

Abstract
Background
This study examined the improvement of dysmenorrhoea and menorrhagia after uterine artery embolisation (UAE) in women with symptomatic adenomyosis and identified factors that could predict the improvement of dysmenorrhoea and menorrhagia.
Methods
This retrospective study included women with adenomyosis who underwent bilateral UAE between December 2014 and December 2016. The percentage of the volume of the absence of contrast enhancement on T1-weighted images was evaluated 5–7 days after UAE. A receiver operating characteristic (ROC) analysis was used to determine a cut-off point and predict the improvement of dysmenorrhoea and menorrhagia.
Results
Forty-eight patients were included. At 24 and 36 months after UAE, the improvement rates for dysmenorrhoea and menorrhagia were 60.4% (29/48) and 85.7% (30/35), and the recurrence rates were 19.4% (7/36) and 9.1% (3/33), respectively. Only the percentage of the volume of the absence of contrast enhancement on T1-weighted images was associated with the improvement of dysmenorrhoea (p = 0.001, OR = 1.051; 95% CI: 1.02–1.08) and menorrhagia (p = 0.006, OR = 1.077; 95% CI: 1.021–1.136). When the cut-off value of the ROC analysis was 73.1%, sensitivity, specificity, positive predictive value, and negative predictive value for the improvement of dysmenorrhoea were 58.6%, 94.7%, 94.4%, and 60%, while they were 58.9%, 80%, 100%, 100%, and 45.5% for the improvement of dysmenorrhoea.
Conclusion
Bilateral UAE for symptomatic adenomyosis led to good improvement of dysmenorrhoea and menorrhagia. The percentage of the volume of the absence of contrast enhancement on T1-weighted images of the uterus in postoperative magnetic resonance imaging might be associated with the improvement of dysmenorrhoea and menorrhagia.
PLAIN LANGUAGE SUMMARY
This study examined the improvement of dysmenorrhoea and menorrhagia after uterine artery embolisation in women with symptomatic adenomyosis and identified factors that could predict the improvement of dysmenorrhoea and menorrhagia. This retrospective study included women with adenomyosis who underwent uterine artery embolisation. A total of 48 patients were included. Only the percentage of the volume of the absence of contrast enhancement on T1-weighted images was associated with improvement of dysmenorrhoea and menorrhagia. Bilateral uterine artery embolisation for symptomatic adenomyosis led to good improvement. The percentage of the volume of the absence of contrast enhancement on images in postoperative T1-weighted magnetic resonance imaging of the uterus might be associated with the improvement of dysmenorrhoea and menorrhagia.
Introduction
Adenomyosis is a common gynecological disease characterised by an enlarged uterus due to the invasion of the myometrium by the endometrium. It often occurs in women aged 30–50, causing heavy menstrual bleeding, dysmenorrhoea, and infertility (Templeman et al. Citation2008, Senturk and Imamoglu Citation2015, Struble et al. Citation2016, Abbott Citation2017). Traditional hormonal therapy creates a micro-environment with low oestrogen and high progesterone (Shaaban et al. Citation2015, Osuga et al. Citation2017); however, traditional hormonal therapy has shortcomings, including poor response, long-term side effects, and symptom recurrence after withdrawal (Tsui et al. Citation2014, Pontis et al. Citation2016). Furthermore, the standard surgical treatment for adenomyosis is hysterectomy, but it is unacceptable for patients requiring fertility preservation (Soave et al. Citation2018). The most important challenge in the treatment of adenomyosis is relieving the clinical symptoms (dysmenorrhoea and menorrhagia) while preserving fertility.
Uterine artery embolisation (UAE) has a certain prospect in the treatment of adenomyosis due to its advantages of minimal invasiveness, quick recovery, few complications, and preservation of the uterus (Kim et al. Citation2007, Bratby and Walker Citation2009). While the short-term results of UAE for symptomatic adenomyosis are promising, the mid-to-long-term efficacy remains to be confirmed (Popovic et al. Citation2011, De Bruijn et al. Citation2017b). Previous short-term follow-up studies reported that magnetic resonance imaging (MRI) features could be predictors of disease prognosis after UAE (Kim et al. Citation2011, Jung et al. Citation2012). Nevertheless, the factors associated with mid- to long-term symptom relief after UAE for adenomyosis are unclear (Popovic et al. Citation2011, Zhou et al. Citation2016, Dessouky et al. Citation2019).
The present study examined the improvement of dysmenorrhoea and menorrhagia after UAE in women with symptomatic adenomyosis and the relevant factors that could be used to predict these improvements.
Methods
Study design and patients
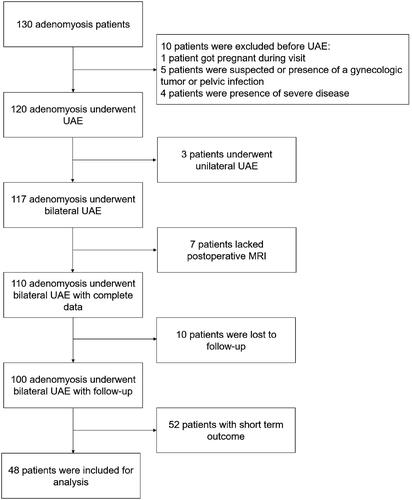
Between December 2014 and December 2016, 130 patients diagnosed with adenomyosis based on typical clinical symptoms (e.g. progressive dysmenorrhoea and/or menorrhagia) and magnetic resonance imaging (MRI) findings of adenomyosis sought for UAE at our hospital. For symptomatic adenomyosis, the criteria for performing UAE were conservative treatment failure and preservation of fertility. Among 130 patients with adenomyosis, 1 patient got pregnant during visit and abandoned UAE therapy. Five patients who were suspected or presence of a gynaecologic tumour or pelvic infection did not receive UAE therapy. The exclusion of four additional patients were warranted due to the presence of severe disease that contraindicated UAE treatment. 117 patients underwent successful bilateral UAE; the remaining 3 patients underwent unilateral UAE, given challenges in catheterising one of uterine artery. The postoperative MRI was not performed on seven patients, leading to incomplete data. Ten patients were lost to follow-up. Fifty-two patients had short-term clinical outcome (less than 36 months). A total of 48 patients completed a mid-to-long term follow-up. shows the STROBE flow chart of patients included in study analysis.
Figure 1. STROBE flow chart of patients included in study analysis.
MRI
All patients underwent pre-procedural MRI 4–7 days before UAE and follow-up MRI 5–7 days after UAE, as per routine practice. Pelvic MRI was performed using a 3.0-T Magnetom Trio scanner (Siemens Healthcare, Erlangen, Germany) and a phased-array body coil. All patients underwent axial and sagittal fast spin-echo T2WI and contrast-enhanced sagittal T1WI. Contrast-enhanced MRI was performed 2 min after intravenous gadolinium infusion (GE Healthcare, County Cork, Ireland) at 0.1 mmol/kg body weight.
Two radiologists (YG and MJL, each with >20 years of experience in pelvic MRI) working together confirmed the diagnosis of adenomyosis and determined the category of adenomyosis by analysing the following parameters: 1) morphological type of adenomyosis (diffuse or focal) and 2) pure adenomyosis or adenomyosis with myomas. The MRI diagnostic criteria for adenomyosis included diffuse or focal thickening of the junction zone (>12 mm in thickness), an ill-defined low signal-intensity area of the myometrium, or punctuated high signal-intensity myometrial foci (Byun et al. Citation1999, Reinhold et al. Citation1999).
The junction zone thickness was measured at its widest aspect on sagittal MRI (). The uterine volume before and after UAE was measured on MRI as follows: volume = length × width × height × 0.523 for a prolate ellipse (Orsini et al. Citation1984). The volume of the absence of contrast enhancement on T1-weighted images after UAE was measured by the equation for a prolate ellipse. The percentage of the absence of contrast enhancement was defined as the volume of the absence of contrast enhancement on T1-weighted images divided by the postoperative volume of the uterus measured on follow-up MRI (). For accuracy, the measurement procedure was repeated three times, and the average values were calculated.
Figure 2. A 36-year-old patient with adenomyosis. The posterior wall of the uterus was locally thickened, and the muscle layer signal was reduced (white arrows). The thickness of the junctional zone is defined as the maximum thickness of the junctional zone in the sagittal position of T2WI (white line).
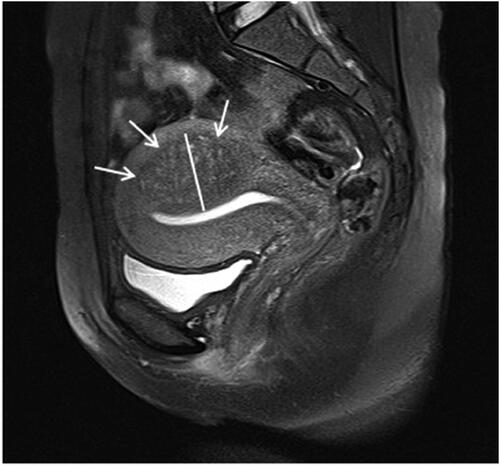
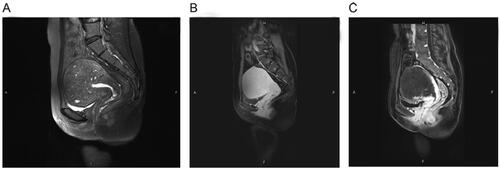
Figure 3. A 35-year-old woman with symptomatic adenomyosis. (A) Pre-procedural sagittal T2WI showing junctional zone thickening of the uterus with punctate high signal intensity myometrial foci. (B) Pre-procedural sagittal T2WI showing homogeneous enhancement of the adenomyosis lesion. (C) Follow-up gadolinium-enhanced T1-weighted MRI at 4 days after UAE showing the non-enhancement area. The percentage of the absence of contrast enhancement was 0.853.
Uterine arterial embolisation
All procedures in this study were conducted by the same experienced interventional radiologist with >10 years of experience in UAE. The common right femoral access under local anaesthesia was used in all patients. A 5-F Yashiro catheter (Cook, Bloomington, IN, USA) was distally advanced into the uterine artery. The primary embolic agent was trisacryl gelatine microspheres (Biosphere Medical, Rockland, MA, USA), with a diameter of 500–700 μm or 700–900 μm. Because the gaps among the microspheres can allow blood flow recovery and embolisation failure, a small amount of gelatine sponge strip (Jingling Pharmaceutical Co., Ltd., Nanjing, Jiangsu, China) was added to reinforce embolisation. Embolisation was performed until the blood flow in the ascending uterine artery was completely stopped.
Outcomes
Follow-up was routinely conducted at the outpatient clinic or via telephone at 6, 12, 24, and 36 months after UAE. The degree of dysmenorrhoea was classified according to the visual analog scale (VAS) scores (or verbal descriptor scale 1–10 when over the phone), where 0–3 indicated mild, 4–7 moderate, and 8–10 severe. The degree of menorrhagia was classified according to the number of sanitary pads in one menstrual cycle as normal (0–19 pads needed in one menstrual cycle), large (20–30 pads needed), and vast (>30 pads needed). The alleviation of dysmenorrhoea and menorrhagia after UAE was evaluated. A reduction of ≥50% in the VAS dysmenorrhoea score after UAE was defined as alleviation, and <50% was regarded as no alleviation (Zheng et al. Citation2018). The same principle was applied for menorrhagia, which was evaluated based on the number of sanitary pads used in the period following UAE compared with the period preceding the operation. Amenorrhoea was defined as three consecutive menstrual periods missed (Stokes et al. Citation2010, Scheurig-Muenkler et al. Citation2011). Recurrence was defined as symptoms reaching the alleviation criterion after UAE but gradually increasing to reach the no-alleviation criterion or when symptoms reappeared according to the patient’s judgement 6 months after UAE.
Statistical analysis
Continuous variables conforming to the normal distribution (according to the Kolmogorov-Smirnov test) were described as means ± standard deviations, while those not conforming to the normal distribution were described as medians and quartile ranges. Univariable logistic regression was used to identify predictors of the mid-to-long-term therapeutic response after UAE. Receiver operating characteristic (ROC) curve analysis was used to determine the cut-off point of the absence of contrast enhancement percentage to predict the mid-to-long-term therapeutic response. SPSS 24.0 (IBM, Armonk, NY, USA) was used for statistical analysis. p < 0.05 indicated a statistically significant difference.
Reporting statement declaration
The reporting of this study complies with the STROBE checklist (Von Elm et al. Citation2008).
Results
Characteristics of the patients
Forty-eight patients with a mean age of 37.3 ± 5.6 years were included in the study. Their demographic data are shown in . Thirty women (62.5%) had diffuse adenomyosis, and 18 (37.5%) had focal adenomyosis. Ten women (20.8%) had myomas.
Table 1. Demographic characteristics of the patients.
Bilateral UAE was technically successful in all patients, and the 36-month follow-up was completed. Six patients (12.5%) with a mean age of 41 (35–46) developed permanent amenorrhoea immediately after UAE. Three patients (6.3%; 36, 45, and 45 years of age) developed amenorrhoea 12 months after UAE. Temporary amenorrhoea occurred in three patients (6.3%; 28, 32, and 40 years of age) within 12–24 months after UAE. During follow-up, one patient (2.1%) underwent a hysterectomy 13 months after UAE (the symptoms of dysmenorrhoea and heavy menstruation were uncontrolled). Six patients (12.5%) required additional treatment for recurrence or lack of improvement at a median of 24 (19-34) months after UAE. There were no cases of postoperative pregnancies.
A contrast-enhanced MRI was performed 5-7 days after UAE. The median uterine volume increased from 266.0 cm3 (169.2–401.3 cm3) to 291.9 cm3 (183.8–379.5 cm3), and the growth rate of volume was 60.4% (29/48), mainly due to edoema resulting from UAE. The median volume of the absence of contrast enhancement on postoperative T1-weighted images was 159.6 cm3 (107.6–260.1 cm3). The median percentage of the volume of the absence of contrast enhancement on T1-weighted images over the volume of the postoperative uterus was 67.2% (37.3%–79.3%). Two patients (4.2%, 28, and 36 years of age) had 0% non-enhancement volume and no improvement at follow-up. Figure S1 shows the distribution of the patients according to the percentage of the volume of the absence of contrast enhancement on T1-weighted images over the volume of the postoperative uterus.
Improvement in dysmenorrhoea and menorrhagia
Six months after UAE, dysmenorrhoea was alleviated in 36 patients (75%). Twelve months after UAE, 35 patients (72.9%) experienced improvement, and the recurrence rate was 2.8% (1/36). Twenty-nine (60.4%) patients experienced mid-to-long-term (24-36 months) alleviation of dysmenorrhoea, and the recurrence rate was 19.4% (7/36) (Table S1). Seven patients with recurrence underwent laparoscopic resection of adenomyosis (n = 4), percutaneous microwave ablation (n = 1), high-intensity focused ultrasound (HIFU) (n = 1), and HIFU combined with a levonorgestrel-releasing intrauterine device (n = 1).
Among the 48 patients, 35 (72.9%) had menorrhagia before UAE. At 6 months, alleviated menorrhagia was observed in 33 patients (94.3%), while the condition did not improve in two patients (5.7%). At 12 months after UAE, improvement was observed in 31 patients (88.6%), and the recurrence rate was 6.1% (2/33). Thirty patients (85.7%) showed mid-long-term (24–36 months) alleviation of menorrhagia, with a recurrence rate of 9.1% (3/33) (Table S1).
Univariable analysis for dysmenorrhoea and menorrhagia
In the univariable logistic analyses, only the percentage of the volume of the absence of contrast enhancement on T1-weighted images over the volume of the postoperative uterus was associated with the improvement in dysmenorrhoea (p = 0.001, OR = 1.045; 95% CI: 1.017–1.074) (). The AUC for predicting the improvement in dysmenorrhoea was 0.821 (95% CI: 0.705–0.937) (). From the ROC analysis, 73.1% of non-enhancing tissue with respect to total uterine volume was the optimal cut-off value for predicting the mid-long-term improvement in dysmenorrhoea. The cut-off of 73.1% had a sensitivity, specificity, PPV, and NPV of 58.6%, 94.7%, 94.4%, and 60%, respectively.
Figure 4. (A) ROC curve for predicting the mid-term improvement in dysmenorrhoea. (B) ROC curve for predicting the mid-term improvement in menorrhagia.
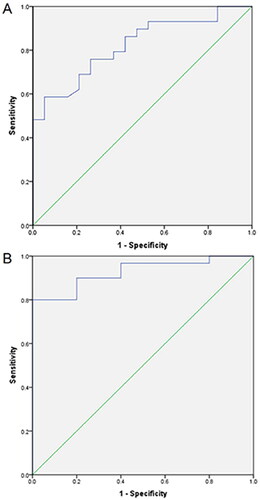
Table 2. Univariable analyses of improvement in dysmenorrhoea at 3 years after UAE.
In the univariable logistic analyses, only the percentage of the volume of the absence of contrast enhancement on T1-weighted images over the volume of the postoperative uterus was significantly associated with the mid-long-term improvement in menorrhagia (p = 0.006, OR = 1.077; 95% CI: 1.021–1.136) (), while age, junctional zone thickness, CA125 before UAE, baseline uterine volume, type of lesion, and myoma were not associated. Therefore, no multivariable analysis could be performed. The AUC for predicting the improvement in menorrhagia was 0.927 (95% CI: 0.834–1) (). From the ROC analysis, 58.9% of non-enhancing tissue with respect to total uterine volume was the optimal cut-off value to predict the mid-long-term improvement in menorrhagia. The cut-off of 58.9% had a sensitivity, specificity, PPV, and NPV of 80%, 100%, 100%, and 45.5%, respectively.
Table 3. Univariable analyses of the improvement in menorrhagia at 3 years after UAE.
Discussion
The results of this study suggested that bilateral UAE for symptomatic adenomyosis led to good mid-to-long-term clinical outcomes. In addition, the percentage of the non-enhanced volume of the uterus in postoperative MRI was associated with the improvement of dysmenorrhoea and menorrhagia. These results might have implications for early counselling and planning optimal management in patients using postoperative MRI.
The most common symptoms of adenomyosis are heavy menstrual bleeding and abdominal pain, accompanied by anaemia, urinary and gastrointestinal symptoms, pregnancy complications, and infertility. Symptomatic adenomyosis significantly burdens public health, quality of life, and social economy (Schrager et al. Citation2022). Radical surgery (hysterectomy) can solve this problem definitively, but many premenopausal women have a desire for fertility (Vitale et al. Citation2020). Like patients with uterine fibroids who can benefit from minimally invasive procedures such as hysteroscopic myolysis (Vitale et al. Citation2023) and non-surgical approaches (De Franciscis et al. Citation2022), patients with adenomyosis expect minimally invasive procedures to resolve serious clinical symptoms. Uterine artery embolisation has shown promising prospects in treating adenomyosis due to various advantages (Kim et al. Citation2007, Bratby and Walker Citation2009). Although many treatments can relieve the symptoms of adenomyosis, the recurrence of symptoms is still the main problem of UAE in the management of adenomyosis. Bratby and Walker (Citation2009) reported that the mid-term recurrence rate of menorrhagia was 54.5%, while the recurrence rate of dysmenorrhoea ranged from 9% to 18%. In this study, the recurrence rates of dysmenorrhoea and menorrhagia were 19.4% and 9.1%, respectively. It could be speculated that different embolisation materials might lead to different mid-to-long-term outcomes after UAE, but these materials need further examination and comparison. The embolisation materials used in the literature are PVA particles of 250–710 μm, with irregular shapes and easy to aggregate. In this study, TGM particles with a diameter of 500–700/700–900 μm were used; they have a hydrophilic surface and a spherical shape that prevent aggregation within the catheter lumen and vasculature, facilitating delivery. Gelatine sponge pledgets were used for secondary supplemental embolisation to reinforce the primary embolisation, which may prolong the ischaemia time of the lesion and cause sufficient necrosis for a better and more lasting improvement. Nevertheless, the type and particle size is controversial and subjective as there is still no sufficient evidence, and different studies used different types/sizes of particles (Mccluggage et al. Citation2000, Pelage et al. Citation2002, Pelage et al. Citation2003, Pelage et al. Citation2005, Gaia et al. Citation2009, Bilhim et al. Citation2011, Poujade et al. Citation2013).
Few studies have reported the factors that predict UAE outcomes. Kim et al. (Citation2011) suggested that dark signal intensity (SI) of adenomyosis (an SI similar to that of the rectus abdominis muscle) was the most favourable predictive factor for UAE on MRI. Jung and colleagues (Citation2012) found that the T2-weighted signal intensity ratio of adenomyosis on preoperative MRI could be used as a predictor for early (mid-term, 18 months) therapeutic response of UAE. Previous studies also reported a correlation between lesion necrosis of adenomyosis and clinical outcomes. Bae et al. (Citation2015) suggested that the percentage of necrosis in patients with adenomyosis after UAE might predict symptom recurrence at the mid-term (range 18–48 months) follow-up, with a cut-off percentage of necrosis of 34.3% (AUC = 0.721). Zheng et al. (Citation2018) reported that complete necrosis was a predictor of good outcomes after UAE and that CA125 and accompanying endometriosis could be used as surrogate markers indicating complete necrosis. A different study (Stokes et al. Citation2010) showed that the blood flow of uterine myomas and normal myometrium disappeared within 1 day after UAE, while the blood flow of normal myometrium gradually recovered within 5–7 days after UAE; however, the myoma tissue still showed no blood supply. Therefore, an MRI review was conducted within 5–7 days after UAE to verify the necrosis of the adenomyosis lesion after a short time after UAE. The present study suggested that patients with >73.1% and >58.9% of the ratio of the volume of the absence of contrast enhancement on T1-weighted images divided by the volume of the postoperative uterus after UAE were more likely to experience improvement in dysmenorrhoea and menorrhagia during a mid-to-long-term follow-up. These results suggest that MRI after UAE might be used as a predictor for mid-term prognosis.
It has been reported that the main advantage of UAE, compared with a hysterectomy, is the potential preservation of fertility (Popovic et al. Citation2011). This view is also supported by De Bruijn et al. (Citation2017a), who reported that 97.9% of patients avoided hysterectomy. Nevertheless, complications such as myometrial necrosis, necrotising endometritis, and permanent amenorrhoea can occur after UAE (Goodwin and Walker Citation1998). The Asherman syndrome has also been reported after UAE (Wang et al. Citation2020). According to a meta-analysis conducted in 2017 (De Bruijn et al. Citation2017b), permanent amenorrhoea was reported in 28 out of 445 patients (6.3%) across 13 studies; all those patients were >40 years. In three other studies (Siskin et al. Citation2001, Lohle et al. Citation2007, Bratby and Walker Citation2009), which involved 62 patients, 13 (20.9%, all >45 years) developed permanent amenorrhoea after UAE. In the present study, permanent amenorrhoea occurred in nine out of 48 patients (18.8%) (median age: 40 years; range: 35–46 years). Permanent amenorrhoea after UAE might result from non-targeted embolisation of the ovaries through utero-ovarian anastomoses and damage to the endometrium. Gelatine sponge pledgets were used to ensure the cessation of blood flow, which may prolong the time of ischaemia and damage, or the blood flow to the ovary. Thus, it is necessary to evaluate the ovary function before UAE and choose appropriate embolic agents according to the utero-ovarian anastomoses shown by DSA. Sheikh et al. (Citation2020) showed that two types of utero-ovarian anastomoses carried an increased risk of ovarian failure after UAE, and protective coiling seems to be an adequate strategy for avoiding ovarian failure. Women aged > 45 years are at a much greater risk of ovarian failure after UAE than women aged < 45 years (Palomo et al. Citation2009, Lanciego et al. Citation2012, Kaump and Spies Citation2013). Nonetheless, young women who desire to preserve their uterus should be cautious with UAE because of the possible occurrence of premature menopause. In the present study, one patient had to undergo a hysterectomy, three patients developed amenorrhoea by 12 months, and three patients had transient amenorrhoea. Therefore, UAE carries some risk of losing fertility. In the present study, no pregnancy was reported by the time this manuscript was written.
This study mainly examined the mid- and long-term efficacy prediction of adenomyosis treatment using UAE for the first time. The present study considered the whole uterus instead of only the lesion, considering that the lesion can become necrotic. In addition, evaluating the whole uterus can provide a better idea of the future dysmenorrhoea in the remaining viable uterus. The absence of enhancement after partial embolisation of the lesion indicated that the lesion was in an ischaemic state, inhibiting the cells, which may be the reason for improving symptoms. Since only the lesion was ischaemic, the normal myometrium blood supply was normal, and patients did not suffer from complications such as uterine ischaemic necrosis.
There are limitations in the present study. First, it was a single-center, retrospective study with a small sample size, not adequate for multivariable analyses. Second, the criteria for improvement and recurrence of menorrhagia relied mainly on subjective patient assessment. Third, indistinct margins of the area of non-enhancement on T1-weighted images could result in inaccurate volume measurement. Fourth, quality of life was not formally assessed and could not be analysed in this study.
In conclusion, our results suggested that bilateral UAE for symptomatic adenomyosis led to good mid-long-term clinical outcomes. Furthermore, the percentage of the volume of the absence of contrast enhancement on T1-weighted images over the volume of the postoperative uterus was associated with symptom improvement. The cut-off points were 73.1% and 58.9% for dysmenorrhoea and menorrhagia, respectively. These results might have implications for early counselling and planning optimal patient management by postoperative MRI.
Ethical approval
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. The study was approved by the Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University ([2018]070). The need for individual consent was waived because of the retrospective nature of the study.
Consent for publication
Not applicable.
Authors’ contributions
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. Siqi Hu: Study design, Data analysis, and Manuscript writing. Wenbo Guo: Study design, Project development, Revised the manuscript. Song Chen: Data analysis. Zhiqiang Wu: Gather data. Wenquan Zhuang: Revised the manuscript. Jianyong Yang: Project development and Revised the manuscript.
Supplemental Material
Download Zip (46.2 KB)Acknowledgments
The authors would like to thank all study participants who were enrolled in this study.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
All data generated or analysed during this study are included in this published article and supplementary information files.
Additional information
Funding
References
- Abbott, J.A., 2017. Adenomyosis and abnormal uterine bleeding (AUB-A)-pathogenesis, diagnosis, and management. Best Practice & Research. Clinical Obstetrics & Gynaecology, 40, 1–10.
- Bae, S.H., et al., 2015. Uterine artery embolization for adenomyosis: percentage of necrosis predicts midterm clinical recurrence. Journal of Vascular and Interventional Radiology, 26 (9), 1290–1296.e2.
- Bilhim, T., et al., 2011. Polyvinyl alcohol particle size for uterine artery embolization: a prospective randomized study of initial use of 350-500 mum particles versus initial use of 500-700 mum particles. Journal of Vascular and Interventional Radiology, 22 (1), 21–27.
- Bratby, M.J. and Walker, W.J., 2009. Uterine artery embolisation for symptomatic adenomyosis–mid-term results. European Journal of Radiology, 70 (1), 128–132.
- Byun, J.Y., et al., 1999. Diffuse and focal adenomyosis: MR imaging findings. Radiographics: a Review Publication of the Radiological Society of North America, Inc, 19 Spec No (suppl_1), S161–S70.
- De Bruijn, A. M., et al., 2017a. Uterine artery embolization for symptomatic adenomyosis: 7-year clinical follow-up using UFS-Qol questionnaire. CardioVascular and Interventional Radiology, 40 (9), 1344–1350.
- De Bruijn, A.M., et al., 2017b. Uterine artery embolization for the treatment of adenomyosis: a systematic review and meta-analysis. Journal of Vascular and Interventional Radiology, 28 (12), 1629–1642.e1.
- De Franciscis, P., et al., 2022. Hysteroscopic and ultrasonographic evaluation of ulipristal acetate treatment for symptomatic myomas in premenopausal women: a prospective study. Minimally Invasive Therapy & Allied Technologies:: official Journal of the Society for Minimally Invasive Therapy, 31 (3), 435–440.
- Dessouky, R., et al., 2019. Management of uterine adenomyosis: current trends and uterine artery embolization as a potential alternative to hysterectomy. Insights into Imaging, 10 (1), 48.
- Gaia, G., et al., 2009. Menses recovery and fertility after artery embolization for PPH: a single-center retrospective observational study. European Radiology, 19 (2), 481–487.
- Goodwin, S.C. and Walker, W.J., 1998. Uterine artery embolization for the treatment of uterine fibroids. Current Opinion in Obstetrics & Gynecology, 10 (4), 315–320.
- Jung, D.C., et al., 2012. Prediction of early response to uterine arterial embolisation of adenomyosis: value of T2 signal intensity ratio of adenomyosis. European Radiology, 22 (9), 2044–2049.
- Kaump, G.R. and Spies, J.B., 2013. The impact of uterine artery embolization on ovarian function. Journal of Vascular and Interventional Radiology, 24 (4), 459–467.
- Kim, M.D., et al., 2007. Long-term results of uterine artery embolization for symptomatic adenomyosis. American Journal of Roentgenology, 188 (1), 176–181.
- Kim, M.D., et al., 2011. Uterine artery embolization for symptomatic adenomyosis: a new technical development of the 1-2-3 protocol and predictive factors of MR imaging affecting outcomes. Journal of Vascular and Interventional Radiology, 22 (4), 497–502.
- Lanciego, C., et al., 2012. Utero-ovarian anastomoses and their influence on uterine fibroid embolization. Journal of Vascular and Interventional Radiology, 23 (5), 595–601.
- Lohle, P.N., et al., 2007. Uterine artery embolization for symptomatic adenomyosis with or without uterine leiomyomas with the use of calibrated tris-acryl gelatin microspheres: midterm clinical and MR imaging follow-up. Journal of Vascular and Interventional Radiology, 18 (7), 835–841.
- Mccluggage, W.G., et al., 2000. Pathologic features of uterine leiomyomas following uterine artery embolization. International Journal of Gynecological Pathology: official Journal of the International Society of Gynecological Pathologists, 19 (4), 342–347.
- Orsini, L.F., et al., 1984. Pelvic organs in premenarcheal girls: real-time ultrasonography. Radiology, 153 (1), 113–116.
- Osuga, Y., Fujimoto-Okabe, H. and Hagino, A., 2017. Evaluation of the efficacy and safety of dienogest in the treatment of painful symptoms in patients with adenomyosis: a randomized, double-blind, multicenter, placebo-controlled study. Fertility and Sterility, 108 (4), 673–678.
- Palomo, M.C.E., et al., 2009. P587 Amenorrhea after uterine fibroid embolization in women under age 45 and women over age 45. International Journal of Gynecology & Obstetrics, 107 (S2), S579–S580.
- Pelage, J.P., et al., 2005. Midterm results of uterine artery embolization for symptomatic adenomyosis: initial experience. Radiology, 234 (3), 948–953.
- Pelage, J.P., et al., 2002. Uterine artery embolization in sheep: comparison of acute effects with polyvinyl alcohol particles and calibrated microspheres. Radiology, 224 (2), 436–445.
- Pelage, J.P., et al., 2003. Limited uterine artery embolization with tris-acryl gelatin microspheres for uterine fibroids. Journal of Vascular and Interventional Radiology:, 14 (1), 15–20.
- Pontis, A., et al., 2016. Adenomyosis: a systematic review of medical treatment. Gynecological Endocrinology: The Official Journal of the International Society of Gynecological Endocrinology, 32 (9), 696–700.
- Popovic, M., et al., 2011. Uterine artery embolization for the treatment of adenomyosis: a review. Journal of Vascular and Interventional Radiology, 22 (7), 901–909; quiz 909.
- Poujade, O., et al., 2013. Uterine necrosis following pelvic arterial embolization for post-partum hemorrhage: review of the literature. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 170 (2), 309–314.
- Reinhold, C., et al., 1999. Uterine adenomyosis: endovaginal US and MR imaging features with histopathologic correlation. Radiographics: a Review Publication of the Radiological Society of North America, Inc, 19 Spec No (suppl_1), S147–S60. Spec No,
- Scheurig-Muenkler, C., et al., 2011. Uterine artery embolization for symptomatic fibroids: long-term changes in disease-specific symptoms and quality of life. Human Reproduction, 26 (8), 2036–2042.
- Schrager, S., et al., 2022. Adenomyosis: diagnosis and management. American Family Physician, 105 (1), 33–38.
- Senturk, L.M. and Imamoglu, M., 2015. Adenomyosis: what is new? Women’s Health, 11 (5), 717–724.
- Shaaban, O.M., et al., 2015. Levonorgestrel-releasing intrauterine system versus a low-dose combined oral contraceptive for treatment of adenomyotic uteri: a randomized clinical trial. Contraception, 92 (4), 301–307.
- Sheikh, G.T., et al., 2020. Angiographic detection of utero-ovarian anastomosis and influence on ovarian function after uterine artery embolization. Cardiovascular and Interventional Radiology, 43 (2), 231–237.
- Siskin, G.P., et al., 2001. Uterine artery embolization for the treatment of adenomyosis: clinical response and evaluation with MR imaging. AJR. American Journal of Roentgenology, 177 (2), 297–302.
- Soave, I., et al., 2018. Treatment options and reproductive outcome for adenomyosis-associated infertility. Current Medical Research and Opinion, 34 (5), 839–849.
- Stokes, L.S., , C., et al., 2010. Quality improvement guidelines for uterine artery embolization for symptomatic leiomyomas. Journal of Vascular and Interventional Radiology, 21 (8), 1153–1163.
- Struble, J., Reid, S. and Bedaiwy, M.A., 2016. Adenomyosis: a clinical review of a challenging gynecologic condition. Journal of Minimally Invasive Gynecology, 23 (2), 164–185.
- Templeman, C., et al., 2008. Adenomyosis and endometriosis in the California Teachers Study. Fertility and Sterility, 90 (2), 415–424.
- Tsui, K.H., et al., 2014. Medical treatment for adenomyosis and/or adenomyoma. Taiwanese Journal of Obstetrics & Gynecology, 53 (4), 459–465.
- Vitale, S.G., et al., 2023. Hysteroscopic laser ablation of symptomatic uterine fibroids: insights from a prospective study. Climacteric: The Journal of the International Menopause Society, 26 (5), 497–502.
- Vitale, S.G., et al., 2020. Hysteroscopic treatment of submucosal fibroids in perimenopausal women: when, why, and how? Climacteric: The Journal of the International Menopause Society, 23 (4), 355–359.
- Von Elm, E., et al., 2008. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Journal of Clinical Epidemiology, 61 (4), 344–349.
- Wang, Y., et al., 2020. Asherman syndrome in adenomyosis treated with uterine artery embolization: incidence predictive factors. La Radiologia Medica, 125 (5), 437–443.
- Zheng, R., et al., 2018. Predisposing factors for predicting the therapeutic response of adenomyosis after uterine artery embolization: serum CA125 levels and accompanying endometriosis. Diagnostic and Interventional Radiology , 24 (6), 364–371.
- Zhou, J., et al., 2016. Outcomes in adenomyosis treated with uterine artery embolization are associated with lesion vascularity: A long-term follow-up study of 252 cases. PLOS One, 11 (11), e0165610.