, threatened abortion, preterm births and LBW. They were used in isolation or combination through the Boolean AND and OR operators.
Inclusion and exclusion criteria
Inclusion criteria were organised according to the Problem or Population, Interventions/exposure, Comparison and Outcome (PI(E)CO) as follows: Population: all pregnant women in the age range of 15–49 years; Intervention/exposure: vaginal bleeding during the first trimester of pregnancy (0–13 weeks); Comparison: vaginal bleeding during the first trimester of pregnancy vs. no vaginal bleeding; Outcome: clinical adverse outcomes including preterm birth, IUGR, LBW, preeclampsia, PROM, placental abruption, abortion, stillbirth, caesarean delivery, placental previa, Apgar score <7 at 5 min and hospitalisation in the NICU.
Exclusion criteria were studies conducted on mothers with specific types of diseases (induced pregnancy); studies on vaginal bleeding during pregnancy that did not provide required data on the estimation of the odds ratio (OR); qualitative studies, case reports, review articles and interventional studies.
Quality assessment
The researchers assessed the quality of selected studies using a scoring system based on the Newcastle–Ottawa Scale checklist (NOS) for non-randomisation studies (case-control and cohort studies). In this checklist, the ‘star system’ of scoring is used, and if it has high quality in the designated areas, it will be awarded a star. In cohort studies, this checklist has three parts: Selection, Comparability and Exposure, and in case-control studies, it has three parts: selection, comparability and outcome. The selection section can receive a maximum of 4 stars, the comparability section can receive a maximum of two stars and the exposure or outcome can receive a maximum of 3 stars. Total stars of 0–5, 6–7 and 8–9 were considered low quality, moderate quality and high quality, respectively. Studies with a star of upper 5 were selected for the quantitative meta-analysis process (Peterson et al. Citation2011).
Screening and data extraction
The search results were entered into Endnote version x8-1 software (Philadelphia, PA, US) and duplicate titles were removed. Then, the title and abstract of the articles were reviewed based on the inclusion and exclusion criteria, and irrelevant articles were removed. In the next step, the full text of the articles was studied by two researchers (SD and AK) and a third person as an epidemiologist. If the articles were rejected by two researchers, the reasons were mentioned, and in case of disagreement between them, the article was evaluated by the third researcher.
A checklist was used to extract data from the selected studies in terms of the sample size, study location, study years, type of study, vaginal bleeding during pregnancy, clinical outcomes associated with vaginal bleeding during the first trimester of pregnancy, the ORs and the corresponding 95% confidence interval (CI). They were used to present the clinical outcomes (pre-specified outcomes) of the present review as preterm birth vs. term birth, IUGR vs. lack of IUGR, LBW vs. normal birth weight, preeclampsia vs. lack of preeclampsia, abortion vs. lack of abortion, stillbirth vs. live birth, PROM vs. lack of PROM, placental previa and placental abruption vs. normal placenta, Apgar score less than 7 in the fifth minute vs. Apgar score more than 7 and admission to the NICU vs. non-hospitalisation. If the OR was not directly mentioned in these studies, it was estimated by the researchers using statistical methods.
Statistical analysis
For the estimation of the OR and standard deviation (SD), the OR = and SD = (OR)
formulae were used (Tenny and Hoffman Citation2023). The combination of results in heterogeneous studies was performed using the random-effects model. For homogeneous studies, the fixed-effects model in the meta-analysis was used. Heterogeneity across studies was evaluated through the Q statistics and I2 statistics with the significance level of p < 0.10. I2 0–50%: not important; 50–75%: moderate heterogeneity and >75% high heterogeneity, were considered (Huedo-Medina et al. Citation2006). Sensitivity analysis was performed to investigate the influence of each study or a group of studies on the overall risk estimate at a time; for instance, studies with a small sample size or with a low-quality score were deleted. Potential publication bias was assessed through the visual inspection of Begg’s funnel plot in which the log ORs were plotted against their standard errors (SEs) (Begg and Mazumdar Citation1994, Egger et al. Citation1997).
Results
Study selection and characteristics
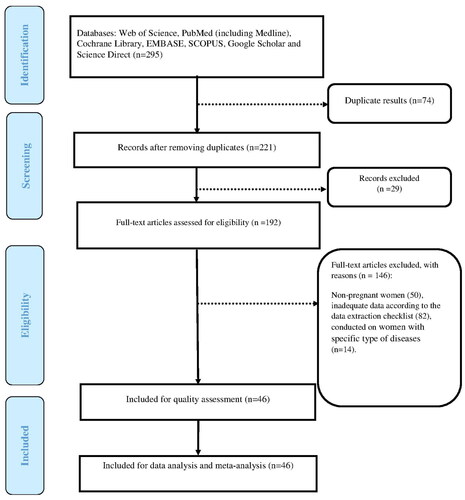
The search process led to retrieving 295 articles, of which 74 and 29 were excluded, because of duplicate titles and irrelevance to the review topic. The full-text reading led to the deletion of 132 articles based on the inclusion criteria. Moreover, the lack of a clear definition of the study population, insufficient information needed to estimate the OR and the inclusion of mothers with specific types of diseases led to the deletion of 14 more articles. Finally, 46 articles were eligible criteria and included in the review ().
Figure 1. The PRISMA flow diagram.
A total of 46 articles with a sample size of 1,554,141 people, that were conducted between 1983 and 2023 were entered into the meta-analysis process. They included 30 cohort studies (Alijahan et al. Citation2014, Arafa et al. Citation2000, Awoleke Citation2012, Batzofin et al. Citation1994, Bushtyreva et al. Citation2015, Dadkhah et al. Citation2012, De Sutter et al. Citation2006, Enaruna et al. Citation2020, Hasan et al. Citation2009, Karim Citation1998, Khalajinia and Sadeghimoghadam Citation2011, Kim et al. Citation2005, Lykke et al. Citation2010, McPherson et al. Citation2013, Norman et al. Citation2010, Palatnik and Grobman Citation2015, Ramaeker and Simhan Citation2012, Riahinejad et al. Citation2011, Salim et al. Citation2020, Schuster et al. Citation2022, sengodan et al. Citation2016, Sharami et al. Citation2013, Smits et al. Citation2012, Sohrabi and Ghanbarigorgani Citation2010, Strobino and Pantel-Silverman Citation1989, Suganya and Subbarayan Citation2019, Williams et al. Citation1991, Yakıştıran et al. Citation2015, Yang et al. Citation2004, Yazdani et al. Citation2015) and 16 case-control studies (Addisu et al. Citation2020, Akhavan Citation2004, Ananth et al. Citation2006, Berkowitz et al. Citation1983, Edwards et al. Citation2012, Eskild and Vatten Citation2009, Guruvare et al. Citation2015, Hossain et al. Citation2007, Ishtiaq et al. Citation2014, Kayode et al. Citation2016, Lykke et al. Citation2010, Nagy et al. Citation2005, Pitaphrom and Sukcharoen Citation2006, Sipilä et al. Citation1992, Sun et al. Citation2012, Szymusik et al. Citation2015). Of the 46 included studies, 11 were assessed as moderate quality, 35 as high quality and none of the included studies were assessed as being of Low quality. The characteristics of the studies are described in Table S1.
Synthesis of results
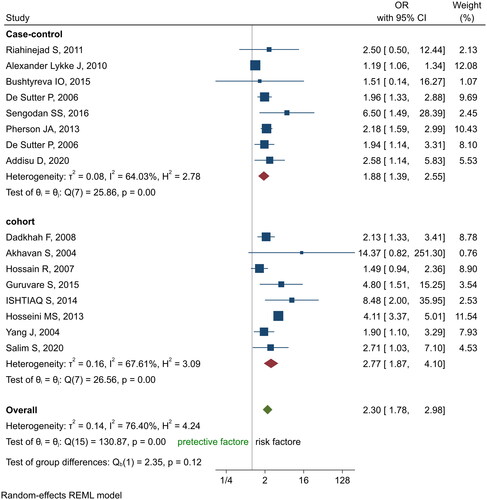
The association between vaginal bleeding during the first trimester of pregnancy and PROM was investigated based on the findings of 15 studies (Addisu et al. Citation2020, Akhavan Citation2004, Bushtyreva et al. Citation2015, Dadkhah et al. Citation2012, De Sutter et al. Citation2006, Guruvare et al. Citation2015, Hoseini and Yaghoubipour Citation2012, Hossain et al. Citation2007, Ishtiaq et al. Citation2014, Lykke et al. Citation2010, McPherson et al. Citation2013, Riahinejad et al. Citation2011, Salim et al. Citation2020, Sengodan et al. Citation2016, Suganya and Subbarayan Citation2019) with a sample size of 92,822 women. Vaginal bleeding during the first trimester of pregnancy significantly increased PROM in pregnant women (OR 2.3, CI 95%: 1.8, 3.0). The I2 index was reported 76.4% indicating a high degree of heterogeneity of the studies (p < 0.001). Therefore, the random effects model was used to analyse the data ().
Figure 2. Forest plots of the odds ratio of vaginal bleeding during the first trimester of pregnancy with PROM and 95% confidence interval based on a random effect model in meta-analysis.
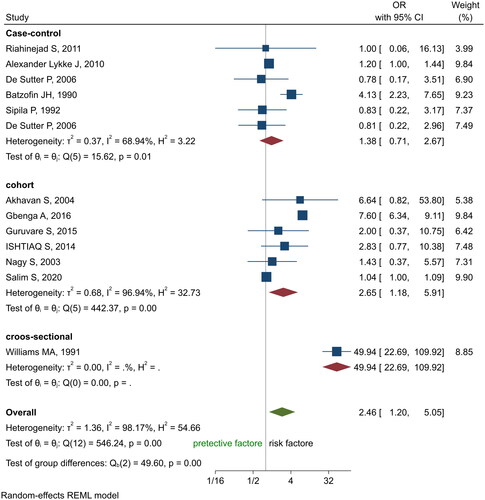
The relationship between vaginal bleeding during the first trimester of pregnancy and stillbirth was assessed using the findings of 13 studies (Akhavan Citation2004, Batzofin et al. Citation1994, De Sutter et al. Citation2006, Guruvare et al. Citation2015, Ishtiaq et al. Citation2014, Kayode et al. Citation2016, Lykke et al. Citation2010, Nagy et al. Citation2005, Riahinejad et al. Citation2011, Salim et al. Citation2020, Sipilä et al. Citation1992, Suganya and Subbarayan Citation2019, Williams et al. Citation1991) conducted between 1990 and 2020 and with a sample size of 122,297 women. It was found that bleeding during the first trimester of pregnancy significantly increased the risk of stillbirths (RR 2.5, CI 95%: 1.2, 5.0) ().
Figure 3. Forest plots of the odds ratio of vaginal bleeding during the first trimester of pregnancy with stillbirth and 95% confidence interval based on a random effect model in meta-analysis.
Also, the meta-analysis of 11 studies with a sample size of 410,078 women on the assessment of the odds of preeclampsia concerning vaginal bleeding during the first trimester of pregnancy showed that the odd ratio of preeclampsia in women with vaginal bleeding during the first trimester of pregnancy was 1.5 times greater than that of women without a history of bleeding. However, this association was statistically significant (CI 95%: 1.1, 1.9). The I2 index was reported 61.4% (, ).
Figure 4. Forest plots of the odds ratio of vaginal bleeding during the first trimester of pregnancy with preeclampsia and 95% confidence interval based on a random effect model in meta-analysis.
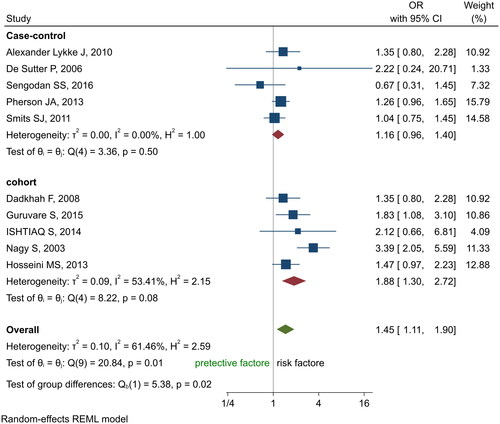
Table 1. Associations between vaginal bleeding in the first trimester of pregnancy with clinical outcomes in mother and infant based on random effect meta-analysis.
Vaginal bleeding during the first trimester of pregnancy significantly increased LBW (RR 2.0, 1.5–2.6), preterm birth (RR 1.8, 1.6–2.0), abortion (RR 4.3, 2.0–9.0), placental abruption (RR 2.2, 1.4–3.3), placental previa (RR 1.9, 1.5–2.4) and admission to the NICU (RR 2.4, 1.1–4.0) (). There was no statistically significant relationship between caesarean section (RR 1.0, 0.9–1.2), IUGR (RR 1.2, 0.7–1.9), low Apgar score (RR 1.6, 0.9−2.6), and bleeding during the first trimester of pregnancy (). Regarding the relationship between bleeding during the first trimester of pregnancy and caesarean delivery, the I2 value was 36.5% indicating the consistency between the studies. Therefore, the fixed-effects model was used for data analysis.
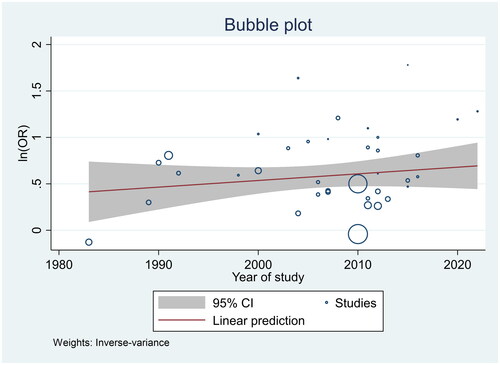
The symmetry of the diagram in the funnel plot indicated no publication bias (). Also, it was not statistically significant based on the Egger test (p = 0.24). Meta-regression based on the gradient of the chart showed a decrease in relative risk with the increase in the number of studies’ sample sizes, but it was not statistically significant (p = 0.48) (). Sensitivity analyses to investigate whether results were changed when one study was removed at a time showed a fairly robust result after removing individual studies from the meta-analysis (data are not shown).
Figure 5. Funnel chart of the odds ratio in the selected studies.
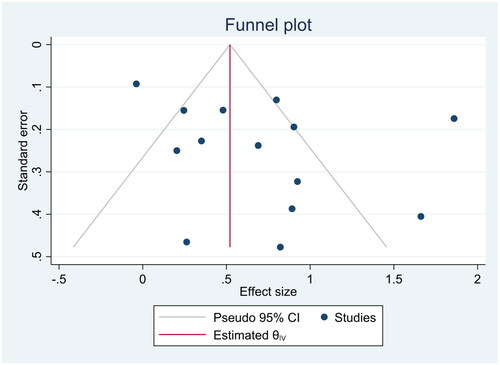
Figure 6. Meta-regression chart of the odds ratio of preterm birth upon the study year.
Discussion
This systematic review and meta-analysis were conducted with the aim of investigating the relationship between vaginal bleeding in the first trimester of pregnancy and clinical outcomes in mothers and infants. In this study, vaginal bleeding in the first trimester of pregnancy was associated with PROM. In the studies conducted, between 14% and 19.4% of women with a history of vaginal bleeding in the first trimester of pregnancy had PROM (Davari-Tanha et al. Citation2008, Hossain et al. Citation2007, Sarmalkar et al. Citation2016). In Oppenraaij et al.’s (Citation2009) and Saraswat et al.’s (Citation2010) review studies (OR 1.78, 95% CI 1.28, 2.48) the risk of PROM was increased in women with a history of vaginal bleeding in the first trimester of pregnancy (Oppenraaij et al. Citation2009, Saraswat et al. Citation2010). A comparison of the results of the present review with those mentioned above shows that bleeding during the first trimester of pregnancy increases the risk of PROM and can have adverse effects on the foetus. Vaginal bleeding during the first trimester of pregnancy causes placental abruption, placenta previa as well as PROM (Saraswat et al. Citation2010). PROM in pregnant women causes intra-amniotic inflammation, intra-amniotic infection, chorioamnionitis and septicaemia. It can cause distress, cord compression, necrotising enterocolitis, hypoxia and pulmonary hypoplasia in the foetus (Cobo et al. Citation2011, Dars et al. Citation2014, Shim et al. Citation2004). Therefore, the prevention of bleeding during pregnancy has a major role in the reduction of PROM and its adverse effects.
In this study, preterm delivery and LBW were more common in women with a history of vaginal bleeding in the first trimester of pregnancy. Saraswat et al. showed a statistically significant relationship between LBW (OR 1.83, CI 95%: 1.48–2.88), preterm birth (OR: 2.05 CI 95%: 1.76–4.2) and bleeding history during the first trimester of pregnancy (Saraswat et al. Citation2010). In other studies, the risk of preterm birth and LBW was increased in these women (Oppenraaij et al. Citation2009, Tuuli et al. Citation2011). However, multiple births, PROM and exposure to domestic violence are associated with LBW and preterm birth and can affect the relationship between bleeding and adverse pregnancy outcomes (Karimi et al. Citation2016).
Bleeding during pregnancy can be associated with PROM, placental previa, and placental abruption. At 28–34 weeks of gestation, it can lead to preterm birth and LBW (Szymusik et al. Citation2015, Tuuli et al. Citation2011, Williams et al. Citation1991, Xiao 2019, Yakıştıran et al. Citation2015). As a result, premature birth and LBW have significant effects on the infant’s growth and development (Tuuli et al. Citation2011).
The results of this meta-analysis showed that placental abruption and placental previa were more common in women with a history of vaginal bleeding in the first trimester of pregnancy. However, this relationship is bilateral, and about 1% of the causes of bleeding in pregnancy are attributed to placental abruption (Baumfeld et al. Citation2017, Oyelese and Ananth Citation2006, Tuuli et al. Citation2011). In the conducted studies, the prevalence of placental abruption and placental previa in women with a history of vaginal bleeding is 1% and 2%, respectively, and the risk of placental abruption and placental previa in women with a history of bleeding in the first trimester of pregnancy is higher compared to other women (Amirkhani et al. Citation2013, Mulik et al. Citation2004, Norman et al. Citation2010, Oppenraaij et al. Citation2009, Sarmalkar et al. Citation2016). In a study by Tuuli et al. bleeding during pregnancy increases the risk of developing placental abruption by 5.7 times (Tuuli et al. Citation2011).
Our meta-analysis showed the risk of vaginal bleeding during the first trimester of pregnancy to the risk of placental abruption and placental previa. In women with placental abruption, foetal death occurs in 50% of cases. Also, placental abruption and placental previa, especially in less than 34 weeks of gestation, can lead to premature birth and LBW (Ishtiaq et al. Citation2014, Williams et al. Citation1991). Accordingly, the occurrence of placental abruption and placental previa is of particular importance due to their effects on the foetus’s health.
In this review, bleeding in the first trimester of pregnancy was associated with an increase in miscarriage and stillbirth. In the study of Saraswat, women with a history of bleeding during the first trimester of pregnancy had a higher rate of abortion incidents (OR: 2.15) in comparison with those women without a history of bleeding (Saraswat et al. Citation2010). This rate was 7%, 21% and 17% in the studies of Sarmalkar et al. (Citation2016), Agarwal (2014) and Ahmed et al. (Citation2012), respectively (Ahmed et al. Citation2012, Grawal et al. Citation2014, Sarmalkar et al. Citation2016). Tuuli et al. showed that bleeding during the first trimester of pregnancy increased the risk of abortion and incidence of stillbirth by 2.18 and 2.9 times, respectively (Tuuli et al. Citation2011). Bleeding during the first trimester of pregnancy causes abnormalities in the growth and development of the foetus (Bever et al. Citation2018). Therefore, as a risk factor, it can increase the probability of abortion and stillbirth, which deserves serious consideration. The fate of 50% of foetuses in women with bleeding during pregnancy due to placental abruption and placental previa is stillbirth or miscarriage. Also, PROM as a result of bleeding in the first trimester of pregnancy can lead to premature birth and miscarriage.
This meta-analysis showed no significant association between bleeding during the first trimester of pregnancy and preeclampsia, caesarean delivery, IUGR, low Apgar score and admission to the NICU. Similarly, in the study of Saraswat et al. (Citation2010), preeclampsia (OR: 0.99, CI 95%: 0.84–1.17) and caesarean section (OR: 0.92, CI 95% 0.73–1.16) had no significant correlations with the history of bleeding during the first trimester of pregnancy. However, there was a significant relationship between the Apgar score of less than 7 in the fifth minute (OR 1.2, 95% CI: 1.03–1.4), IUGR (OR: 1.54 CI 95%: 1.18–2.0), admission to the NICU (OR 1.13, CI 95%: 1.03–1.23) and the history of vaginal bleeding during the first trimester of pregnancy. Inconsistency between our review results and those of Saraswat’s research can be due to the lower number of included studies in Saraswat’s study (Saraswat et al. Citation2010). In the study by Norman et al. no significant relationship was found between bleeding during pregnancy and preeclampsia as well as IUGR (Norman et al. Citation2010). In this review, although bleeding during the first trimester of pregnancy increased the risk of preeclampsia, IUGR, caesarean section, Apgar score < 7, and admission to the NICU, it was not statistically significant. Therefore, it cannot be conclusively stated that bleeding during pregnancy increases related adverse clinical outcomes.
Strengths and limitations
In our review, nearly all included studies were medium to high quality according to the NOS. Likewise, the quality of meta-analyses is mainly reliant on the quality of the original studies included in data analysis. The current meta-analysis included prospective cohort studies that were valuable for assessing the cause-and-effect association. Therefore, our findings can have implications for interventions aiming at the prevention of adverse pregnancy clinical outcomes. In this review, different adverse clinical effects of pregnancy were simultaneously included to avoid splitting results in different reports across the globe, which improved its generalisability. However, the following limitations should be considered during the interpretation of the findings: there was a lack of integrated definition for LBW in the studies (birth weight <2500 g or <2000 g). In this study, the weight was considered less than 2500 g. Also, in the field of premature birth, in the studies, the gestational age was reported to be less than 37 or 34 weeks, and in this study, the age was considered to be less than 37 weeks. Not reporting the OR or the information needed to estimate it, which led to the exclusion of some studies; the presence of unmatched participants, or uncontrolled confounder variables in some studies that might have affected the pooled estimates; unknown sources of heterogeneity amongst the studies.
Conclusions
Bleeding during the first trimester of pregnancy increases the chance of preterm birth, PROM, LBW, abortion, stillbirth, placental abruption and placental previa. Hence, it is essential to identify the causes of this phenomenon and take appropriate healthcare measures to prevent bleeding during pregnancy, and pay special attention to its undesirable clinical outcomes.
Ethics approval
This study was approved by Shahroud University of Medical Sciences (Ethical code: IR.SHMU.REC.1399.025).
Contributions to authorship
Arezoo Karimi: Data collection, data extraction, writing the manuscript, approval of the final version to be published;
Kourosh Sayehmiri: Data analysis and interpretation and quality appraisals, approval of the final version to be published;
Salman Daliri: Data collection, data extraction, writing the manuscript, approval of the final version to be published;
Mojtaba Vaismoradi: Writing the manuscript, critical interpretation of content, approval of the final version to be published;
Mostafa Dianatinasab: Writing the manuscript, critical interpretation of content; approval of the final version to be published.
Supplemental Material
Download MS Word (32.2 KB)Acknowledgements
The authors would like to thank the Deputy of Research and Technical Information of Shahroud University of Medical Sciences for supporting this research.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article [and/or] its Supplementary materials.
Additional information
Funding
References
- Addisu, D., Melkie, A. and Biru, S., 2020. Prevalence of preterm premature rupture of membrane and its associated factors among pregnant women admitted in Debre Tabor General Hospital, North West Ethiopia: institutional-based cross-sectional study. Obstetrics and Gynecology International, 2020, 4034680–4034687.
- Ahmed, S., et al., 2012. Pregnancy outcome in women with threatened miscarriage: a year study. Materia Socio-Medica, 24 (1), 26–28.
- Akhavan, S., 2004. Pregnancy outcomes in patients with subcoronary hemorrhage in the first trimester of gestation compared with the control group in patients referring to specialized clinics in the years 81 and 82. Journal of Kourdestan University Medical Science, 9 (33), 31–36.
- Alijahan, R., et al., 2014. Prevalence and risk factors associated with preterm birth in Ardabil, Iran. Iranian Journal of Reproductive Medicine, 12 (1), 47–56.
- Amirkhani, Z., et al., 2013. Maternal and perinatal outcomes in pregnant women with first trimester vaginal bleeding. Journal of Family and Reproductive Health, 7 (2), 57–61.
- Ananth, C.V., et al., 2006. Evidence of placental abruption as a chronic process: associations with vaginal bleeding early in pregnancy and placental lesions. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 128 (1–2), 15–21.
- Arafa, M., et al., 2000. Outcomes of pregnancies complicated by early vaginal bleeding. Eastern Mediterranean Health Journal, 6 (2–3), 457–464.
- Awoleke, J., 2012. Maternal risk factors for low birth weight babies in Lagos, Nigeria. Archives of Gynecology and Obstetrics, 285 (1), 1–6.
- Batzofin, J., Fielding, W. and Fridman, E., 1994. effect of vaginal bleeding in early pregnancy on outcom. Obstetrics & Gynecology, 63 (4), 515–518.
- Baumfeld, Y., et al., 2017. Placenta associated pregnancy complications in pregnancies complicated with placenta previa. Taiwanese Journal of Obstetrics & Gynecology, 56 (3), 331–335.
- Begg, C.B. and Mazumdar, M., 1994. Operating characteristics of a rank correlation test for publication bias. Biometrics, 50 (4), 1088–1101.
- Berkowitz, G.S., et al., 1983. Early gastational bleeding and pregnancy outcome: a multivariable analysis. International Journal of Epidemiology, 12 (2), 165–173.
- Bever, A.M., et al., 2018. Fetal growth patterns in pregnancies with first-trimester bleeding. Obstetrics and Gynecology, 131 (6), 1021–1030.
- Bushtyreva, I.O., et al., 2015. Pregnancy outcomes in pregnant women with subchorionic hematoma. International Journal of Biomedicine, 5 (3), 137–140.
- Cobo, T., et al., 2011. Clinical and inflammatory markers in amniotic fluid as predictors of adverse outcomes in preterm premature rupture of membranes. American Journal of Obstetrics and Gynecology, 205 (2), 126. e121-126–e128.
- Dadkhah, F., Kashanian, M. and Eliasey, G., 2012. Pregnancy outcomes in pregnant women with history of vaginal bleeding in the first half of pregnancy. Urmia Medical Journal, 23 (3), 254–259.
- Dars, S., et al., 2014. Maternal morbidity and perinatal outcome in preterm premature rupture of membranes before 37 weeks gestation. Pakistan Journal of Medical Sciences, 30 (3), 626–629.
- Davari-Tanha, F., et al., 2008. Threatened abortion: a risk factor for poor pregnancy outcome. Acta Medica Iranica, 46 (4), 314–320.
- De Sutter, P., et al., 2006. First-trimester bleeding and pregnancy outcome in singletons after assisted reproduction. Human Reproduction (Oxford, England), 21 (7), 1907–1911.
- Dee Zhen, L., 2017. Effects of subchorionic haematoma on pregnancy outcomes. Australian Medical Student Journal, 8 (1), 41–45.
- Dolatian, M., et al., 2013. Preterm delivery and psycho–social determinants of health based on World Health Organization model in Iran: a narrative review. Global Journal of Health Science, 5 (1), 52.
- Dongol, A., Mool, S. and Tiwari, P., 2011. Outcome of pregnancy complicated by threatened abortion. Kathmandu University Medical Journal, 9 (33), 41–44.
- Edwards, D.V., et al., 2012. First-trimester bleeding characteristics associate with increased risk of preterm birth: data from a prospective pregnancy cohort. Human Reproduction, 27 (1), 54–60.
- Egger, M., et al., 1997. Bias in meta-analysis detected by a simple, graphical test. BMJ, 315 (7109), 629–634.
- Enaruna, N., Anya, C. and Anyanwu, C., 2020. Early and late pregnancy complications in women who experience first trimester vaginal bleeding at a University Hospital, Benin City, Nigeria. Journal of Medicine and Biomedical Research, 19 (1), 23–32.
- Eskild, A. and Vatten, L., 2009. Abnormal bleeding associated with preeclampsia: a population study of 315,085 pregnancies. Acta Obstetricia et Gynecologica Scandinavica, 88 (2), 154–158.
- Grawal, S., et al., 2014. A predicting adverse maternal and perinatal outcome after threatened miscarriage. Open Journal of Obstetrics and Gynecology, 04 (01), 1–7.
- Guruvare, S., et al., 2015. Factors influencing pregnancy outcome in women with vaginal bleeding before midpregnancy: a prospective case control study. International Journal of Reproduction, Contraception, Obstetrics and Gynecology, 4 (3), 601–605.
- Hasan, R., et al., 2010. Patterns and predictors of vaginal bleeding in the firsttrimester of pregnancy. Annals of Epidemiology, 20 (7), 524–531.
- Hasan, R., et al., 2009. Association between first-trimester vaginal bleeding and miscarriage. Obstetrics and Gynecology, 114 (4), 860–867.
- Hoseini, M. and Yaghoubipour, S., 2012. The role of vaginal bleeding in the first trimester of pregnancy on late pregnancy outcomes. Scientific Journal of the Islamic Republic of Iran Medical Organization, 30 (3), 250–255.
- Hossain, R., et al., 2007. Risk of preterm delivery in relation to vaginal bleeding in early pregnancy. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 135 (2), 158–163.
- Huedo-Medina, T.B., et al., 2006. Assessing heterogeneity in meta-analysis: q statistic or I2 index? Psychological Methods, 11 (2), 193–206.
- Ishtiaq, S., Qadir, T., and SHarafali, H., 2014. Maternal and perinatal outcom in threatened miscarriage in first trimester. Isra Medical Journal, 6 (3), 169–172.
- Karim, S.A., 1998. Effects of first and second trimester vaginal bleeding on pregnancy outcome. Journal of the Pakistan Medical Association, 48 (2), 40–42.
- Karimi, A., Daliri, S., and SayehMiri, K., 2016. The relationship between violence during pregnancy and low birth weight: a meta-analysis study. Hayat, Journal of School of Nursing and Midwifery, Tehran University of Medical Sciences, 22 (3), 216–228.
- Kayode, G.A., et al., 2016. Predicting stillbirth in a low resource setting. BMC Pregnancy and Childbirth, 16 (1), 1–8.
- Khalajinia, Z. and Sadeghimoghadam, P., 2011. Incidence and maternal risk factors related to preterm delivery in qom province, 2007. Journal of Qom University of Medical Sciences, 5 (1), 30–36.
- Kim, Y., et al., 2005. Risk factors for preterm birth in Korea: a multicenter prospective study. Gynecologic and Obstetric Investigation, 60 (4), 206–212.
- Liberati, A., et al., 2009. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Medicine, 6 (7), e1000100.
- Lykke, J., et al., 2010. First-trimester vaginal bleeding and complications later in pregnancy. Obstetrics and Gynecology, 115 (5), 935–944.
- Madan, I., et al., 2010. The frequency and clinical significance of intra-amniotic infection and/or inflammation in women with placenta previa and vaginal bleeding: an unexpected observation. Journal of Perinatal Medicine, 38 (3), 275–279.
- McPherson, J. A., et al., 2013. Adverse outcomes in twin pregnancies complicated by early vaginal bleeding. American Journal of Obstetrics and Gynecology, 208 (1), 56.e1–5.
- Morisaki, N., et al., 2014. Risk factors for spontaneous and provider‐initiated preterm delivery in high and low Human Development Index countries: a secondary analysis of the World Health Organization Multicountry Survey on Maternal and Newborn Health. BJOG: An International Journal of Obstetrics and Gynaecology, 121 (s1), 101–109.
- Mulik, V., Bethel, J. and Bhal, K., 2004. A Retrospective population-based study of primigravid women on the potential effect of threatened miscarriage on obstetric outcome. Journal of Obstetrics and Gynaecology: The Journal of the Institute of Obstetrics and Gynaecology, 24 (3), 249–253.
- Mustafa, G., et al., 2009. Pregnancy outcome of patients complicated by threatened abortion. The Internet Journal of Gynecology and Obstetrics, 14, 1–4.
- Nagy, S., et al., 2005. Clinical significance of subchorionic and retroplacental hematomas detected in the first trimester of pregnancy. Orvosi Hetilap, 146 (42), 2157–2161.
- Norman, S., et al., 2010. Ultrasound-detected subchorionic hemorrhage and the obstetric implications. Obstetrics and Gynecology, 116 (2 Pt 1), 311–315.
- Nour, N.M., 2012. Premature delivery and the millennium development goal. Reviews in Obstetrics and Gynecology, 5 (2), 100.
- Oppenraaij, R. V., et al., 2009. Predicting adverse obstetric outcome after early pregnancy events and complications: a review. Human Reproduction Update, 15 (4), 409–421.
- Oyelese, Y. and Ananth, C.V., 2006. Placental abruption. Obstetrics and Gynecology, 108 (4), 1005–1016.
- Palatnik, A. and Grobman, W., 2015. The relationship between first-trimester subchorionic hematoma, cervical length, and preterm birth. American Journal of Obstetrics and Gynecology, 213 (3), 403.e1–4.
- Peterson, J., et al., 2011. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hospital Research Institute, 2 (1), 1–12.
- Pitaphrom, A. and Sukcharoen, N., 2006. Pregnancy outcomes in placental abruption. Journal of the Medical Association of Thailand = Chotmaihet Thangphaet, 89 (10), 1572–1578.
- Ramaeker, D.M. and Simhan, H.N., 2012. Sonographic cervical length, vaginal bleeding, and the risk of preterm birth. American Journal of Obstetrics and Gynecology, 206 (3), 224. e221-224–e224.
- Riahinejad, S., et al., 2011. Effect of vaginal bleeding in first trimester of pregnancy on pregnancy Outcomes. Journal of Isfahan Medical School, 29 (156), 1296–1302.
- Salim, S., Ravishankar, D., and Vg, V.K., 2020. A study on first trimester vaginal bleeding and outcome of pregnancy in Thiruvananthapuram, Kerala. Age (Years), 19 (4), 400.
- Saraswat, L., et al., 2010. Maternal and perinatal outcome in women with threatened miscarriage in the first trimester: a systematic review. BJOG: An International Journal of Obstetrics and Gynaecology, 117 (3), 245–257.
- Sarmalkar, M.S., Singh, S., and Nayak, A.H., 2016. Maternal and perinatal outcome in women with threatened abortion in first trimester. International Journal of Reproduction, Contraception, Obstetrics and Gynecology, 5 (5), 1438–1445.
- Schuster, H.J., et al., 2022. Risk factors for spontaneous preterm birth among healthy nulliparous pregnant women in the Netherlands, a prospective cohort study. Health Science Reports, 5 (3), e585.
- Sengodan, S. S., Dhanapal, M. and Subramanian, V., 2016. Pregnancy Outcome in First Trimester Bleed. Indian Journal of Applied Research, 6 (7), 46–53.
- Sharami, S.H., et al., 2013. The relationship between vaginal bleeding in the first and second trimester of pregnancy and preterm labor. International Journal of Reproductive BioMedicine, 11 (5), 385–390.
- Shim, S. S., et al., 2004. Clinical significance of intra-amniotic inflammation in patients with preterm premature rupture of membranes. American Journal of Obstetrics and Gynecology, 191 (4), 1339–1345.
- Sipilä, P., et al., 1992. Perinatal outcome of pregnancies complicated by vaginal bleeding. British Journal of Obstetrics and Gynaecology, 99 (12), 959–963.
- Smits, L.J., et al., 2012. Patterns of vaginal bleeding during the first 20 weeks of pregnancy and risk of pre-eclampsia in nulliparous women: results from the SCOPE study. Acta Obstetricia et Gynecologica Scandinavica, 91 (11), 1331–1338.
- Sohrabi, D. and Ghanbarigorgani, M., 2010. Study of some risk factors of pregnancy on preterm delivery in mothers referred to Valiasr Hospital in Zanjan in 2007. Journal of Faculty of Nursing and Midwifery, Urmia, 9 (31), 84–89.
- Strobino, B. and Pantel-Silverman, J., 1989. Gestational vaginal bleeding and pregnancy outcome. American Journal of Epidemiology, 129 (4), 806–815.
- Suganya, K. and Subbarayan, L.M., 2019. Maternal and perinatal outcomes in women with first trimester vaginal bleeding. Journal of Family and Reproductive Health, 8 (11), 4.
- Sun, L., et al., 2012. First trimester vaginal bleeding and adverse pregnancy outcomes among Chinese women: from a large cohort study in China. The Journal of Maternal-Fetal & Neonatal Medicine, 25 (8), 1297–1301.
- Sutter, P.D., et al., 2006. First-trimester bleeding and pregnancy outcome in singletons after assisted reproduction. Human Reproduction, 21 (7), 1907–1911.
- Szymusik, I., et al., 2015. The association of first trimester bleeding with preterm delivery. Journal of Perinatal Medicine, 43 (5), 525–529.
- Tenny, S. and Hoffman, M., 2023. Odds ratio. StatPearls [Internet]. Tampa, FL: StatPearls Publishing. [Updated 2023 May 22]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431098/
- Tuuli, M., et al., 2011. Perinatal outcomes in women with subchorionic hematoma: a systematic review and meta-analysis. Obstetrics and Gynecology, 117 (5), 1205–1212.
- Williams, M.A., et al., 1991. Adverse infant outcomes associated with first-trimester vaginal bleeding. Obstetrics and Gynecology, 78 (1), 14–18.
- Yakıştıran, B., Yüce, T. and Söylemez, F., 2015. First trimester bleeding and pregnancy outcomes: case-control study. International Journal of Women’s Health and Reproduction Sciences, 4 (1), 4–7.
- Yang, J., et al., 2004. Vaginal bleeding during pregnancy and preterm birth. American Journal of Epidemiology, 160 (2), 118–125.
- Yazdani, S., et al., 2015. the comparition of the risk factors in the term and preterm delivery. j Babol Univ Med Sci, 16 (15), 7–12.