

Abstract
Background
The relationship between amniotic fluid inflammatory biomarkers and preterm birth in second- or third-trimester pregnancy has been a focus, and understanding the correlation between these markers and preterm birth is important for early identification and intervention in preterm birth. The aim of this study was to explore potential inflammatory biomarkers in second- or third-trimester pregnancy amniotic fluid associated with preterm birth.
Methods
On November 30, 2023, we searched literature involved the influence of second- or third-trimester pregnancy amniotic fluid inflammatory biomarkers on preterm birth through PubMed, Web of Science, Embase, Scope, CNKI, WanFang, VIP and China Biomedical Databases. The search languages were Chinese and English. Included outcomes indexes were combined utility analysis via R software.
Results
A total of 11 articles were included in the combined utility analysis. This combined analysis revealed significant differences in several inflammatory biomarkers in amniotic fluid between the two groups (MD = 6.87, 95%CI: 0.26 − 13.47, P < 0.01); the difference in amniotic fluid IL-6 between the two groups (MD = 5.73, 95%CI: 3.13–8.32, P < 0.01); the difference in amniotic fluid IL-10 between the two groups (MD = 0.11, 95%CI: −3.26–3.48, P < 0.01); the difference in amniotic fluid CRP between the two groups (MD = 21.34, 95%CI: 11.69–30.89, P < 0.01); the difference in amniotic fluid MCP-1 between the two groups (MD = 312.14, 95%CI: 211.34–412.97, P < 0.01); the difference in the amniotic fluid MMP-9 between the two groups (MD = 0.86, 95%CI: −0.10–1.82, P < 0.01); and the difference in TNF-α in amniotic fluid between the two groups (MD = 22.78, 95%CI: −5.05–50.61, P < 0.01).
Conclusions
The inflammatory biomarkers IL-1β, IL-6, IL-10, CRP, TNFα, MCP-1 and MMP-9 in the amniotic fluid of patients in the second- or third-trimester pregnancy were all correlated with preterm birth.
PLAIN LANGUAGE SUMMARY
The premature foetus has many serious complications in the near and long term because of the immature organs, which is related to the long-term incidence of cerebral palsy, developmental delay and retinopathy of prematurity, which is the main cause of perinatal foetal death. Preterm birth cases are accompanied by infection of pathogenic microorganisms in amniotic cavity, which then leads to inflammatory reaction in amniotic cavity. However, research on the correlation between inflammatory markers and preterm birth has shown certain complexity and differences. The results of this meta-analysis show that the inflammatory biomarkers interleukin-1 beta (IL-1β), interleukin-6 (IL-6) and interleukin-10 (IL-10), C-reactive protein (CRP), tumour necrosis factor-alpha (TNF-α), monocyte chemoattractant protein-1 (MCP-1) and matrix metalloproteinase-9 (MMP-9) in amniotic fluid of patients in the second- or third-trimester pregnancy are significant between the preterm birth group and the control group, and the expression level of inflammatory factors in amniotic fluid of patients in the preterm birth group is elevated, thus suggesting that these inflammatory factors may be able to predict preterm birth.
Introduction
Preterm birth is defined as delivery before 37 completed weeks of gestation (Tambor et al. Citation2015; Wu and Zhou Citation2019). With the development of perinatal medicine, there is an increasing awareness of risk factors and underlying mechanisms associated with preterm birth. However, in developed countries the preterm birth rate is still 5% to 9%, even in the United States, the incidence of preterm birth is still more than 10% (Tambor et al. Citation2015; Vogel et al. Citation2018). Preterm infants are at risk of numerous short- and long-term complications owing to the immaturity of several organs, including but not limited to cerebral palsy, developmental delays and retinopathy of prematurity, which are closely related to the long-term morbidity of up to 75% of preterm infants, and are a major cause of perinatal infant mortality (Goldenberg et al. Citation2008; Yoneda et al. Citation2011). There are numerous factors that contribute to preterm birth, but many studies have identified infection as one of the leading factors. Tambor et al. found that nearly 50% of preterm birth were associated with an intra-amniotic microbial infection that triggered an inflammatory response in the amniotic cavity (Tambor et al. Citation2015). In addition, inflammatory makers in amniotic fluid may predict preterm birth. For example, when the level of interleukin 8 (IL-8) in the amniotic fluid is ≥ 25.5 ng/mL, the accuracy of predicting delivery within 3 days reaches 80.9% (Yoneda et al. Citation2011). In some cases, preterm birth may result from asymptomatic intrauterine infections early in pregnancy, when microbial invasion is present and leads to increased expression of pro-inflammatory cytokines and chemokines (Wenstrom et al. Citation1998; Borna et al. Citation2009). This inflammatory response triggered by microbial invasion, especially in the amniotic cavity, is thought to be one of the key mechanisms leading to preterm birth (Goldenberg et al. Citation2000). However, the correlation between inflammatory biomarkers and preterm birth presents complexity and variability across studies. Although the majority of studies support the association of certain inflammatory markers, such as monocyte chemoattractant protein-1 (MCP-1), matrix metalloproteinase-9 (MMP-9), C-reactive protein (CRP) and various interleukins (e.g. interleukin-1 beta (IL-1β), interleukin-6 (IL-6) and interleukin-10 (IL-10)) with an increased risk of preterm birth, there is controversy over the role of tumour necrosis factor-alpha (TNF-α) in preterm birth (La Sala et al. Citation2012). Therefore, this study aims to analyse, through a meta-analysis, the association between inflammatory biomarkers including monocyte chemoattractant protein-1 (MCP-1), matrix metalloproteinase (MMP-9), C reactive protein (CRP), IL-1β, IL-6, IL-10 and TNF-α inflammatory biomarkers and preterm birth from the perspective of meta-analysis, in order to resolve the disagreement among the existing studies, and to help us better understand the pathophysiological process of preterm birth, which may also reveal new therapeutic targets and provide new strategies to reduce the rate of preterm birth.
Methods
Literature search
Computer searched literature through PubMed, Web of Science, Embase, Scope, CNKI, WanFang, VIP and China Biomedical Databases. The protocol for this review was registered with PROSPERO (number: CRD42024531338). The keywords used for the search were ‘preterm birth’, ‘premature rupture of membranes’, ‘cytokines’, ‘amniotic fluid’, ‘intra-amniotic’, ‘cytokines’, ‘second- or third-trimester pregnancy’, and so on. The literature search time was from the establishment of each database to 24th October 2022. The search language was restricted to Chinese and English, and the search strategy was based on PubMed as shown below:
#1 preterm birth OR premature rupture of membranes [Title/Abstract]
#2 amniotic fluid OR intra-amniotic [Title/Abstract]
#3 cytokines OR cytokines [Title/Abstract]
#4 second- or third-trimester pregnancy [Title/Abstract]
#5 #1 AND #2 AND #3 AND #4
Inclusion criteria
(1) Study objects: patients in second- or third-trimester pregnancy, regardless of age and gravidity; (2) Study types: cohort study or randomised controlled study; (3) Grouping: preterm birth group and full-term delivery group; (4) The outcome indicators included IL-1β, IL-6, IL-10, CRP, TNFα, MCP-1, and MMP-9.
Exclusion criteria
(1) Articles published in Chinese or English; (2) The subjects were animals; (3) Cases of twin or multiple pregnancies; (4) Review, news, review, meta-analysis and other types of articles; (5) The data included in the outcome indicators were incomplete or the data could not be entered; (6) Literature on the known presence of infections during pregnancy, particularly chorioamnionitis; (7) Cases of preterm birth due to infections that have not been explicitly excluded from the literature.
Literature data extraction
The data were extracted by two researchers. And the extracted data types included study authors, publication time, study area, number of patients, age, and gestational age of patients.
Quality assessment
The Newcastle-Ottawa Scale (NOS) score was used to evaluate the literature quality of the included literature. The NOS score above 7 was high-quality literature, and 5–7 was classified as medium-quality literature.
Outcome indicators
The outcome measures were selected as inflammatory biomarkers, including IL-1β, IL-6, IL-10, MMP-9, CRP, TNF-α and MCP-1.
Statistical analysis
R 4.2.1 software was used for meta-analysis of the outcome indicators. The data types analysed in this study were continuous variables, with the effect size represented by the mean difference (MD) and 95% confidence interval (CI). The heterogeneity test value P and I2 value were used to test the Na. When I2 > 50%, indicating substantial heterogeneity among the included studies, a random-effects model was employed for the analysis. Publication bias test was performed by Egger’s and Begg’s test, P > 0.05, there was no publication bias in the included literature, and P < 0.05 in the combined effect size analysis was statistically significant.
Results
Literature search results
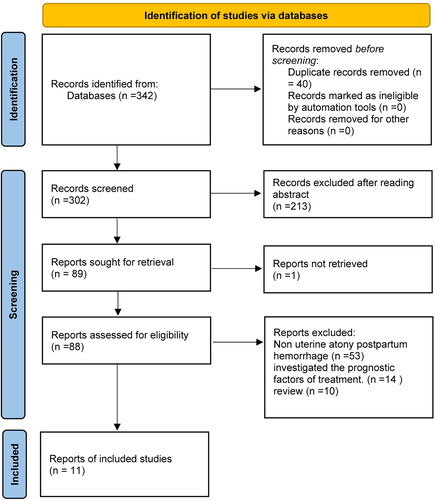
The literature search was carried out according to the established inclusion and exclusion criteria, and a total of 11 literatures were finally included after screening, including 2 Chinese articles (Yang et al. Citation2016; Han Huijie et al. Citation2022), and 9 English articles (Wenstrom et al. Citation1998; Ghezzi et al. Citation2002; Puchner et al. Citation2011; Oh et al. Citation2011; La Sala et al. Citation2012; Cobo et al. Citation2012; Son et al. Citation2016; Musilova et al. Citation2018; Kim et al. Citation2022), as shown in .
Figure 1. Flow diagram of literature search and selection criteria.
Basic characteristics of included articles
A total of 11 articles include ≥ 1 outcome indexes were included in this study (Wenstrom et al. Citation1998; Ghezzi et al. Citation2002; Oh et al. Citation2011; Puchner et al. Citation2011; Cobo et al. Citation2012; La Sala et al. Citation2012; Yang et al. Citation2016; Son et al. Citation2016; Musilova et al. Citation2018; Han Huijie et al. Citation2022; Kim et al. Citation2022). Among them, the outcome indicators included IL-1β in 4 articles; IL-6 in 8 articles; IL-10 in 5 articles; TNF-α in 5 articles, MCP-1 in 5 articles; CRP in 4 articles; and MMP-9 in 4 articles (see ).
Table 1. Summary of descriptive characteristics of included articles.
Evaluation of literature quality
According to NOS score to evaluate the literature quality, there were 3 medium-quality literatures and 8 high-quality literatures. The detailed results are shown in .
Table 2. Evaluation of literature quality.
Synthesis of results from the meta-analysis
The relationship between amniotic fluid IL-1β and preterm birth
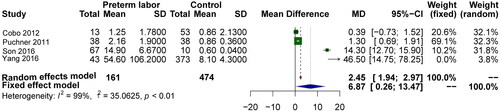
This part includes 4 articles. The effect of IL-1β level in amniotic fluid of preterm group and control group in second- or third-trimester pregnancy. Heterogeneity analysis found that I2=99%, and a random model was used for meta-analysis, as shown in . The combined effect size results showed that there was a significant difference in IL-1β (MD = 6.87, 95%CI: 0.26 to 13.47, P < 0.01; ), indicating that the increase in amniotic fluid IL-1β in the second- or third-trimester pregnancy is associated with preterm birth. Risk of bias test analysis results Begg’s test (Z = 1.36, P = 0.17), Egger’s (t = 0.92, P = 0.17), there may be publication bias among the included literatures.
Figure 2. Forest plot of the relationship between amniotic fluid IL-1β and preterm birth.
The relationship between amniotic fluid IL-6 and preterm birth
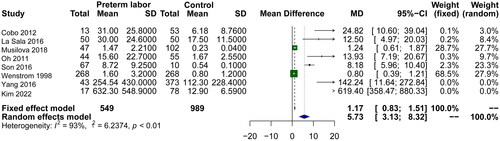
Eight articles reported the effect of IL-6 levels in amniotic fluid of preterm and control patients in the second- or third-trimester pregnancy. Heterogeneity analysis found that I2=93%, randomised model was used for meta-analysis, as shown in . The analysis results of the combined effect size showed that there was a significant difference in IL-6 in amniotic fluid between the two groups (MD = 5.73, 95%CI: 3.13–8.32, P < 0.01; ), that is, the increase of IL-6 in amniotic fluid in the second- or third-trimester pregnancy was related to the preterm birth. The results of bias risk test were Begg’s test (Z = 0.99, P = 0.32) and Egger’s test (t = 5.80, P = 0.001). There may be publication bias among the included studies.
Figure 3. Forest plot of the relationship between amniotic fluid IL-6 and preterm birth.
The relationship between amniotic fluid IL-10 and preterm birth
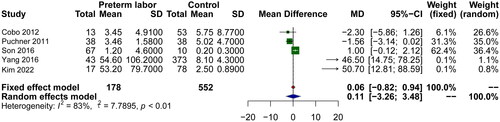
Five literatures reported the effect of IL-10 levels in amniotic fluid of preterm and control groups in the second- or third-trimester pregnancy. Heterogeneity analysis found that I2=83%. A random model was used for meta-analysis, as shown in . The analysis results showed that the combined effect size showed that there was a significant difference in amniotic fluid IL-10 between the two groups of patients (MD = 0.11, 95%CI: −3.26–3.48, P < 0.01; ), that is, the increase of IL-10 in the amniotic fluid of patients in the second- or third-trimester pregnancy is related to the preterm birth. The risk of bias test analysis results was Begg’s test (Z = 0.49, P = 0.62), Egger’s (t = 1.06, P = 0.36), and there was no publication bias among the included studies.
Figure 4. Forest plot of the relationship between amniotic fluid IL-10 and preterm birth.
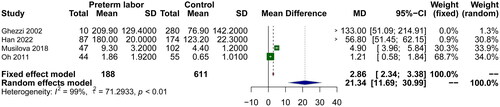
The relationship between amniotic fluid CRP and preterm birth
Four literatures reported the effect of CRP levels in the amniotic fluid of the preterm group and the control group in the second- or third-trimester pregnancy. Heterogeneity analysis found that I2 = 99%. A random model was used for meta-analysis, as shown in , the analysis results of the combined effect size showed that there was a significant difference in amniotic fluid CRP between the two groups (MD = 21.34, 95%CI: 11.69–30.89, P < 0.01; ). The increase of CRP in the amniotic fluid of patients in the second- or third-trimester pregnancy is related to the preterm birth. Risk of bias test analysis results Begg’s test (Z = 0.68, P = 1.00), Egger’s (t = 1.74, P = 0.23). There was no publication bias among the included studies.
Figure 5. Forest plot of the relationship between amniotic fluid CRP and preterm birth.
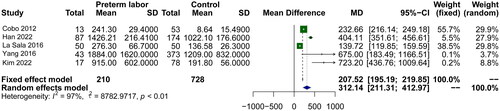
The relationship between amniotic fluid MCP-1 and preterm birth
There are 8 literatures that reported the effect of MCP-1 level in amniotic fluid of preterm group and control group in the second- or third-trimester pregnancy. Heterogeneity analysis found that I2=97%. A random model was used for meta-analysis, as shown in . The analysis results showed that the combined effect size showed that there was a significant difference in amniotic fluid MCP-1 between the two groups of patients (MD = 312.14, 95%CI: 211.31–412.97, P < 0.01; ), that is, the increase of MCP-1 in the amniotic fluid of patients in the second- or third-trimester pregnancy was associated with preterm birth. The results of the risk of bias test were analysed by Begg’s test (Z=-0.49, P = 0.62), Egger’s (t = 1.13, P = 0.34), there was no publication bias among the included studies.
Figure 6. Forest plot of the relationship between amniotic fluid MCP-1 and preterm birth.
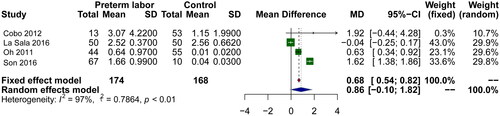
The relationship between amniotic fluid MMP-9 and preterm birth
Four literatures reported the effect of MMP-9 levels in the amniotic fluid of the preterm group and the control group in the second- or third-trimester pregnancy. Heterogeneity analysis found that I2=97%, and a random model was used for meta-analysis, as shown in . The analysis results showed that the combined effect size showed that there was a significant difference in amniotic fluid MMP-9 between the two groups of patients (MD = 0.86, 95%CI: −0.10–1.82, P < 0.01; ), that is, the increase of MMP-9in the amniotic fluid of patients in the second- or third-trimester pregnancy is related to the preterm birth. The risk of bias test analysis results was Begg’s test (Z = 0.68, P = 0.49), Egger’s (t = 0.26, P = 0.82), and there was no publication bias among the included studies.
Figure 7. Forest plot of the relationship between amniotic fluid MMP-9 and preterm birth.
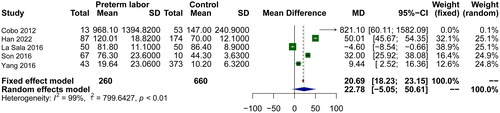
The relationship between amniotic fluid TNF-α and preterm birth
Five studies reported the effect of TNF-α levels in amniotic fluid of preterm and control groups during the second-or third-trimesters of pregnancy. Heterogeneity analysis revealed an I2 value of 99%, leading to the use of a random-effects model for the meta-analysis, as illustrated in . The analysis results showed that the combined effect size showed that there was a significant difference in amniotic fluid TNF-α between the two groups of patients (MD = 22.78, 95%CI: −5.05–50.61, P < 0.01; ), suggesting that an increase in TNF-α levels in the amniotic fluid during second- or third-trimester pregnancy is associated with preterm birth. Risk of bias was assessed using Begg’s test (Z = 0.00, P = 1.00) and Egger’s test (t = 0.27, P = 0.80), indicating no publication bias among the included studies.
Figure 8. Forest plot of the relationship between amniotic fluid TNF-α and preterm birth.
Discussion
Intra-amniotic infection is significantly associated with an increased risk of preterm birth, and levels of inflammatory biomarkers in amniotic fluid can directly reflect the inflammatory state of the uterine cavity (Kunze et al. Citation2016; Wu and Zhou Citation2019). Inflammatory biomarkers in amniotic fluid can directly reflect the state of intrauterine inflammation. Numerous studies have demonstrated that elevated levels of specific inflammatory biomarkers such as interleukin-1β (IL-1β), IL-6, IL-8, monocyte chemotactic protein-1 (MCP-1), and interferon gamma (IFN-γ) in amniotic fluid are significantly associated with preterm birth. For example, Cobo et al. found that inflammatory factors such as IL1β, IL-6, IL-8, MCP-1, and IFN-γ in the amniotic fluid of pregnant women increased, and the levels of IL-6 and IL-10 is the best factor for predicting preterm birth with ruptured membranes (Cobo et al. Citation2012). Amniotic fluid CRP concentration ≥110 ng/mL had a sensitivity of 80.8% and a specificity of 69.5% for predicting spontaneous preterm birth (Ghezzi et al. Citation2002), which proved that subclinical intrauterine or foetal inflammatory process in early pregnancy may be an important cause of preterm birth in late pregnancy. However, in iatrogenic preterm birth with more complex preterm birth factors, there were no correlation between inflammatory biomarkers in second-trimester amniotic fluid and preterm birth (Payne et al. Citation2014). We therefore excluded literature on iatrogenic preterm birth from our study. In another study, the analysis of inflammatory factors in amniotic fluid showed that the levels of IL-1α, IL-1β, IL-4, IL-6, IL-8, MCP-1, and IFN-γ were significantly different between preterm and term delivery women. While there was no significant difference in the levels of TNF-α, MMP-2, MMP-9 (La Sala et al. Citation2012). Although the relationship between inflammatory factors and preterm birth has been inflammatory in many studies, there seems to be some disagreement (La Sala et al. Citation2012; Son et al. Citation2016).
The present study critically screened and included 11 papers of moderate or higher quality, all of which were based on patients in second- or third-trimester pregnancy, to assess the correlation between inflammatory biomarkers in amniotic fluid and preterm birth. Although indications of publication bias were found when analysing IL-6 levels in amniotic fluid, with Begg’s test (Z = 0.99, P = 0.32) not showing significance and Egger’s test (t = 5.80, P = 0.001) pointing to possible bias, the results of the combined analyses nevertheless showed that IL-1β, IL-6, IL-10, CRP, TNF-α, MCP-1, and MMP-9, which are inflammatory biomarkers, were significantly different between the preterm and control groups, suggesting that they may have potential value in predicting preterm birth. Physiologically, the expression levels of these inflammatory biomarkers reflect the inflammatory state within the amniotic cavity, and the inflammatory environment of the amniotic cavity is closely related to the mechanisms of preterm birth. Specifically, IL-1β and IL-6 are early mediators of the inflammatory response in the uterine cavity, and they play a key role in activating immune cells in the uterine cavity and facilitating the transmission of inflammation (Cobo et al. Citation2012), whereas IL-10, as an anti-inflammatory cytokine, has a more complex role in pregnancy, which may be related to modulating the immune response and suppressing inflammation (Musilova et al. Citation2018). CRP is an acute phase protein whose elevated levels in vivo are usually associated with a state of systemic inflammation (La Sala et al. Citation2012). TNF-α is another core factor in the inflammatory process that induces the production of inflammatory cytokines and may directly affect the integrity of the foetal membranes (Son et al. Citation2016). MCP-1 is a chemokine that recruits monocytes to sites of inflammation, while MMP-9 is involved in the degradation of the foetal membranes, all of these mechanisms are closely related to the pathological processes involved in the development of preterm birth (Son et al. Citation2016), and these molecular changes are not only visible in the amniotic fluid, but may also affect the placental function, and even be transmitted via the placenta, influencing the development of the foetal immune system.
This study faced several limitations. Firstly, it included only 11 pieces of literature, a relatively small sample size. Additionally, the literature search was limited to Chinese and English, potentially omitting relevant studies. Secondly, there was significant heterogeneity among the included studies, and a publication bias was noted in the IL-6 segment, which might have affected the meta-analysis results. The differences in cytokine measurement methods across studies led to substantial variability in outcome indicators. Furthermore, the data for these indicators were derived directly from the original articles and presented as medians (minimum value to maximum value), following the conversion method of Luo et al. (Citation2018), potentially impacting the analysis. Thus, there is an urgent need to incorporate additional literature to further substantiate this conclusion.
In summary, although amniotic fluid inflammatory biomarker monitoring is not yet commonly used in current clinical practice, the evidence provided in this study provides new directions for future research. Further study of the physiological relevance and clinical application of these biomarkers may be helpful in the prevention and management of preterm birth, particularly in the development of personalised intervention strategies. Our findings promote a deeper understanding of the pathophysiological mechanisms behind preterm birth and may guide clinical practice and policy development in the future, ultimately reducing the significant health burden associated with preterm birth.
Authors’ contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Cong Wang and Qin Chen. The first draft of the manuscript was written by Yan Wang, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Disclosure statement
The authors have no conflicts of interest to declare.
Data availability statement
The data used to support the findings of this study are included within the article.
Additional information
Funding
References
- Borna, S., Mirzaie, F. and Abdollahi, A., 2009. Mid-trimester amniotic fluid C-reactive protein, ferritin and lactate dehydrogenase concentrations and subsequent risk of spontaneous preterm labour. Australian & New Zealand Journal of Obstetrics & Gynaecology, 49 (4), 1–9.
- Cobo, T., et al., 2012. Intra-amniotic inflammation predicts microbial invasion of the amniotic cavity but not spontaneous preterm delivery in preterm prelabor membrane rupture. Acta Obstetricia et Gynecologica Scandinavica, 91 (8), 930–935.
- Ghezzi, F., et al., 2002. Elevated amniotic fluid C-reactive protein at the time of genetic amniocentesis is a marker for preterm delivery. American Journal of Obstetrics and Gynecology, 186 (2), 268–273.
- Goldenberg, R. L., et al., 2008. Epidemiology and causes of preterm birth. The Lancet, 371 (9606), 75–84.
- Goldenberg, R. L., Hauth, J. C. and Andrews, W. W., 2000. Intrauterine infection and preterm delivery. New England Journal of Medicine, 342 (20), 1500–1507.
- Han Huijie, S. J., et al., 2022. Study on the relationship between spontaneous preterm labor and amniotic fluid inflammatory cytokines and ureaplasma urealyticum infection in the second trimester of pregnancy. Zhongguo Bingan, 23 (1), 97–100.
- Kim, S. A., et al., 2022. Inflammatory proteins in the amniotic fluid, plasma, and cervicovaginal fluid for the prediction of intra-amniotic infection/inflammation and imminent preterm birth in preterm labor. American Journal of Perinatology, 39 (7), 766–775.
- Kunze, M., et al., 2016. Cytokines in noninvasively obtained amniotic fluid as predictors of fetal inflammatory response syndrome. American Journal of Obstetrics and Gynecology, 215 (1), 96.e1-8–96.e8.
- La Sala, G. B., et al., 2012. Protein microarrays on midtrimester amniotic fluids: a novel approach for the diagnosis of early intrauterine inflammation related to preterm delivery. International Journal of Immunopathology and Pharmacology, 25 (4), 1029–1040.
- Luo, D., et al., 2018. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Statistical Methods in Medical Research, 27 (6), 1785–1805.
- Musilova, I., et al., 2018. Amniotic fluid pentraxins: potential early markers for identifying intra-amniotic inflammatory complications in preterm pre-labor rupture of membranes. American Journal of Reproductive Immunology (New York, N.Y.: 1989), 79 (5), e12789.
- Oh, K. J., et al., 2011. Predictive value of intra-amniotic and serum markers for inflammatory lesions of preterm placenta. Placenta, 32 (10), 732–736.
- Payne, M. S., et al., 2014. Second trimester amniotic fluid cytokine concentrations, Ureaplasma sp. colonisation status and sexual activity as predictors of preterm birth in Chinese and Australian women. BMC Pregnancy and Childbirth, 14 (1), 340.
- Puchner, K., et al., 2011. Mid-trimester amniotic fluid interleukins (IL-1β, IL-10 and IL-18) as possible predictors of preterm delivery. In Vivo (Athens, Greece), 25 (1), 141–148.
- Son, G.-H., et al., 2016. Comparative analysis of midtrimester amniotic fluid cytokine levels to predict spontaneous very pre-term birth in patients with cervical insufficiency. American Journal of Reproductive Immunology (New York, N.Y.: 1989), 75 (2), 155–161.
- Tambor, V., et al., 2015. Potential peripartum markers of infectious-inflammatory complications in spontaneous preterm birth. BioMed Research International, 2015, 343501–343513.
- Vogel, J. P., et al., 2018. The global epidemiology of preterm birth. Best Practice & Research. Clinical Obstetrics & Gynaecology, 52, 3–12.
- Wenstrom, K. D., et al., 1998. Elevated second-trimester amniotic fluid interleukin-6 levels predict preterm delivery. American Journal of Obstetrics and Gynecology, 178 (3), 546–550.
- Wenstrom, K. D., et al., 1998. Intrauterine viral infection at the time of second trimester genetic amniocentesis. Obstetrics and Gynecology, 92 (3), 420–424.
- Wu, Y. and Zhou, X., 2019. Advances in the prediction of preterm labor by inflammatory mediators associated with amniotic fluid in the second trimester WU. International Journal of Obstetrics and Gynecology, 46 (6), 627–631.
- Yang M., et al., 2016. Relationship of cytokines levels and Ureaplasma infection in midtrimester amniotic fluid with spontaneous preterm birth. Chinese Journal of Perinatal Medicine, 19 (4), 263–268.
- Yoneda, S., et al., 2011. Prediction of exact delivery time in patients with preterm labor and intact membranes at admission by amniotic fluid interleukin-8 level and preterm labor index. Journal of Obstetrics and Gynaecology Research, 37 (7), 861–866.