

Abstract
Background
Endometrial cancer (EC) has a high latency, making prognosis difficult to predict. Cancer antigen 125 (CA125) is not specific as a tumour marker for EC; however, complete blood count (CBC) inflammatory markers are associated with prognosis in various malignancies. Thus, this study investigated the value of CBC inflammatory markers combined with CA125 levels in predicting the prognosis of patients with EC.
Methods
In this study, 517 patients with EC were recruited between January 2015 and January 2022, and clinical characteristics, CBC inflammatory markers, and CA125 levels were assessed. Differences in each index at different EC stages and the correlation between the index and EC stage were analysed, and the influence of the index on EC prognosis was evaluated.
Results
Platelet distribution width (PDW) levels were significantly lower in patients with advanced EC than in those with early EC, whereas the systemic immune-inflammation index (SII), neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), platelet-to-lymphocyte ratio (PLR), and CA125 levels were significantly higher in patients with advanced EC (all P < 0.05). ROC curve and multivariate logistic regression analyses indicated that decreased PDW and increased CA125 levels were independent risk factors for EC staging progression. In addition, multivariate Cox regression analysis showed that the combination of low PDW and high CA125 (PDW + CA125 = 2) was an independent prognostic factor of survival in EC patients. Kaplan-Meier survival analysis indicated that patients with low PDW and high CA125 had worse overall survival.
Conclusions
The PDW and CA125 score may be an independent prognostic factor for postoperative overall survival in patients with EC and a useful marker for predicting the prognosis of these patients.
PLAIN LANGUAGE SUMMARY
Endometrial cancer (EC) has a high latency period, and the prognosis of EC is difficult to predict. The inflammatory response within the tumour microenvironment plays an important role in the occurrence and development of cancer. In our study, various inflammatory indicators in complete blood counts were comprehensively analysed, and cancer antigen 125 (CA125) was further used to predict the stage and prognosis of EC. The results showed that patients with low platelet distribution width (PDW) and high CA125 levels had poorer overall survival. The PDW and CA125 score may be used as a new independent prognostic indicator.
Introduction
The incidence of endometrial cancer (EC) is on the rise (Sung et al. Citation2021). Patients with early-stage EC have a good prognosis and most can be cured by surgery, whereas the prognosis of patients with stage III or IV EC is poor, with 5-year survival rates of 47-69% and 15-17%, respectively (Canadian Cancer Society’s Advisory Committee on Cancer Statistics Citation2016, Lee et al. Citation2017,). However, EC has a high latency and a long onset cycle, and early symptoms are not obvious (Reijnen et al. Citation2019). Therefore, predicting the prognosis of EC remains difficult, and it is necessary to explore feasible objective biomarkers to judge prognosis.
Cancer antigen 125 (CA125) is considered to be related to the prognosis of EC (Modarres-Gilani et al. Citation2017), but its specificity as a tumour marker for EC is low. Under certain physiological or pathological conditions (e.g. menstruation, pregnancy status, endometriosis, and hepatitis), the CA125 level also increases to varying degrees (Crosby et al. Citation2018, Friis Petersen et al. Citation2019, Kokot et al. Citation2021, Qin et al. Citation2021,). Therefore, it is not recommended to use CA125 alone as a prognostic marker of EC.
There is a relationship between inflammation and tumours, and the inflammatory response in the cancer cell microenvironment plays an important role in the occurrence and development of tumours (Grivennikov et al. Citation2010). The association between several inflammatory markers, including systemic immune-inflammation index (SII), platelet-to-lymphocyte ratio (PLR), neutrophil-to-lymphocyte ratio (NLR), and platelet distribution width (PDW), and poor prognosis in gynecological solid tumours, including ovarian, cervical, and endometrial cancer, has been reported (Fu et al. Citation2018, Abu-Shawer et al. Citation2019, Matsubara et al. Citation2021), but controversy remains.
Thus, this study investigated the value of complete blood count (CBC) inflammatory markers combined with CA125 levels in predicting the prognosis of patients with EC, with the aim of identifying a more convenient and rapid prognostic indicator, which is conducive to the treatment of EC.
Methods
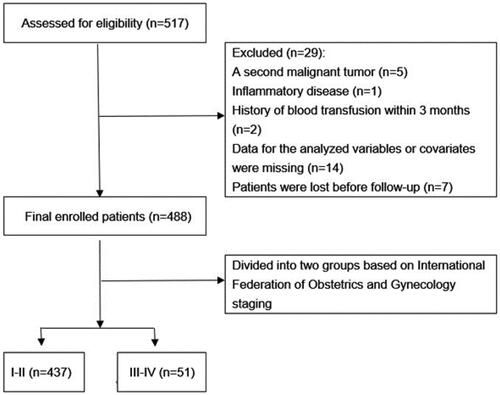
Data from 517 women who underwent primary hysterectomy for EC in our hospital between January 2015 and January 2022 were retrospectively collected. The exclusion criteria were as follows: (1) a second malignant tumour(n = 5); (2) hematological disease, inflammatory disease, myeloproliferative disease, autoimmune disease, or splenectomy(n = 1); (3) preoperative radiotherapy or chemotherapy(n = 0); (4) administration of drugs known to affect platelet count (PLT) and/or platelet function(n = 0); (5) history of blood transfusion within 3 months or history of hormone therapy within 12 months(n = 2); and (6) data for the analysed variables or covariates were missing(n = 14) or patients were lost before follow-up(n = 7). Ultimately, 488 patients were enrolled; Patients were then divided into two groups based on International Federation of Obstetrics and Gynaecology (FIGO) staging (stage I–II and III–IV) due to the difference in the prognoses of patients with early and advanced disease ().
Figure 1. Flow chart for inclusion/exclusion of EC patients.
Demographic and clinical data were obtained from the Fujian Provincial Maternity and Children’s Hospital information system, including age at surgery, body mass index (BMI), menopause, history of diabetes, hypertension, and FIGO staging, and laboratory indicators, including CBC inflammatory markers and CA125 levels, were investigated. CBC inflammatory markers included were: white blood cell count (WBC), absolute neutrophil count (ANC), absolute lymphocyte count (ALC), absolute monocyte count (AMC), PLT, mean platelet volume (MPV), platelet haematocrit (PCT), PDW, SII, NLR, monocyte-to-lymphocyte ratio (MLR), and PLR. SII = PLT × ANC/ALC, NLR = ANC/ALC, MLR = AMC/ALC, PLR = PLT/ALC.
We followed up the survival results of the patients with EC. The median follow-up time was 113.3 months (range 1.2–258.8 months), and the last follow-up was January 2023. Overall survival (OS) was defined as the time from surgery to the last follow-up or death.
We used SPSS 22.0 software for statistical analyses, and differences were considered significant at p < 0.05. Kruskal-Wallis test, unpaired t-test, or Mann-Whitney U test were used to compare continuous variables. Chi-square test or Fisher’s exact test were used to compare the categorical variables. Receiver operating characteristic (ROC) curves were generated for each continuous variable to determine the optimal cut-offs for factors related to EC. Univariate and multivariate logistic regression analyses were used to determine the independent risk factors for EC stage. The OS rate was calculated using the Kaplan-Meier method, and the survival rates between groups were compared using the log-rank test. Univariate and multivariate Cox regression analyses were performed to determine the independent risk factors for OS.
This study was approved by the ethical committee of the Department of Gynaecology of Fujian Provincial Maternity and Children’s Hospital (approval number 2023J011222). The requirement to obtain informed consent from research subjects was waived because of the retrospective nature of the study. The study complied with the principles of the Declaration of Helsinki.
Results
There were no differences in age, BMI, WBC, ANC, ALC, AMC, PLT, MPV, PCT, menopausal status, history of diabetes, or history of hypertension between the groups (all p > 0.05, ). However, the SII, NLR, MLR, PLR, and CA125 levels were significantly higher in stage III-IV patients than in stage I-II patients, and PDW was significantly lower (all p < 0.05, ). ROC curve analysis was used to identify the optimal cut-offs of significantly different factors for predicting EC stage (). Using these cut-off values, univariable and multivariable binary logistic regression analysis found that PDW and CA125 were independent factors influencing EC stage (p < 0.05, ).
Figure 2. ROC curves of the SII, NLR, MLR, PLR, PDW, and CA125 levels in predicting EC stage. ROC: receiver operating characteristic; SII: systemic immune-inflammation index; NLR: neutrophil-to-lymphocyte ratio; MLR: monocyte-to-lymphocyte ratio; PLR: platelet-to-lymphocyte ratio; PDW: platelet distribution width; CA125: cancer antigen 125.
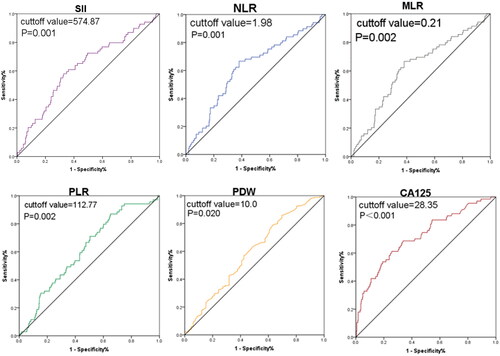
Table 1. Comparison of clinical indicators in early and advanced EC.
Table 2. Univariate and multivariate logistic regression analyses for EC stage.
Low PDW and high CA125 were independent risk factors for the progression of EC stage; therefore, we divided EC patients based on the PDW and CA125 levels into the following three groups: high PDW and low CA125 (0 points), either low PDW or high CA125 (1 point), and both low PDW and high CA125 (2 points). We then compared the clinical features of these three groups (). The results showed that the low PDW/high CA125 group had higher FIGO stage (p < 0.001), but there were no differences in age, BMI, menopausal status, history of diabetes, or history of hypertension among the three groups (all p > 0.05).
Table 3. Associations of PDW and CA125 level with clinical characteristics.
Univariate Cox regression analysis showed that the SII, NLR, PDW/CA125 combination, and FIGO stages were related to OS in EC patients (all p < 0.05, ). Multivariate Cox regression analysis showed that low PDW/high CA125 (i.e., 2 points) was an independent prognostic factor for OS (hazard ratio, 5.156; 95% CI: 1.060–25.075; p = 0.042, ). The Kaplan-Meier curve showed that there was no difference in OS in the 0- and 1-point groups (p = 0.907). However, the OS of the 2-point group was significantly lower (p < 0.05). The 5-year OS rates of the 0-, 1-, and 2-point groups were 97.1%, 96.9%, and 83.3%, respectively, as shown in .
Figure 3. Kaplan–Meier curve for OS of patients with EC stratified by PDW and CA125. (A) Kaplan-Meier curve for OS in EC patients in different PDW + CA125 groups (0 vs 1 vs 2). (B) Kaplan-Meier curve for OS in EC patients in different PDW + CA125 groups (0 and 1 vs 2).
PDW: platelet distribution width; CA125: cancer antigen 125. High PDW + low CA125 = 0 points; either low PDW or high CA125: 1 point; both low PDW and high CA125: 2 points.
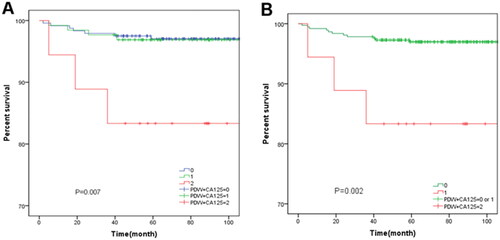
Table 4. Univariate and multivariate Cox proportional hazards regression analyses for OS in EC.
Discussion
In this study, the PDW level was lesser, while SII, NLR, MLR, PLR, and CA125 levels were higher in the later stage than in the early stage of EC (p < 0.05, ). The comparison of the other inflammatory markers was not statistically significant. Decreased PDW and increased CA125 levels were independent risk factors for the progression of EC stage (p < 0.05, and ), and the score of PDW + CA125 was positively correlated with FIGO stage (p < 0.001, ). In addition, multivariate Cox regression analysis showed that PDW + CA125 = 2 was an independent prognostic factor (p < 0.001, ). Kaplan-Meier survival analysis indicated that patients with low PDW and high CA125 had worse overall survival (). By comprehensively analysing each CBC inflammatory index, this study showed that CA125 can be combined with PDW to better predict the progression of EC staging, and the PDW + CA125 score can be used as a novel independent prognostic indicator, which has not been previously reported in the literature.
Tumour cells can stimulate megakaryocyte maturation and induce platelet synthesis, activation, and aggregation through a variety of mediators and cytokines (Vincent and Rafii Citation2004). PDW, a common CBC parameter, is the main indicator of platelet activation. In our study, patients with advanced EC had lower PDW than those with early EC (p < 0.05). Additionally, PDW was an independent factor associated with EC stage. A low PDW is an unfavourable factor for survival in non-small cell lung cancer (Cui et al. Citation2017). Conversely, Qin et al. (Citation2020) showed that a higher PDW is related to a poor prognosis in ovarian cancer. These results highlight the inconsistency of the value of PDW as a prognostic marker. Our study analysed the PDW of EC patients, and we found that PDW was related to EC stage, with a low PDW being a poor prognostic factor for EC, which was consistent with the results of Kurtoglu et al. (Citation2015) and Chen et al, (Citation2020) studies. we speculate that the heterogeneity of platelet size decreases with progression of inflammation, leading to reduced PDW in patients with poor prognosis.
CA125 is widely present in mesothelial and endothelial cells of the female reproductive system. When these cells are stimulated by inflammation or destroyed by tumour cells, CA125 is released, and it is highly expressed in the blood (Epiney et al. Citation2000). Currently, CA125 is considered to be closely related to the occurrence and development of EC (Zhang et al. Citation2020). Our results showed that CA125 level was an independent risk factor for EC progression and that a high expression level of CA125 was a poor prognostic factor for EC.
Notably, PDW + CA125 had a better prognostic value than CA125 or PDW alone. Therefore, our study suggests that the combination of CA125 and PDW can be used for the prognostic analysis of EC.
Our study had certain limitations because it was a single-center, retrospective analysis. Only a small number of women of reproductive age were included, and patients with ovarian borderline tumours were excluded. Consequently, expanding the investigation to include such cases in subsequent studies is necessary. Second, most cases in this study were endometrioid adenocarcinoma, and the influence of molecular characteristics on prognosis should be studied further. Nevertheless, this study provides new ideas and directions for predicting the prognosis of EC and identified a promising combination that may be used as a prognostic indicator for EC.
Conclusion
The inflammatory indicator PDW can be combined with CA125 to determine and track the progression of EC staging. Moreover, their detection is economical, rapid, and convenient for routine monitoring, which is conducive to EC treatment follow-up. The PDW and CA125 score may be an independent prognostic factor for postoperative OS in patients with EC and a useful marker for predicting the prognosis of these patients.
Ethical approval
This study was approved by the ethical committee of the Department of Gynaecology of Fujian Provincial Maternity and Children’s Hospital (approval number 2023KYLLRD01058). The requirement to obtain informed consent from research subjects was waived because of the retrospective nature of the study. The study complied with the principles of the Declaration of Helsinki.
Consent for publication
Not applicable.
Authors’ contributions
Hongxing Lin and Wenhui Zhong designed the study. Hongxing Lin wrote the manuscript. Hongxing Lin, Chengwen Que, and Xiaosong Lin collected, analysed and interpreted the data. Wenhui Zhong, and Liying Zhong critically reviewed, and edited the manuscript. All authors read and approved the final manuscript.
STROBE_checklist.doc
Download MS Word (111 KB)Certificate of editing 2.pdf
Download PDF (299.1 KB)Certificate of editing 1.pdf
Download PDF (304.3 KB)Acknowledgments
Not applicable.
Disclosure of interest
No potential conflict of interest was reported by the authors.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Abu-Shawer, O., et al., 2019. Hematologic markers of distant metastases and poor prognosis in gynecological cancers. BMC Cancer, 19 (1), 1.
- Canadian Cancer Society’s Advisory Committee on Cancer Statistics 2016. Canadian Cancer Statistics. Toronto, ON: Canadian Cancer Society.
- Chen, H., et al., 2020. Nomograms based on the novel platelet index score predict postoperative prognosis in endometrial cancer. Gynecologic Oncology, 158 (3), 689–7.
- Crosby, D.A., et al., 2018. CA125 measured during menstruation can be misleading. Irish Medical Journal, 111 (4), 738.
- Cui, M.M., et al., 2017. Platelet distribution width correlates with prognosis of non-small cell lung cancer. Scientific Reports, 7 (1), 3456.
- Epiney, M., et al., 2000. CA125 production by the peritoneum: in-vitro and in-vivo studies. Human Reproduction , 15 (6), 1261–1265.
- Friis Petersen, J., et al., 2019. Early pregnancy reference intervals; 29 serum analytes from 4 to 12 weeks’ gestation in naturally conceived and uncomplicated pregnancies resulting in live births. Clinical Chemistry and Laboratory Medicine, 57 (12), 1956–1967.
- Fu, S., et al., 2018. Squamous cell carcinoma antigen, platelet distribution width, and prealbumin collectively as a marker of squamous cell cervical carcinoma. Cancer Biomarkers: section A of Disease Markers, 21 (2), 317–321.
- Grivennikov, S.I., et al., 2010. Immunity, inflammation, and cancer. Cell, 140 (6), 883–899.
- Kokot, I., et al., 2021. Diagnostic significance of selected serum inflammatory markers in women with advanced endometriosis. International Journal of Molecular Sciences, 22 (5), 2295.
- Kurtoglu, E., et al., 2015. Platelet indices may be useful in discrimination of benign and malign endometrial lesions, and early and advanced stage endometrial cancer. Asian Pacific Journal of Cancer Prevention, 16 (13), 5397–5400.
- Lee, Y.C., et al., 2017. Treatment strategies for endometrial cancer: current practice and perspective. Current Opinion in Obstetrics & Gynecology, 29 (1), 47–58.
- Matsubara, S., et al., 2021. Prognostic value of pre-treatment systemic immune-inflammation index in patients with endometrial cancer. PLOS One, 16 (5), e0248871.
- Modarres-Gilani, M., et al., 2017. The prognostic role of preoperative serum CA125 levels in patients with advanced endometrial carcinoma. Cancer Biomarkers: section A of Disease Markers, 20 (2), 135–141.
- Qin, C., et al., 2021. Predictive effects of preoperative serum CA125 and AFP levels on post-hepatectomy survival in patients with hepatitis B-related hepatocellular carcinoma. Oncology Letters, 21 (6), 487.
- Qin, L., et al., 2020. Higher platelet distribution width is associated with unfavorable prognosis in ovarian cancer. Cancer Biomarkers: section A of Disease Markers, 28 (3), 365–370.
- Reijnen, C., et al., 2019. Improved preoperative risk stratification with CA-125 in low-grade endometrial cancer: a multicenter prospective cohort study. Journal of Gynecologic Oncology, 30 (5), e70.
- Sung, H., et al., 2021. Global Cancer Statistics 2020: GLOBOCAN Estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a Cancer Journal for Clinicians, 71 (3), 209–249.
- Vincent, L. and Rafii, S., 2004. Vascular frontiers without borders: multifaceted roles of platelet-derived growth factor (PDGF) in supporting postnatal angiogenesis and lymphangiogenesis. Cancer Cell, 6 (4), 307–309.
- Zhang, H., et al., 2020. Clinical application of red cell distribution width, mean platelet volume, and cancer antigen 125 detection in endometrial cancer. Journal of Clinical Laboratory Analysis, 34 (8), e23309.