

Abstract
Background
Prognostic factors-based nomograms have been utilised to detect the likelihood of the specific cancer events. We have focused on the roles of aldehyde dehydrogenase 1 (ALDH1) and p-AKT in predicting the prognosis of BC patients. This study was designed to establish nomograms based on the integration of aldehyde dehydrogenase 1 (ALDH1) and p-AKT in predicting the disease-free survival (DFS) and overall survival (OS) of breast cancer (BC) patients.
Methods
Demographic and clinical data were obtained from BC patients admitted to our hospital between September 2015 and August 2016. Univariate and multivariate Cox regression analyses were utilised to analyse the risk factors of recurrence and mortality. The nomograms for predicting the DFS and OS were established using the screened risk factors. Stratified analysis was performed with the cut-off value of exp (pi) of 4.0-fold in DFS and OS, respectively.
Results
Multivariate Cox regression analysis indicated that ALDH, p-AKT and pathological stage III were independent risk factors for the recurrence among BC patients. ALDH1, p-AKT, pathological stage III and ER-/PR-/HER2- were independent risk factors for the mortality among BC patients. The established nomograms based on these factors were effective for predicting the DFS and OS with good agreement to the calibration curve and acceptable area under the receiver operating characteristic (ROC) curve. Finally, stratified analyses showed patients with a low pi showed significant decrease in the DFS and OS compared with those of high risk.
Conclusion
We established nomograms for predicting the DFS and OS of BC patients based on ALDH1, p-AKT and pathological stages. The ER-/PR-/HER2- may be utilised to predict the OS rather than DFS in the BC patients.
PLAIN LANGUAGE SUMMARY
Many breast cancer patients show poor response after treatment due to recurrence and metastasis. Therefore, early prediction of the disease-free survival and overall survival is crucial to the treatment outcome and clinical decision-making. In this study, we established nomograms with the demographic and clinical data from breast cancer patients admitted to our hospital between September 2015 and August 2016. Univariate and multivariate Cox regression analyses showed that some important proteins and signalling pathways were risk factors for decreased disease-free survival and overall survival of breast cancer patients. On this basis, we established an effective nomogram for predicting the disease-free survival and overall survival of these patients based on these factors. This study offers new options in the predicting the treatment outcome of breast cancer patients.
Introduction
Breast cancer (BC) is one of the most commonly diagnosed malignancies among female population, causing great threats to the public health worldwide (Łukasiewicz et al. Citation2021). Patients with BC are mainly treated by surgery, chemotherapy, radiotherapy and immune therapy, but the treatment outcome is still not good due to recurrence and metastasis (Miller et al. Citation2022; Trayes and Cokenakes Citation2021). Moreover, the evidence and guidelines for BC treatment are not sufficient. Given these situations, clinicians are usually challenged with making reasonable treatment decisions (Burguin et al. Citation2021).
Nowadays, prognostic factors-based nomograms have been widely used to quantify the likelihood of the specific events of cancer, such as recurrence, poor response and poor prognosis (Gold et al. Citation2009; Zhang et al. Citation2022). Indeed, the nomograms can be utilised for predicting the recurrence and mortality in BC, which potentially facilitate to the screening of patients required positive treatment strategies. Actually, it is not possible to include all the demographic, clinical and pathological factors into the nomograms. According to our clinical experiences, we have focused on the roles of aldehyde dehydrogenase 1 (ALDH1) and p-AKT in predicting the prognosis of BC patients (Yu et al. Citation2010; Zhou et al. Citation2018). This leads us to investigate the possibility of integrating ALDH1 and p-AKT in establishing nomograms for predicting the recurrence and mortality of BC. In addition, triple-negative BC (TNBC) is considered the most lethal condition for BC, as these patients show resistance to chemotherapy (Yin et al. Citation2020). Thus, this study was designed to establish nomograms for predicting disease-free survival (DFS) and overall survival (OS) in BC patients based on the combination of ER-/PR-/HER2- and ALDH1 and p-AKT.
Methods
Study design
Chinese female patients with invasive ductal BC admitted to the Department of Thyroid, Breast and Vascular Surgery, Shanghai Fourth People’s Hospital, School of Medicine, Tongji University between September 2015 and August 2016 were included in this retrospective study. The inclusion criteria were as follows: (i) patients with BC aged 18 years or more; (ii) those confirmed with invasive ductal BC based on pathological findings; (iii) received surgery for the treatment. Patients with the following conditions were excluded from this study: (i) with distal metastasis; (ii) those received radiotherapy, chemotherapy and endocrine therapy before surgery; (iii) with poor treatment compliance; (iv) those with other concurrent malignancies. Pathological information collected from each patient included the following aspects: oestrogen receptor (ER) status, progesterone receptor (PR) status, histological tumour type, primary tumour size, axillary lymph node status and clinical stage. The clinical stage was classified based on the American Joint Committee on Cancer tumour node metastasis staging system. This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Shanghai Fourth People’s Hospital, School of Medicine, Tongji University (2020053-001). The requirement for written informed consent was waived.
Data collection
In our previous experiences, we have focused on the prognostic relevance of ALDH1 and p-AKT in BC (Yu et al. Citation2010; Zhou et al. Citation2013). These data revealed that ALDH1 and p-AKT may serve as important predictors for the recurrence and mortality of BC. On this basis, we then collected the age, year of diagnosis, ALDH1 and p-AKT concentrations, lesion size, metastatic lymph nodes, pathological staging (I, II, III) and expression of PR, ER and HER2 from each patient. The concentrations of ALDH1, p-AKT, PR, ER and HER2 were measured using the immunohistochemistry (IHC) according to the previous descriptions (Chen et al. Citation2022; Yu et al. Citation2010; Zhou et al. Citation2018).
Patients’ follow-up
Each patient was followed up by telephone communication. The patients were subject to follow-up until August 2022, or until death. Besides, we tried to ask for the reasons for the death of the patients from their family members.
Statistical analysis
Data analysis was performed using SPSS Statistics 22.0 software and R package (version 4.1.2). Chi-squared test was conducted to compare the difference between categorical variables of the two groups that were presented in a form of percentage (%). Significant difference was defined in the presence of a P value of less than 0.05. Multivariate Cox regression following univariate regression analysis was utilised to analyse the independent risk factors of BC recurrence and mortality. The hazard ratio (HR) and 95% confidence interval (CI) were calculated. The nomograms for predicting the recurrence and mortality of the patient were established using the risk factors screened after multivariate regression analysis. The calibration curve was utilised to compare the predicted recurrence and mortality with these of the actual values after Kaplan-Meier estimation. Upon the establishing of nomograms, we then performed the stratified analysis with the cut-off value of exp (pi) of 4.0-fold in recurrence and mortality, respectively.
Results
Efficiency of ALDH1, p-AKT and pathological stage-based nomogram in predicting the recurrence of BC
In total, 138 patients were included in this study (). Based on the recurrence, BC patients were classified into the recurrence group (n = 32) and non-recurrence group (n = 106). Univariate analysis was initially carried out to investigate the factors related to the recurrence of BC, which indicated statistical differences in the ALDH1 (p < 0.001), p-AKT (p = 0.002) and metastatic lymph node (p = 0.001) between the recurrence group and non-recurrence group (). In addition, pathological stage of III showed statistical differences between the two groups (p = 0.001). Then statistically significant variables screened from the univariate analysis were subjected to multivariate Cox regression analysis, and ALDH (p < 0.001), p-AKT (p = 0.006) and pathological stage III (p < 0.001) were independent risk factors for the recurrence among BC patients ().
Figure 1. Based on the study flowchart, 138 were included in this retrospective analysis. The patients were divided into a recurrence group and non-recurrence group based on the recurrence after treatment. IDBC: invasive ductal breast cancer.
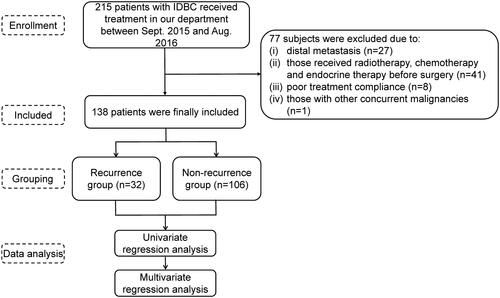
Table 1. Univariate and multivariate regression analysis results for recurrence.
Establishing and validation of a nomogram for predicting BC recurrence
A prognostic nomogram was established for BC based on the Akaike information criteria (AIC) using the variables after multivariate regression including ALDH, p-AKT and pathological stages. The established nomograph could predict the 3-year DFS and 5-year DFS of the BC patients, respectively ().
Figure 2. Prediction nomogram for the 3-yr and 5-yr DFS using ALDH1, p-AKT, and pathological stages in BC patients (A). Calibration curve and ROC curve of the nomogram for predicting DFS in BC patients (B). (a, b) The consistence of predicted 3-yr and 5-yr DFS and the actual 3-yr and 5-yr DFS. (c) The AUC calibration plot. Kaplan-Meier curves for the DFS of BC patients after PI-based stratification (C). DFS: disease-free survival; ALDH1: aldehyde dehydrogenase 1; ROC: receiver operating characteristic; BC: breast cancer; AUC: area under the ROC curve.
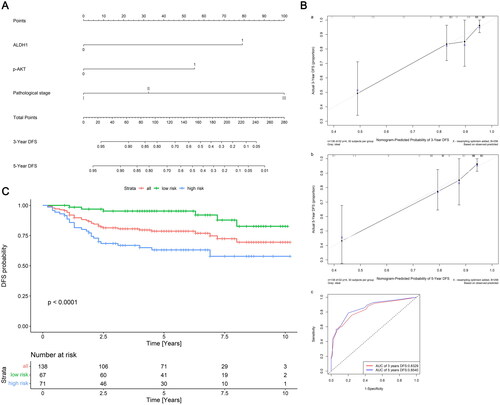
The calibration curves for the 3-year and 5-year DFS were then drawn to validate the efficiency of the nomogram, respectively. As shown in , there was a good agreement between the actual 3-year and 5-year DFS and the predicted 3-year and 5-year DFS. Besides, the area under the ROC curve (AUC) was 0.83 and 0.85, respectively ().
Stratified analysis of patients’ DFS using prognostic index
In this section, we stratified the patients into low and high PI groups, based on exp (pi) values of less than 4.0-fold and ≥4.0-fold increase in the death risk. The number of BC patients in low and high PI risk groups was 67 and 71, respectively. Patients with a low PI value showed a significantly higher DFS probability compared with the high-risk patients (p < 0.001, ).
Efficiency of ALDH1, p-AKT, pathological stage and ER-/PR-/HER2- based nomogram in predicting the mortality of BC
Based on the death outcome, the patients were classified into mortality group (n = 25) and survival group (n = 113), respectively. Univariate analysis indicated statistical differences in the ALDH1 (p = 0.001), p-AKT (p = 0.006) and lymph node number (p = 0.008), pathological stage of III (p = 0.003), and ER-/PR-/HER2- (p = 0.036) between the two groups. According to the multivariate Cox regression analysis, ALDH1 (p = 0.013), p-AKT (p = 0.011), pathological stage of III (p = 0.001), and ER-/PR-/HER2- (p = 0.042) were independent risk factors for mortality in BC patients ().
Table 2. Univariate and multivariate regression analysis results for mortality.
Establishing and validation of a nomogram for OS prediction among BC patients
Using AIC, a prognostic nomogram for mortality in patients with BC was established using the variables after multivariate regression including ALDH1, p-AKT, pathological stage, as well as ER-/PR-/HER2-. The established nomograph contributed to the prediction of the 3-year and 5-year OS, respectively ().
Figure 3. Prediction nomogram for the 3-yr and 5-yr OS using ALDH1, p-AKT, pathological stages and ER-/PR-/HER2- in BC patients (A). Calibration curve and ROC of the nomogram for OS in BC patients (B). (a, b) The consistence of predicted 3-yr and 5-yr OS and the actual 3-yr and 5-yr OS. (c) AUC calibration plot. Kaplan-Meier curves for the OS of BC patients after pi-based mortality stratification (C). OS: overall survival; ALDH1: aldehyde dehydrogenase 1; ROC: receiver operating characteristic; BC: breast cancer; AUC: area under the ROC curve; ER: oestrogen receptor; HER2: human epidermal growth factor receptor 2; PR: progesterone receptor.
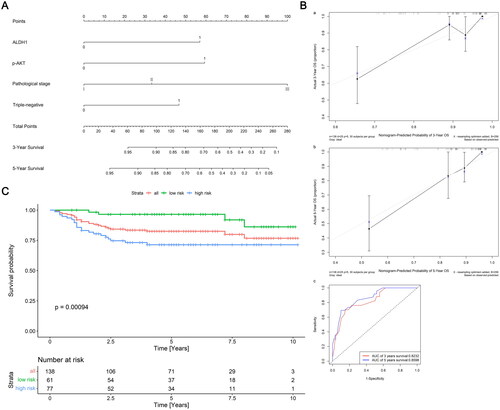
For the validation of the nomogram, we drew the calibration curve for the 3-year and 5-year mortality, respectively. There was a good agreement between the actual 3-year and 5-year OS and the predicted 3-year and 5-year OS (). The AUC for the 3-year OS was 0.85, while that of the 5-year OS was 0.87 ().
Stratified analysis of patients’ mortality using prognostic index
In this section, we stratified the patients into low and high pi groups, based on exp (pi) values of less than 4.0-fold and ≥4.0-fold increase in the death risk. The number of BC patients in low and high pi risk groups was 61 and 77, respectively. Patients with a low PI value showed a significantly higher OS probability compared with the high-risk patients (p = 0.00094, ).
Discussion
BC ranks as the second leading cause for cancer-related death in the female population. To date, many BC patients still show a poor prognosis due to recurrence and metastasis after treatment. Besides, the number of cancer-related deaths is disturbingly increasing annually, which is a severe threat to the public health, especially the developing countries (Siegel et al. Citation2021). We have focused on the predictive roles of ALDH1 and p-AKT in the prediction of BC prognosis. Besides, increased concentration of ALDH1 was associated with a poor outcome (Ozaki et al. Citation2022), while the PI3K/AKT signalling pathway was well acknowledged to responsible for the chemotherapy resistance and metastasis of cancer cells (Rascio et al. Citation2021). Therefore, we aimed to establish nomograms for predicting the DFS and OS in BC patients based onALDH1 and p-AKT.
Early screening of recurrence and metastasis is crucial for the treatment of BC patients, in order to obtain a satisfactory outcome. Up to now, ALDH1 has been reported to be related to the BC outcome, but our understanding on it is still limited. ALDH1, a cancer stem cell marker, was associated with a shorter survival and poor clinical response to adjuvant chemotherapy (Panigoro et al. Citation2020). In a meta-analysis, Han et al. indicated that ALDH1 may be more valuable as an effective treatment target for long-term survival in patients with advanced cancers (Han et al. Citation2019). In a study focused on the ALDH1 expression in patients received chemotherapy with cyclophosphamide, Khoury et al. indicated that ALDH1A1 may predict poor prognosis after chemotherapy in the neoadjuvant setting with substantial residual cancer burden (Khoury et al. Citation2012). Moreover, in a study focused on evaluating the expression of ALDH1 in ipsilateral recurrence, BC patients with ipsilateral recurrence along with the expression of ALDH1 and Ki-67 showed a poorer prognosis compared with the counterparts without ALDH1 and Ki-67 expression (Saba and Jaffe Citation1980). Consistently, our data showed that ALDH1 could be adopted in the nomogram for predicting DFS and OS in BC patients. In the future, more studies are required to investigate the potential mechanism in this process.
As a complicated signalling pathway that triggers proliferation of cancer cells, PI3K/AKT is closely related to the endocrine resistance in BC. PI3K/AKT signalling pathway showed a close link with the invasion and metastasis of BC. In addition, phosphorylation of AKT was reported to participate in BC metastasis and recurrence. Enumeration studies have indicated that PI3K/AKT inhibitors or rapalogs are active in BC (Miricescu et al. Citation2020). Such pathway involved in resistance of BC with overexpression of HER2- to trastuzumab. In a previous preclinical study, PI3K/AKT pathway inhibitor could synergistically act with trastuzumab in resistant cells (Liu et al. Citation2020). Meanwhile, preclinical evidence showed that inhibition of PI3K/AKT pathway contributed to the sensitisation of BC cells to doxorubicin (Roudier et al. Citation2006). The p-AKT expression was negatively correlated with the prognosis of patients with BC (Tokunaga et al. Citation2006). As a member of AGC family of protein kinase, AKT also involved in the survival, proliferation, invasion and angiogenesis of cancers. More importantly, activating mutations and amplification of AKT components are reported to involve in the pathogenesis of BC (Shariati and Meric-Bernstam Citation2019). For the mechanism, AKT could inactivate proapoptotic proteins, such as procaspase-9 and BCL-2 antagonist of cell death. Besides, AKT could prevent cyclin D1 degradation through phosphorylating and inhibiting the glycogen synthase kinase 3β (GSK3β) (Arcaro and Guerreiro. Citation2007). Consistently, our previous study showed p-AKT was associated with poor prognosis in female population in mainland China with invasive ductal BC (Zhou et al. Citation2018). In this study, p-AKT expression was adopted in the established nomogram for predicting recurrence and mortality in BC patients, and its efficiency was confirmed to be effective after the stratified analysis.
The pathological staging, combining the clinical staging and histopathological findings, has been considered as the gold standard for cancer staging (Plichta et al. Citation2019). Upon stage estimation, we could determine the final prognostic stage in a more accurate manner, which then could predict the prognosis effectively. As there might be discordance between clinical and pathological stages in BC patients, we selected the pathological stage data from each patient in this study. Finally, the nomograms established using pathological stage were approved to be effective for predicting the recurrence and mortality.
It has been well acknowledged that PR, ER and HER2 are usually detected in BC samples. These markers are reliable with less cost for the patients, which is helpful for the therapeutic decision of the clinicians. BC could be divided into the following subtypes according to the IHC results: i) Liminal A subtype (high ER and PR; HER2: negative; low Ki67); ii) Liminal B subtype (positive ER and/or PR; HER2: negative; high Ki67); iii) triple-negative subtype (ER, PR and HER2 negative); and iv) HER2 positive subtype (ER and PR negative; HER2 positive) (Inic et al. Citation2014; Provenzano et al. Citation2018; Yin et al. Citation2020). Significant differences are available in the tumour characteristics, demographic data, and survival of the patients based on these subtypes, which have been described for all combined BC stages in the presence of stratification by St. Gallen risk categories (Parise et al. Citation2009). Among these subtypes, TNBC has tended to behave more aggressively than other types of BC. Unlike the other breast cancer subtypes, there are no approved targeted treatment options available nowadays, despite the utilisation of immunotherapy for those with advanced TNBC expressing programmed cell death ligand 1 (PD-L1) (Núñez Abad et al. Citation2022). These all confirmed that the PR-, ER- and HER2--negative may be related to a poor prognosis among the BC patients. In this study, PR-, ER- and HER2-negative was adopted in the nomogram for predicting OS among BC patients, which was approved to be effective for predicting the BC mortality.
There are really some limitations in our study. Our study shows a lack of an external cohort. Therefore, in the future, external cohort is required to validate our proposed nomogram. We could not include all the potential prognostic factors into the nomogram. On this basis, we cannot make predictions that are absolutely accurate. Nevertheless, the validation data demonstrated good fitness of the present nomogram, which confirmed the efficiency of the established nomograms. Finally, we did not integrate the other markers such as PDL-1 (Azim et al. Citation2022) with prognostic impact into the nomogram. In the future, we will collect more data and integrate more markers with prognostic impacts.
Conclusions
We proposed a nomogram based on ALDH1, p-AKT, and pathological stage for predicting the DFS of BC, together with a nomogram based on ALDH1, p-AKT, pathological stage and ER-/PR-/HER2- for predicting OS among BC patients. Kaplan-Meier curve and Log-rank test on the 3-yr and 5-yr DFS and OS analysis validated the efficiency of risk stratification based on the nomogram.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Shanghai Fourth People’s Hospital, School of Medicine, Tongji University (2020053-001). Informed consent was obtained from all individual participants included in the study.
Authors’ contribution
LY: study design, conceptualisation, project administration and supervision; JS: study design, conceptualisation, project administration and supervision, editing the original draft; LZ: data curation, formal analysis, investigation, methodology, writing the original draft; LB: data curation, formal analysis, investigation, methodology; HZ: investigation, methodology, writing the original draft; CG: data curation, formal analysis; SL: editing the draft.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Additional information
Funding
References
- Arcaro, A. and Guerreiro, A. S., 2007. The phosphoinositide 3-kinase pathway in human cancer: genetic alterations and therapeutic implications. Curr Genomics, 8 (5), 1–8.
- Azim, H. A., et al., 2022. Programmed death-ligand 1 (pd-l1) expression predicts response to neoadjuvant chemotherapy in triple-negative breast cancer: a systematic review and meta-analysis. Biomarkers: biochemical Indicators of Exposure, Response, and Susceptibility to Chemicals, 27 (8), 764–772.
- Burguin, A., Diorio, C. and Durocher, F., 2021. Breast cancer treatments: updates and new challenges. J Pers Med, 11 (8), 808.
- Chen, C. J., et al., 2022. Correlation of er, pr, and her2 at the protein and mrna levels in asian patients with operable breast cancer. Bioscience Reports., 42 (1), BSR20211706.
- Gold, J. S., et al., 2009. Development and validation of a prognostic nomogram for recurrence-free survival after complete surgical resection of localised primary gastrointestinal stromal tumour: a retrospective analysis. Lancet Oncology., 10 (11), 1045–1052.
- Han, S., et al., 2019. Prognostic value of aldh1 and nestin in advanced cancer: a systematic meta-analysis with trial sequential analysis. Therapeutic Advances in Medical Oncology, 11, 1758835919830831.
- Inic, Z., et al., 2014. Difference between luminal a and luminal b subtypes according to ki-67, tumor size, and progesterone receptor negativity providing prognostic information. Clinical Medicine Insights. Oncology, 8, 107–111.
- Khoury, T., et al., 2012. Aldehyde dehydrogenase 1a1 expression in breast cancer is associated with stage, triple negativity, and outcome to neoadjuvant chemotherapy. Modern Pathology., 25 (3), 388–397.
- Liu, R., et al., 2020. Pi3k/akt pathway as a key link modulates the multidrug resistance of cancers. Cell Death & Disease, 11 (9), 797.
- Łukasiewicz, S., et al., 2021. Breast cancer-epidemiology, risk factors, classification, prognostic markers, and current treatment strategies-an updated review. Cancers, 13 (17), 4287.
- Miller, K. D., et al., 2022. Cancer treatment and survivorship statistics. CA Cancer J Clin, 72 (5), 409–436.
- Miricescu, D., et al., 2020. Pi3k/akt/mtor signaling pathway in breast cancer: From molecular landscape to clinical aspects. International Journal of Molecular Sciences., 22 (1), 173.
- Núñez Abad, M., et al., 2022. Programmed death-ligand 1 (pd-l1) as immunotherapy biomarker in breast cancer. Cancers, 14 (2), 307.
- Ozaki, A., et al., 2022. High expression of p62 and aldh1a3 is associated with poor prognosis in luminal b breast cancer. Anticancer Research, 42 (7), 3299–3312.
- Panigoro, S. S., et al., 2020. Aldh1 cancer stem cell marker as a prognostic factor in triple-negative breast cancer. International Journal of Surgical Oncology, 2020, 7863243.
- Parise, C. A., et al., 2009. Breast cancer subtypes as defined by the estrogen receptor (er), progesterone receptor (pr), and the human epidermal growth factor receptor 2 (her2) among women with invasive breast cancer in california, 1999-2004. The Breast Journal, 15 (6), 593–602.
- Plichta, J. K., et al., 2019. Clinical and pathological stage discordance among 433,514 breast cancer patients. Am J Surg, 218 (4), 669–676.
- Provenzano, E., Ulaner, G. A. and Chin, S. F., 2018. Molecular classification of breast cancer. PET Clinics, 13 (3), 325–338.
- Rascio, F., et al., 2021. The pathogenic role of pi3k/akt pathway in cancer onset and drug resistance: an updated review. Cancers, 13 (16), 3949.
- Roudier, E., Mistafa, O. and Stenius, U., 2006. Statins induce mammalian target of rapamycin (mtor)-mediated inhibition of akt signaling and sensitize p53-deficient cells to cytostatic drugs. Molecular Cancer Therapeutics, 5 (11), 2706–2715.
- Saba, T. M. and Jaffe, E., 1980. Plasma fibronectin (opsonic glycoprotein): Its synthesis by vascular endothelial cells and role in cardiopulmonary integrity after trauma as related to reticuloendothelial function. The American Journal of Medicine, 68 (4), 577–594.
- Shariati, M. and Meric-Bernstam, F., 2019. Targeting akt for cancer therapy. Expert Opin Investig Drugs, 28 (11), 977–988.
- Siegel, R. L., et al., 2021. Cancer statistics, 2021. CA: a Cancer Journal for Clinicians, 72 (1), 7–33.
- Tokunaga, E., et al., 2006. Akt is frequently activated in her2/neu-positive breast cancers and associated with poor prognosis among hormone-treated patients. International Journal of Cancer., 118 (2), 284–289.
- Trayes, K. P. and Cokenakes, S. E. H., 2021. Breast cancer treatment. Am Fam Physician, 104 (2), 171–178.
- Yin, L., et al., 2020. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Research, 22 (1), 61.
- Yu, P., et al., 2010. Prognostic relevance of aldh1 in breast cancer: a clinicopathological study of 96 cases. The Chinese-German Journal of Clinical Oncology, 9 (1), 31–35.
- Zhang, C., Zhao, S. and Wang, X., 2022. Prognostic nomogram for early gastric cancer after surgery to assist decision-making for treatment with adjuvant chemotherapy. Frontiers in Pharmacology, 13, 845313.
- Zhou, L., et al., 2013. Molecular markers of therapeutic resistance in breast cancer. Human Pathology., 44 (7), 1421–1428.
- Zhou, L., et al., 2018. Expression of pakt is associated with a poor prognosis in Chinese women with invasive ductal breast cancer. Oncology Letters, 15 (4), 4859–4866.