

Abstract
Background
Epidural analgesia has emerged as one of the best methods that can be used to reduce labour pain. This study was conducted to assess awareness, attitudes, and practices of pregnant women who visited maternity and antenatal healthcare clinics about epidural analgesia during normal vaginal birth.
Methods
This multicentre study was conducted in a cross-sectional design among pregnant women using a pre-tested questionnaire. The study population in this study was pregnant women who visited maternity and antenatal healthcare clinics in Palestine.
Results
In this study, a total of 389 pregnant women completed the questionnaire. Of the pregnant women, 381 (97.9%) were aware of the existence of epidural analgesia, 172 (44.2%) had already used epidural analgesia, and 57 (33.1%) experienced complications as a result of epidural analgesia. Of the pregnant women, 308 (79.2%) stated that epidural analgesia should be available during vaginal birth. Of the pregnant women, 243 (62.5%) stated that they would use epidural analgesia if offered for free or covered by insurance. Multivariate logistic regression showed that women who were younger than 32 years, who have used epidural analgesia, and those who stated that epidural analgesia should be available during vaginal birth were 2.78-fold (95% CI: 1.54–5.04), 4.96-fold (95% CI: 2.71–9.10), and 13.57-fold (95% CI: 6.54–28.16) more likely to express willingness to use epidural analgesia, respectively.
Conclusions
Pregnant women had high awareness of the existence, moderate knowledge, and positive attitudes towards epidural analgesia for normal vaginal birth. Future studies should focus on educating pregnant women about all approaches that can be used to reduce labour pain including their risks and benefits.
PLAIN LANGUAGE SUMMARY
This study focused on what pregnant women at maternity clinics in Palestine know and think about getting epidural shots during normal births to help lessen the pain when women give birth. Most of the pregnant women have heard about epidural shots and said that these shots should be offered during normal birth. Most of the pregnant women said that they would consider using epidural shots once offered for free or covered by insurance. Younger women, those who had used an epidural before, and those who thought epidurals should be available during birth were more likely to want to use an epidural again.
Introduction
Labour is a physiologic process during which the products of conception are expelled outside the uterus. The onset of labour is defined as regular, painful uterine contractions resulting in progressive cervical effacement and dilatation (Kiely Citation2017). Labour pain is one of the most severe types of pain that women can experience (Koyyalamudi et al. Citation2016). A considerable percentage of women report anxiety as a fear of pregnancy and childbirth because of the severity of labour pain (Junge et al. Citation2018, Deng et al. Citation2021). Epidural analgesia has emerged as one of the best methods that can be used to reduce labour pain (Srebnik et al. Citation2020, Liu et al. Citation2021). Labour pain can affect both the mother and the foetus (Smorti et al. Citation2020). Therefore, management of this pain could be important for the mother and the child. Additionally, management of this pain can improve the quality of life for women of bearing age (Junge et al. Citation2018, Srebnik et al. Citation2020, Liu et al. Citation2021, Deng et al. Citation2021).
Women of childbearing age can be educated about the availability, advantages, and disadvantages of different methods available for the management of labour pain (Junge et al. Citation2018). Among the different methods available to manage labour pain, epidural analgesia is one of the most frequently used methods (Srebnik et al. Citation2020, Liu et al. Citation2021). In this method, local anaesthetics and analgesics are injected into the epidural space to block the nerve roots (Halliday et al. Citation2022).
According to the Palestinian Central Bureau of Statistics, there were 141,092 registered live births in Palestine in 2021 (Statistics Citation2021). Little is known on the use of epidural analgesia in Palestine. Epidural analgesia has many advantages including providing pain relief during the first and second stages of labour, facilitating mother cooperation during labour, provision of analgesia for episiotomy, instrumental birth, and the possibility of either vaginal or caesarean birth (Halliday et al. Citation2022, Anim-Somuah et al. Citation2018). On the other hand, epidural analgesia can be associated with the risk of hypotension, headache, central nervous system infections, trauma due to insertion, and increased risk of obstetric interventions (Anim-Somuah et al. Citation2018, Malevic et al. Citation2019).
Pregnant women lack knowledge about epidural analgesia; therefore, obstetricians, anaesthesiologists, and providers of antenatal care should provide education and information on epidural analgesia to pregnant women and women of childbearing age (Alshahrani Citation2019, Malevic et al. Citation2019, Ageel et al. Citation2022, Ali Alahmari et al. Citation2020).
Little is known about what pregnant women who visit maternity and antenatal healthcare clinics in developing countries know about the availability of epidural analgesia for normal vaginal birth in Palestine as a developing country. Additionally, little is also known about what pregnant women know about the benefits and risks of epidural analgesia in normal vaginal birth (Almuntashiri et al. Citation2022, Parajuli et al. Citation2024). Therefore, this study aimed to assess the awareness, attitudes, and practices of pregnant women who visit maternity and antenatal healthcare clinics about epidural analgesia during normal vaginal birth. The study also aimed to identify predictors of high knowledge and willingness to use epidural analgesia in normal vaginal birth. The findings of this study might inform future practices in gynaecology and obstetrics, anaesthesiology, and antenatal care in developing countries.
Methods
Study design
This multicentre study was conducted in a cross-sectional design among pregnant women using a pre-tested questionnaire. The study was conducted and reported in adherence to the strengthening of the reporting of observational studies in epidemiology (STROBE) statement (Vandenbroucke et al. Citation2007). Adherence to the STROBE statement is shown in Supplementary Table S1.
Study population and sample size
The study population in this study was pregnant women who visited maternity and antenatal healthcare clinics in Palestine. The sample size was calculated using Daniel’s formula. An online sample size calculator was used to compute the number of pregnant women needed for this study (www.raosoft.com). The sample size was calculated at a 95% confidence interval (95% CI) accepting a margin of error of 5%. The sample size needed for this study was approximately 385 pregnant women.
Recruitment and data collection
In this study, the pregnant women were included if they visited maternal and antenatal healthcare clinics in Palestine, were older than 18 years old, expressed willingness to respond to items in a questionnaire, and agreed to provide written informed consent. A convenience sampling technique was used to recruit the pregnant women in this study. Field researchers visited the maternity and antenatal healthcare clinics and approached the pregnant women. The field researchers explained the objectives of the study to the potential participants, invited them to take part in the study, and obtained their informed consent.
The data were collected using a questionnaire that was developed from previous studies (Gari et al. Citation2017, Alshahrani Citation2019, Ali Alahmari et al. Citation2020, Ageel et al. Citation2022, Almuntashiri et al. Citation2022). The face and content validity of the questionnaire was assessed by a panel of experts. Because the women were native Arabic speakers, the questionnaire was developed in Arabic language. The panel was composed of anaesthesiologists (n = 2), gynaecologists (n = 3), and pharmacologists (n = 2). The panellists rated each item in the questionnaire using a 5-point Likert scale (1 = strong disagreement with the suitability of the item, 5 = strong agreement with the suitability of the item). The items on which the panellists agreed were included in the final questionnaire. Conflicting ratings were resolved through discussion and consensus. The questionnaire contained three sections. The first section contained 7 items that were designed to collect the sociodemographic variables of the women including age, place of residence, educational level, employment status, self-rated satisfaction with household income, having a health insurance, and number of children. The second section contained 7 items. In this section, the women were asked about their awareness of the existence of epidural analgesia for normal birth, sources of information about epidural analgesia, whether they have used epidural analgesia before, whether they have experienced complications as a result of epidural analgesia, and opinion on the availability of epidural analgesia during vaginal birth. The women were also asked whether they would use epidural analgesia if offered for free or covered by insurance and the reasons for not using epidural analgesia. The third section contained a knowledge test of 18-items about epidural analgesia. The women could answer each item by choosing either no, yes, or I don’t know. The questionnaire is shown in Table S2.
A pilot test was conducted among 20 women who did not participate in the large study. The women were asked to respond to and provide written feedback on the readability and comprehensibility of the questionnaire. The test-retest method was used to assess the stability of responses over a short period. The women were asked to respond to the questionnaire twice. Responses in both rounds were correlated using Pearson’s correlations. It was decided a priori that a Pearson’s r of > 0.80 would indicate acceptable test-retest reliability. In this study, the Pearson’s r was 0.92 which indicated excellent test-retest reliability. The internal consistency of the items was tested using Cronbach’s alpha statistics. It was decided a priori that a Cronbach’s alpha of > 0.70 would indicate acceptable internal consistency. In this study, Cronbach’s alpha was > 0.70 which indicated acceptable internal consistency.
Data analysis
The data were analysed using IBM SPSS version 21.0 for Windows. Data were expressed as numbers and percentages. For the knowledge questions, women were awarded 1 point for each correct answer, and knowledge scores were expressed as percentages that could range from 0 to 18. The knowledge scores were converted into percentages and ranged from 0% to 100%. Knowledge scores were compared using Student’s t-test. Categorical data were compared using chi-square or Fisher’s exact test. The variables that were significantly associated with the knowledge scores were retained in a multiple linear regression model. Odds ratios (OR) with their 95% 95% CI were calculated using multivariate logistic models. Statistical significance was indicated by a p-value < 0.05.
Ethical considerations
The study was conducted in adherence to the international ethical standards governing scientific studies. Approvals were obtained from the Institutional Review Board of An-Najah National University (Approval #Med. Nov. 2021/4), the Office of Health Education of the Palestinian Ministry of Health, and administrators of the maternity and antenatal healthcare clinics. The pregnant women provided written informed consent before they took part in the study.
Results
Demographic variables of the pregnant women
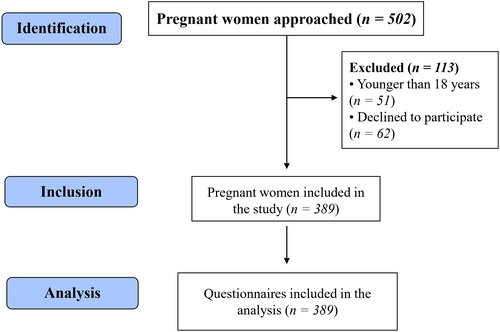
Of the 502 pregnant women who were approached, a total of 389 pregnant women completed the questionnaire (response rate = 77.5%). The STROBE flowchart is shown in .
Figure 1. Flow diagram of women recruitment.
The mean age of the pregnant women was 32.1 ± 8.0 years. Of the pregnant women, 221 (56.8%) lived in urban areas, 301 (77.4%) had a university degree, 218 (56.0%) were employed, 249 (64.0%) were satisfied with their household income, and 321 (82.5%) had health insurance. Of the pregnant women, 172 (44.2%) had more than 2 children. Detailed demographic variables of the women are shown in .
Table 1. Demographic variables of the women who participated in the study (n = 389).
Awareness, attitude, and experience with epidural analgesia
In this study, the vast majority of the pregnant women (97.9%) were aware of the existence of epidural analgesia for normal birth. The pregnant women stated that they were informed about epidural analgesia by other women who used it before, gynaecologists/obstetricians, friends or family, social media or the internet, anaesthesiologists, and nurses or midwives.
Of the pregnant women, 172 (44.2%) have already used epidural analgesia. Of those, 57 (33.1%) experienced complications as a result of epidural analgesia. Of the pregnant women, 308 (79.2%) stated that epidural analgesia should be available during vaginal birth. Of the pregnant women, 243 (62.5%) stated that they would use epidural analgesia if offered for free or covered by insurance. The reasons for not using epidural analgesia included being in their first pregnancy, fear of the adverse effects did not suffer severe labour pain, desire to experience normal birth without analgesia, faster birth, and lack of awareness about epidural analgesia. Detailed answers from the pregnant women are shown in .
Table 2. Awareness, attitude, and experience with epidural analgesia.
Of the pregnant women, 298 (76.6%) knew that only physicians with adequate privileges can administer epidural analgesia, 269 (69.2%) knew that epidural analgesia was one of the most effective methods of reducing labour pain in a normal birth, 247 (63.5%) knew that epidural analgesia was less painful than labour, 220 (56.6%), 220 (56.6%) knew that epidural analgesia does not affect birth outcomes, and 197 (50.6%) knew that epidural analgesia needed signing informed consent. On the other hand, more than half of the women lacked knowledge of the adverse effects that could be associated with epidural analgesia. Detailed answers from the pregnant women are shown in .
Table 3. Answers of the women on the knowledge items.
Association between demographic, attitude, and experience of women with knowledge scores about epidural analgesia
In this study, the mean knowledge scores were significantly higher for pregnant women who had university degrees, were employed, were satisfied with their household income, had children, had used epidural analgesia before, have experienced complications as a result of epidural analgesia, did not agree that epidural analgesia should be available during vaginal birth, and those who would not use epidural analgesia even if it was offered for free or covered by insurance. Details of the associations are shown in Table S3.
When the variables that were significantly associated with the knowledge scores were retained in multiple linear regression, having used epidural analgesia and having experienced complications as a result of epidural analgesia were strongly and significantly associated. Details of the multiple linear regression model are shown in Table S4.
Association between demographic, attitude, and experience of women with the willingness to use epidural analgesia if offered for free or covered by health insurance
In this study, willingness to use epidural analgesia if offered for free or covered by health insurance was significantly associated with place of residence, educational level, having used epidural analgesia, and agreement that epidural analgesia should be available during vaginal birth as shown in Table S5.
When the variables that were significantly associated with willingness to use epidural analgesia were included in a multivariate logistic regression model, women who were younger than 32 years, who have used epidural analgesia, and those who stated that epidural analgesia should be available during vaginal birth were 2.78-fold (95% CI: 1.54–5.04), 4.96-fold (95% CI: 2.71–9.10), and 13.57-fold (95% CI: 6.54–28.16) more likely to express willingness to use epidural analgesia as shown in Table S6.
Discussion
In this study, the vast majority of the pregnant women were aware of the existence of epidural analgesia for normal birth and their main resource information was other women who used it before and gynaecologists/obstetricians. The awareness reported in this study was comparatively higher than that reported among pregnant women in developing countries like Nigeria and Saudi Arabia (Oladokun et al. Citation2009, Gari et al. Citation2017, Olaleye et al. Citation2020, Ageel et al. Citation2022, Almuntashiri et al. Citation2022). These findings might be explained by the multiple sources from which the pregnant women received information. Moreover, less than half (44.2%) of the pregnant women had used epidural analgesia before. Again, this percentage was higher than that reported in other developing countries (Oladokun et al. Citation2009, Ageel et al. Citation2022). When the pregnant women were asked to state the reason for not using epidural analgesia, 42.9% stated that it was their first pregnancy. Additionally, the majority of the pregnant women stated that epidural analgesia should be available during vaginal birth and they would use epidural analgesia if offered for free or covered by insurance. These findings indicate a positive attitude of the pregnant women included in this study towards epidural analgesia.
In this study, knowledge of epidural analgesia was associated with having a university degree, being employed, and expressing satisfaction with household income. These findings were not surprising as educated women could have searched for more information about epidural analgesia. The findings reported in this study were consistent with those previously reported elsewhere (Oladokun et al. Citation2009, Ali Alahmari et al. Citation2020, Ageel et al. Citation2022). Moreover, women with university degrees were more likely to be employed and report higher household income. Again, knowledge of epidural analgesia was associated with having used epidural analgesia. These findings were consistent with those previously reported in other studies (Oladokun et al. Citation2009, Gari et al. Citation2017, Olaleye et al. Citation2020, Ageel et al. Citation2022, Almuntashiri et al. Citation2022). The women who used epidural analgesia were more likely to have children and have experienced complications as a result of epidural analgesia. Therefore, they were more likely to not agree that epidural analgesia should be available during vaginal birth and would refuse to use epidural analgesia even if it was offered for free or covered by insurance. Therefore, multiple linear regression showed that having used epidural analgesia and having experienced complications as a result of epidural analgesia were predictors of higher knowledge scores. Fear of complications and fear of adverse effects were previously reported as the main reasons for not using epidural analgesia in normal birth (Van den Bussche et al. Citation2007, Chang et al. Citation2008). The prevalence rate of failed epidural analgesia was reported at 15.2% (Ismail et al. Citation2021). Taken together, these findings might indicate that anaesthesiologists, gynaecologists and obstetricians, nurses, midwives, and other providers of antenatal care should design interventions to explain the benefits and risks of epidural analgesia for women with low educational levels.
In this study, younger women, who have used epidural analgesia, and those who stated that epidural analgesia should be available during vaginal birth were likely to express willingness to use epidural analgesia. The findings reported in this study were consistent with those reported in Saudi Arabia and Nigeria (Oladokun et al. Citation2009, Gari et al. Citation2017, Ageel et al. Citation2022, Almuntashiri et al. Citation2022). Probably, more studies are needed to further investigate and analyse the decisions of pregnant women to use epidural labour analgesia using appropriately validated models. For the first time, the knowledge, attitudes, and practices of pregnant women visiting maternity and antenatal healthcare clinics in Palestine regarding epidural analgesia for normal vaginal birth were assessed in this study. The findings reported in this study could be informative to anaesthesiologists, gynaecologists and obstetricians, nurses, midwives, and other providers of antenatal care in developing countries.
Strengths and limitations of the study
The findings reported in this study should be interpreted after considering the following strengths and limitations. First, this is the first study of knowledge, attitudes, and practices of pregnant women visiting maternity and antenatal healthcare clinics in Palestine regarding epidural analgesia for normal vaginal birth. The findings of this study might be informative to anaesthesiologists, gynaecologists and obstetricians, nurses, midwives, and other providers of antenatal care in developing countries. Second, a large sample size was used in this study. The findings reported from large studies are more rigorous than those reported from studies with small sample sizes. Additionally, the sample used in this study was diversified in terms of age groups, place of residence, educational level, employment status, household income level, health insurance status, and the number of previous pregnancies. This diversity should have improved the representativeness and external validity of the findings reported in this study. Third, the questionnaire used in this study was assessed for face and content validity, test re-test reliability, and internal consistency. These diagnostics should have improved rigour in this study.
On the other hand, the study has some limitations. First, the study was conducted in a cross-sectional design. Cross-sectional studies are time-limited because the results represent the views and opinions of the participants within the time frame in which the study was conducted. Second, this was an observational study and no interventions were administered. Probably, the findings could have been more interesting had an intervention, such as an educational intervention, been tested. Third, the data collected in this study were self-reported by the participants. Therefore, desirability and recall bias could not be excluded in this study as women might have tended to provide more positive answers. Fourth, the sample was recruited using a convenience sampling approach. Compared to probability sampling techniques, non-probability sampling techniques are associated with higher selection bias.
Conclusions
Pregnant women had high awareness of the existence, moderate knowledge, and positive attitudes towards epidural analgesia for normal vaginal birth. Higher knowledge could be predicted by having used and having experienced complications as a result of epidural analgesia. Willingness to use epidural analgesia was predicted by younger age, previous use of epidural analgesia, and stating that epidural analgesia should be available during vaginal birth. Future studies should focus on educating pregnant women about all approaches that can be used to reduce labour pain including their risks and benefits.
Authors’ contributions
Ramzi Shawahna contributed to conception and design, analysis and interpretation of data, drafting and revising the work, approving the final version, and accepting accountability for all aspects of the work.
Dana Khaskia contributed to acquisition, analysis and interpretation of data, drafting the work, approving the final version and accepting accountability for all aspects of the work.
Donya Ali contributed to acquisition, analysis and interpretation of data, drafting the work, approving the final version and accepting accountability for all aspects of the work.
Hajar Hodroj contributed to acquisition, analysis and interpretation of data, drafting the work, approving the final version and accepting accountability for all aspects of the work.
Mohammad Jaber contributed to conception and design, analysis and interpretation of data, drafting and revising the work, approving the final version, and accepting accountability for all aspects of the work.
Iyad Maqboul contributed to conception and design, analysis and interpretation of data, drafting and revising the work, approving the final version, and accepting accountability for all aspects of the work.
Hatim Hijaz contributed to conception and design, analysis and interpretation of data, drafting and revising the work, approving the final version, and accepting accountability for all aspects of the work.
Supplemental Material
Download MS Word (56.3 KB)Acknowledgements
The authors would like to thank the women who participated in this study. An-Najah National University is acknowledged for making this study possible.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
All data relevant to this study were included in the manuscript or as supplementary materials. The data sets used in the analysis can be obtained from the corresponding author upon request.
Additional information
Funding
References
- Ageel, M., et al., 2022. Knowledge and practice of and attitude toward epidural analgesia among pregnant women in Jazan Region of Saudi Arabia. Cureus, 14 (6), 1.
- Ali Alahmari, S. S., et al., 2020. Knowledge, attitude, and practice of childbearing women toward epidural anesthesia during normal vaginal delivery in Alsanayeah Primary Health Care in Khamis Mushait. Journal of Family Medicine and Primary Care, 9 (1), 99–8.
- Almuntashiri, W. M., et al., 2022. Awareness among pregnant women about epidural Analgesia: a cross-sectional study. Anesthesiology Research and Practice, 2022, 7388833.
- Alshahrani, M. S., 2019. An evaluation of the different types of labor pain relief, preferred methods of pain relief, and effects of social media on awareness and knowledge among pregnant women. A cross-sectional study in the Kingdom of Saudi Arabia. Saudi Medical Journal, 40 (9), 914–921.
- Anim-Somuah, M., et al., 2018. Epidural versus non-epidural or no analgesia for pain management in labour. The Cochrane Database of Systematic Reviews, 5 (5), Cd000331.
- Chang, K. Y., et al., 2008. Decision analysis for epidural labor analgesia with Multiattribute Utility (MAU) model. The Clinical Journal of Pain, 24 (3), 265–272.
- Deng, Y., et al., 2021. A comparison of maternal fear of childbirth, labor pain intensity and intrapartum analgesic consumption between primiparas and multiparas: a cross-sectional study. International Journal of Nursing Sciences, 8 (4), 380–387.
- Gari, A., et al., 2017. Awareness of epidural analgesia among pregnant women in Jeddah, Saudi Arabia. Electronic Physician, 9 (5), 4274–4280.
- Halliday, L., Nelson, S. M. and Kearns, R. J., 2022. Epidural analgesia in labor: a narrative review. International Journal of Gynaecology and Obstetrics, 159 (2), 356–364.
- Ismail, S., et al., 2021. Failure rate of labor epidural: an observational study among different levels of trainee anesthesiologists in a university hospital of a developing country. Journal of Anaesthesiology, Clinical Pharmacology, 37 (2), 210–215.
- Junge, C., et al., 2018. Labor pain in women with and without severe fear of childbirth: a population-based, longitudinal study. Birth, 45 (4), 469–477.
- Kiely, D. J., 2017. Management of spontaneous labour at term in healthy women. Journal of Obstetrics and Gynaecology Canada, 39 (4), 220–221.
- Koyyalamudi, V., et al., 2016. New labor pain treatment options. Current Pain and Headache Reports, 20 (2), 11.
- Liu, X., et al., 2021. The effect of epidural analgesia on maternal-neonatal outcomes: a retrospective study. Ginekologia Polska, 92 (9), 637–641.
- Malevic, A., Jatuzis, D. and Paliulyte, V., 2019. Epidural Analgesia and back pain after labor. Medicina, 55 (7), 55.
- Oladokun, A., et al., 2009. Awareness and desirability of labor epidural analgesia: a survey of Nigerian women. International Journal of Obstetric Anesthesia, 18 (1), 38–42.
- Olaleye, O., Dada, S. O. and Alabi, G. O., 2020. Awareness and utilization of obstetric epidural analgesia in labour among pregnant women in Wesley Guild Hospital Ilesha, Nigeria. International Quarterly of Community Health Education, 2020, 272684X20972839.
- Parajuli, B. D., et al., 2024. Knowledge and attitude about labor epidural analgesia among pregnant women attending antenatal clinic. Journal of Nepal Health Research Council, 21 (4), 623–628.
- Smorti, M., et al., 2020. Psychological factors and maternal-fetal attachment in relation to epidural choice. Midwifery, 88, 102762.
- Srebnik, N., et al., 2020. The impact of epidural analgesia on the mode of delivery in nulliparous women that attain the second stage of labor. Journal of Maternal-Fetal and Neonatal Medicine, 33, 2451–2458.
- Statistics, P. C. B. O., 2021. Number of Registered Live Births in Palestine. Ramallah, Palestine: Palestinian Central Bureau of Statistics and Ministry of Health.
- Van Den Bussche, E., et al., 2007. Why women prefer epidural analgesia during childbirth: the role of beliefs about epidural analgesia and pain catastrophizing. European Journal of Pain, 11 (3), 275–282.
- Vandenbroucke, J. P., et al., 2007. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. PLoS Medicine, 4 (10), e297.