

Abstract
Background
Preterm birth is a significant obstetrical concern around the globe. With this study, we aimed to determine whether a prior singleton pregnancy preterm birth increases the likelihood of preterm birth in subsequent twin pregnancies. We designed his systematic review to provide valuable information for pregnant women and obstetricians during counselling and for individuals involved in the planning of preventive strategies.
Methods
We comprehensively searched the PubMed, Embase and Scopus databases to identify relevant studies published until October 2023 following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We applied a random-effects meta-analysis to the data gathered from the selected studies.
Results
Among the 460 initially identified studies, only eight met the eligibility criteria. The analysis of incidence revealed an event rate of 9.5% (95% CI, 4.4–19.5%) for a history of preterm singleton birth in the cohort of women with subsequent twin pregnancies. Subgroup analyses focused on the risk of preterm twin births (<37 weeks, <34 weeks and <32 weeks) in women with prior preterm singleton births. Our results revealed a significantly elevated risk of subsequent preterm twin births associated with prior preterm singleton births at <37 weeks (OR, 2.94; 95% CI, 1.99–4.33; p < .001), <34 weeks (OR, 1.89; 95% CI, 1.67–2.14; p < .001) and <32 weeks (OR, 2.51; 95% CI, 1.58–3.99; p < .001), without heterogeneity in the included studies.
Conclusions
Our systematic analysis indicates a consistent and statistically significant association between a history of preterm singleton births and preterm twin births at various gestational ages. These findings underscore the importance of the obstetric history during assessments to predict the risk of preterm births in twin pregnancies. Clinicians should monitor pregnancies with a history of preterm singleton births, as targeted interventions and improved prenatal care can mitigate the risk of preterm birth during twin pregnancies.
Plain Language Summary
Preterm birth, a global concern, prompted a study examining whether a prior preterm singleton birth raises the risk of preterm birth in subsequent twin pregnancies. Conducting a systematic review of 460 studies, only eight met the eligibility criteria. The meta-analysis revealed a 9.5% incidence of preterm singleton births in subsequent twin pregnancies. Further analysis demonstrated a significantly elevated risk of preterm twin births at <32 weeks for those with a history of preterm singleton births. The study concludes that a consistent and statistically significant association exists between prior preterm singleton births and increased preterm twin birth risk at various gestational ages. This underscores the importance of considering obstetric history in assessing preterm birth risk in twin pregnancies. Clinicians are advised to closely monitor pregnancies with a history of preterm singleton births for interventions targeted and improved prenatal care.
Introduction
Preterm births remain a significant obstetric global challenge. In 2020, over 15 million infants representing over 11% of all live births, entered the world prematurely (Goldenberg et al. Citation2008, Blencowe et al. Citation2012, Citation2013, Ashorn et al. Citation2020). Preterm birth and its complications are a leading cause of neonatal mortality among infants who would otherwise be healthy (Goldenberg et al. Citation2008, Gupta Basuray et al. Citation2023). These complications can extend beyond infancy, leading to conditions such as cerebral palsy, visual impairments and chronic ailments that persist into adulthood (Barker Citation2004, Goldenberg et al. Citation2008, Alves and Alves Citation2024). Recurrent spontaneous preterm birth refers to the occurrence of more than one instance of preterm birth characterised by spontaneous labour initiation while membranes are still intact or after preterm membrane rupture (Romero et al. Citation2006, Goldenberg et al. Citation2008, Iams and Berghella Citation2010, Agrawal and Hirsch Citation2012, Zhao et al. Citation2012); awareness of this phenomenon is important.
Spontaneous preterm births impact the well-being of infants and should be considered when making informed family planning decisions. A comprehensive understanding of the likelihood of recurrent preterm birth is invaluable for women contemplating subsequent pregnancies (Iams and Berghella Citation2010, Morken Citation2012, Zhao et al. Citation2012). This information is equally crucial for obstetricians who provide patient counselling and devise strategies for prevention of complications (Morken Citation2012, Zhao et al. Citation2012). The foetuses of women with twin pregnancies face an elevated risk of preterm birth, with approximately 40% of women carrying twin pregnancies delivering before the 37th week of gestation (Facco et al. Citation2008, Morken Citation2012, Zhao et al. Citation2012, Easter et al. Citation2018). However, a nuanced exploration of the recurrence risk in diverse pregnancy subtypes is notably absent from the existing literature. To address this gap, we designed a systematic review to provide a definitive overview of the likelihood of recurrent spontaneous preterm birth.
Our study population included women with diverse pregnancy scenarios: a twin pregnancy after a preterm singleton birth, a singleton pregnancy after a preterm twin birth, and a singleton pregnancy after a preterm singleton birth. Additionally, we gathered clinical data on the trajectory of pregnancies following term deliveries of both singletons and twins (Ananth et al. Citation2008, Facco et al. Citation2008, Michaluk et al. Citation2013, Fox et al. Citation2015, Easter et al. Citation2018, Berveiller et al. Citation2020, Ward et al. Citation2023). By synthesising this comprehensive knowledge, our goal was to provide evidence to empower women, guide medical professionals and inform strategies within the nursing department for mitigating the impact of recurrent spontaneous preterm births (Goldenberg et al. Citation2008, Blencowe et al. Citation2012, Citation2013).
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to conduct this review and meta-analysis (Page et al. Citation2021).
Protocol registration
https://www.crd.york.ac.uk/prospero/#searchadvanced, CRD42023467016.
Search strategy
To identify relevant studies, we applied a comprehensive search strategy on PubMed, Embase, Web of Science and Scopus databases using appropriate keywords and Boolean operators. Our primary focus was to explore the risks of preterm birth in women with twin pregnancy after having had a preterm singleton birth. The search terms used included: ‘Twin pregnancy’, ‘twins’, ‘preterm birth’, ‘premature delivery’, ‘preterm labor’, ‘prior pregnancy’, ‘singleton pregnancy’, ‘reproductive history’, ‘neonatal outcomes’, ‘obstetric outcomes’, ‘risk factors’, ‘twin gestation’, ‘preterm birth rates’ and ‘pregnancy complications’. We applied inclusion and exclusion criteria to identify studies that met our research objectives. The search strategy aimed to gather the most relevant and up-to-date evidence to provide valuable information.
Inclusion criteria
Studies conducted on humans.
Studies on women with subsequent twin gestations with and without a history of singleton pre-term birth.
Studies following a cohort, case-control or observational study design, or including a secondary analysis from a randomised controlled trial.
Peer-reviewed publications.
Studies published in English.
Exclusion criteria
Studies not focusing on women with subsequent twin gestations or not reporting histories of pre-term birth.
Studies conducted in non-English languages.
Animal and in vitro studies.
Case reports, editorials, commentaries and letters.
Studies with incomplete or unavailable data.
Study selection and quality assessment
Two reviewers (PS and WW) independently assessed the eligibility of the studies for inclusion in the meta-analysis. Each study underwent a thorough evaluation based on predetermined criteria to ensure its relevance to the research question. The same reviewers independently conducted the literature search to minimise bias and improve the accuracy of study selection. Discrepancies or differences were resolved after consulting a third reviewer (YJ) to arrive at a consensus.
We assessed the risk of bias using the ROBINS-I tool. Two reviewers (PS and WW) independently assessed the methodological quality of the studies, and discrepancies were arbitrated by a third reviewer (YJ). Additionally, we conducted a GRADE (Grading of Recommendations, Assessment, Development and Evaluation) level of evidence assessment to evaluate the quality of evidence across included studies.
Data extraction
We gathered data meticulously, ensuring that relevant information was systematically extracted. We recorded data such as study type, groups involved, sample size, women with preterm births, and average maternal age. Additionally, we collected data on gestational age, interpregnancy period and reported risks of preterm births. Moreover, we collected information on the evaluation of risk estimates and variables that were adjusted in the included studies to obtain the risk estimates of prior preterm delivery.
Data analysis
To conduct the data analysis, we used Comprehensive Meta-analysis version 3.0 and applied a random-effects model (Borenstein Citation2022). We designed our meta-analysis to elucidate the association between our primary outcome: prior preterm singleton birth and preterm births in subsequent twin pregnancies. In terms of the secondary outcomes, additional analyses examined risks of different prior singleton birth periods on the overall risks of preterm birth on a twin pregnancy. Furthermore, we carried out a leave-one-out sensitivity analysis to assess the robustness of our findings and to identify any influential studies. This allowed us to systematically exclude each study from the meta-analysis one at a time and evaluate the impact on the overall results, ensuring the reliability of our conclusions.
In our leave-one-out sensitivity analysis, we specifically reported studies whose exclusion resulted in a change in the p value compared to the overall analysis. This approach ensured that we focused on identifying studies that had a substantial impact on the statistical significance of our findings. To evaluate the level of heterogeneity among the studies, we calculated I2 values. We classified heterogeneity as low (I2 values between 0 and 25%), moderate (I2 values between 25 and 75%) and considerable (I2 values ≥75%) (Higgins and Thompson Citation2002). To assess publication bias via Duval and Tweedie’s trim and fill procedure (Duval and Tweedie Citation2000), all analyses conducted in this study adhered to a significance level of 5%.
Results
General characteristics of the studies included
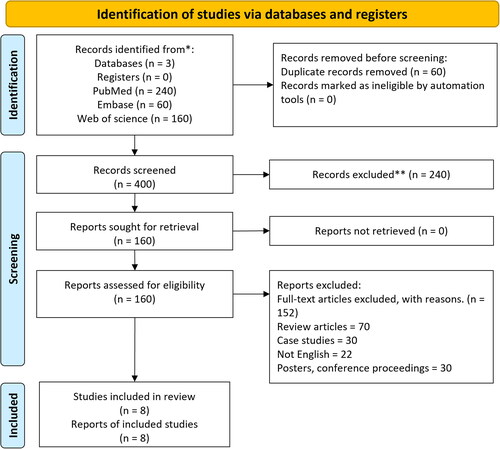
Throughout our systematic search of the literature, we initially identified 460 studies. After applying the predetermined inclusion criteria, eight studies were considered appropriate for inclusion, as depicted in . These selected studies exhibited heterogeneity in terms of their designs, with one being a secondary analysis of a randomised controlled trial (Easter et al. Citation2018) and the other seven retrospective cohort studies (Ananth et al. Citation2008, Facco et al. Citation2008, Schaaf et al. Citation2012, Michaluk et al. Citation2013, Fox et al. Citation2015, Berveiller et al. Citation2020, Ward et al. Citation2023). Supplementary Table 1 presents the details of the extracted data from these studies.
Figure 1. PRISMA flowchart.
Participant information
The analysis incorporated data from 73,888 twin expectant mothers, with 3481 of them presenting a history of preterm singleton delivery. The mean participant’s age was 32.3 ± 2.4 years.
Assessment of study quality
We assessed the methodological quality of the cohort studies in the analysis using the ROBINS-I tool (Sterne et al. Citation2016). Supplementary Table 2 summarises the findings of this assessment, revealing a high risk of bias across the studies included, with many having missing data and showing signs of selection bias (Supplementary Table 2). Additionally, the table also summarises the level of evidence based on the GRADE assessment which was low for one study (Easter et al. Citation2018), and moderate for the rest of the seven studies (Ananth et al. Citation2008, Facco et al. Citation2008, Schaaf et al. Citation2012, Michaluk et al. Citation2013, Fox et al. Citation2015, Berveiller et al. Citation2020, Ward et al. Citation2023).
Meta-analysis outcomes
Incidence of preterm singleton births
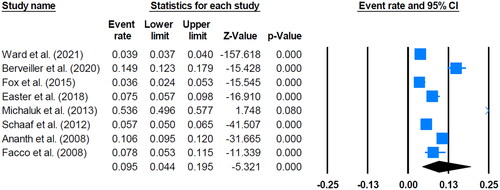
The event rate analysis of all the included studies demonstrated an incidence of 9.5% for preterm singleton birth in the women with subsequent twin pregnancies (; 95% CI, 4.4–19.5%; p < .01), without heterogeneity (I2, 0%). Additionally, our leave-one-out sensitivity analysis resulted in no studies whose removal led to a different p value outcome (Supplementary Figure 1).
Figure 2. Forest plot for twin expectant mothers with a history of preterm singleton birth.
Publication bias
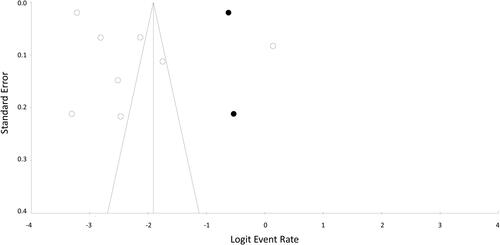
To assess publication bias, we applied Duval and Tweedie’s trim and fill method, which estimates the number of missing studies on either side of the mean effect of a funnel plot. According to our results, two studies were missing on the right side of the mean effect. The overall random effect models yielded a point estimate of 0.95 (95% CI, 0.04–0.19). We calculated point estimates imputed using the trim and fill method as 0.12 (95% CI, 0.51–0.28). shows the publication bias assessment details.
Figure 3. Publication bias analysis according to the Duval and Tweedie’s method.
Risk of preterm birth (<37 weeks) after preterm twin birth
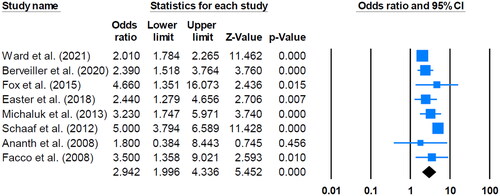
The analysis from all the included studies demonstrated that a prior preterm singleton birth (at <37 weeks) significantly increased the risk of having a preterm birth in a subsequent twin pregnancy (; OR, 2.94; 95% CI, 1.99–4.33; p < .001), without heterogeneity (I2, 0%). Additionally, our leave-one-out sensitivity analysis resulted in no studies whose removal led to a different p value outcome (Supplementary Figure 2).
Figure 4. Comparative outcomes for twin expectant mothers between those with and without a history of preterm birth (<37 weeks).
Risk of preterm birth (<34 weeks) after a preterm twin birth
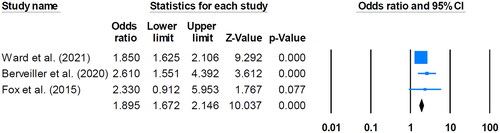
The analysis of three studies demonstrated that a prior preterm singleton birth (at <34 weeks) significantly increased the risk of the subsequent preterm twin birth (; OR, 1.89; 95% CI, 1.67–2.14; p < .001), without heterogeneity (I2, 0%). Additionally, our leave-one-out sensitivity analysis resulted in no studies whose removal led to a different p value outcome (Supplementary Figure 3).
Figure 5. Comparative outcomes for twin expectant mothers between those with and without a history of preterm birth (<34 weeks).
Risk of preterm birth (<32 weeks) after a preterm twin birth
Our analysis of the three studies included demonstrated that a prior preterm singleton birth (at <32 weeks) significantly increased the risk of subsequent preterm twin births (; OR, 2.51; 95% CI, 1.58–3.99; p < .001), without heterogeneity (I2, 0%). Additionally, our leave-one-out sensitivity analysis resulted in no studies whose removal led to a different p value outcome (Supplementary Figure 4).
Figure 6. Comparative outcomes for twin expectant mothers between those with and without a history of preterm birth (<32 weeks).

Discussion
The global challenge of preterm births, which profoundly impact neonatal health and may lead to long-term developmental outcomes, prompted us to design this systematic review and meta-analysis. We assessed possible associations between obstetric characteristics and the risk of spontaneous preterm births in women with singleton or multiple pregnancies.
We selected eight studies that met our criteria out of the initial 460 identified through our systematic search. The studies selected included a secondary analysis of a randomised controlled trial and seven retrospective cohort studies (Ananth et al. Citation2008, Facco et al. Citation2008, Schaaf et al. Citation2012, Michaluk et al. Citation2013, Fox et al. Citation2015, Easter et al. Citation2018, Berveiller et al. Citation2020, Ward et al. Citation2023). The different designs of the selected studies allowed us to thoroughly explore the possible association between preterm singleton births and subsequent twin pregnancies. Our analysis was based on a large dataset with information from 73,888 twin expectant mothers, including 3481 with a history of preterm singleton delivery. The participants’ average age was 32.3 years, highlighting the diverse representation of expectant mothers in our analysis. The event rate analysis across all included studies aimed to uncover the incidence of preterm singleton births within the twin pregnancy population. The findings revealed an incidence of 9.5% (; 95% CI, 4.4–19.5%; p < .01). Thus, nearly one in 10 twin pregnancies is associated with a preterm singleton birth. The narrow CI enhances the precision of our estimate, and the statistical significance (p < .01) emphasises the reliability of this observed incidence. Importantly, the absence of heterogeneity (I2, 0%) suggests a consistent pattern among the studies, indicating uniformity in the reported incidence rates. Also, the lack of heterogeneity enhances the reliability of our meta-analysis, demonstrating that the studies included were measuring the same phenomenon in a consistent manner. Moreover, our analysis results on the association between a history of preterm singleton births (at <37 weeks) and the subsequent risk of preterm twin births showed a substantial and statistically significant association (; OR, 2.94; 95% CI, 1.99–4.33; p < .001). Therefore, individuals with a prior preterm singleton birth face a nearly threefold higher risk of experiencing preterm twin births than individuals without such a history. Similarly, the absence of heterogeneity (I2, 0%) enhances the internal validity of our findings. Moreover, the consistency across studies in reporting increased risks reinforces the robustness of the observed association. We conducted subgroup analyses by stratifying preterm births at different gestational weeks (<37, <34 and <32 weeks). The results from three studies on the risk for women having had a singleton preterm birth at <34 weeks consistently demonstrated significantly increased risks (; OR, 1.89; 95% CI, 1.67–2.14; p < .001). Thus, women with twin pregnancies and a history of preterm singleton births are nearly twice as likely to experience preterm twin births at <34 weeks than women with twin pregnancies without a positive preterm singleton birth history. The absence of heterogeneity (I2, 0%) underscores the consistent pattern observed across studies, reinforcing the reliability of the association.
The subgroup analysis of three studies for women with a history of singleton preterm births at <32 weeks showed a significantly increased risk (; OR, 2.51; 95% CI, 1.58–3.99; p < .001), suggesting that these women face more than a twofold increased risk of experiencing preterm twin births at this very early gestational age compared with women without such a history. Again, we found no evidence of heterogeneity for these studies (I2, 0%). The results from our review confirm the significantly heightened risk of preterm twin births associated with prior preterm singleton births, and support previous findings (Kazemier et al. Citation2014).
A history of preterm singleton delivery may increase the risks of preterm twin delivery through various interconnected mechanisms (Schaaf et al. Citation2012, Michaluk et al. Citation2013, Fox et al. Citation2015). First, there could be underlying maternal factors, such as uterine abnormalities or cervical incompetence, that predispose a woman to preterm births, and these factors may persist in subsequent pregnancies, increasing the likelihood of preterm delivery in twins (Agrawal and Hirsch Citation2012, Morken Citation2012, Gupta Basuray et al. Citation2023, Ward et al. Citation2023). Second, a previous preterm birth may indicate an inherent susceptibility to factors such as infections, inflammation or hormonal imbalances, which can contribute to premature labour and delivery in subsequent pregnancies (Romero et al. Citation2006, Agrawal and Hirsch Citation2012). Third, the physiological stress on the uterus during a preterm birth might lead to changes in the uterine environment that make the organ less conducive to a full-term pregnancy, especially when carrying multiple foetuses (Romero et al. Citation2006, Calvin Citation2011, Agrawal and Hirsch Citation2012, Vidal et al. Citation2014, Ribeiro de Andrade Ramos and da Silva Citation2018). Overall, a history of preterm singleton delivery can serve as an indicator of complex, multifactorial risks that may influence subsequent twin pregnancies, highlighting the importance of closely monitoring and managing pregnancies in women with such a history to mitigate potential risks.
The details of the potential mechanisms enhancing the likelihood of preterm births in a woman with a previous preterm birth remain unclear. Unfortunately, we were not able to evaluate these mechanisms comprehensively in our systematic review and meta-analysis due to the paucity of available data. The complex nature of pregnancy and the many factors influencing preterm birth make it difficult to draw definitive conclusions. Further research with a focus on investigating these potential mechanisms and their interplay is warranted.
Our comprehensive findings consistently highlighted a substantial association between a previous preterm singleton birth and an enhanced risk of preterm twin births. The absence of heterogeneity strengthens the internal validity of our results, suggesting a coherent pattern across the diverse studies included in our analysis. Thus, our results are important for healthcare nursing professionals and clinicians advising and monitoring expectant mothers with preterm birth histories, informing targeted interventions and care strategies to mitigate the heightened risks associated with preterm births.
Limitations of our study
Limitations of our study need to be carefully considered in interpreting our findings. First, our study pool was relatively limited, as only eight out of 460 identified studies met our inclusion criteria. The small sample size imposes constraints on the generalisability of our results, highlighting the necessity for more extensive research exploring the intricate associations between obstetric history and recurrent preterm births.
Furthermore, the variability in reporting obstetric history details, including the circumstances of prior preterm births, may have introduced biases in the assessment of factors impacting subsequent pregnancies. Specifically, distinguishing between spontaneous and medically indicated preterm births is crucial, as their aetiologies may influence the recurrence risk differently. Unfortunately, the available data did not permit subanalyses based on this distinction, which underscores a gap in the literature and highlights the need for future research to provide more comprehensive data in this regard. Additionally, our meta-analysis included studies conducted across diverse geographical locations (France, Canada and USA) and over varying time periods. Differences in healthcare practices, policies and temporal trends may contribute to contextual variability, potentially affecting the applicability of our findings to specific populations or obstetric settings. Therefore, caution should be exercised when extrapolating our results to other contexts. Likewise, we acknowledge that the observed event rate of 9.5% for a history of preterm singleton births in women with twin pregnancies may appear low, and it could potentially be a type II error due to the limited number of studies included in our review. Although we attempted to address this concern by conducting a publication bias assessment, the small number of included studies may have affected the reliability of our findings. Moreover, while meta-regression analysis could offer insights into potential sources of heterogeneity and enhance the robustness of our findings, constraints in available data prevented us from conducting this analysis. This limitation underscores the need for future studies to incorporate meta-regression analysis to better understand the influence of key covariates and moderators on the association between obstetric history and recurrent preterm births.
We recognise the importance of addressing these limitations and advocating for future larger, well-designed studies to account for heterogeneity, explore diverse populations and utilise standardised methodologies. Despite these limitations, our study lays a valuable foundation for further investigations into the nuanced association between obstetric history and the risk of recurrent spontaneous preterm births in women carrying either singleton or multiple pregnancies.
Conclusions
After our analysis of data from eight studies, we uncovered an incidence of 9.5% for a history of preterm singleton births in women with twin pregnancies. Understanding and addressing preterm births in twin pregnancies is important to improve the outcomes of neonates. Our results indicate a significantly heightened risk across various gestational age thresholds. Women carrying twin pregnancies with a history of premature single births have a heightened risk of having premature twin births at an early gestational age. Our findings pave the way for improved risk assessments, informed decision-making and enhanced obstetrical care strategies, fostering the goal of healthier outcomes for both mothers and their infants.
Author contributions
Substantial contributions to the conception or design of the work: P. Shen and Y. Jiang.
The acquisition, analysis or interpretation of data for the work: P. Shen, W. Wu and Y. Jiang.
Drafting the work: P. Shen and W. Wu.
Reviewing it critically for important intellectual content: Y. Jiang.
Final approval of the version to be published: P. Shen, W. Wu and Y. Jiang.
Supplemental Material
Download Zip (101.5 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
The data that support the findings of this study are openly available in PubMed, Embase and Scopus databases.
Additional information
Funding
References
- Agrawal, V. and Hirsch, E., 2012. Intrauterine infection and preterm labor. Seminars in Fetal & Neonatal Medicine, 17 (1), 1–9.
- Alves, J.G.B. and Alves, L.V., 2024. Early-life nutrition and adult-life outcomes. Jornal de Pediatria, 100 (Suppl. 1), S4–S9.
- Ananth, C.V., Kirby, R.S., and Vintzileos, A.M., 2008. Recurrence of preterm birth in twin pregnancies in the presence of a prior singleton preterm birth. Journal of Maternal-Fetal & Neonatal Medicine, 21 (5), 289–295.
- Ashorn, P., et al., 2020. The Lancet Small Vulnerable Newborn Series: science for a healthy start. Lancet, 396 (10253), 743–745.
- Barker, D.J.P., 2004. The developmental origins of chronic adult disease. Acta Paediatrica Supplement, 93 (446), 26–33.
- Berveiller, P., et al., 2020. Risk of preterm birth in a twin pregnancy after an early-term birth in the preceding singleton pregnancy: a retrospective cohort study. British Journal of Gynecology, 127 (5), 591–598.
- Blencowe, H., et al., 2012. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet, 379 (9832), 2162–2172.
- Blencowe, H., et al., 2013. Born too soon: the global epidemiology of 15 million preterm births. Reproductive Health, 10 (Suppl. 1), S2.
- Borenstein, M., 2022. Chapter 27 – comprehensive meta-analysis software. In: M. Egger, J.P.T. Higgins and G.D. Smith, eds. Systematic reviews in health research. Oxford, UK: John Wiley & Sons Ltd.
- Calvin, S., 2011. Care for women with prior preterm birth. American Journal of Obstetrics and Gynecology, 204 (3), e7.
- Duval, S. and Tweedie, R., 2000. A nonparametric “trim and fill” method of accounting for publication bias in meta-analysis. Journal of the American Statistical Association, 95 (449), 89–98.
- Easter, S.R., et al., 2018. Obstetric history and likelihood of preterm birth of twins. American Journal of Perinatology, 35 (11), 1023–1030.
- Facco, F.L., Nash, K., and Grobman, W.A., 2008. Are women who have had a preterm singleton delivery at increased risk of preterm birth in a subsequent twin pregnancy? American Journal of Perinatology, 25 (10), 657–659.
- Fox, N.S., et al., 2015. Preterm birth or small for gestational age in a singleton pregnancy and risk of recurrence in a subsequent twin pregnancy. Obstetrics and Gynecology, 125 (4), 870–875.
- Goldenberg, R.L., et al., 2008. Epidemiology and causes of preterm birth. Lancet, 371 (9606), 75–84.
- Gupta Basuray, R., et al., 2023. Increasing exclusive nursery care of late preterm and low birth weight infants. Hospital Pediatrics, 13 (11), 992–1000.
- Higgins, J.P.T. and Thompson, S.G., 2002. Quantifying heterogeneity in a meta-analysis. Statistics in Medicine, 21 (11), 1539–1558.
- Iams, J.D. and Berghella, V., 2010. Care for women with prior preterm birth. American Journal of Obstetrics and Gynecology, 203 (2), 89–100.
- Kazemier, B., et al., 2014. Impact of obstetric history on the risk of spontaneous preterm birth in singleton and multiple pregnancies: a systematic review. British Journal of Gynecology, 121 (10), 1197–1208; discussion 1209.
- Michaluk, A., et al., 2013. Predicting preterm birth in twin pregnancy: was the previous birth preterm? A Canadian experience. Journal of Obstetrics and Gynaecology Canada, 35 (9), 793–801.
- Morken, N.-H., 2012. Preterm birth: new data on a global health priority. Lancet, 379 (9832), 2128–2130.
- Page, M.J., et al., 2021. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. British Medical Journal, 372, n71.
- Ribeiro de Andrade Ramos, B. and da Silva, M.G., 2018. The burden of genetic and epigenetic traits in prematurity. Reproductive Sciences, 25 (4), 471–479.
- Romero, R., et al., 2006. The preterm parturition syndrome. British Journal of Gynecology, 113 (Suppl. 3), 17–42.
- Schaaf, J.M., et al., 2012. Recurrence risk of preterm birth in subsequent twin pregnancy after preterm singleton delivery. British Journal of Gynecology, 119 (13), 1624–1629.
- Sterne, J.A., et al., 2016. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. British Medical Journal, 355, i4919.
- Vidal, A.C., et al., 2014. Maternal stress, preterm birth, and DNA methylation at imprint regulatory sequences in humans. Genetics & Epigenetics, 6, 37–44.
- Ward, C., Nakagawa, S., and Cheng, Y.W., 2023. Prior term birth decreases the risk of preterm birth in a subsequent twin gestation. American Journal of Perinatology, 40 (2), 206–213.
- Zhao, X., et al., 2012. Reducing preterm births in China. Lancet, 380 (9848), 1144–1145; author reply 1145.