

 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
A well-known complication of laparoscopic management of gynaecologic masses and cancers is the need to perform an intraoperative conversion to laparotomy. The purpose of this study was to identify novel patient risk factors for conversion from minimally invasive to open surgeries for gynaecologic oncology operations.
Methods
This was a retrospective cohort study of 1356 patients ≥18 years of age who underwent surgeries for gynaecologic masses or malignancies between February 2015 and May 2020 at a single academic medical centre. Multivariable logistic regression was used to study the effects of older age, higher body mass index (BMI), higher American Society of Anaesthesiologist (ASA) physical status, and lower preoperative haemoglobin (Hb) on odds of converting from minimally invasive to open surgery. Receiver operating characteristic (ROC) curve analysis assessed the discriminatory ability of a risk prediction model for conversion.
Results
A total of 704 planned minimally invasive surgeries were included with an overall conversion rate of 6.1% (43/704). Preoperative Hb was lowest for conversion cases, compared to minimally invasive and open cases (11.6 ± 1.9 vs 12.8 ± 1.5 vs 11.8 ± 1.9 g/dL, p<.001). Patients with preoperative Hb <10 g/dL had an adjusted odds ratio (OR) of 3.94 (CI: 1.65–9.41, p=.002) for conversion while patients with BMI ≥30 kg/m2 had an adjusted OR of 2.86 (CI: 1.50–5.46, p=.001) for conversion. ROC curve analysis using predictive variables of age >50 years, BMI ≥30 kg/m2, ASA physical status >2, and preoperative haemoglobin <10 g/dL resulted in an area under the ROC curve of 0.71. Patients with 2 or more risk factors were at highest risk of requiring an intraoperative conversion (12.0%).
Conclusions
Lower preoperative haemoglobin is a novel risk factor for conversion from minimally invasive to open gynaecologic oncology surgeries and stratifying patients based on conversion risk may be helpful for preoperative planning.
PLAIN LANGUAGE SUMMARY
Minimally invasive surgery for management of gynaecologic masses (masses that affect the female reproductive organs) is often preferred over more invasive surgery, because it involves smaller surgical incisions and can have overall better recovery time. However, one unwanted complication of minimally invasive surgery is the need to unexpectedly convert the surgery to an open surgery, which entails a larger incision and is a higher risk procedure. In our study, we aimed to find patient characteristics that are associated with higher risk of converting a minimally invasive surgery to an open surgery. Our study identified that lower levels of preoperative haemoglobin, the protein that carries oxygen within red blood cells, is correlated with higher risk for conversion. This new risk factor was used with other known risk factors, including having higher age, higher body mass index, and higher baseline medical complexity to create a model to help surgical teams identify high risk patients for conversion. This model may be useful for surgical planning before and during the operation to improve patient outcomes.
Introduction
Gynaecologic malignancies are a major cause of morbidity and mortality with an annual national economic burden of $3.8 billion, over half of which can be attributed to hospital stays for workup and eventual management (Yue et al. Citation2020). These cancers are often managed surgically, either through laparotomy or minimally invasive approaches including traditional laparoscopy and robotic-assisted laparoscopy (Morice et al. Citation2016, Chandra et al. Citation2019). With the proper patient indications and clinical context, minimally invasive techniques have been shown to improve certain patient outcomes, including decreased intraoperative blood loss and shorter lengths of hospitalisation compared to open laparotomy, which has led to an increasing interest in expanding the role of robotic-assisted management of gynaecologic cancers (Lindfors et al. Citation2018, Uccella et al. Citation2018). However, a well-known risk of minimally invasive surgery is the need to intraoperatively convert the surgery to an open case, which has been shown to have worse patient outcomes, including higher postoperative complication and morbidity rates (Eltabbakh et al. Citation1999, Sokol et al. Citation2003, Lim et al. Citation2016). The risk of conversion is significant, as some studies have reported conversion rates between 6–17% for gynaecologic oncology surgeries (Cunningham et al. Citation2015, Brown et al. Citation2019). Therefore, due to the high incidence and poor clinical outcomes of converted surgeries, there has been increasing interest in identifying patient risk factors for conversion. Within the field of gynaecologic oncology, prior studies have identified several factors correlated with increased conversion risk, including higher age, lower hospital/surgeon case volume, higher body mass index (BMI) and prior abdominopelvic surgeries (Scribner et al. Citation2001, Sokol et al. Citation2003, Chi et al. Citation2004, Leonard et al. Citation2005, Fanning and Hossler Citation2010, Twijnstra et al. Citation2013, Keurentjes et al. Citation2018).
However, identifying additional risk factors for needing an intraoperative conversion may provide opportunities for improved preoperative counselling and perioperative planning. This study aims to identify novel patient risk factors for conversion from minimally invasive to open surgeries for gynaecologic oncology operations. Novel and known patient risk factors for conversion will be used in conjunction to create a risk prediction model.
Materials and methods
This was a retrospective cohort study analysing electronic health records (EHR) of all patients 18 years of age who underwent lower abdominal surgeries for management of gynaecologic masses or malignancies. Institutional review board approval was granted by the University of California, San Francisco (IRB #20-30743). All surgeries were performed by one of eight high-volume surgeons with similar practise patterns from the gynaecologic oncology service at a single academic medical centre between February 2015 to May 2020 (Mowat et al. Citation2016). Exclusion criteria included patients who underwent non-gynaecologic surgeries and patients who had non-abdominal procedures such as vulvar surgery or gynaecologic exams under anaesthesia (). Perioperative care for all gynaecologic patients was according to our institutional implementation of the Enhanced Recovery After Surgery (ERAS) Society Gynaecologic/Oncology guidelines. A power analysis was performed to determine the required sample size to obtain an area under the receiver operating characteristic curve (AUROC) of 0.85 with the width of the 95% confidence interval being 0.15 in the prediction of conversion risk. Based on a prior study that reported a conversion risk of 7% for laparoscopic surgery on a gynaecologic oncology service, a total sample size of 585 patients was needed to adequately power this study (Hanley and McNeil Citation1982, Chi et al. Citation2004).
Figure 1. Patient selection flowchart.
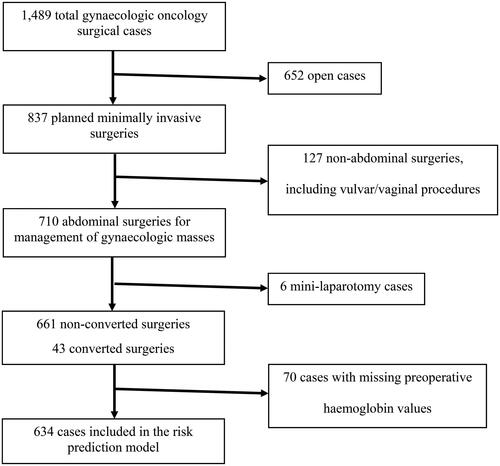
Demographic, perioperative, and postoperative variables were extracted from patients’ EHR. Missing data was addressed using available-case analysis. Surgeries were categorised as either open, minimally invasive, or minimally invasive-to-open conversion cases. Minimally invasive surgeries were performed either laparoscopically or robotic-assisted. Converted mini-laparotomy cases, defined as a less invasive laparotomy with a smaller incision for specimen extraction, were excluded from the statistical analysis. Demographic and perioperative measures were compared between the three surgical groups using ANOVA for normally distributed variables and Kruskal-Wallis test for non-parametric variables. Fisher’s exact test was used to compare categorical variables across groups.
The primary outcome variable was the risk of conversion from minimally invasive to laparotomy, which was defined as an open incision that was made to continue a planned surgery after starting through a minimally invasive approach. Predictor variables, chosen a priori based on prior literature for conversion risk factors as well as available variables of the database, included demographics and preoperative metrics including age, BMI, American Society of Anaesthesiologist (ASA) physical status, insurance type, primary mass location, and preoperative haemoglobin (Hb) (Sokol et al. Citation2003, Chi et al. Citation2004, Leonard et al. Citation2005, Fanning and Hossler Citation2010, Twijnstra et al. Citation2013). Primary mass location was categorised as either adnexal, uterine, vaginal/cervical, or other (which included unknown mass locations and gastrointestinal masses). Preoperative Hb was defined as the most recent Hb lab value within 30 days of the surgery date. Based on the predictor variables’ distributions, higher age had a cut-off of >50 years, high BMI had a cut-off of ≥30 kg/m2, high ASA physical status had a cut-off of >2, and low preoperative Hb had a cut-off of <10 g/dL. Simple and multiple logistic regression models were performed to examine the relationship between these variables and the risk of conversion.
The discriminatory ability of a risk prediction model for conversion was measured by the AUROC, using multivariable logistic regression with known and novel risk factors for conversion. This risk prediction model was validated and corrected for optimism using bootstrap sampling with a sample size of 600 and replicated 500 times. The c-statistic was calculated as a measure of the AUROC and represents the discriminatory value of the prediction model. The prediction model was also evaluated by calculating the risk and odds ratios for conversion within this patient cohort, based on the number of positive patient risk factors.
Statistical significance was set to be p<.05 and all statistical analyses were performed using Stata version 16.1 (StataCorp). The reporting of this study is concordant with the STROBE guidelines (Elm et al. Citation2007).
Results
There were a total of 1356 gynaecologic oncology surgeries performed between February 2015 and May 2020 included in the analysis. Out of 704 cases planned for a minimally invasive approach, 43 (6.1%) of these cases were converted to laparotomy. Minimally invasive, open, and conversion cases did not statistically differ in age or distance from residential zip code to the hospital. Conversion cases had highest BMI, lowest median income based on residential zip code, and highest rates of government-supported insurance coverage ().
Table 1. Patient demographics and characteristics.
The most common indication for conversion in our patient cohort was adhesions (33%), extensive tumour burden (21%) and poor visualisation (16%) (). Intraoperatively, conversion cases had the longest average duration of surgery and highest median volumes of crystalloid solutions, transfusion of packed red blood cells (RBCs) and estimated blood loss (EBL). Postoperatively, compared to open and minimally invasive cases, conversion cases were most likely to recover in an ICU (25.6% vs 12.9% vs 1.1%, p<.001), had the longest median total length of stay (5(4,12) vs 4(3,7) vs 1(0,1) days, p<.001), and were most likely to be discharged to a skilled nursing or rehabilitation facility (21.4% vs 7.4% vs 0.4%, p<.001). Overall, conversion cases had highest total cost of hospitalisation (median: $22,549 vs $17,943 vs $7,812, p<.001) ().
Figure 2. Indications for conversion surgery (N = 43).
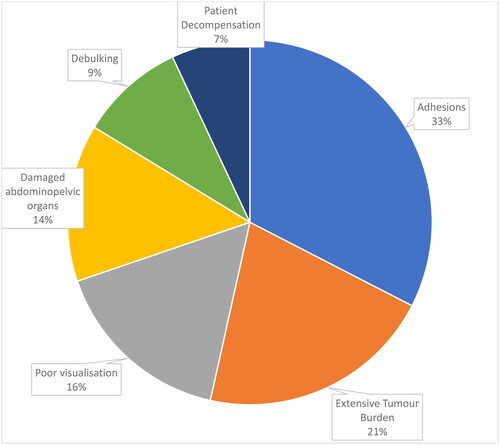
Table 2. Preoperative, intraoperative and postoperative outcomes by surgery type.
Preoperative Hb was documented for 1230 of 1356 total patients, including 634 of 704 planned minimally invasive cases and 596 of 652 open cases. Preoperative Hb levels were lowest for conversion cases, compared to minimally invasive and open cases (11.6 ± 1.9 vs 12.8 ± 1.5 vs 11.8 ± 1.9, p<.001) ().
Simple logistic regression showed that patients with preoperative Hb <10 g/dL had an odds ratio (OR) of 4.09 (CI: 1.76–9.47, p=.001) for conversion and patients with BMI ≥30 kg/m2 had an OR of 3.01 (CI:1.62–5.62, p=.001) for conversion. Having ASA physical status >2 (OR:2.01, p=.04) and having Medicare insurance (OR:2.48, p=.01) were also associated with increased odds of conversion. In multiple logistic regression models, preoperative Hb <10 g/dL (adjusted OR:3.94, p=.002) and BMI ≥30 kg/m2 (adjusted OR:2.86, p=.001) continued to be correlated with higher odds of conversion ().
Table 3. Simple and multiple logistic regressions models for odds of conversion (N = 704).
Using a multivariable logistic regression, the predictive variables for conversion that were included in the prediction model were age >50 years, BMI ≥30 kg/m2, ASA physical status >2, and preoperative haemoglobin <10 g/dL. Only patients who were planned for minimally invasive surgery and had non-missing values of demographic information and preoperative measurements (N = 634) were included in the final analytic sample for the prediction model. The AUROC for this prediction model was 0.71 (). When corrected for optimism using bootstrap sampling, the c-statistic was 0.68. Based on these four risk factors, this patient cohort had an associated conversion risk of 1.6% for patients with 0 risk factors, 4.7% with 1 risk factor, and 12.0% with 2 or more risk factors. Compared to patients with no risk factors, patients with 1 risk factor had an OR of 3.1 (CI:0.85–17.0, p=.06) for conversion and patients with 2 or more risk factors had an OR of 8.5 (CI:2.5–44.6, p<.001) for conversion. Further stratification was not performed for patients with 2+ risk factors because few patients had 3 or 4 risk factors ().
Figure 3. Receiver operating characteristic (ROC) curve for the conversion risk predictor model. Predictive variables included age >50 years, body mass index (BMI) ≥30 kg/m2, American Society of Anaesthesiologists (ASA) physical status >2, and preoperative haemoglobin <10 g/dL. (N = 634).
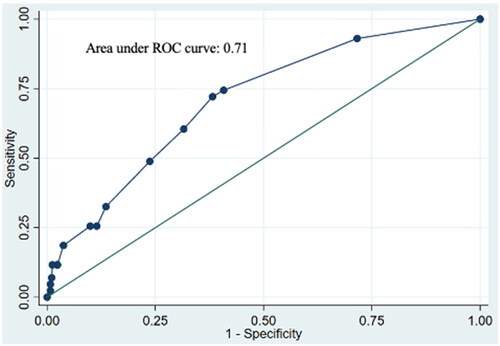
Table 4. Risk of conversion stratified by number of patient risk factors.
Discussion
The purpose of this study was to identify risk factors for conversion from minimally invasive procedures to open laparotomy surgery for gynaecologic oncology patients. In our analysis, lower preoperative haemoglobin was correlated with increased odds of conversion. To our knowledge, this is a novel relationship that adds to our understanding of how we can identify patients at higher risk for conversion in gynaecologic oncology. We also found that higher BMI is a risk factor for conversion, which is in accordance with prior studies (Fanning and Hossler Citation2010, Twijnstra et al. Citation2013, Matsuo et al. Citation2016).
Our overall conversion rate of 6.1% is consistent with prior gynaecologic oncology literature (Chi et al. Citation2004, Brown et al. Citation2019). Compared to open and minimally invasive cases, conversion surgeries have the highest intraoperative blood loss, highest rates of postoperative recovery in an ICU, highest overall length of stay, highest total hospitalisation cost, and were least likely to be discharged directly home. These findings are consistent with studies that have identified worse patient outcomes for converted gynaecologic surgery (Eltabbakh et al. Citation1999, Scribner et al. Citation2001, Sokol et al. Citation2003). Therefore, there is a great incentive to better anticipate conversion cases to optimise patient outcomes through improved perioperative planning.
The relationship between low preoperative haemoglobin and poorer cancer outcomes has been previously studied. Baseline anaemia has been shown to be highly prevalent in cancer patients; the pathophysiology of which has been linked to overactivity of inflammatory cytokines leading to poor erythropoiesis (Birgegård et al. Citation2005). Within our study cohort and in prior studies, the most common reasons for conversions include greater extent of disease, the presence of metastases requiring debulking, and high burden of adhesions most likely due to prior abdominopelvic surgeries (Sokol et al. Citation2003, Leonard et al. Citation2005, Lim et al. Citation2016). In our study, the above factors cumulatively accounted for over 60% of the converted cases. Greater disease burden, presence of metastases requiring debulking, and more pathologic adhesions all lead to elevated inflammatory cytokines, which is then reflected in a lower preoperative haemoglobin. This may explain the pathophysiologic relationship between lower preoperative haemoglobin and higher risk for conversion.
It is unclear whether surgical patients benefit from treatment of low preoperative haemoglobin. One study showed that intravenous iron treatment did not decrease the risk of mortality, length of hospitalisation, or complication rates (Richards et al. Citation2020) while another study found that perioperative blood transfusions did not decrease the risk of postoperative mortality or morbidity (Richards et al. Citation2015). These findings suggest that low preoperative haemoglobin values may have clinical utility more as a herald of disease extent rather than through the direct effect of having low haemoglobin.
A risk prediction model for conversion was made through logistic regression modelling, using known patient risk factors for conversion as well as the novel risk factor of low preoperative haemoglobin. The dichotomised risk factors in our model included age >50 years, BMI ≥30 kg/m2, ASA physical status >2, and preoperative haemoglobin <10 g/dL. This prediction model showed an acceptable discriminatory ability with an AUROC of 0.71. Even when corrected for optimism, the c-statistic was 0.68, indicating a reasonable model. Within our cohort, these risk factors seem to have synergistic effects and patients with multiple risk factors had higher risk of conversion. Patients with two or more risk factors had highest risk, with 12% of patients needing a conversion.
Therefore, we propose that low preoperative haemoglobin values can be used in conjunction with other risk factors for intraoperative conversion to better inform preoperative planning and counselling. Surgical teams may better anticipate higher probability of an intraoperative conversion and as a result, surgical planning and resource allocation can be tailored for these patients to improve surgical outcomes, ensure patient safety, and optimise postoperative management. In our study, converted cases had worse outcomes than open cases, including higher transfusion requirements, more postoperative ICU stays, and higher likelihood of discharging to a facility. Therefore, a prediction tool may also be beneficial for improved patient selection, allowing surgical teams to hold discussions with high-risk patients to consider the option of performing an open case instead of attempting a high-risk minimally invasive surgery. From the patients’ perspective, they will be better informed of the risk for a more invasive procedure that would require a longer hospitalisation and more extensive recovery process.
Several limitations exist for this study. First, our database did not contain information on other known risk factors for conversion, including history of prior abdominopelvic surgeries and mass size. Our study also lacked information on other possible risk and preventative factors such as cancer-related serologic markers and history of neoadjuvant chemotherapy, which may also affect risk for conversion. Broadening our database would likely further strengthen the discriminatory ability of the risk prediction model proposed in this study. We also acknowledge that a possible confounder variable that was not included in our study is whether patients received preoperative transfusions; although one study found that perioperative transfusions prior to gynaecologic surgery did not affect postoperative outcomes (Richards et al. Citation2015). Another limitation was that it was not possible to stratify conversion cases by how well the surgeon was able to anticipate an intraoperative conversion. There were likely some conversion cases for which perioperative planning were already in place to manage the patient more like a laparotomy case than as a minimally invasive case, thereby improving their postoperative outcomes. Identifying and reclassifying these cases would further strengthen the differences in postoperative outcomes between converted and non-converted cases. Lastly, our study cohort did not have enough patients to further stratify patients with 2 or more risk factors. We would expect that patients with more risk factors would have higher conversion rates. Future studies will aim to validate our risk prediction model in another patient cohort.
Conclusions
While minimally invasive gynaecologic oncology surgeries are becoming increasingly utilised, intraoperative conversion to open surgery is a well-described complication. However, not much is known about patient risk factors for conversion. This retrospective cohort study identified that lower preoperative haemoglobin is associated with higher rates of conversion. A novel risk prediction model incorporating lower preoperative haemoglobin, higher BMI, higher age, and higher ASA class displayed acceptable discriminatory ability in predicting conversion risk for gynaecologic oncology surgeries. Further studies are needed to validate this model in larger patient populations.
Authors’ contributions
KHN contributed to the conception and methodology, data acquisition, analysis, writing-original draft. HJ contributed to the methodology, data acquisition, analysis, validation, writing-review & editing. SM contributed to the analysis, validation, writing-review & editing. LMC contributed to the conception and methodology, data acquisition, validation, writing-review & editing, supervision. LLC contributed to the conception and methodology, data acquisition, validation, writing-review & editing, supervision. All authors reviewed the results and approved the final version of the manuscript.
Data availability statement
The data described in this study was not made openly available due to patient identifying information. It can be made available upon reasonable request from the corresponding author.
Additional information
Funding
References
- Birgegård, G., et al., 2005. Cancer-related anemia: pathogenesis, prevalence and treatment. Oncology, 68 (Suppl 1), 3–11.
- Brown, J., et al., 2019. When less is more: minimally invasive surgery compared with laparotomy for interval debulking after neoadjuvant chemotherapy in women with advanced ovarian cancer. Journal of Minimally Invasive Gynecology, 26 (5), 902–909.
- Chandra, A., et al., 2019. Ovarian cancer: current status and strategies for improving therapeutic outcomes. Cancer Medicine, 8 (16), 7018–7031.
- Chi, D.S., et al., 2004. Ten-year experience with laparoscopy on a gynecologic oncology service: analysis of risk factors for complications and conversion to laparotomy. American Journal of Obstetrics and Gynecology, 191 (4), 1138–1145.
- Cunningham, M.J., et al., 2015. Body mass index, conversion rate and complications among patients undergoing robotic surgery for endometrial carcinoma. Journal of Robotic Surgery, 9 (4), 339–345.
- Elm, E.V., et al., 2007. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet (London, England), 370 (9596), 1453–1457.
- Eltabbakh, G.H., et al., 1999. Analysis of failed and complicated laparoscopy on a gynecologic oncology service. Gynecologic Oncology, 74 (3), 477–482.
- Fanning, J. and Hossler, C., 2010. Laparoscopic conversion rate for uterine cancer surgical staging. Obstetrics and Gynecology, 116 (6), 1354–1357.
- Hanley, J.A. and McNeil, B.J., 1982. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology, 143 (1), 29–36.
- Keurentjes, J.H.M., et al., 2018. Surgical volume and conversion rate in laparoscopic hysterectomy: does volume matter? A multicenter retrospective cohort study. Surgical Endoscopy, 32 (2), 1021–1026.
- Leonard, F., et al., 2005. Total laparoscopic hysterectomy: preoperative risk factors for conversion to laparotomy. Journal of Minimally Invasive Gynecology, 12 (4), 312–317.
- Lim, C.S., et al., 2016. Risk factors and outcomes for conversion to laparotomy of laparoscopic hysterectomy in benign gynecology. Obstetrics and Gynecology, 128 (6), 1295–1305.
- Lindfors, A., et al., 2018. Robotic vs open surgery for endometrial cancer in elderly patients: surgical outcome, survival, and cost analysis. International Journal of Gynecological Cancer: Official Journal of the International Gynecological Cancer Society, 28 (4), 692–699.
- Matsuo, K., et al., 2016. Predictive factor of conversion to laparotomy in minimally invasive surgical staging for endometrial cancer. International Journal of Gynecological Cancer: Official Journal of the International Gynecological Cancer Society, 26 (2), 290–300.
- Morice, P., et al., 2016. Endometrial cancer. The Lancet, 387 (10023), 1094–1108.
- Mowat, A., Maher, C. and Ballard, E., 2016. Surgical outcomes for low-volume vs high-volume surgeons in gynecology surgery: a systematic review and meta-analysis. American Journal of Obstetrics and Gynecology, 215 (1), 21–33.
- Richards, T., et al., 2020. Preoperative intravenous iron to treat anaemia before major abdominal surgery (PREVENTT): a randomised, double-blind, controlled trial. Lancet (London, England), 396 (10259), 1353–1361.
- Richards, T., et al., 2015. Impact of preoperative anaemia and blood transfusion on postoperative outcomes in gynaecological surgery. PLoS One, 10 (7), e0130861.
- Scribner, D.R., et al., 2001. Laparoscopic pelvic and paraaortic lymph node dissection: analysis of the first 100 cases. Gynecologic Oncology, 82 (3), 498–503.
- Sokol, A.I., Chuang, K. and Milad, M.P., 2003. Risk factors for conversion to laparotomy during gynecologic laparoscopy. Journal of the American Association of Gynecologic Laparoscopists, 10 (4), 469–473.
- Twijnstra, A.R.H., et al., 2013. Clinical relevance of conversion rate and its evaluation in laparoscopic hysterectomy. Journal of Minimally Invasive Gynecology, 20 (1), 64–72.
- Uccella, S., et al., 2018. Laparoscopic Versus open hysterectomy for benign disease in uteri weighing >1 kg: a retrospective analysis on 258 patients. Journal of Minimally Invasive Gynecology, 25 (1), 62–69.
- Yue, X., et al., 2020. Economic burden and treatment patterns of gynecologic cancers in the United States: evidence from the Medical Expenditure Panel Survey 2007–2014. Journal of Gynecologic Oncology, 31 (4), e52.