

Abstract
This study aimed to compare the tissue damage caused by barbed sutures and conventional sutures using scanning electron microscopy (SEM). Porcine myocardium was incised and sutured using different thread types: barbed suture, (STRATAFIX® Spiral PDS PLUS) and conventional sutures, (VICRYL® and PDS Plus®). Needle hole shapes were examined at magnifications of 30×–100×. VICRYL® suture damaged the tissue and created large gaps around the needle holes. The tissue around the needle holes was smoother and less damaged in the single suture ligations with PDS®; however, a large gap had formed. In the continuous suture with STRATAFIX®, the tissue around the needle holes was significantly smoother and minimally damaged, with no noticeable gaps around the needle holes. Barbed sutures reduced the load on needle holes and minimised tissue damage owing to the dispersion of traction forces by the barbs compared with conventional sutures.
Introduction
Barbed sutures are obtained using a suture thread with barbed projections. There is no need to pull the thread with barbed suture as with the traditional needle and thread, as the barbs on the suture thread hold the wound together, enabling faster and easier suturing (Greenberg and Goldman Citation2013). Barbed sutures have been introduced in the surgical and aesthetic facial plastic surgery fields (Murtha et al. Citation2006, Ruff Citation2006), and their use in obstetrics and gynaecology surgery has increased in recent years (Greenberg and Einarsson Citation2008). Although strong tension is necessary when suturing the myometrium in caesarean section or uterine myomectomy, the possibility of the myometrium tearing owing to the excessive tension increases the risk of bleeding. A few studies indicate that barbed sutures not only decreased suturing time but also reduced the need for additional haemostatic sutures in caesarean sections and decreased blood loss in total laparoscopic myomectomy (Bogliolo et al. Citation2015, Gardella et al. Citation2018, Agarwal et al. Citation2021, Raischer et al. Citation2022).
In barbed sutures, there is a potential risk of tissue damage due to the barbs backtracking; however, no studies have verified this. Therefore, we evaluated the differences in tissue damage caused by barbed and conventional suture materials used for uterine closure using scanning electron microscopy (SEM).
Methods
Sample preparation
Porcine myocardium was purchased by Johnson & Johnson from a company licenced to provide animal tissues for medical experimentation and provided free of charge to us for suture practice. Porcine myocardium was used because it was more readily available than other animals and because of all muscular tissues, the thickness of porcine myocardium is similar to that of the myometrium of the human uterus.
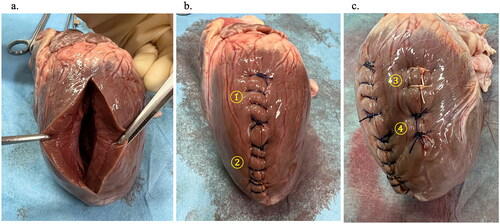
Porcine myocardium was incised with a scalpel and then sutured using different types of threads: Barbed thread, STRATAFIX® Spiral PDS PLUS, was used for continuous suturing, while conventional threads, VICRYL® and PDS Plus®, were used for continuous and single ligature suturing and for single ligature suturing, respectively, (all sizes: 0; ETHICON, Johnson, & Johnson) (). VICRYL® and PDS Plus® have traditionally been used for caesarean sections and myomectomy at our institution. The suturing was performed by a single operator with a tension equivalent to that of conventional surgical procedures.
Figure 1. Suturing and ligature procedures on porcine myocardium. a. Porcine myocardium incised with a scalpel. b, c. Porcine myocardium sutured using different types of threads. 1. Continuous suture with VICRYL®. 2. Continuous suture with STRATAFIX® Spiral PDS PLUS. 3. Single suture ligation with VICRYL®. 4. Single suture ligation with PDS Plus®.
SEM
The sutured porcine myocardium was cut into 1 cm squares, fixed overnight in 0.1 mol/l phosphate buffer (pH 7.4) with 2.5% glutaraldehyde. The specimens were then dehydrated through a graded ethanol series (Okada et al. Citation2017). The samples were then incubated in t-butyl alcohol at room temperature. After the t-butyl alcohol had solidified, it was freeze-dried. The specimens were coated with osmium and examined using SEM (S-4800, Hitachi).
Quantification of tissue damage
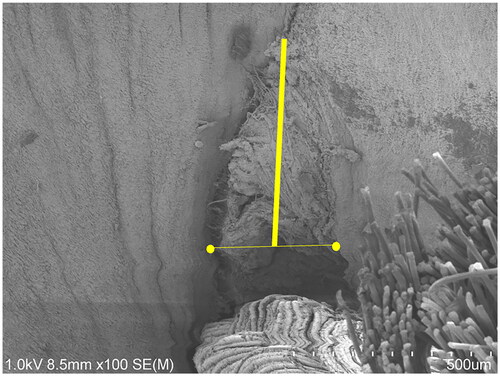
First, we observed the shape of each needle hole using images with magnifications ranging from 30× to 100×. Next, we measured the length of the line connecting the top of the crevice and the centre of the line drawn between the two ends of the base of the muscle crevice (). The length of the gaps was measured at four different locations for each material, and the median values were compared. For statistical analysis, Mann-Whitney U test was performed using SPSS version 23 (IBM, Armonk, New York, USA). A p value of <0.05 was considered statistically significant.
Figure 2. Gap measuring. The length of the line connecting the top of the crevice and the centre of the line drawn between the two ends of the base of the muscle crevice (thick yellow line) was measured.
Results
shows the SEM images of the needle holes for each suture. In the continuous sutures with VICRYL®, the tissues were torn, large gaps were formed at the ligated area (a-1), and significant tissue damage around the needle holes and fraying of the thread were also observed at the midpoint (a-2). In the single suture ligations with VICRYL®, significant tissue damage around the needle holes and a large gap (b) were observed. In the single suture ligations with PDS Plus®, the tissues around the needle holes appeared smoother and less damaged compared with the single suture ligations with VICRYL®. However, large gaps were still observed (c). In the single suture ligations, the surrounding tissues were strongly pulled towards the ligated area (b, c). STRATAFIX® Spiral PDS PLUS uses a loop configuration at the end of the suture, eliminating the need for traditional ligatures (d-1 and d-2; starting points of the sutures). The tissues around the needle holes were noticeably smoother with minimal damage. Additionally, no gaps were observed at the initial insertion site (d-2). Even at the midpoint, the tissues were extremely smooth, and the surrounding tissue was raised owing to barb catching (d-3, d-4). The median lengths of the gaps were as follows: continuous suture and single suture ligation with VICRYL®, 504 μm and 550 μm, respectively; single suture ligation with PDS Plus®, 537 μm; and continuous suture with STRATAFIX® Spiral PDS Plus, 112 μm (). Although the length was not significantly different between the holes, the barbed suture was smoother with smaller fissures.
Figure 3. SEM images of each suture type. a. Continuous sutures with VICRYL®. b. Single suture ligation with VICRYL®. c. Single suture ligation with PDS Plus®. d. Continuous suture with STRATAFIX® Spiral PDS PLUS. The images in the bottom row are enlarged, focusing on the yellow circled area in the top row.
SEM: scanning electron microscopy
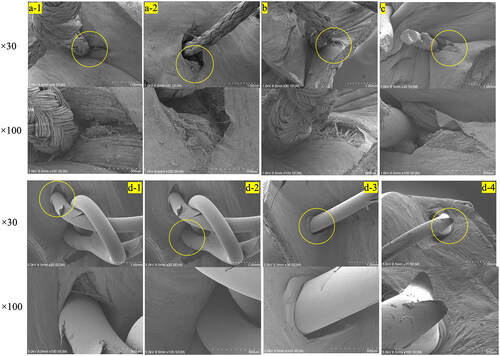
Table 1. Comparing the lengths of the gaps.
Discussion
We investigated the effects of the types of sutures using different threads on tissues using SEM. Although a few reports have compared types of sutures using SEM, this is the first study to observe the microstructure of barbed sutures within muscle tissue. In this study, we found that barbed sutures caused less damage to the surrounding tissue than conventional sutures.
Several systematic reviews have reported on the usefulness of barbed sutures in obstetrics and gyneacology (Bogliolo et al. Citation2015, Gardella et al. Citation2018, Agarwal et al. Citation2021, Raischer et al. Citation2022). It has been reported that particularly in the case of caesarean sections, there was a significant reduction in the need for additional sutures for haemostasis (Raischer et al. Citation2022). Conventional sutures often lead to tissue tearing owing to the concentration of traction forces, especially at the knot site, which can sometimes lead to bleeding from needle holes and necessitate additional sutures for haemostasis. During a caesarean section, the uterine muscles are soft, making tissue tearing especially prone to occur because of suturing. Barbed suture may minimise damage to needle holes and reduce bleeding by distributing the suturing pressure across the entire length of the thread by securing the tissue through each barb. Our study showed that the microstructure of the tissue around the barbed suture threads was smooth and had fewer tears. Tissue damage caused by the barbs did not appear to be a significant issue. Based on this result, the effect is further enhanced in the uterus, which has become soft owing to pregnancy, and a reduction in the risk of tissue tearing and associated bleeding can be expected. Barbed sutures are considered suitable for suturing organs, such as the uterus, which require strong traction during suturing while being prone to bleeding.
Only a few studies have used SEM to observe barbed sutures, and many of them have primarily investigated the ease of bacterial adhesion (Morris et al. Citation2017). According to these studies, barbed sutures exhibit reduced bacterial adhesion, contributing to reduced postoperative complications. One issue to be aware of when using this beneficial thread is post-operative bowel obstruction: there have been several reports of bowel obstruction following barbed suture, requiring measures such as the shortening the thread tails and use of the antiadhesive barriers (Guglielmo et al. Citation2021).
Our study has three limitations. One is that the tissues of porcine myocardium and uterine muscle are different. Thus, the impact on the needle holes may be different, especially during caesarean sections, as the uterine muscle contracts rapidly within a short period, which can introduce different effects. However, there is currently no suturing model that accurately mimics this scenario. The second limitation is the inability to measure the traction force during suturing. Although suturing was performed by a single operator with appropriate tension to approximate tissue apposition, the sutures might exert varying levels of traction force. If several surgeons use different tissues or suturing methods, different results may be achieved. The third is that tissues tend to shrink during dehydration; therefore, the size of the needle holes may differ from the actual size.
In conclusions, barbed sutures may reduce the load on needle holes and minimise tissue damage owing to the dispersion of traction forces by the barbs. Therefore, the use of barbed suture could reduce bleeding during suturing, especially from the needle holes. This study provides valuable insights into the benefits of barbed sutures and encourages further exploration of their applications in medical procedures.
Ethical consideration
Not applicable.
Authors’ contribution
T.S. Conceptualisation, methodology, data curation, formal analysis and writing original draft. H.O. Methodology and data curation. M.I and T.F. Supervision
Acknowledgements
We extend our gratitude to Chihiro Takada who contributed to the sample preparation and SEM observations.
Disclosure statement
M. I. received lecture honoraria from Ethicon (Tokyo, Japan). The other authors have no conflicts of interest to declare.
Data availability statement
Raw data were generated at Gifu University Graduate School of Medicine. Derived data supporting the findings of this study are available from the corresponding author T.S on request.
Additional information
Funding
References
- Agarwal, S., et al., 2021. Barbed vs conventional suture at cesarean delivery: a systematic review and meta-analysis. Acta Obstetricia et Gynecologica Scandinavica, 100 (6), 1010–1018.
- Bogliolo, S., et al., 2015. Barbed suture in minimally invasive hysterectomy: a systematic review and meta-analysis. Archives of Gynecology and Obstetrics, 292 (3), 489–497.
- Gardella, B., et al., 2018. What is the role of barbed suture in laparoscopic myomectomy? A meta-analysis and pregnancy outcome evaluation. Gynecologic and Obstetric Investigation, 83 (6), 521–532.
- Greenberg, J.A. and Einarsson, J.I., 2008. The use of bidirectional barbed suture in laparoscopic myomectomy and total laparoscopic hysterectomy. Journal of Minimally Invasive Gynecology, 15 (5), 621–623.
- Greenberg, J.A. and Goldman, R.H., 2013. Barbed suture: a review of the technology and clinical uses in obstetrics and gynecology. Reviews in Obstetrics and Gynecology, 6 (3–4), 107–115.
- Guglielmo, S., et al., 2021. Case report: bowel occlusion following the use of barbed sutures in abdominal surgery. A single-center experience and literature review. Front Surg, 20 (8), 626505.
- Morris, M.R., et al., 2017. Decreased bacterial adherence, biofilm formation, and tissue reactivity of barbed monofilament suture in an in vivo contaminated wound model. The Journal of Arthroplasty, 32 (4), 1272–1279.
- Murtha, A.P., et al., 2006. Evaluation of a novel technique for wound closure using a barbed suture. Plastic and Reconstructive Surgery, 117 (6), 1769–1780.
- Okada, H., et al., 2017. Three-dimensional ultrastructure of capillary endothelial glycocalyx under normal and experimental endotoxemic conditions. Critical Care, 21 (1), 261.
- Raischer, H.B., et al., 2022. Knotless barbed versus conventional suture for closure of the uterine incision at cesarean delivery: a systematic review and meta-analysis. Journal of Minimally Invasive Gynecology, 29 (7), 832–839.
- Ruff, G., 2006. Technique and uses for absorbable barbed sutures. Aesthetic Surgery Journal, 26 (5), 620–628.