

Abstract
Background
Adolescent pregnancy is defined as pregnancy occurring in young women between the ages of 10 and 19 years. Adolescent pregnancies, which are among the social healthcare concerns in developed and developing countries, have negative effects on maternal and infant health. Pregnancy in adolescence puts the health of both the mother and child at risk, as adolescent pregnancies have higher rates of eclampsia, systemic infection, low birth weight, and preterm delivery compared to other pregnancies. In this study, the effects of education level, smoking, and marital status on maternal and foetal outcomes in adolescent pregnancies were evaluated.
Methods
The records of a total of 960 pregnant women (480 pregnant adolescents aged 15–19 years and 480 pregnant adult women aged 20–26 years) were examined retrospectively. The demographic data of the groups and maternal and foetal outcomes of the pregnancies were compared. A logistic regression model was established as a statistical method for reducing confounding effects.
Results
Unmarried women were statistically significantly more prevalent in the adolescent group (38.3% vs. 7.3%). Among the considered risk factors, preeclampsia (2.9% vs. 0.8%) and smoking (29.8% vs. 9.8%) were statistically significantly more common in the adolescent group. When the groups were compared in terms of risk factors in pregnancy, it was found that pregnancy in adolescence was associated with a 3.04-fold higher risk of smoking, 5.25-fold higher risk of being unmarried, 3.50-fold higher risk of preeclampsia, and 1.70-fold higher risk of intrauterine growth retardation (IUGR).
Conclusions
This study demonstrates an increased risk of preeclampsia, IUGR, and smoking during pregnancy in adolescent pregnant women. These findings can be used to identify adolescent pregnancies requiring specific assistance and to take measures to reduce the probability of adverse outcomes.
PLAIN LANGUAGE SUMMARY
In this study, we examine the risks of adolescent pregnancies. Adolescent pregnancy is a public health problem, and it is more common in underdeveloped or developing countries. We believe that non-governmental organisations and governments should take precautions regarding adolescent pregnancies and protect this legally vulnerable sociodemographic group from pregnancy. For healthier and more conscientious pregnancy experiences, mothers must be of appropriate age, having passed the period of adolescence. Adolescent pregnancies, which come with many risks, and especially risks of preeclampsia, premature birth, and maternal death, should be minimised or prevented.
Introduction
Adolescence is defined as the transition from childhood to adulthood and it involves processes of psychological and social changes. Adolescent pregnancy is recognised as a public healthcare concern by the World Health Organisation (WHO) because of its psychosocial impacts on the health of both the mother and child (Flores Valencia et al. Citation2017). According to the WHO, 21 million adolescent pregnancies occurred annually in developing countries as of 2019, 50% of which were unwanted and 12 million of which resulted in the mother giving birth (World Health Organization Citation2023). There are increased risks of preterm birth, gestational diabetes, intrauterine growth retardation (IUGR), low-birth-weight babies, pregnancy-induced hypertension, and preterm premature rupture of membranes in cases of adolescent pregnancies (Malabarey et al. Citation2012; Traisrisilp et al. Citation2015). Preterm birth is commonly defined as any birth before the completion of 37 weeks of gestation (Quinn et al. Citation2016). Although the rates of pregnancy in adolescence are decreasing with each passing year on a global scale, there are regional differences in the rates of change. Overall, adolescent pregnancies decreased globally from 64.5 per 1000 women in 2000 to 42.5 per 1000 women in 2021. However, although the estimated adolescent birth rate is declining, the number of births continues to increase (Diabelková et al. Citation2023). It is important to understand the maternal and foetal risks of adolescent pregnancies to help prevent or reduce the number of adolescent pregnancies. The present study was conducted with the aim of identifying the risk factors experienced by adolescent pregnant women with evidence-based data by comparing the peripartum outcomes of adolescent pregnant women with those of a control group of pregnant adult women.
Methods
The study was conducted in rural areas in the Southeastern Anatolian region of Turkey, covering the period between January 2016 and November 2022. A population-based cross-sectional study was conducted in a single centre with data retrospectively collected from hospital records. The records of pregnant women were evaluated retrospectively. Using the G*Power program, it was concluded that 385 women should be analysed in the study group for a 94% confidence interval and 470 or more should be analysed for a 95% confidence interval. Thus, the study group included 480 pregnant adolescents. The control group was selected to be equal in size, including 480 pregnant women aged 20–26 years. The demographic data of the groups (maternal age at birth, marital status, smoking history, and education level) and maternal and foetal outcomes (delivery type, gestational week at birth, birth weight, 5-minute Apgar scores, preterm labour, preeclampsia, and IUGR) were compared. Maternal age was defined as the mother’s age at the time of the birth. All patients included in the study had singleton pregnancies and were between the ages of 15 and 26 years. Smoking one or more cigarettes per day was considered as a smoking habit. When education levels were evaluated, four groupings were made, including those who had never attended school or had not completed primary education, those who had completed primary education, those who had completed high school, and those who had education at the university level or beyond. Foetal weight below the tenth percentile according to gestational week was accepted as IUGR and the 24th gestational week was accepted as the limit of viability. Patients with non-viable pregnancies (<24 weeks), multiple pregnancies, and chronic diseases were excluded from the study. The study was conducted in line with the principles of the Declaration of Helsinki as revised in Brazil in 2013 (World Medical Association Declaration of Helsinki, 2013). Ethics committee approval was received on 06.01.2023 with Number E-68051626-949-206470075.
Statistical analysis
The conformity of the data to normal distribution was evaluated with kurtosis and skewness values. Mean ± standard deviation values were calculated for the data. Independent variables were evaluated with logistic regression as binary variables. Student’s t-test was used for parametric variables with normal distribution and the Mann-Whitney U test was used for those without normal distribution. A logistic regression model was established as a statistical method for reducing confounding factors. The chi-square test was used for categorical variables. Statistical evaluations were performed with IBM SPSS Statistics 25.0 (IBM Corp., Armonk, NY, USA) and the significance level was taken as p < 0.05 ().
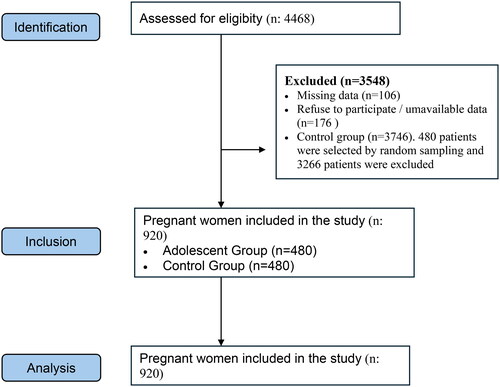
Figure 1. Strengthening the reporting of observational studies in epidemiology (STROBE).
Flow diagram of patients recruitment.
Results
A total of 480 pregnant adolescents between the ages of 15 and 19 years and 480 pregnant adult women between the ages of 20 and 26 years were included in this study. According to the demographic data, the mean age of the pregnant adolescents was 17.28 ± 1.14 years, while the mean age of the women in the control group was 23.16 ± 1.85 years. Rates of smoking (9.8% vs. 29.8%) and being unmarried (38.3% vs. 7.3%) were higher among the adolescents compared to the control group. Individuals who did not complete primary school or received no education were grouped together with primary school graduates, with the other educational categories including high school graduates and university graduates. For each of these categories, the rates were higher in the control group ().
Table 1. Demographic data of pregnant adolescents and the control group with comparisons of education level, marital status, and smoking by groups.
APGAR scores were evaluated using binary logistic regression and were found to be similar between the groups (). In terms of maternal and foetal outcomes, gestational age at birth, birth weight, and preterm labour rates were found to be similar between the groups. The number of caesarean deliveries was lower at 106 (22.1%) in the adolescent group compared to 135 (28.1%) in the control group (p = 0.03). The rate of preeclampsia was significantly higher in cases of adolescent pregnancies at 14 (2.9%) versus 4 (0.8%). The rate of IUGR was also significantly higher in adolescent pregnancies at 51 (10.6%) versus 30 (6.3%) ().
Table 2. Infants’ APGAR scores measured at the 5th minute after birth were similar between the groups.
Table 3. Maternal and foetal outcomes of pregnant adolescents and the control group.
Compared to the control group, pregnant adolescents had 3-fold higher risk of smoking during pregnancy (OR: 3.04; 95% CI: 2.24–4.12; p < 0.001), 3.5-fold higher risk of preeclampsia (OR: 3.50; 95% CI: 1.16–10.5; p < 0.017), 5.25-fold higher risk of being unmarried (OR: 5.25; 95% CI: 3.74–7.37; p < 0.001), and 1.70-fold higher risk of IUGR (OR: 1.70; 95% CI: 1.10–2.62; p < 0.015) ().
Table 4. Risk levels of pregnant adolescents in terms of adverse pregnancy outcomes and conditions.
Discussion
Adolescent pregnancies come to the forefront as a matter of debate and an important healthcare concern in the fields of public health and obstetrics (Chandra-Mouli et al. Citation2013). Several previous studies have demonstrated that adolescent pregnancies have negative effects for both maternal and infant health (Thato et al. Citation2007). The WHO reported that 50% of adolescent pregnancies are unintended pregnancies with high levels of risk (World Health Organization Citation2023). The present study was conducted in a city in the region with the highest fertility rate (2.78%) in Turkey. The sociodemographic risk factors that are known to be more common among pregnant adolescents include poverty, low education levels, inadequate prenatal care, and being unmarried (Gortzak-Uzan et al. Citation2001; Chen et al. Citation2007). In the present study, similar to previous studies, due to the sociocultural structure of the region, adolescent pregnancy was found to be associated with a 5.25-fold increase in the risk of being unmarried. There is also a close relationship between adolescent pregnancy and education level. In this study, the level of education in cases of adolescent pregnancy was found to be significantly lower at all considered levels (i.e. having never studied or completed primary education, having completed primary education, having completed high school, and having completed university or higher education). In a study that analysed the data of 3.8 million pregnant women, Chen et al. concluded that as the age of adolescent mothers decreased, the week of delivery decreased (Chen et al. Citation2007). In the present study, however, it was found that gestational age at birth and the risk of preterm birth were similar between the groups. In their study conducted with 711 pregnant adolescents with a mean age of 17.8 years, Demir et al. concluded that birth weight did not differ among mothers in adolescence (Demir et al. Citation2011). No significant differences were detected in birth weight in the present study between the two groups, which supports the previous result. In their study conducted in 2020, Wong et al. found that 5-minute APGAR scores were low at birth in cases of adolescent pregnancy (Wong et al. Citation2020). No differences were detected in the present study between the groups in terms of 5-minute APGAR scores, similar to the findings of two different hospital-based studies (Jolly Citation2000; Conde-Agudelo et al. Citation2005). Studies speculating that the rate of caesarean section delivery is lower among adolescent mothers are predominant (Hediger et al. Citation1997; Lao & Ho Citation1997; Al-Ramahi & Saleh Citation2006). In the present study, the caesarean section rate was found to be lower in the adolescent group (22.1%) compared to the control group (28.1%) (p = 0.03), similar to previous studies. It was speculated by Karai et al. that the rate of preeclampsia was higher in adolescent pregnancies, although the obtained difference was not statistically significant, and Rexhapi et al. reported similar findings in the same year (Karai et al. Citation2019; Rexhepi et al. Citation2019). In the present study, the risk of preeclampsia was increased 3.5-fold in adolescence, which is consistent with the data in the literature. In a meta-analysis of 38 full-text articles reporting studies conducted in Turkey with a total of 80,249 patients (adolescents: 20,768; controls: 59,481) to compare adolescent and adult pregnancies and outcomes for maternal and infant health, it was concluded that the risk of IUGR is higher in cases of adolescent pregnancies (Karaçam et al. Citation2021). Similarly, in the present study, the risk of IUGR was 1.7 times higher in adolescent pregnancies. Furthermore, it is known that adolescents are more likely to smoke and consume alcohol during pregnancy than women of older ages and that smoking and/or alcohol consumption has significant effects on the health of both pregnant adolescents and their foetuses (Bottorff et al. Citation2014). Jain et al. found that the probability of adolescent mothers smoking during pregnancy was double that of women aged 20–35 in Canada (Jain et al. Citation2018). In the present study, it was found that there was a 3.04-fold increase in the likelihood of smoking during pregnancy among adolescent pregnant women.
Conclusion
Adolescent pregnancy is a concern in terms of not only the infant’s health but also the health of society as a whole, especially on the level of families. There are increased maternal and foetal risks in cases of adolescent pregnancies. It is clear that the role of motherhood, suitable only for adults, is not appropriate for individuals who become pregnant in adolescence, when they have not yet completed their physical development and still have childhood characteristics. Furthermore, expecting a person who is still a child herself to be a mother to another child is asking for a greater sacrifice than can realistically be made. The probability of having a healthy pregnancy is lower and antenatal follow-up care is insufficient in adolescent pregnancies compared to pregnant adult women. The first and most important approach to adolescent pregnancies must be preventing them. In situations where they cannot be prevented, the detection of adolescent pregnancies and the initiation of antenatal care as soon as possible, the participation of pregnant women in antenatal care visits as often as possible, and the proper planning of delivery are important requirements for maternal and infant health.
Authors’ contributions
All the authors have accepted responsibility for the entire content of this submitted manuscript and approved its submission.
Informed consent
Informed consent was obtained from all study participants.
Acknowledgements
We express our gratitude to all the participants who contributed to this study.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Additional information
Funding
References
- Al-Ramahi, M. and Saleh, S., 2006. Outcome of adolescent pregnancy at a university hospital in Jordan. Archives of Gynecology and Obstetrics, 273 (4), 1–6.
- Bottorff, J. L., et al., 2014. Tobacco and alcohol use in the context of adolescent pregnancy and postpartum: a scoping review of the literature. Health & Social Care in the Community, 22 (6), 561–574.
- Chandra-Mouli, V., Camacho, A. V. and Michaud, P.-A., 2013. WHO guidelines on preventing early pregnancy and poor reproductive outcomes among adolescents in developing countries. The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 52 (5), 517–522.
- Chen, X.-K., et al., 2007. Teenage pregnancy and adverse birth outcomes: a large population based retrospective cohort study. International Journal of Epidemiology, 36 (2), 368–373.
- Conde-Agudelo, A., Belizán, J. M. and Lammers, C., 2005. Maternal-perinatal morbidity and mortality associated with adolescent pregnancy in Latin America: Cross-sectional study. American Journal of Obstetrics and Gynecology, 192 (2), 342–349.
- Demir, B., et al., 2011. Evaluation of adolescent pregnancies: 10-year experience of a hospital in rural Turkey.
- Diabelková, J., et al., 2023. Adolescent pregnancy outcomes and risk factors. International Journal of Environmental Research and Public Health, 20 (5), 4113.
- Flores Valencia, M. E., Nava-Chapa, G. and Arenas-Monreal, L., 2017. Embarazo en la adolescencia en una región de México: un problema de Salud Pública. Revista de Salud Pública, 19 (3), 374–378.
- Gortzak-Uzan, L., et al., 2001. Teenage pregnancy: risk factors for adverse perinatal outcome. The Journal of Maternal-Fetal Medicine, 10 (6), 393–397.
- Hediger, M. L., et al., 1997. Young maternal age and preterm labor. Annals of Epidemiology, 7 (6), 400–406.
- Jain, L. H., et al., 2018. Characteristics and outcomes of adolescent births in Nova Scotia: a retrospective cohort study. Journal of Obstetrics and Gynaecology Canada, 40 (11), 1459–1465.
- Jolly, M., 2000. Obstetric risks of pregnancy in women less than 18 years old. Obstetrics & Gynecology, 96 (6), 962–966.
- Karaçam, Z., Kizilca Çakaloz, D. and Demir, R., 2021. The impact of adolescent pregnancy on maternal and infant health in Turkey: systematic review and meta-analysis. Journal of Gynecology Obstetrics and Human Reproduction, 50 (4), 102093.
- Karai, A., et al., 2019. Adverse perinatal outcome in teenage pregnancies: an analysis of a 5-year period in Southeastern Hungary. The Journal of Maternal-Fetal & Neonatal Medicine, 32 (14), 2376–2379.
- Lao, T. T. and Ho, L. F., 1997. The obstetric implications of teenage pregnancy. Human Reproduction (Oxford, England), 12 (10), 2303–2305.
- Malabarey, O. T., et al., 2012. Pregnancies in young adolescent mothers: a population-based study on 37 million births. Journal of Pediatric and Adolescent Gynecology, 25 (2), 98–102.
- Quinn, J.-A., et al., 2016. Preterm birth: Case definition & guidelines for data collection, analysis, and presentation of immunisation safety data. Vaccine, 34 (49), 6047–6056.
- Rexhepi, M., et al., 2019. Hospital-based study of maternal, perinatal and neonatal outcomes in adolescent pregnancy compared to adult women pregnancy. Open Access Macedonian Journal of Medical Sciences, 7 (5), 760–766.
- Thato, S., Rachukul, S. and Sopajaree, C., 2007. Obstetrics and perinatal outcomes of Thai pregnant adolescents: a retrospective study. International Journal of Nursing Studies, 44 (7), 1158–1164.
- Traisrisilp, K., et al., 2015. Pregnancy outcomes among mothers aged 15 years or less. The Journal of Obstetrics and Gynaecology Research, 41 (11), 1726–1731.
- Wong, S. P. W., et al., 2020. Risk factors and birth outcomes associated with teenage pregnancy: a Canadian sample. Journal of Pediatric and Adolescent Gynecology, 33 (2), 153–159.
- World Health Organization. 2023. WHO 2023. Guide to citing Internet sources [online]. September 1. Available from: https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnan# [1 September 2023]. Adolescent Pregnancy. https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnan#