

Abstract
Background
Women with obesity are at increased risk of excessive gestational weight gain. Women with a body mass index (BMI) of 40 kg/m2 or more are known to have different patterns of weight gain than women with lower levels of obesity. This study therefore aimed to determine the characteristics associated with gestational weight gain (GWG) among women with a BMI of 40 kg/m2 or more.
Methods
Secondary analysis was undertaken on a retrospective cohort of women with a BMI of 40 kg/m2 or more, with a singleton pregnancy referred to an antenatal healthy lifestyle service between 2009 and 2015 (n = 735). GWG was calculated by subtracting weight at the first antenatal appointment from final recorded weight in pregnancy provided the final weight was recorded from at least 34 + 0 weeks gestation. Univariable and multiple linear regression analyses were employed to determine the association between GWG and different maternal and infant characteristics.
Results
Average GWG among women with a BMI of 40 kg/m2 or more was 6.0 (±7.1)kg. Multiple regression showed GWG decreased with increasing BMI and increasing parity. Other socio-demographic factors were also significantly associated with GWG, with higher GWG seen among those with high levels of deprivation, where the highest household occupation was of a manual nature, in older women and women of non-White British ethnicity.
Conclusion
GWG in this cohort of women with a BMI of 40 kg/m2 or more was within Institute of Medicine recommendations. Using a systems approach to GWG management that incorporates biological, psychological and socio-ecological factors is important.
PLAIN ENGLISH SUMMARY
Women with the highest levels of obesity are known to have different patterns of weight gain during pregnancy than other women. This study looked at what factors were linked to pregnancy weight gain in women with the highest levels of obesity. Pregnancy weight gain was calculated by subtracting the woman’s weight at her first pregnancy appointment from her weight at the end of pregnancy, providing she was at least 34 weeks pregnant when she was weighed.
The higher the woman’s body mass index above 40 kg/m2 at the start of pregnancy, the less weight they gained in pregnancy. Women gained less weight during pregnancy if they already had one or more children rather than were having their first baby or if they lived in households where no one worked. Weight gain was also linked to whether the woman lived in a deprived area and weight gain was higher in women from an ethnic minority. In the future any interventions during pregnancy to help women gain the correct amount of weight need to consider multiple things including how many children they already have, as well as the influence of the woman’s family and friends and where the woman lives.
Introduction
A body mass index (BMI) of 25.0–29.9 kg/m2 is classified as overweight and a BMI ≥30kg/m2 as obese, with obesity subdivided into three classes, class I (BMI 30.00–34.99 kg/m2), class II (BMI 35.00–39.99 kg/m2) and class III (BMI ≥40.00 kg/m2) (WHO 2000). Across most of the globe overweight and obesity during pregnancy has increased over recent decades (Devlieger et al. Citation2016). In England rates of obesity during pregnancy have approximately tripled from 7.6% in 1989 (Heslehurst et al. Citation2010) to 22.2% in 2018–2019 (National Health Service (NHS) Digital Citation2019). Individuals with the highest levels of obesity (BMI ≥40kg/m2) were rare several decades ago. However, recently the incidence of women with a BMI ≥40kg/m2 in early pregnancy has been found to vary being 1.6% in Spain (Williamson et al. Citation2020), 3.3% in England (Public Health England (PHE)), 2019a) and 9.7% in the United States (Williamson et al. Citation2020).
Numerous adverse risks are associated with maternal obesity during pregnancy for both the woman and neonate (Lutsiv et al. Citation2015; Santos et al. Citation2019). Maternal overweight or obesity are estimated to be linked to 23.9% of pregnancy complications, with the highest risk of complications occurring in women with a BMI ≥40kg/m2 (Santos et al. Citation2019). Additionally, women with obesity prior to pregnancy are at increased risk of excessive gestational weight gain (GWG) (Samura et al. Citation2016). The Institute of Medicine (IOM) recommends a GWG between 5 and 9 kg for women with obesity (Rasmussen & Yaktin Citation2009). However, 44% of women with obesity gain more than this recommended weight (Rogozińska et al. Citation2017). Increased GWG is itself associated with many adverse outcomes such as increased risk of caesarean birth (Goldstein et al. Citation2017), labour induction (Xu et al. Citation2021), large for gestational age infants (Santos et al. Citation2019; Goldstein et al. Citation2017), long term maternal weight retention (Samura et al. Citation2016), and childhood obesity (Voerman et al. Citation2019).
Several studies have explored whether factors such as maternal age, ethnicity, parity, socio-economic status, marital status, education, and smoking status are associated with GWG (Lindberg et al. Citation2016; Samura et al. Citation2016; Garmendia et al. Citation2017; Emery et al. Citation2021; Cheng et al. Citation2021). Women with a BMI ≥40kg/m2 are at the highest risk of many adverse pregnancy outcomes (Lutsiv et al. Citation2015; Santos et al. Citation2019; D’Souza et al. Citation2019) and are known to have different GWG patterns to other women with lower levels of obesity (Lindberg et al. Citation2016). However, women with a BMI ≥40kg/m2 are underrepresented in current research, with no studies specifically looking at factors associated with GWG among this subgroup of women. Given the increasing prevalence of women with a BMI ≥40kg/m2 attending for perinatal care (Devlieger et al. Citation2016), better understanding of the factors associated with GWG in this group of women is particularly pertinent.
The objective of this study was therefore to determine the characteristics associated with GWG among women with a BMI of 40 kg/m2 or more.
Methods
Participants and procedures
Secondary analysis of a retrospective cohort study was undertaken of women who booked for antenatal care from July 2009 to 2015 in a National Health Service Trust in the Yorkshire and Humber region of England. This Trust had high rates of maternal obesity and deprivation compared to the rest of England (Public Health England (PHE) Citation2019b). Women were eligible for inclusion if they had a BMI ≥40kg/m2 when first attending for antenatal care and had a singleton pregnancy that remained viable at 24 weeks gestation. Maternal and neonatal data were obtained from routinely collected pregnancy and birth health records.
At the NHS Trust during this time women with a BMI ≥40kg/m2 were offered access to a midwife-led antenatal healthy lifestyle service. This has been described in full elsewhere (West Citation2010; Fair and Soltani Citation2023). At this service women were routinely offered either one (July 2009–2011) or three visits (2012–2015), with women also able to access the service for additional appointments if they desired. Women were offered support and advice at this service covering four key aspects: minimising GWG, healthy eating, undertaking physical activity, and breastfeeding.
Measures
Sociodemographic data
At the first antenatal appointment women self-reported educational level, smoking status, marital status and ethnicity, as well as the occupation of herself and her partner. The highest occupation category for each household (either the woman or her partner) was calculated using the three category National Statistics Socio-Economic Classification (NS-SEC) system (Office for National Statistics (ONS), Citation2010). Furthermore, postcode was used to determine an Index of Multiple Deprivation (IMD) score. This is the official measure of relative deprivation in England, combining information from seven domains (income, employment, education, health, crime, housing and living environment) to give an overall score from 1 (most deprived) to 32844 (least deprived) (Smith et al. Citation2015). These scores were designated into quintiles.
Maternal BMI
BMI was calculated using weight and height measured at the first antenatal appointment. In a small minority of cases (n = 9) BMI was obtained from the medical records as weight or height were not recorded to calculate BMI independently.
Pregnancy and intrapartum data
Women self-reported parity. Other pregnancy and intrapartum related data were documented by healthcare providers such as, birthweight and infant sex, as well as expected date of birth on ultrasound from which gestation at appointments and birth were calculated.
Gestational weight gain
The final recorded weight in pregnancy was used, providing the gestation of this weight was at least the middle of the third trimester (34 + 0 weeks gestation). If a weight was not recorded from 34 + 0 weeks gestation onwards the woman was classified as not having GWG recorded. GWG was determined by subtracting weight at the first antenatal appointment from final weight. Given variation in GWG timings, gestation at the first and last recorded weight in pregnancy were adjusted for within the multiple regression analysis.
Statistical analysis
Logical checks and data cleaning were carried out and inconsistencies returned to the field for clarification. Characteristics were compared between women who had GWG recorded (n = 618) and those who did not (n = 117) using student’s t-test or Chi-square test. For women who had a recorded GWG, the independent relationship between GWG and maternal socio-demographic characteristics, pregnancy characteristics and infant characteristics were explored using linear regression with GWG as the dependent variable. Variables were chosen by consulting previous literature on the topic (Lindberg et al. Citation2016; Samura et al. Citation2016; Garmendia et al. Citation2017; Emery et al. Citation2021; Cheng et al. Citation2021). Factors were then entered into a multiple regression main effects linear model to determine the significance of each variable on GWG once controlling for other factors. The multiple regression model was adjusted for birthweight, gestation at the first antenatal weight, gestation at the final recorded weight and gestation at birth. Education was omitted from the multiple regression model due to the large number of missing cases. Additionally marital status was omitted from the multiple regression model as this factor had high variance inflation factors leading to concerns over multi-collinearity. A separate model was constructed for women whose pregnancies were not complicated by either diabetes (type 1, type 2 or gestational) or hypertension (pre-existing or pregnancy induced). For each linear regression model, assumptions were checked using standard regression diagnostics for linearity, normality, leverage and influence. Where outliers or points of potentially high leverage were identified, data analysis was rerun after removal of these points to determine any impact on the significance or direction of the effect size. Where differences in the magnitude or direction of the effect size were noted, both effect sizes have been presented. For all models the unstandardised β co-efficient alongside its 95% confidence interval (CI) are presented. p < 0.05 was regarded as statistically significant. All analyses were undertaken in SPSS 26.0.
Ethical approvals
This study was approved by the East England - Cambridge East Research Ethics Committee (IRAS: project number 207998). The need for informed consent was waived by the ethics committee due to the retrospective nature of this study.
Results
provides a flowchart of study participant selection. Of the 735 eligible women, 618 had their GWG recorded. Women with and without the primary outcome GWG were compared (). Women who already had two or more children or who gave birth prematurely were significantly less likely to have GWG recorded. Women whose highest household occupation was classified as either ‘routine or manual’ or ‘housewife/unemployed/student’ also tended to be less likely to have GWG recorded. Of women who gave birth prematurely, 64.8% (n = 46) did not have GWG recorded. These women and those who moved away from the area (n = 18) accounted for 55% of those lacking the outcome of GWG.
Figure 1. STROBE flow chart of study participant selection.
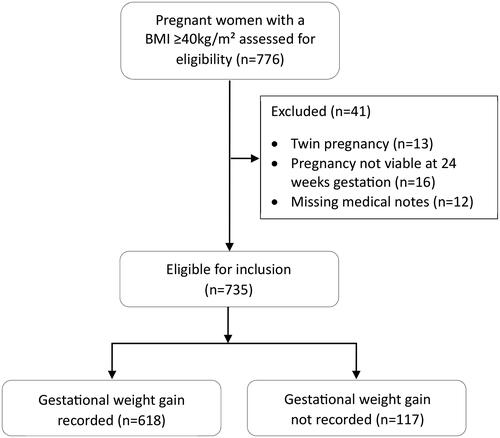
Table 1. Maternal characteristics of women with and without gestational weight gain outcome recorded.
Mean GWG was 6.0 kg (±7.1) and ranged from a weight loss of 17.6 kg to weight gain of 27.6 kg. The average gestation of the final weight was 37.4 (±1.8) weeks, with a median final weight to birth interval of 1.9 weeks (interquartile range 0.9–3.1 weeks). GWG decreased with increasing maternal BMI at the first antenatal appointment and parity (). GWG increased with ethnicity other than white British and in households with someone in employment. Compared to those in the most deprived quintile, women in the second most deprived quintile had a significantly higher weight gain during pregnancy. Compared to attending no antenatal healthy lifestyle service appointments, attending one, two or three or more appointments had no impact on GWG.
Table 2. Crude regression coefficients and 95% confidence intervals for each variable with gestational weight gain.
Within the multiple regression main effects linear model (), maternal BMI, parity, ethnicity, deprivation and highest household occupation remained significantly independently associated with GWG. However, within the multiple regression model only women whose highest household occupation was a manual occupation had higher GWG. Furthermore, maternal age became significant within the multiple regression model. This multiple regression model accounted for 21.1% of the total variance in GWG. After removing the thirteen outliers/points of high leverage (Table S1), factors significantly associated with GWG remained the same except that maternal age was no longer significant and smoking status when booking for antenatal care was associated with increased GWG. When only looking at pregnancies that were not complicated by diabetes or hypertension, the factors associated with GWG remained the same except for maternal age which was no longer significantly associated with GWG (Table S2).
Table 3. Multiple regression model of factors associated with gestational weight gain in women with a BMI ≥ 40kg/m² (n = 596).
Discussion
Average weight gain within this cohort was 6.0 kg which is within the 5–9kg range recommended for women with obesity (Rasmussen & Yaktin Citation2009). The present study showed wide variability in GWG among women with a BMI ≥40kg/m2. The multiple regression model showed that GWG decreased with increasing BMI and increasing parity. Higher GWG was seen among those with high levels of deprivation, where the highest household occupation was of a manual nature, in older women and women of non-White British ethnicity.
Previous studies and reviews of women of all BMI categories have similarly noted maternal BMI (Kirchengast and Hartmann Citation2013; Cheney et al. Citation2017), and parity (Deputy et al. Citation2015; Heery et al. Citation2015; Pawlak et al. Citation2015; Garmendia et al. Citation2017; Rogozińska et al. Citation2017; Nunnery et al. Citation2018; Cheng et al. Citation2021) to be factors associated with GWG or excessive GWG, although these factors were not always significant when adjusting for covariates. Parity has also previously been associated with GWG when specifically looking at women with obesity (Raymond et al. Citation2014; Deputy et al. Citation2015). In all instances nulliparous women had higher GWG or were at increased risk of excessive GWG.
The literature regarding deprivation is inconsistent. Low socio-economic status or proxy measures of socioeconomic status such as education, employment or housing type have been found to increase the odds of GWG below guidelines (Lindberg et al. Citation2016), increase risk of excessive GWG in early pregnancy (Cheney et al. Citation2017) and to have no significant impact on GWG (Garmendia et al. Citation2017; Cheng et al. Citation2021) even though all of the studies were undertaken in high income countries. A complicated interaction between deprivation and GWG was noted within this study. Once controlling for other factors GWG was higher in women in the second most deprived quintile compared to those in the most deprived quintile, and higher in those from a manual occupation than in those who were unemployed or a housewife. The reasons for this are unclear but may be due to women in the most deprived quintile being less able to afford a healthy lifestyle, particularly an adequate quantity of food during pregnancy. Within this cohort after controlling for confounders such as deprivation there was a trend for those who smoked to have a higher GWG, which became significant after removing outliers. Other studies have similarly shown current and previous history of smoking to be significantly associated with GWG outside of the recommended range (Kirchengast and Hartmann Citation2013; Pawlak et al. Citation2015; Lindberg et al. Citation2016), although women with a BMI ≥40kg/m2 were a small minority of these samples.
Maternal age has been noted to be associated with GWG in previous studies, with women with excessive GWG noted to be younger on average than those with inadequate or adequate GWG (Kirchengast and Hartmann Citation2013; Cheng et al. Citation2021). Others have also found women over 35 years of age to have significantly lower GWG than younger women (Heery et al. Citation2015) and for GWG to decrease with increasing maternal age (Rogozińska et al. Citation2017). This previously noted effect may in part be explained by nulliparous women having higher GWG, as only one study adjusted for parity (Rogozińska et al. Citation2017). Additionally, BMI increases with maternal age (National Health Service (NHS) Digital Citation2019) and as there is a trend for GWG to decrease with increasing BMI (Siega-Riz et al. Citation2020) this may also partly explain the lower GWG with advancing maternal age. Within our multiple regression analysis that adjusted for parity and maternal BMI there was a trend towards higher GWG with advancing maternal age after the removal of outliers.
Women of ethnicity other than white British had higher GWG within this study, despite their mean BMI being higher at the start of pregnancy. However, given the limited number of women on non-white ethnicity these results should be treated with caution. The literature regarding the impact of ethnicity on GWG provides a complex picture. One study noted that women of non-Irish nationality had increased GWG (Heery et al. Citation2015), and another that being of African American ethnicity was associated with increased odds of excess GWG (Nunnery et al. Citation2018). Others have however noted non-White ethnicity to decrease mean GWG (Rogozińska et al. Citation2017) or the odds of GWG above recommendations (Pawlak et al. Citation2015; Lindberg et al. Citation2016). These differences may be explained by the ethnic composition within the studies, as a further study found some ethnicities to be associated with inadequate GWG and others with excess GWG among women with obesity (Deputy et al. Citation2015).
Attendance at the antenatal healthy lifestyle service was not significantly associated with GWG in either the univariate or multiple regression analysis. No data was collected by the service regarding whether service attendance led to any improvements in diet or physical activity. When women with access to the antenatal healthy lifestyle service have previously been compared to women in a separate NHS Trust who did not have access to such a service, the only clinical outcome that favoured the lifestyle service was breastfeeding at discharge from the hospital (Fair and Soltani Citation2023). No impact on other outcomes such as vaginal birth, birthweight or preterm birth were noted (Fair and Soltani Citation2023).
Given the higher GWG among nulliparous women and the complex inter-ethnic variability noted within this and previous studies, the importance of adapting interventions to the needs of nulliparas and specific ethnic groups is highlighted. This is especially important given that women themselves report wanting more information in their first pregnancy (Fair et al. Citation2022). Additionally, current interventions are believed to inadequately consider culture and ethnic differences (Byrd et al. Citation2018) despite known ethnic health disparities (Jardine et al. Citation2021). Furthermore, the multifaceted interaction between GWG and ethnicity, socioeconomic status and other maternal and infant outcomes, emphasise the need to consider obesity and GWG management not just at an individual level, but through a wider lens that incorporates social, environmental, political and economic responsibilities and implications (Devlieger et al. Citation2016). A systems approach to obesity has therefore been recommended (Lee et al. Citation2017). This approach addresses all interconnected factors that contribute to obesity including the individual biological variables such as genetics and physiological aspects, psychological effects and socio-ecological factors (Lee et al. Citation2017). Incorporating socio-ecological factors moves from an exclusively individual focus to also tackle the influences on women from their family and home, work and peers, community, industry, government, culture and society (Hill Citation2021).
Strengths and limitations of the study
This study explored the factors associated with GWG within a large sample of women with a BMI ≥40kg/m2, a category often lacking in previous studies. Some limitations however need to be acknowledged. Women within this cohort had been invited to an antenatal healthy lifestyle service, however attendance at this service had no impact on GWG suggesting the results are still generalisable to a wider population. Retrospective data collection is known for its limitations around data completeness (Hasson et al. Citation2015). Poor documentation of maternal education was particularly evident within this study. Additionally, women of high parity and those whose highest household occupation was classified as housewife, unemployed or student were significantly less likely to have a final weight within the medical notes. This may have influenced the impact of these factors within the multiple regression model. The retrospective nature of the study also limited the availability of some factors previously noted in the literature to be associated with GWG such as psychosocial factors and maternal diet. Women were routinely weighed at booking and at 36 weeks gestation within the Trust with the antenatal healthy lifestyle service. To capture as many women as possible we included anyone who had a final weight recorded from 34 weeks gestation onwards. However, a large proportion of women who gave birth prematurely did not have a final weight recorded, so this study is largely applicable to women with a term or late preterm birth. Given the multiple tests undertaken within the univariate and multiple regression model the probability of a type 1 error increases; it is therefore possible that some of the findings within this study were chance findings and did not actually represent observed differences. Additionally, outliers within the multiple regression model suggested the model fitted less well for the few cases where BMI was 60 or more and when women attended for their first antenatal care appointment after 26 weeks gestation.
Conclusions
Among women with a BMI ≥40kg/m2, higher GWG was seen among those who were nulliparous, with high levels of deprivation and where the highest household occupation was of a manual nature. While there were too few cases within this analysis to make generalisations, the requirement for further understanding around GWG according to ethnicity among women with a high BMI has been demonstrated. Furthermore, the study has highlighted the need to specifically focus on the effectiveness of any interventions developed among nulliparous women and those from more deprived backgrounds.
Authors’ contributions
FF and HS developed the protocol; FF assisted with data collection; FF analysed and interpreted the data; HS supervised analysis and interpretation of the data; FF wrote the manuscript; HS revised the manuscript; FF and HS agreed the final manuscript.
Supplemental Material
Download MS Word (36.2 KB)Acknowledgments
With thanks to the support and assistance of all those within Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust particularly; Alison Williams, Patricia Wilkinson, Alexandra Goss, Emma Adams. With thanks to Katie Marvin-Dowle for her role in supporting data management. We would also like to acknowledge Ellen Marshall for her statistical advice and support.
Data availability statement
The datasets used and/or analysed during the current study are not publicly available within a repository as they belong to the Hospital Trust, but the data is available from the corresponding author on reasonable request.
Additional information
Funding
References
- Byrd, A.S., Toth, A.T. and Stanford, F.C., 2018. Racial disparities in obesity treatment. Current Obesity Reports, 7 (2), 130–138.
- Cheney, K., et al., 2017. Prevalence and predictors of early gestational weight gain associated with obesity risk in a diverse Australian antenatal population: a cross-sectional study. BMC Pregnancy and Childbirth, 17 (1), 296.
- Cheng, T.S., et al., 2021. Sociodemographic determinants of prepregnancy body mass index and gestational weight gain: The Mutaba’ah study. Obesity Science & Practice, 8 (3), 308–319.
- D’Souza, R., et al., 2019. Maternal body mass index and pregnancy outcomes: a systematic review and metaanalysis. American Journal of Obstetrics & Gynecology Mfm, 1 (4), 100041.
- Deputy, N.P., et al., 2015. Prevalence and characteristics associated with gestational weight gain adequacy. Obstetrics and Gynecology, 125 (4), 773–781.
- Devlieger, R., et al., 2016. Maternal obesity in Europe: where do we stand and how to move forward? A scientific paper commissioned by the European Board and College of Obstetrics and Gynaecology (EBCOG). European Journal of Obstetrics, Gynecology, and Reproductive Biology, 201, 203–208.
- Emery, R.L., et al., 2021. Factors associated with early gestational weight gain among women with pre-pregnancy overweight or obesity. Journal of Obstetrics and Gynaecology: The Journal of the Institute of Obstetrics and Gynaecology, 41 (6), 864–869.
- Fair, F.J. and Soltani, H., 2023. A retrospective comparative study of antenatal healthy lifestyle service interventions for women with a raised body mass index. Women and Birth: journal of the Australian College of Midwives. https://doi.org/10.1016/j.wombi.2023.08.010.
- Fair, F.J., et al., 2022. Everything is revolved around me being heavy … it’s always, always spoken about.” Qualitative experiences of weight management during pregnancy in women with a BMI of 40kg/m2 or above. PLoS One, 17 (6), e0270470.
- Garmendia, M.L., et al., 2017. Predictors of gestational weight gain among Chilean pregnant women: The Chilean Maternal and Infant Nutrition Cohort study. Health Care for Women International, 38 (8), 892–904.
- Goldstein, R.F., et al., 2017. Association of gestational weight gain with maternal and infant outcomes. A Systematic review and meta-analysis. JAMA, 317 (21), 2207–2225.
- Hasson, F., McKenna, H. and Keeney, S., 2015. Surveys. Ch 19. In: K. Gerrish and J. Lathlean, eds. The research process in nursing. 7th ed. Chichester: John Wiley and Sons.
- Heery, E., et al., 2015. Prediction of gestational weight gain – a biopsychosocial model. Public Health Nutrition, 18 (8), 1488–1498.
- Heslehurst, N., et al., 2010. A nationally representative study of maternal obesity in England, UK: trends in incidence and demographic inequalities in 619 323 births, 1989-2007. International Journal of Obesity (2005), 34 (3), 420–428.
- Hill, B., 2021. Expanding our understanding and use of the ecological systems theory model for the prevention of maternal obesity: A new socioecological framework. Obesity Reviews, 22 (3), e13147.
- Jardine, J., et al., 2021. Adverse pregnancy outcomes attributable to socioeconomic and ethnic inequalities in England: a national cohort study. Lancet (London, England), 398 (10314), 1905–1912.
- Kirchengast, S. and Hartmann, B., 2013. Determinants of gestational weight gain with special respect to maternal stature height and its consequences for newborn vital parameters. Anthropological Review, 76 (2), 151–162.
- Lee, B.Y., et al., 2017. A systems approach to obesity. Nutrition Reviews, 75 (suppl 1), 94–106.
- Lindberg, S., et al., 2016. Prevalence and predictors of unhealthy weight gain in pregnancy. WMJ, 115 (5), 233–237.
- Lutsiv, O., et al., 2015. The effects of morbid obesity on maternal and neonatal health outcomes: a systematic review and meta-analyses. Obesity Reviews, 16 (7), 531–546.
- National Health Service (NHS) Digital. 2019. NHS Maternity Statistics 2018-2019. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/nhs-maternity-statistics/2018-19 [Accessed 28 September 2023].
- Nunnery, D., Ammerman, A. and Dharod, J., 2018. Predictors and outcomes of excess gestational weight gain among low-income pregnant women. Health Care for Women International, 39 (1), 19–33.
- Office for National Statistics (ONS). 2010. The National Statistics Socio-economic Classification Coding Tool (SOC2010). Available from: https://onsdigital.github.io/dp-classification-tools/standard-occupational-classification/ONS_NSSEC_discovery_tool.html [Accessed 20 April 2023].
- Pawlak, M.T., et al., 2015. The effect of race/ethnicity on gestational weight gain. Journal of Immigrant and Minority Health, 17 (2), 325–332.
- Public Health England (PHE). 2019a. Health of women before and during pregnancy: health behaviours, risk factors and inequalities. An updated analysis of the maternity services dataset antenatal booking data. London: Public Health England.
- Public Health England (PHE). 2019b. Public health outcomes framework. Available from: https://fingertips.phe.org.uk/profile/public-health-outcomes-framework/data#page/1 [Accessed 20 April, 2023].
- Rasmussen, K.M., and Yaktin, A.L., 2009. Institute of medicine and national research council committee to reexamine IOM pregnancy weight guidelines. In Weight gain during pregnancy: Re-examining the Guidelines. Washington DC: The National Academies Press.
- Raymond, J.E., Foureur, M.J. and Davis, D.L., 2014. Gestational weight change in women attending a group antenatal program aimed at addressing obesity in pregnancy in New South Wales, Australia. Journal of Midwifery & Women’s Health, 59 (4), 398–404.
- Rogozińska, E., et al., 2017. Effects of antenatal diet and physical activity on maternal and fetal outcomes: individual patient data meta-analysis and health economic evaluation. Health Technology Assessment (Winchester, England), 21 (41), 1–158.
- Samura, T., et al., 2016. Factors associated with excessive gestational weight gain: Review of current literature. Global Advances in Health and Medicine, 5 (1), 87–93.
- Santos, S., et al., 2019. Impact of maternal body mass index and gestational weight gain on pregnancy complications: an individual participant data meta-analysis of European, North American and Australian cohorts. BJOG: An International Journal of Obstetrics & Gynaecology, 126 (8), 984–995.
- Siega-Riz, A.M., et al., 2020. The current understanding of gestational weight gain among women with obesity and the need for future research. National Academy of Medicine Perspectives, Discussion Paper, National Academy of Medicine, Washington DC.
- Smith, T., et al., 2015. The English indices of deprivation 2015. Technical report. Department for Communities and Local Government, London.
- Voerman, E., et al., 2019. Maternal body mass index, gestational weight gain, and the risk of overweight and obesity across childhood: An individual participant data meta-analysis. PLoS Medicine, 16 (2), e1002744.
- West, C., 2010. Developing a support service for overweight women. Pract Midwife, 13 (10), 19–21.
- Williamson, K., Nimegeer, A. and Lean, M., 2020. Rising prevalence of BMI ≥40kg/m2: A high-demand epidemic needing better documentation. Obes Rev, 21 (4), e12986.
- Xu, H., et al., 2021. Gestational weight gain and delivery outcomes: A population-based cohort study. Paediatric and Perinatal Epidemiology, 35 (1), 47–56.