

Introduction
Pyoderma gangrenosum (PG) is a rare non-infectious skin disease of undetermined origin which characterised by destructive and necrotising skin ulcer (George et al. Citation2019). Its histopathological feature is dense neutrophil infiltration in the affected tissue, which is not caused by bacterial, viral, or other microbial infection (Alavi et al. Citation2017). Currently, there is a lack of established diagnostic criteria and management for PG. Therefore, in order to enhance patient outcomes, it is imperative to promptly diagnose the condition and implement a comprehensive therapeutic approach.
Case presentation
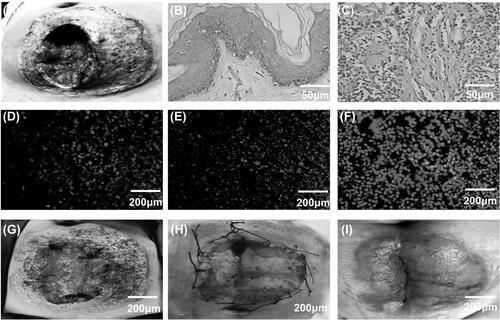
This study presented the case of a 34-year-old female patient who underwent a caesarean section due to preterm premature rupture of membranes and acute chorionic amniotic membrane inflammation. On the first day after the surgery, the patient experienced a fever reaching 40 degrees Celsius. Given the likelihood of infection, a treatment regimen consisting of piperacillin, sulbactam, cefoperazone, doxycycline, and meropenem was administered. However, the management of body temperature and wound ulceration remained uncontrolled. The incision site exhibited pronounced swelling and redness, resulting in the formation of an ulcerated surface characterised by irregular edges and severe localised pain. As a consequence of persistent hyperpyrexia and deteriorating health, the patient was transferred to our hospital on the eighth day post-surgery. Because of high fever and severe wound ulceration, blood tests including c-reactive protein and calcitonin original were conducted. The results were reported as follows, leukocyte 34.97 × 109/L (3.5–9.9 × 109/L), neutrophil percentage 95% (40–75%), neutrophil value 31.74 × 109/L (1.8–6.3 × 109/L), calcitonin original 2.92 ng/ml (0–0.05 ng/ml), c-reactive protein 268 mg/L (0–6 mg/L). showed the wound at 8th day after caesarean section. A longitudinal wound measuring approximately 12 × 14 × 4 cm3 was observed in the abdominal region, with complete dehiscence of the wound extending to the depth of the anterior sheath of the rectus abdominis. Small blisters, redness, and skin ulceration was observed around the wound. On the surface, there was extensive yellow-white necrotic tissue and liquefied adipose tissue. The test of wound skin tissue shown that bacterial, fungal cultures and the syphilis serum reaction was negative, the antibiotics were discontinued at once when the results came back. Haematoxylin and eosin staining showed the skin tissue from patient had many neutrophils cells infiltration compared with normal skin tissue (). Using the triple immunofluorescence test of Histone 2B antibody (green), Myeloperoxidase antibody (red) and DAPI (4′,6-diamidino-2-phenylindole, purple), we found skin tissue biopsies from patient showed signs of collocation of green and red fluorescence which suggested neutrophil extracellular traps (NETs) ().
Figure 1. (A) Image of abdominal wound on day 8 after caesarean section. (B,C) Haematoxylin and eosin staining of skin tissue from normal pregnant woman and PG patients. (D–F) Triple immunofluorescence detection for NETs formation using histone 2B antibody, Myeloperoxidase antibody and DAPI in skin tissue samples of PG patients. (G) Image of abdominal wound on the seventh day following treatment. (H) Image of abdominal wound after skin grafting. (I) Image of abdominal wound after 15 months.
Although many diagnostic criteria had been proposed for PG, there are no standardised criteria for the diagnosis (Yamamoto et al. Citation2023). The Paracelsus score identified the highest proportion of patients in the PG cohort (Carter et al. Citation2021). According to the Paracelsus score, this particular patient exhibited three major criteria: progressive disease course, absence of relevant differential diagnoses, and a reddish-violaceous wound border. Additionally, the study observed the fulfilment of two minor criteria and two additional criteria, namely the presence of a distinctively peculiar ulcer shape, intense pain exceeding a score of 4 on the Visual Analog Scale (VAS), histopathological evidence of supportive inflammation, and an undermined wound margin. A diagnosis of highly likely PG necessitates a score exceeding 10 points, and this patient’s score amounted to 15 points. The combination of positive findings regarding neutrophil cell infiltration and NETs formation in skin tissues strongly supported the likelihood of PG.
The patient was treated with methylprednisolone (80 mg/day iv), and human immunoglobulin (200 mg/kg/day iv for 5 days, total dosage were 60 g). The wound was treated with silver ion antibacterial gel and epidermal growth factor for external application. On the second day after therapy, the body temperature returned to normal and the wound range did not expand further. The inflammation and swelling surrounding the ulcer gradually subsided over a period of time. After 5 days of treatment, the methylprednisolone was changed to prednisone (40 mg/day po) and other therapies was stopped. On the seventh day following treatment, a wound debridement procedure was conducted to eliminate necrotic tissue (see . Subsequently, after 15 days of treatment, the patient underwent skin grafting at a general hospital, resulting in complete wound healing after a duration of 15 months ().
Discussion
Pyoderma gangrenosum may manifest initially as papules, pustules, or nodules, exhibiting characteristic traits of sudden onset and rapid dissemination (Simman et al. Citation2021). Sasor et al. conducted a retrospective analysis of 2,273 PG patients in the United States from 2008 to 2010, and the results revealed that only 22.6% of PG patients were diagnosed for the first time (Sasor et al. Citation2018). Some patients had symptoms such as fever, muscle pain, and joint pain (DeFilippis et al. Citation2015). In a comprehensive analysis of PG occurring after breast surgery, leukocytosis was observed in 21 out of 37 cases and fever in 27 cases (Tuffaha et al. Citation2016). In this case, the patient presented with acute onset, high fever, uncontrolled wound ulceration, and concurrent leukocytosis. The aetiology of PG may be idiopathic, and it is frequently comorbid with hematological malignancies, arthritis, or autoimmune diseases. Pregnancy was known to induce changes in immune responses that facilitate foetal tolerance (Stuebe et al. Citation2012; Ramos et al. Citation2015; Inversetti et al. Citation2023). In cases where there is skin invasive manipulation and immune disorders during pregnancy, PG may develop following caesarean section.
PG is characterised by a dense neutrophilic infiltrate in the affected tissue (Wollina and Haroske Citation2011). Recently studies have shown that neutrophils could form a net structure consisting of nucleic acid substances and granular proteins outside the cell, known as Neutrophil extracellular traps(NETs). NETs possess pathogen-hunting capabilities, also have the potential to cause harm to surrounding cells and tissues (Papayannopoulos and Zychlinsky, Citation2009; Manda-Handzlik et al. Citation2020). Croia et al. found the NETs were highly expressed in the skin tissue of the PG patient compared to normal parturient women (Croia et al. Citation2021, Ogawa et al. Citation2021). Immunofluorescent images indicated that the histopathologic location and depth of NETs formation in PG varied by the clinical subtypes (Ishikawa and Yamamoto Citation2023). In this case, immunofluorescence test showed Histone 2B and Myeloperoxidase increased outside cells, which suggested that NETs formation. The presence of neutrophil infiltrates and formation of NETs in skin tissues, along with a high Paracelsus score in patients, help us to diagnose PG.
Currently there are formal guidelines to treat PG in Japan (Yamamoto et al.Citation2023). In this guideline, systemic administration of corticosteroids, immunosuppressant, or colchicine is believed to be effective (Recommendation grade: A). In additional studies, systemic corticosteroids and cyclosporine are recommended as the first-line treatment for PG (Maronese et al. Citation2022). Intravenous immunoglobulin (IVIG) has been used as an adjunct therapy to corticosteroids, effectively reducing the need for high steroid doses in refractory cases of PG. In this particular case, cyclosporine was not utilised due to the patient’s need for lactation. The patient received systemic corticosteroid and IVIG treatment and obtained good efficacy, which supported the importance of combination treatment for PG patients.
This case demonstrated the important of combination therapy regimens for the PG patients, and NETs formation provided relatively reliable predictor for PG early diagnosis. Of course, further studies are necessary on the relationship between NETs and PG.
Ethical approval
The patient signed an informed consent statement. This study was approved by the ethics committee of Hunan Provincial Maternal and Child Health Hospital (2021-S084).
Acknowledgments
We would like to thank Dr. Hui Tian for the English language review.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Additional information
Funding
References
- Alavi, A., et al., 2017. Pyoderma gangrenosum: an update on pathophysiology, diagnosis and treatment. American Journal of Clinical Dermatology, 18 (3), 355–372.
- Carter, H., et al., 2021. Comparison of three diagnostic frameworks for pyoderma gangrenosum. Journal of Investigative Dermatology, 141, 59–63.
- Croia, C., et al., 2021. Evaluation of neutrophil extracellular trap deregulated formation in pyoderma gangrenosum. Experimental Dermatology, 30 (9), 1340–1344.
- Defilippis, E.M., Feldman, S.R. and Huang, W.W., 2015. The genetics of pyoderma gangrenosum and implications for treatment: a systematic review. The British Journal of Dermatology, 172 (6), 1487–1497.
- George, C., Deroide, F. and Rustin, M., 2019. Pyoderma gangrenosum – a guide to diagnosis and management. Clinical Medicine, 19 (3), 224–228.
- Inversetti, A., et al., 2023. Endometrial microbiota and immune tolerance in pregnancy. International Journal of Molecular Sciences, 24 (3), 2995.
- Ishikawa, M. and Yamamoto, T., 2023. Neutrophil extracellular traps formation in the lesional skin of various types of pyoderma gangrenosum. Experimental Dermatology, 32 (11), 2029–2033.
- Manda-Handzlik, A., et al., 2020. Nitric oxide and peroxynitrite trigger and enhance release of neutrophil extracellular traps. Cellular and Molecular Life Sciences, 77 (15), 3059–3075.
- Maronese, C.A., et al., 2022. Pyoderma gangrenosum: an updated literature review on established and emerging pharmacological treatments. American Journal of Clinical Dermatology, 23 (5), 615–634.
- Ogawa, Y., et al., 2021. Neutrophil extracellular traps in skin diseases. Biomedicines, 9 (12), 1888.
- Papayannopoulos, V. and Zychlinsky, A., 2009. NETs: a new strategy for using old weapons. Trends in Immunology, 30 (11), 513–521.
- Ramos, B.D.A., et al., 2015. Microorganisms in the female genital tract during pregnancy: tolerance versus pathogenesis. American Journal of Reproductive Immunology, 73 (5), 383–389.
- Sasor, S.E., et al., 2018. Pyoderma gangrenosum demographics, treatments, and outcomes: an analysis of 2,273 cases. Journal of Wound Care, 27 (Sup1), S4–S8.
- Simman, R., et al., 2021. An unusual presentation of blastomycosis-like pyoderma gangrenosum. Wounds, 33 (8), 203–206.
- Stuebe, A.M., et al., 2012. Maternal BMI, glucose tolerance, and adverse pregnancy outcomes. American Journal of Obstetrics and Gynecology, 207 (1), 62.e1–62.e7.
- Tuffaha, S.H., et al., 2016. Pyoderma gangrenosum after breast surgery: diagnostic pearls and treatment recommendations based on a systematic literature review. Annals of Plastic Surgery, 77 (2), e39–e44.
- Wollina, U. and Haroske, G., 2011. Pyoderma gangraenosum. Current Opinion in Rheumatology, 23 (1), 50–56.
- Yamamoto, T., et al., 2023. Clinical guidance of pyoderma gangrenosum. The Journal of Dermatology, 50 (9), e253–e275.