

Abstract
Background
Lichen sclerosus (LS) is a chronic, inflammatory disease of the genital and extra genital skin, causing pruritus, soreness, pain and dyspareunia. The aim of this study was to investigate whether Low Level Laser Therapy (LLLT) can improve the quality of life in women with Lichen sclerosus (LS) and insufficient topical treatment.
Methods
In a descriptive prospective observational study conducted between 02.01.2016 and 08.01.2018, we included 100 women with LS with insufficient topical treatment because of poor response of symptoms. All participants received ten LLLT treatments (808 nm and 500 mW) over a period of 8 weeks. The first four treatments were planned as two treatments per week. The remaining six treatments were planned as once a week. A Danish health-related quality of life tool (HRQoL test) monitored the effect.
Results
A total of 94 patients completed the study, median age of 62 [InterQuartile Range 53–69]. There was a statistically significant improvement in seven of the eight domains of the HRQoL test after ten LLLT. We found the results of DoloTest to be statistically significant in all of the groups except for smoking (p < 0.094).
Conclusions
LLLT treatment can improve the quality of life in women with LS.
PLAIN LANGUAGE SUMMARY
Lichen sclerosus is a chronic, inflammatory disease of the genital and extra genital skin, causing pruritus, soreness, pain and dyspareunia. This study aimed to investigate whether Low Level Laser Therapy can improve the quality of life in women with Lichen sclerosus and insufficient topical treatment. The study proposed a supplemental therapy to insufficient topical treatment in patients with Lichen sclerosus. This study indicated that Low Level Laser Therapy treatment can improve the quality of life in women with Lichen sclerosus.
Introduction
Lichen sclerosus (LS) is a chronic, inflammatory disease of the genital and extra genital skin. The overall prevalence of LS is unknown because of asymptomatic cases (Kirtsig & Sclerosus Citation2016). Among patients in a gynaecologic clinic the prevalence is approximately 1.7% (Lee & Fischer Citation2018). LS can appear in any age even childhood; however, it is often diagnosed in peri- or postmenopausal women. Many women with LS describe a lower quality of life compared to women without LS (Pérez-López & Vieira-Baptista Citation2017). Also LS is frequently associated with sexual dysfunction and anxiety (Yıldız et al. Citation2022). The aetiology is still not well documented though autoimmune diseases among women with LS or first-degree relatives are common (Fistarol & Itin Citation2013). LS usually affects the anogenital area causing pruritus, soreness, pain and dyspareunia. It can cause fusion and resorption of labia minora, phimosis of the clitoral hood and stenosis of the introitus. The disease is associated with an increased risk of squamous cell carcinoma in approximately 2.2% of the cases (Vieira-Baptisa et al. Citation2022).
First-line treatment is ultra-potent topical steroids such as clobetasol propionate, which often leads to symptomatic relief (Lee & Fischer Citation2018). In some cases, further treatment is needed due either to reduced effect of the treatment or it is requested by the patient because of fear of the long-term consequences by using topical steroids. However, the use of topical steroids is safe if appropriately done, and the risk of cancer is reduced with use of ultrapotent topical steroids. Topical calcineurin inhibitors are also useful due to their significant anti-inflammatory activity; however, it is often poorly tolerated, and malignant transformation has been described during treatment (Fistarol & Itin Citation2013). Despite adequate use of topical steroids or calcineurin inhibitors, some patients still experience symptoms creating a need for additional therapy.
Low Level Laser Therapy (LLLT) referred to also as photobiomodulation has throughout the literature only been described in one study as an alternative to the treatment of LS (Belotto et al. Citation2017). LLLT works by the principle of photons being absorbed by mitochondrial chromophores in the skin initiating diverse pathways leading stem cells to activate tissue repairing, regeneration and decreasing inflammation (Avci et al. Citation2013). The effect of LLLT is found to be promising in a variety of skin diseases including vitiligo an autoimmune skin disease and psoriasis a chronic inflammatory skin disease such as LS (Zhang & Wu Citation2018).
The aim of this study was to investigate whether LLLT improves the quality of life in women with LS experiencing insufficient effect of topical treatment because of poor response in symptoms.
Methods
Study subjects
One Hundred women with LS were included at Lillebaelt Hospital, Denmark in the period from 02.01.2016 to 08.01.2018. The patients were informed about the purpose of the research and the fact that LLLT was not standard-of-care treatment in our out-patient clinic. All patients who declined to take part in the study received standard-of-care treatment (topical steroid or topical calcineurin inhibitors) according to Danish national guidelines. During the study-period 118 patients were eligible to the study and 100 patients gave their consent to participate. 18 patients declined to participate because of the extent of the study. The non-participants did not differ on any of the parameters mentioned in . Patients enrolled in the study received both standard-of-care treatment and LLLT. Patients were recruited voluntarily. No compensation was offered. Ninety-four patients completed the study. Six patients were excluded, as they did not complete the HRQoL test after treatment (). The inclusion criteria were women with LS of age ≥ 18, who did not have significant relief in symptoms despite of topical treatment with ultrapotent steroids (clobetasol propionate or betamethasone valerat) or calcineurin inhibitors (tacrolimus ointment 0.1%) for a treatment period longer than 3 months. Histopathological verification of the diagnosis was not a requirement as a trained gynaecologist with expertise in LS before inclusion saw all patients. No patient with a history of vulvar intraepithelial neoplasia where included.
Figure 1. Flowchart.
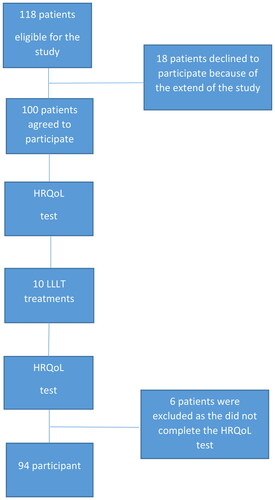
Table 1. Characteristics of cohort and status at initiation of study. N = 94.
The patients received 10 LLLT (Easy Laser®, Denmark) treatments of 808 nm and 500 mW. Every treatment was with a duration of 10 minutes. The first four treatments where planned as two treatments per week. The remaining six treatments where planned as once a week due to logistic considerations. The patient received the LLLT treatment while lying in the same position as during a gynecological examination. The light waves were placed 10 centimetres from the anogenital area covering the symptomatic area. If the patient had symptoms from both the vulva and the area around the rectum, the light were replaced after 10 minutes of treatment making sure no area were treated twice. All patients were recommended to continue their topical treatment during the study period.
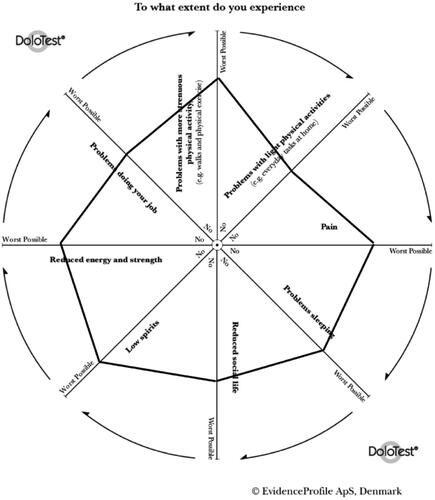
We used a Danish health-related quality of life tool (DoloTest®) to evaluate the effect of the treatment. The DoloTest® will be referred to as HRQoL test. The HRQoL test is a validated Danish tool developed for pain patients. It is validated against the Medical Outcomes Study Short Form Surveys (SF36TM) (Kristiansen et al. Citation2010). The HRQoL test requires little time and is therefore easy to use in a clinical setting (Nielsen et al. Citation2018). It is composed of eight domains arranged in a radar plot; pain, problems sleeping, reduced social life, low spirit, reduced energy and physical strength, problems at work, problems with more strenuous physical activity, and problems with light physical activity. Starting with the domain pain the patient marks every domain horizontally moving clockwise and thereby creates a graphic illustration, which helps the physician and the patient to understand the impact of the condition. The larger the shaded area the more the patient feels affected (). Every mark represents a score. The maximum score of the HRQoL test is the total sum of the eight domains multiplied by 100, the maximum score being 800. The patients completed the HRQoL test before first LLLT treatment and after the last treatment. No deviation from the protocol was made.
Figure 2. A DoloTest profile.
Statistical analysis
Statistical analyses were conducted by the STATA software (version 15; StataCorp LP). We analysed the results from the DoloTest using Mann-Whitney U test and Chi-Square test. No power calculation was made because this was the first study to investigate LLLT as a treatment of LS.
Ethics statement
Scientific Ethics Committee of Denmark and The Danish Data Protection Agency approved the study (S-20182000-49). Written informed consents was obtained from all patients enrolled in the study.
Results
Among the 94 participants included in this study, all patients completed the HRQoL test before and after ended treatment. Median age at time for inclusion was 62 years [InterQuartile Range, IQR 53–69]. The median time from the patient experienced the first symptoms until they were diagnosed (diagnostic delay) was 2 years [IQR 0–8]. In 61 patients, the diagnosis was histopathological confirmed, while the remaining 33 patients were diagnosed by clinical examination. There were no difference on the two groups (diagnosed either with biopsy or clinical examination) when it comes to the demographic data, symptoms of LS or use of treatment before starting LLLT. Burning and itching was the two most common symptoms in our population ().
All patients completed the HRQoL test before and after ended treatment. The results were statistically significant in seven out of the eight domains of the test. The improvement was especially seen on the domains pain (p < 0.001), low spirit (p < 0.001), problems with more strenuous physical activity (p < 0.001) and sleep (p < 0.001). On the domain problems at work, the difference was not found to be statistically significant (p > 0.314) (; ).
Figure 3. DoloTest parametres median scores before and after using laser therapy. N = 94.
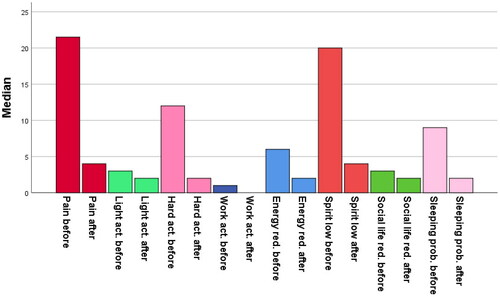
Table 2. DoloTest parametres median scores (and IQR) before and after using laser therapy. N = 94.
We categorised the patients into different groups (), which might have an impact on the results of the treatment. We found the results to be statistically significant in all of the groups except for smoking (p < 0.094). However, the effect seemed to be highest in patients under the age of 62 years, patients with a diagnostic delay of more than two years, patients with disease more than three years, patients with a weekly use of topical treatment above 4 times, and patients who were diagnosed clinically.
Table 3. Total DoloTest median score (and IQR) before and after using laser therapy with and without characteristic. N = 94.
No adverse events have been reported throughout the study period or later.
Discussion
In this study, we have focused on the impact of LLLT on quality of life in women with LS. We included 94 women with LS and insufficient effect of topical treatment. We found that ten LLLT treatments improved the patients’ quality of life immediately after end of treatment. The improvement was seen to be highest on the parameters pain (p < 0.001), low spirit (p < 0.001), problems with more strenuous physical activity (p < 0.001), and sleep (p < 0.001). On the domain problems at work the difference was not found to be statistically significant (p > 0.314).
To our knowledge, this study is one of the first of its kind that investigates the effect of LLLT in patients with LS.
Our data was collected between January 2, 2016, and August 8, 2018. Initially, it was conducted as a quality assurance measure; however, due to the positive results we obtained, we found it beneficial for other clinicians to be aware of.
A limitation to our study is the absence of registration regarding the improvement or aggravation in symptoms before and after treatment. As one of the main goals in treating LS is relief in symptoms, it would have been valuable to see on which symptoms the effect was most significant. Another limitation is that we have not made a HRQoL test as a follow-up to see whether the results were lasting. The main limitation of our study is however the fact that we have not included a control group, which would have given us the possibility to include blinding. At the end, we acknowledge the fact that a nurse was present for each treatment, as their guidance and care might have influenced on the effect of the treatment.
The age group and the average diagnostic delay in our study population are comparable to finding by others (Kirtsig & Sclerosus Citation2016, Pérez-López & Vieira-Baptista Citation2017, Lee & Fischer Citation2018). LS is more often diagnosed in postmenopausal women. This may be one of the reasons for the diagnostic delay as both patients and physicians can confuse the symptoms of LS with the symptoms of vulvovaginal atrophy due to lower oestrogen levels. Other reasons for the diagnostic delay could be women not seeking help, physician’s lack of training, etc.
We found a statistically significant lower total score of the HRQoL test after end of LLLT treatment indicating a better quality of life immediately after ended treatment. There was also an overall improvement in seven of the eight domains of the test with the largest improvement on pain, sleeping problems, low spirit, and problems with more strenuous physical activity. Especially the fact that pain is reduced is important. When the patients experience less pain, they most likely sleep better, which again causes a higher level of energy and ability to cope with normal social and physical activities and thereby improving quality of life. We found no statistically significant improvement on the domain problems at work. The median age in our population was 62 years indicating the majority of our patients were at the end of their working life and thereby were less likely to have a strenuous job.
The effect seemed to be highest in women under the median age of 62 years. This might indicate that the skins ability to regenerate as a result of the LLLT treatment is higher the younger the women are. The improvement was also seen to be highest in women with disease more than 3 years, in women with a diagnostic delay above 2 years and the group diagnosed clinically. This leaves us to think that the disease might be more developed in these patients and thereby the potential to benefit from the treatment is even higher. It might also indicate, that the more developed the disease is, the higher the risk that topical treatment is not enough to reduce the symptoms and thereby leaves us with an even greater need of supplement treatment alternatives such as LLLT. The fact that the effect is also found to be high in the group with a need of topical treatment above 4 times a week underlines this latter statement.
The only group in which we did not find the effect to be statistically significant was in the group of patients who were smoking. This does not come as a surprise as it is well known that the healing process in smokers is reduced. However, it emphasises how important it is to encourage patients with LS to stop smoking.
We do believe that LLLT can improve the quality of life for patients with LS. After completed the study, we have carried out a regime with one monthly treatment in a period of six months after the initial ten treatments on a subset of patients upon their request, which further supports the benefit of LLLT as a an alternative supplement treatment to patients with LS and insufficient effect of topical treatment.
We also wanted to explore whether the Danish HRQoL test is a useful tool for patients with LS. To our knowledge, the test has not been used to describe the quality of life in patients with LS before. We opted for the HRQoL test, as patients with LS in our experience often describe their life affected in the same parameters as patients with pain conditions, however we acknowledge the fact, that it has not been validated for use in patients with LS. The majority of the patients and all of the staff helping the patients with the test found it easy to work with. Some patients found it difficult to mark each point on the domains, however, when comparing the shaded area from both test most patients found the visual effect very useful and the effort worthwhile.
We found that LLLT should be considered as a supplemental therapy to topical treatment in patients with LS affected on their quality of life; however, randomised studies on the topic are needed. We found that the visual effect of the HRQoL test is useful for the patients, when it comes to comprehending the impact of the condition on the quality of life and do recommend others to use the test.
Authors’ contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by all authors. The first draft of the manuscript was written by Pia Kirstine Berthelsen, Mohammed Rohi Khalil and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Acknowledgements
Poul Bak Thorsen, PhD. Department of Gynecology and Obstetrics, University Hospital of Southern Denmark, Lillebaelt Hospital, Kolding, Denmark.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Avci, P., et al., 2013. Low-level laser (light) therapy (LLLT) in skin: stimulating, healing, restoring. Seminars in Cutaneous Medicine and Surgery, 32 (1), 1–7.
- Belotto, R.A., Chavantes, M.C. and Tardivo, J.P., 2017. Therapeutic comparison between treatments for Vulvar Lichen Sclerosus: study protocol of a randomized prospective and controlled trial. Womens Health, 17 (61), 1–8.
- Fistarol, S.K. and Itin, P.H., 2013. Diagnosis and treatment of lichen sclerosus: an update. American Journal of Clinical Dermatology, 14 (1), 27–47.
- Kirtsig, G. and Sclerosus, L., 2016. Presentation, diagnosis and management. Dtsch Arztebl Int, 113, 337–343.
- Kristiansen, K., Lyngholm-Kjaerby, P. and Moe, C., 2010. Introduction and validation of DoloTest®: a new health related quality of life tool used in pain patients. Pain Practice: The Official Journal of World Institute of Pain, 10 (5), 396–403. Volume
- Lee, A. and Fischer, G., 2018. Diagnosis and treatment of vulvar Lichen sclerosus: an update for dermatologists. American Journal of Clinical Dermatology, 19 (5), 695–706.
- Nielsen, M. K., et al., 2018. The DoloTest® in a specialized headache center among patients receiving psychological treatment. A pilot study. Scandinavian Journal of Pain, 18 (3), 431–439.
- Pérez-López, F. R. and Vieira-Baptista, P., 2017. Lichen sclerosus in women: a review. Climacteric: The Journal of the International Menopause Society, 20 (4), 339–347.
- Vieira-Baptista, P., et al., 2022. Risk of development of vulvar cancer in women with Lichen sclerosus or Lichen planus: a systematic review. Journal of Lower Genital Tract Disease, 26 (3), 250–257.
- Yıldız, Ş., et al., 2022. Evaluation of genital self-image and sexual dysfunction in women with vulvar Lichen planus or Lichen sclerosus. Journal of Psychosomatic Obstetrics and Gynaecology, 43 (2), 99–106.
- Zhang, P. and Wu, M.X., 2018. A clinical review of phototherapy for psoriasis. Lasers in Medical Science, 33 (1), 173–180.