

Abstract
Background
To analyse changes in lipid levels during the development of intrahepatic cholestasis of pregnancy (ICP) and identify new biomarkers for predicting ICP.
Methods
A retrospective case-control study was conducted to analyse 473 pregnant women who underwent regular prenatal examinations and delivered at the Women and Children’s Hospital, School of Medicine, Xiamen University, between June 2020 and June 2023, including 269 normal pregnancy controls and 204 pregnant women with cholestasis.
Results
Patients with ICP with gestational diabetes mellitus (GDM) have lower high-density lipoprotein (HDL) levels than in those without GDM. Total bile acid (TBA) levels were significantly higher in pregnant women with GDM than those without. The apolipoprotein A (APOA) level was lower in patients with ICP and hypothyroidism than those without hypothyroidism. TBA levels were significantly higher in pregnant women with hypothyroidism than those without. Triglyceride (TG) levels were significantly higher in patients with preeclampsia (PE) than those without. HDL and APOA levels were lower in women with ICP complicated by preterm delivery than those with normal delivery. The AUC (area under the curve) of the differential diagnosis of cholestasis of pregnancy for the APOA/APOB (apolipoprotein B) ratio was 0.727, with a sensitivity of 85.9% and specificity of 47.5%.
Conclusions
The results suggested that dyslipidaemia is associated with an increased risk of ICP and its complications. The timely detection of blood lipid and bile acid levels can assist in the diagnosis of ICP and effectively prevent ICP and other complications.
Plain Language Summary
Intrahepatic cholestasis of pregnancy (ICP) is recognized as one of the most severe complications during pregnancy. Currently, elevated fasting serum total bile acid (TBA) levels are commonly used as diagnostic markers for ICP. However, it has been observed that women diagnosed with ICP often do not exhibit elevated TBA levels. Additionally, other medical conditions can also lead to increased TBA levels. Our study has revealed a potential correlation between abnormal lipid metabolism and the occurrence and progression of ICP and its associated complications. Specifically, we found that patients with ICP who have higher serum bile acid levels tend to have more disrupted lipid metabolism, as well as a higher risk of complications and adverse pregnancy outcomes. This manuscript is the first to investigate the link between dyslipidemia and ICP, as well as other pregnancy complications. As a result, our findings offer a foundation for the clinical diagnosis and treatment of ICP and its comorbidities during pregnancy, while also highlighting the need for further research in this area.
Keywords:
Introduction
Intrahepatic cholestasis of pregnancy (ICP) is one of the most serious complications of pregnancy, affecting approximately 0.1–2% of pregnant women globally and approximately 2.3–6.0% of pregnant women in China (Hofmann and Hagey Citation2008, 2016). ICP occurs only during pregnancy and resolves independently by the end of pregnancy. However, the probability of recurrence increases significantly (Piechota and Jelski Citation2020, Panaitescu et al. Citation2021). ICP is associated with an increase in the incidence of adverse perinatal outcomes, including spontaneous premature birth, foetal distress, intrauterine death and growth restriction, low Apgar scores, and fluid meconium contamination (Wensink Citation2016, Monrose et al. Citation2021). Bile acids have important functions in the body and play crucial roles in fat digestion and absorption. The main characteristics of cholestasis are the obstruction of bile flow and excessive accumulation of bile acids. Due to the surfactant properties of hydrophobic bile acids, direct action on the plasma membrane bilayer result in changes in membrane proteins and disruption of cell integrity (Perez and Briz Citation2009, Li and Chiang Citation2017). Bile acids induce cytotoxic effects through a series of reactions, including oxidative stress (Perez and Briz Citation2009). Elevated levels of bile acids can induce liver cells to produce pro-inflammatory mediators, attract immune cells and trigger liver inflammation, ultimately leading to cholestatic liver injury (Panaitescu et al. Citation2021, Majsterek et al. Citation2022). Severe oxidative stress and mitochondrial damage play important roles in impacting fertility disorders induced by bile stasis in male and female rats (Ommati et al. Citation2019). Water-soluble bile acids, such as ursodeoxycholic acid (UDCA), have therapeutic value in complications related to bile stasis (Stamp and Jenkins Citation2008). However, excessive accumulation of hydrophobic bile acids in the body may affect multiple organs, including kidneys, liver, skeletal muscles and heart (Fickert et al. Citation2013, O’Brien et al. Citation2016, Bosoi et al. Citation2017).
Lipids play crucial roles in cellular structure, function, signal transduction and energy storage. For example, lecithin, a structural lipid, is decreased in patients with ICP. The obstruction of PC secretion into bile, as well as a significant decrease in phospholipid concentration in bile, can damage bile duct cell membranes and cause biliary tract lesions, leading to common bile duct diseases. In addition, total bile acid (TBA) levels are closely related to lipid metabolism, absorption and regulation, particularly of cholesterol. Since cholesterol is degraded into bile acids in the liver, this suggests abnormal changes in blood lipid levels, which may be related to the generation of bile acids and bile acid metabolic disorders. Furthermore, the liver plays a major role in lipid metabolism, and damage to the liver may exacerbate abnormalities in lipid metabolism. Bile acid is absorbed by the intestine and directly regulates cholesterol synthesis in the liver and intestinal mucosal cells, suggesting that abnormal lipid metabolism inevitably leads to abnormal bile acid metabolism. Differences in lipid physiology during pregnancy and in patients with ICP have also been documented. This is because of bile stasis in the central area of the hepatic lobules in patients with ICP, which leads to liver cell and organ damage, resulting in abnormal lipid metabolism.
Currently, elevated fasting serum TBA levels are the most commonly used laboratory diagnostic markers for ICP (Lammert et al. Citation2000, Walker et al. Citation2002, Williamson and Geenes Citation2014). However, women diagnosed with intracranial pressure in clinical practice often do not have elevated TBA levels (Holland RL Citation1987, Egerman and Riely Citation2004). Other diseases can also result in elevated serum TBA levels (Reyes and Sjövall Citation2000). Based on the limitations of using bile acids to diagnose ICP in clinical practice, our study aimed to analyse the correlation between blood lipid levels and ICP as well as the role of blood lipid levels in the occurrence and development of gestational bile stasis and other adverse pregnancy outcomes to assist clinicians in preventing and treating gestational bile stasis and other adverse pregnancy outcomes, and to provide a theoretical basis for the pathogenesis of gestational bile stasis.
Methods
Pregnant women aged 20–40 years in the second and third trimesters (≥14 weeks) who visited the Women and Children’s Hospital, School of Medicine, Xiamen University from 1 January 2020 to 6 April 2023 were selected. According to the ICP diagnosis and treatment guidelines published in 2015, participants were divided into two groups: the gestational cholestasis group (experimental group, n = 204) and a control group (269 healthy pregnant women). The average age of the experimental normal control groups were 31.45 ± 3.738 y and 29.74 ± 3.325 y, respectively, with no significant difference between the two groups (p > .05).
Pregnant women aged 20–40 years (gestational age ≥14 weeks) who visited our hospital for prenatal care were included in the study. Pregnant women were excluded if they had: (1) acute or chronic liver disease; (2) viral hepatitis; (3) an autoimmune disease; (4) biliary obstruction; (5) abnormal abdominal ultrasonography findings; or (6) another disease leading to liver dysfunction. Women with ICP undergo foetal monitoring from the time of diagnosis until delivery, and medical therapy, including UDCA, to relieve their symptoms.
Serum triglyceride (TG), total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL), apolipoprotein A (APOA), apolipoprotein B (APOB), alanine aminotransferase (ALT), aspartate aminotransferase (AST) and TBA levels were measured before treatment.
The diagnostic criteria for ICP were based on guidelines published in 2015. ICP usually starts in the palms and soles of the feet, and then gradually worsens in the limbs, trunk and face. Pruritus involving palms and soles with scratches often indicates the need to identify ICP and differentiate it from other skin diseases during pregnancy. Elevated fasting serum TBA levels (≥10 μmol/L) during pregnancy can be used to diagnose ICP. Patients with normal TBA levels accompanied by other unexplained abnormal liver functions, mainly mild-to-moderate elevations in serum ALT and AST levels, can be diagnosed with ICP if accompanied by increased glycine and serum bilirubin levels, mainly direct bilirubin levels. Skin pruritus and abnormal liver function spontaneously returned to normal after delivery. Skin pruritus usually disappears within 1–2 days after pregnancy termination and liver function returns to normal within 28–42 days after pregnancy.
Enzyme colorimetry was used to measure TG and TC levels; immunoturbidimetry was used to measure LDL and HDL levels; immunoturbidimetry was used to measure APOA and APOB levels; and enzyme cycling was used to measure TBA levels.
SPSS software (IBM, Armonk, NY) was used for statistical analyses. Count data were expressed as (cases (%)) and were analysed using the Chi-square test. Data with a normal distribution are represented as the mean ± standard deviation, and comparisons between groups were analysed using Student’s t-test. Data with a non-normal distribution are expressed as the median (M) (quartile (P25–P75)), and comparisons between groups were performed using Wilcoxon’s rank sum test and p ≤ .05 was considered statistically significant. Receiver operating characteristic (ROC) curves were used to evaluate the diagnostic efficacy of biochemical indicators to determine the specificity, sensitivity and optimum cut-off values for this index. The diagnostic values of the indicators were determined by calculating the area under the curve (AUC). The criteria were as follows: <0.5 indicated no diagnostic value, ≥0.5 to <0.7 indicated low diagnostic accuracy and ≥0.7 to 0.9 indicated medium accuracy. The diagnostic accuracy was considered high at AUC ≥0.9, and p ≤ .05 was considered statistically significant.
This study was approved by the Medical Ethics Committee of Women and Children’s Hospital of Xiamen University (approval number: KY-2023-042-K01) and adhered to the principles of the Declaration of Helsinki.
Results
A total of 204 patients with ICP were included in the experimental group and 269 healthy pregnant women were included in the control group. All women delivered at full term and had no foetal chromosomal or structural anomalies (). LDL, TC, APOB and TGs levels were significantly higher in patients with ICP than healthy pregnant controls (p < .05). The levels of APOA and HDL/LDL and APOA/APOB ratios were lower in the ICP group than the control group (p < .05). However, there was no significant difference in HDL levels between the two groups ().
Figure 1. Patient flow diagram in this study. All women deliver at full term with no foetal chromosomal or structural anomalies.
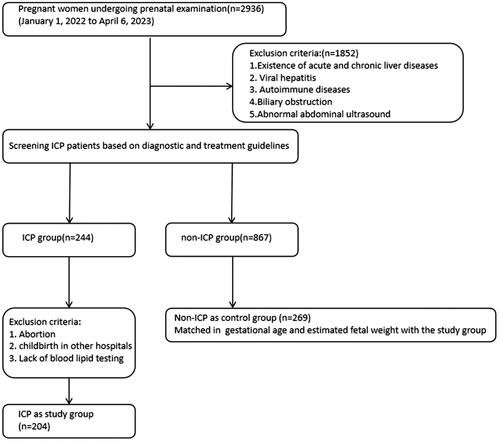
Table 1. Analysis of differences in lipid levels between patients with cholestasis of pregnancy and normal pregnant controls.
Pearson’s correlation coefficient analysis demonstrated that AL and AST levels were significantly correlated with HDL, LDL and APOA levels and APOA/APOB and HDL/LDL ratios. LDL levels were positively correlated, whereas all other levels were negatively correlated. TBA levels were negatively correlated with HDL, CHOL, TG and APOA levels, and APOA/APOB and HDL/LDL ratios. The specific statistical parameters are listed in .
Table 2. Correlation analysis between changes in serum ALT, AST and TBA levels and blood lipid levels in patients with ICP (n = 204).
ROC curve analysis and calculation of the AUC demonstrated that LDL, TC, APOB and APOA levels and the APOA/APOB and HDL/LDL ratios all exhibited some capacity for the diagnosis of cholestasis of pregnancy (p < .001; ). The APOA/APOB ratio was the largest (0.727). When the cut-off value was less than 1.4781, the sensitivity and specificity for the diagnosis of cholestasis of pregnancy were 0.859 and 0.475, respectively. APOB was the second-most abundant protein (p = .695). When the cut-off value exceeded 1.165, the sensitivity and specificity of the diagnosis of cholestasis of pregnancy were 0.874 and 0.475, respectively. When the cut-off value for the HDL/LDL ratio was less than 1.165, the sensitivity and specificity for the diagnosis of cholestasis of pregnancy were 0.844 and 0.456, respectively. When the cut-off value for APOA was less than 1.755, the sensitivity and specificity for the diagnosis of cholestasis of pregnancy were 0.613 and 0.574, respectively ().
Figure 2. ROC curves for the differential diagnosis of cholestasis of pregnancy for each blood lipid index. (A) Receiver operating characteristic (ROC) curves of triglyceride (TG), apolipoprotein B (APOB), low-density lipoprotein (LDL) and total cholesterol (TC) levels for the differential diagnosis of cholestasis of pregnancy. (B) ROC curves of apolipoprotein A (APOA) levels, the APOA/APOB ratio and the high density lipoprotein (HDL)/LDL ratio for the differential diagnosis of cholestasis of pregnancy.
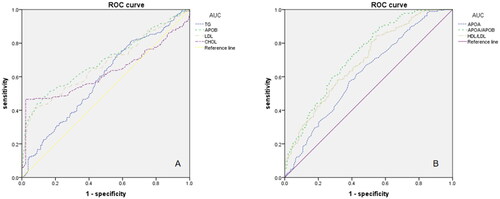
Table 3. Evaluation of the diagnostic effect of each indicator on cholestasis of pregnancy.
Logistic regression analysis showed that, after adjusting for confounding factors with age as a covariate, LDL, CHOL, TG, APOA, APOB, APOA/APOB and HDL/LDL were all independent risk factors for ICP ().
Table 4. Regression analysis of intrahepatic cholestasis of pregnancy risk factors.
HDL levels were significantly lower, whereas bile acid levels were significantly higher, in patients with ICP complicated by gestational diabetes mellitus (GDM), compared with ICP without GDM (p < .05). There were no significant differences in TG, TC, APOA, APOB or LDL levels ().
Table 5. Analysis of differences in serum lipid and bile acid levels between patients with uncomplicated ICP and ICP with pregnancy complications.
There were no significant differences in levels of HDL, TC, APOA, LDL, TGs, APOB or bile acids between patients with ICP complicated by gestational hypertension and those without ICP ().
APOA levels were significantly lower, and bile acid levels were significantly higher, in patients with ICP and hypothyroidism, than those without hypothyroidism (p < .05). There were no significant differences in TG, HDL, LDL, APOB or CHOL levels between the two groups ().
TG levels were significantly higher in patients with ICP complicated by preeclampsia (PE) than in those with ICP without PE (p < .05). There were no significant differences in TC, APOA, APOB, HDL or LDL levels between the two groups ().
There were no significant differences in HDL, LDL, TG, TC, APOA, APOB or bile acid levels between patients with and without haemolytic streptococcal infection ().
There were no significant differences in HDL, LDL, TC, TG, APOA, APOB or bile acid levels between patients with ICP and premature membrane rupture and those without premature membrane rupture ().
There were no significant differences in the TG, HDL, LDL, APOA, APOB, TC or bile acid levels between patients with ICP who underwent caesarean section and those who underwent natural delivery ().
The levels of HDL and APOA were lower in women with ICP who had preterm delivery than those who had term delivery; however, the levels of TGs, APOB, LDL and bile acids were higher in those who delivered full-term (p < .05). There was no significant difference in TC levels between the two groups ().
Discussion
ICP is a pregnancy-related condition. Maternal serum bile acid levels are currently regarded as the most important serological indicators for the diagnosis and monitoring of ICP (Liu Citation2016, Li Citation2019, Liu et al. Citation2009). Recent studies have suggested that the onset of serum lipid level disorders in patients with ICP is earlier than that of bile acid elevation (Hao et al. Citation2016). By analysing changes in blood lipid levels during the development of cholestasis during pregnancy, suggest that monitoring blood lipid levels during pregnancy also has diagnostic and predictive value for the risk of ICP and its complications. In clinical practice, understanding changes in blood lipid levels can reflect the status of liver lipid metabolism, combined with an evaluation of the degree of liver damage using liver function indicators at the appropriate time.
Lipids play crucial roles in the structure, function, signalling and energy storage of cells. Thus, the disruption of lipid metabolism and transport has implications for human diseases. In bile acid metabolism, the main role of very LDLs is to carry cholesterol to the liver for transformation and clearance. Cholesterol is transformed into bile acids after degradation in the liver, and bile acids are closely related to the metabolism, absorption and regulation of lipids, especially cholesterol (Wen and Liu Citation2015). When serum bile acid levels increase, cholesterol and TG levels also increase significantly (Lin 2009). Furthermore, some studies have demonstrated that there are differences in blood lipid changes in pregnant patients with and without ICP. This may be due to cholestasis in bile capillaries in the central area of the liver lobule in patients with ICP, which leads to increased liver cell damage, liver organ damage and abnormal lipid metabolism (Wen and Liu Citation2015). The pathogenesis of ICP remains unclear. The results of the present study showed that lipid metabolism disorders were present in patients with ICP, consistent with the results of Lu et al. (Citation2021). Sheng et al. (Citation2017) reported that changes in blood lipid levels may be the direct result of cholestasis or one of the influencing factors leading to ICP. The results of the present study showed that TC, TG, LDL and APOB levels were higher in patients with ICP than those with normal pregnancies, suggesting that ICP is associated with abnormal lipid metabolism. The detection of lipid levels in early pregnancy is helpful in guiding early intervention, indicating that ALT, AST and bile acid levels correlate with some lipid parameters in patients with ICP. In clinical practice, lipid changes that reflect the status of liver lipid metabolism status, combined with liver function indicators, may be used to evaluate the degree of liver injury, allowing appropriate treatment plans to be provided at the appropriate time.
Increased dyslipidaemia and changes in blood lipid composition may be related to the occurrence and development of pregnancy-related complications (Sheng et al. Citation2017). Under normal physiological conditions, an increase in blood lipid levels during pregnancy leads to an increase in blood viscosity and peroxide products, which cause the deposition of blood lipids in the vascular wall of the placenta, thereby damaging vascular endothelial cells and affecting both the immune and coagulation systems. If the damage develops further, a series of pregnancy complications, including hypertensive disorders of pregnancy and GDM, may occur (Zheng and Zhai Citation2013).
Zhou et al. (Citation2020) demonstrated that levels of TG, TC and LDL-cholesterol are higher, while the level of HDL-cholesterol (HDL-C) is lower, in patients with GDM than those with a normal pregnancy. The results of the present study also showed that the HDL-C levels in patients with ICP and GDM were lower than those in patients with ICP without GDM. HDL-C actively protects the maternal vascular endothelium during pregnancy (Sulaiman et al. Citation2016). LDL synthesis increases with increasing gestational age, whereas lipoprotein activity gradually decreases, leading to an increase in TC, TG, LDL and other blood lipid indicators in the third trimester (Gao and Zhu Citation2016). Owing to the limited metabolic capacity of the liver for glycogen metabolism, excess glycogen is stored in peripheral tissues as very LDLs under the action of hepatic insulin-sensitising substances (Zhou et al. Citation2020). However, patients with ICP may suffer from liver damage and decreased metabolic capacity due to cholestasis, resulting in an inability to store glycogen and an abnormal glucose metabolism (Cossu et al. Citation2018, McKenzie-Sampson et al. Citation2018, Li and Li Citation2019). Abnormal lipid metabolism in patients with gestational cholestasis, especially an increase in TC levels and a decrease in HDL-C levels, may increase the risk of GDM.
Similar results were also reported by Chen and Qiu (Citation2013). Among the blood lipids tested in patients with hypothyroidism during pregnancy, HDL levels decreased, and LDL, cholesterol and TG levels significantly increased (Zheng and Zhai Citation2013). The results of the present study showed that the APOA levels were lower in patients with ICP complicated by hypothyroidism than those without hypothyroidism. Both studies suggest that abnormal lipid metabolism in patients with cholestasis of pregnancy may increase the risk of hypothyroidism.
Abnormal lipid metabolism in pregnant women may lead to significantly increased TG levels in the third trimester, damage to vascular endothelial function, and an increased risk of PE (Zeng Citation2021). The results of the present study showed that TG levels were higher in patients with ICP complicated by PE than those without ICP, suggesting that abnormal lipid metabolism in patients with gestational cholestasis may increase the risk of PE.
The proportion of caesarean sections and premature deliveries is lower in pregnant women with normal blood lipid levels than in women with abnormal blood lipid levels, mainly because the incidence of diseases during pregnancy increases when women have abnormal blood lipid levels. Thus, they are more likely to undergo caesarean section. An increase in the blood lipid concentration in pregnant women leads to endothelial cell dysfunction, chronic inflammation and increased blood coagulation, which cause pathological changes in maternal placental arteries and veins, placental ischaemia and hypoxia, and further cause premature delivery and foetal distress (Guo Citation2017, Zhou Citation2019). Abnormal lipid metabolism in ICP patients may lead to an increased rate of preterm births. The results of the present study indicated that the levels of LDL, TGs, apolipoprotein and bile acids were higher in women with preterm delivery than in those with term delivery. Therefore, improving the control of blood lipid levels in patients with ICP will help reduce the incidence of foetal complications. In conclusion, regular measurements of lipid levels in patients with ICP are helpful for physicians to diagnose and intervene in associated complications.
ROC curves were used to evaluate the diagnostic efficacy of the related biochemical indicators. The APOA/APOB ratio had the largest AUC (0.727), indicating its diagnostic value. When the AUC of the APOA/APOB ratio was 0.727 and the cut-off value was less than 1.4781, the diagnostic values for ICP were 0.859 and 0.475, respectively. These results suggest that the APOA/APOB ratio can be used as a novel biomarker for diagnosis of ICP.
Cholestasis refers to a significant decrease in bile flow. The liver is the main organ affected by cholestasis, but other organs, including the heart, kidneys, nervous system, skeletal muscles and reproductive system, may also be affected (Ommati et al. Citation2019). Kidneys are the most affected extrahepatic organs in patients with cholestasis (Betjes and Bajema Citation2006, Erlinger Citation2014, Aniort et al. Citation2017, Krones et al. Citation2017), and kidney damage caused by bile stasis is known as biliary nephropathy (Holt et al. Citation1999). The redox state of glutathione in the kidneys of animals with cholestasis is altered (Martínez-Cecilia et al. Citation2016), and key target points, including proteins and lipids, are also affected by bile stasis. Previous studies have reported that bile stasis significantly reduces tissue antioxidant capacity and lipid peroxidation and protein carbonisation are significantly reduced (Ommati et al. Citation2020, Ommati et al. Citation2021a, Citation2021b, Citation2021c). Cholestasis can also lead to pulmonary fibrosis and respiratory distress, and oxidative stress and inflammatory responses play important roles in its pathogenesis (Ommati et al. Citation2023a, Citation2023b). In summary, the consequences of oxidative stress, inflammatory reactions, mitochondrial damage and other cholestatic reactions are not limited to the liver. It causes damage to multiple organs and increases the risk of complications in pregnant women. Therefore, for clinical diagnosis and treatment, we should strengthen the prevention and treatment of cholestasis and actively identify early markers of ICP, thereby improving early detection and treatment of ICP.
Statins are widely prescribed for the treatment of dyslipidaemia. A previous report described a decrease in cholesterol and serum TBA levels in patients with primary biliary cirrhosis (PBC) after taking pravastatin (Kurihara et al. Citation1993). Another case report described a significant improvement in cholestasis and hypercholesterolaemia in patients with PBC (Kamisako and Adachi Citation1995). However, recent studies do not support these results. In patients with PBC and incomplete biochemical reactions to UDCA, atorvastatin does not improve bile stasis (Stojakovic et al. Citation2007). Therefore, more data are needed to explore whether cholesterol-lowering drugs affect ICP.
In conclusion, the occurrence and development of cholestasis and its complications during pregnancy may be associated with abnormal lipid metabolism. Higher serum bile acid levels in patients with ICP indicate more disordered lipid metabolism, greater risk of complications, and adverse pregnancy outcomes in patients with ICP. Therefore, it is important to actively control bile acid and blood lipid levels in patients with ICP and treat them effectively. However, the pathogenesis of cholestasis of pregnancy requires consideration of the influence of multiple factors, including genes, environment, hormone level changes, diet, exercise, chronic diseases and family history. Simultaneously, multi-centre studies with a larger sample size are required to verify these results. In clinical practice, bile acid and blood lipid levels in pregnant women should be closely monitored (Zhong Citation2004) to improve the diagnosis and early prevention of ICP. This may improve both maternal and neonatal outcomes (Zhang Citation2018). At the same time, the findings of the present study will play a positive role in the further exploration of the pathogenesis of cholestasis of pregnancy and the treatment of the disease. These results have clinical significance, as they suggest that follow-up monitoring of blood lipid changes is beneficial in reducing the risk of complications of cholestasis during pregnancy.
Author contributions
Huibin Huang: conception and design, analysis and interpretation of data, drafting the work, writing the manuscript and approval of the final version to be published.
Juan Li: conception and design, analysis and interpretation of data, drafting the work, writing the manuscript and approval of the final version to be published.
Tianhua Chen: conception and design, analysis and interpretation of data, drafting the work, writing the manuscript and approval of the final version to be published.
Meidan Lu: conception and design, analysis of data and approval of the final version to be published.
Gunsang Zhuoma: analysis of data and writing the manuscript, approval of the final version to be published.
Lijin Chen: drafting the work and critical interpretation of content, approval of the final version to be published.
Yuebin Gan: writing the manuscript, approval of the final version to be published.
Huiming Ye: conception and design, analysis and interpretation of data, drafting the work, writing the manuscript and critical interpretation of content, approval of the final version to be published.
Acknowledgements
We would like to thank Editage (www.editage.cn) for English language editing.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
All generated raw data and/or analysed data from the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Aniort, J., et al., 2017. Bile cast nephropathy caused by obstructive cholestasis. American Journal of Kidney Diseases, 69 (1), 1–9.
- Betjes, M.G. and Bajema, I., 2006. The pathology of jaundice-related renal insufficiency: cholemic nephrosis revisited. Journal of Nephrology, 19 (2), 229–233.
- Bosoi, C.R., et al., 2017. The bile duct ligated rat: a relevant model to study muscle mass loss in cirrhosis. Metabolic Brain Disease, 32 (2), 513–518.
- Chen, D. and Qiu, P., 2013. A study on the value of lipid metabolism in hypothyroidism during pregnancy. Chinese Journal of Eugenics and Genetics, 21 (2), 79.
- Cossu, E., et al., 2018. Presence of diabetes-specific autoimmunity in women with gestational diabetes mellitus (GDM) predicts impaired glucose regulation at follow-up. Journal of Endocrinological Investigation, 41 (9), 1061–1068.
- Egerman, R.S. and Riely, C.A., 2004. Predicting fetal outcome in intrahepatic cholestasis of pregnancy: is the bile acid level sufficient? Hepatology, 40 (2), 287–288.
- Erlinger, S., 2014. Bile acids in cholestasis: bad for the liver, not so good for the kidney. Clinics and Research in Hepatology and Gastroenterology, 38 (4), 392–394.
- Fickert, P., et al., 2013. Bile acids trigger cholemic nephropathy in common bile-duct-ligated mice. Hepatology, 58 (6), 2056–2069.
- Gao, X. and Zhu, T., 2016. The relationship between serum lipid levels and pregnancy outcomes in pregnant women with diabetes in early and late pregnancy. Anhui Medicine, 20 (11), 2093–2095.
- Guo, X., 2017. A study on the relationship between blood lipid levels and pregnancy outcomes in pregnant women. Hangzhou city: Zhejiang University.
- Hao, H., Liu, Z., and Yang, S., 2016. Changes in blood lipid levels and clinical significance in patients with intrahepatic cholestasis of pregnancy Chinese. Journal of Clinical Obstetrics and Gynecology, 17 (4), 359–361.
- Hofmann, A.F. and Hagey, L.R., 2008. Bile acids: chemistry, pathochemistry, biology, pathobiology, and therapeutics. Cellular and Molecular Life Sciences, 65 (16), 2461–2483.
- Holland, R.L., 1987. Recurrent intrahepatic cholestasis of pregnancy. South Dakota Journal of Medicine, 40 (4), 9–12. Apr
- Holt, S., et al., 1999. Acute cholestasis-induced renal failure: effects of antioxidants and ligands for the thromboxane A2 receptor. Kidney International, 55 (1), 271–277.
- Kamisako, T. and Adachi, Y., 1995. Marked improvement in cholestasis and hypercholesterolemia with simvastatin in a patient with primary biliary cirrhosis. American Journal of Gastroenterology, 90 (7), 1187–1188.
- Krones, E., et al., 2017. NorUrsodeoxycholic acid ameliorates cholemic nephropathy in bile duct ligated mice. Journal of Hepatology, 67 (1), 110–119.
- Kurihara, T., et al., 1993. Experimental use of pravastatin in patients with primary biliary cirrhosis associated with hypercholesterolemia. Clinical Therapeutics, 15 (5), 890–898.
- Lammert, F., et al., 2000. Intrahepatic cholestasis of pregnancy: molecular pathogenesis, diagnosis and management. Journal of Hepatology, 33 (6), 1012–1021.
- Li, C. and Li, Z., 2019. The effect of individualized diet guidance combined with oral hypoglycemic drugs on glucose and lipid metabolism in pregnant women with diabetes and perinatal prognosis. Chinese Journal of Clinical Obstetrics and Gynecology, 20 (3), 243–244.
- Li, H., 2019. Analysis of serum bile acid profile and pregnancy outcomes in intrahepatic cholestasis of pregnancy. Chongqing city: Chongqing Medical University.
- Li, T. and Chiang, J.Y.L., 2017. Bile acid-induced liver injury in cholestasis. Springer International Publishing, 143–172.
- Liu, H., Ao, D., and Wu, Y., 2009. Exploration of the relationship between serum total bile acids and blood lipids. Hainan Medicine, 20 (10), 125.
- Liu, K., 2016. Clinical analysis of 456 cases of intrahepatic cholestasis of pregnancy and hypercholeacidemia of pregnancy. Chongqing city: Chongqing Medical University.
- Lu, Y., et al., 2021. Establishment of trimester-specific reference intervals of serum lipids and the associations with pregnancy complications and adverse perinatal outcomes: a population-based prospective study. Annals of Medicine, 53 (1), 1632–1641.
- Majsterek, M., et al., 2022. Bile acids in intrahepatic cholestasis of pregnancy. Diagnostics, 12 (11), 2746.
- Martínez-Cecilia, D., et al., 2016. Oxidative stress influence on renal dysfunction in patients with obstructive jaundice: a case and control prospective study. Redox Biology, 8, 160–164.
- McKenzie-Sampson, S., et al., 2018. Gestational diabetes and risk of cardiovascular disease up to 25 years after pregnancy: a retrospective cohort study. Acta Diabetologica, 55 (4), 315–322.
- Monrose, E., et al., 2021. Burden of future liver abnormalities in patients with intrahepatic cholestasis of pregnancy. American Journal of Gastroenterology, 116 (3), 568–575.
- O’Brien, A., et al., 2016. Bile duct-ligated mice exhibit multiple phenotypic similarities to acute decompensation patients despite histological differences. Liver International, 36 (6), 837–846.
- Ommati, M.M., et al., 2019. Cholestasis-associated reproductive toxicity in male and female rats: the fundamental role of mitochondrial impairment and oxidative stress. Toxicology Letters, 316, 60–72.
- Ommati, M.M., et al., 2020. Betaine alleviates cholestasis-associated renal injury by mitigating oxidative stress and enhancing mitochondrial function. Biologia, 76 (1), 351–365.
- Ommati, M.M., et al., 2021a. Pentoxifylline mitigates cholestasis-related cholemic nephropathy. Clinical and Experimental Hepatology, 7 (4), 377–389.
- Ommati, M.M., et al., 2021b. Mitigation of cholestasis-associated hepatic and renal injury by edaravone treatment: evaluation of its effects on oxidative stress and mitochondrial function. Liver Research, 5 (3), 181–193.
- Ommati, M.M., et al., 2021c. Metformin alleviates cholestasis-associated nephropathy through regulating oxidative stress and mitochondrial function. Liver Research, 5 (3), 171–180.
- Ommati, M.M., et al., 2023a. Cholestasis-associated pulmonary inflammation, oxidative stress, and tissue fibrosis: the protective role of the biogenic amine agmatine. Pharmacology, 108 (4), 379–393.
- Ommati, M.M., et al., 2023b. Pulmonary inflammation, oxidative stress, and fibrosis in a mouse model of cholestasis: the potential protective properties of the dipeptide carnosine. Naunyn-Schmiedeberg’s Archives of Pharmacology, 396 (6), 1129–1142.
- Panaitescu, A.M., et al., 2021. Pregnancy complications can foreshadow future disease-long-term outcomes of a complicated pregnancy. Medicina, 57 (12), 1320.
- Perez, M.J. and Briz, O., 2009. Bile-acid-induced cell injury and protection. World Journal of Gastroenterology, 15 (14), 1677–1689.
- Piechota, J. and Jelski, W., 2020. Intrahepatic cholestasis in pregnancy: review of the literature. Journal of Clinical Medicine, 9 (5), 1361.
- Reyes, H. and Sjövall, J., 2000. Bile acids and progesterone metabolites in intrahepatic cholestasis of pregnancy. Annals of Medicine, 32 (2), 94–106.
- Sheng, Y., Guo, J., and Chen, Z., 2017. Exploration of the relationship between late pregnancy blood lipid levels and pregnancy complications. Journal of Changzhi Medical College, 31 (3), 207–209.
- Stamp, D., and Jenkins, G., 2008. An overview of bile-acid synthesis, chemistry and function. In: Jenkins GJ, Hardie L, editors. Bile Acids: Toxicology and Bioactivity: The Royal Society of Chemistry. p. 1–13.
- Stojakovic, T., et al., 2007. Atorvastatin in patients with primary biliary cirrhosis and incomplete biochemical response to ursodeoxycholic acid. Hepatology, 46 (3), 776–784.
- Sulaiman, W.N.W., et al., 2016. Does high-density lipoprotein protect vascular function in healthy pregnancy? Clinical Science (London, England: 1979), 130 (7), 491–497.
- Walker, I.A., Nelson-Piercy, C., and Williamson, C., 2002. Role of bile acid measurement in pregnancy. Annals of Clinical Biochemistry, 39 (Pt 2), 105–113.
- Wen, C. and Liu, M., 2015. Blood lipid changes and clinical significance in intrahepatic cholestasis of pregnancy. Modern Medicine and Health, 31 (11), 1617–1618.
- Wensink, M.J., 2016. The risk of infant and fetal death by each additional week of expectant management in intrahepatic cholestasis of pregnancy by gestational age: various objections. American Journal of Obstetrics and Gynecology, 215 (6), 807–808.
- Williamson, C. and Geenes, V., 2014. Intrahepatic cholestasis of pregnancy. Obstetrics and Gynecology, 124 (1), 120–133.
- Zeng, G., Zou, W., and Liu, C., 2021. Study on the characteristics of lipidmetabolism in pre eclampsia, gestational diabetes and intrahepaticcholestasis of pregnancy. Modern Pharmaceutical Applications in China, 15 (8), 78–80.
- Zhang, J., 2018. The effect of total bile acid levels on pregnancy outcomes and perinatal outcomes in pregnant women with intrahepatic cholestasis of pregnancy. Maternal and Child Health Care in China, 33 (13), 2939–2941.
- Zheng, Y. and Zhai, G., 2013. Exploration of pregnancy and abnormal lipid metabolism. Medical Review, 19 (21), 3874–3876.
- Zhong, H., 2004. The clinical significance of elevated serum total bile acids in late pregnancy. Anhui Medicine, 2004 (4), 270.
- Zhou, J., 2019. Analysis of the relationship between abnormal blood lipids in the third trimester of pregnancy and maternal and fetal outcomes in patients with gestational diabetes. Modern Practical Medicine, 31 (1), 75–77.
- Zhou, S., Li, Y., and Lin, J., 2020. The level of blood sugar and blood lipid in pregnant women with diabetes and their influence on pregnancy outcome. Chinese Medical Innovation, 17 (22), 48–51.