

Abstract
Background
Operative vision can frequently be critically reduced during laparoscopic surgery by condensation and other matter accumulating on the distal laparoscope lens. By delivering saline and carbon dioxide across the lens, the OpClear system is designed to maintain operative vision without needing scope removal for lens cleaning. This study evaluates the system’s efficacy in providing high-level visual acuity during laparoscopic hysterectomy while examining its utility through its impact on operative duration.
Methods
A retrospective audit compared efficacy and utility for the three years before and after the implementation of OpClear in a single unit. Thirty-three cases were reviewed pre-OpClear, while 82 cases were analysed in the post-OpClear group. All cases involved routine total laparoscopic hysterectomies (TLH) performed by the same surgeon (AT) with similar complexity levels.
Results
The OpClear system provided a consistently high level of visual acuity throughout the laparoscopic procedures. Scope removals, which typically result in non-productive operating time, were virtually eliminated. Consequently, in highly comparable cases, OpClear usage resulted in a 17-minute reduction in operating time over cases performed without the device. Additionally, in the OpClear group, there were trends towards reduced blood loss and shorter hospital stays, with patients in the OpClear group being discharged on first rather than second postoperatively.
Conclusions
The findings of this audit suggest that the OpClear system provides continuous high-level vision during laparoscopic hysterectomy. Further, reducing periods of non-productive time associated with scope removal for cleaning resulted in shorter operating times. Thus, the system has the potential to enhance safety, improve theatre utilisation and alleviate some of the surgical stresses associated with laparoscopic surgery.
PLAIN LANGUAGE SUMMARY
Keyhole (Laparoscopic) surgery is often better for patients than open surgery as it speeds up recovery and return to normal activities. However, despite technical advances, the surgeon’s view during keyhole operations may be lost by condensation and tissue material sticking to the lens of the laparoscope, the instrument used to see inside the body. For safety, such vision loss demands that operations must be paused so the ‘scope’ can be removed and the lens cleaned. This may occur often during an operation, interrupting its progress. Our audit reviews OpClear, a device that cleans the lens while the scope is in the body, improving vision and reducing pauses. OpClear works by blowing gas and fluid across the lens, washing away contamination. In keyhole hysterectomy operations, OpClear maintained vision and shortened the length of operations. OpClear may lead to safer, shorter keyhole operations and help improve the efficiency of operating departments.
Introduction
Hysterectomy is a common gynaecological operation, with approximately 60,000 cases performed annually in the United Kingdom (Madhvani et al. Citation2019). The laparoscopic approach has become the most popular method for hysterectomy (NHS Digital Citation2018) and is associated with fewer surgical complications, shorter hospitalisation and quicker recovery (Pitter et al. Citation2014, Aarts et al. Citation2015). However, successful laparoscopic surgery demands high-level visual acuity transmitted between the laparoscope and surgical monitor. Although contemporary laparoscopic systems can provide clear vision, condensation, blood, and tissue debris may still obstruct the distal laparoscopic lens (DLL) (Nabeel et al. Citation2022). Such contamination compromises safety, requiring laparoscope removal for cleaning and creating interruptions in surgical progress. Since vision loss can occur multiple times during a procedure, frequent cleaning of the laparoscope is often necessary, resulting in significant cumulative non-productive operating time. The OpClear laparoscopic cleaning system claims to address this problem by cleaning the DLL without needing scope removal. To test this claim, this study presents a single-centre experience reviewing the efficacy and utility of the OpClear system during total laparoscopic hysterectomy.
Methods
This audit aims to evaluate the efficacy of the OpClear system in maintaining visual clarity during total laparoscopic hysterectomy (TLH). Additionally, the audit examines any broader utility of the system resulting from the improvement in vision during laparoscopic surgery. As this was a restrospective audit no formal registration of patients was required.
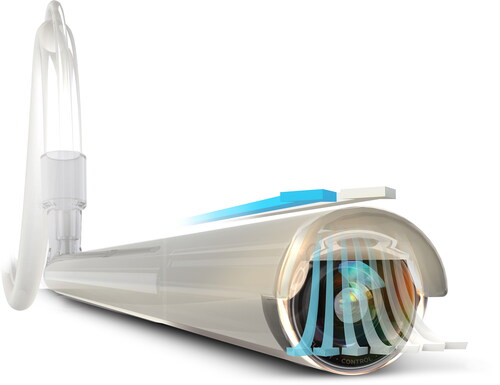
The OpClear® (Cipher Surgical Ltd. UK) system delivers saline and carbon dioxide (CO2) across the DLL, clearing matter from the optical surface. The system comprises a reusable control unit, which manages CO2 and sterile saline delivery via internal software. The control unit connects to a CO2 source and then, via tubing to a disposable ‘C-clip’ laparoscope sheath, fitted before procedures begin (). A refillable 0.9% saline cartridge is placed between the control unit and the sheath, with saline flow activated by CO2 pressure from the control unit. CO2 and saline are delivered to the DLL between the scope and the disposable sheath (). Scope cleaning occurs by two functions. Firstly, ‘auto-demist’ provides continuous CO2 flow across the DLL and prevents fogging due to condensation. Secondly, an ‘active wash’ prompts a 3-second CO2 and saline wash cycle, effectively removing blood, tissue debris, and other particulate matter. This latter function is surgeon-activated via a foot switch.
Figure 1. The OpClear system, showing the control unit, foot switch and C-Clip sheath applied to a laparoscope.

Figure 2. Laparoscope with OpClear sheath applied demonstrating flow path of CO2 and Saline.
A retrospective audit of operating outcomes in TLH was performed. Data was reviewed for consecutive cases performed three years before the introduction of OpClear and compared with those for similar cases three years after introduction.
This unit’s standard practice for TLH is as follows:
With the patient in the lithotomy position, a pneumoperitoneum is achieved with a Verres needle with entry pressure set to 20 mmHg. Laparoscopic ports are inserted under direct vision - a 12 mm umbilical port and 5 mm ports suprapubically and in the left iliac fossa. The pneumoperitoneum pressure is then reduced to 15 mmHg and the patient placed in the Trendelenburg position. A 10 mm, zero-degree laparoscope is inserted. During dissection, a Thunderbeat (Olympus Ltd) hybrid energy device is used to seal and divide tissue. The upper pedicles are sealed and divided before the bladder is mobilised and reflected. The uterine vessels are then sealed and divided. The vagina is delineated using a Clermont Ferrand uterine manipulator before colpotomy is performed with the active blade of the Thunderbeat. The uterus is removed vaginally, and the vault oversewn with a Stratofix© 2.0 suture from Ethicon.
In addition to assessing the ability of the OpClear system to maintain visual acuity during TLH, the wider benefits of improved vision during laparoscopic surgery were also assessed. Accordingly, the study focused on the following outcomes:
The ease of use of the system and its integration into the operating theatre environment.
Effectiveness of the OpClear system in maintaining vision.
The impact of the OpClear system on:
Intra-operative scope cleaning
Operative duration
Estimated blood loss and the length of postoperative hospital stay
The audit review was performed retrospectively. However, all patient and timing information was collected in real time by two data systems independent of the operating team. Firstly, operative data, including the duration of procedures, was recorded using the Unit’s operating theatre management system. Secondly, OpClear usage was recorded intraoperatively by the OpClear control unit.
Results
Thirty-three consecutively treated patients were reviewed in the pre-OpClear group. Previously performed TLHs were excluded on the basis that they were vaginally assisted and non-comparable to others in the OpClear group. Eighty-two consecutively treated patients were examined in the group in which OpClear was used. Four cases, initially in the OpClear group, were excluded due to their requirement for extensive adhesiolysis and/or pre-procedure cystoscopy and insertion of ureteric stents.
The demographics and clinical details of the patients included in the review are shown in and . These data indicate no significant difference between the two groups regarding age, parity, previous caesarian sections or uterine weight. All cases, in both groups were completed successfully with no open conversions or OpClear-related adverse events.
Figure 3. Patient demographics and clinical details.
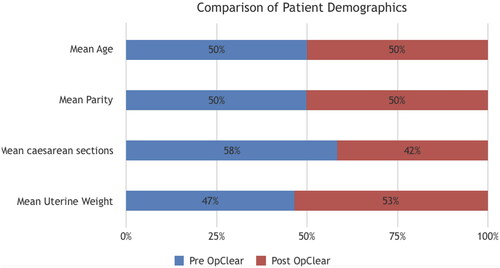
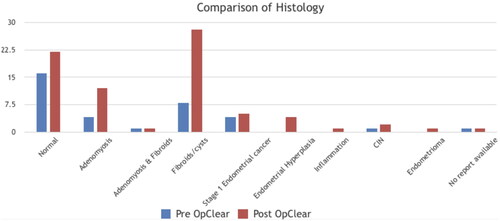
Figure 4. Comparison of histology within the two groups.
Regarding efficacy
OpClear was readily accommodated into the unit’s laparoscopic protocol, easily set up by the operating theatre staff immediately before cases commenced.
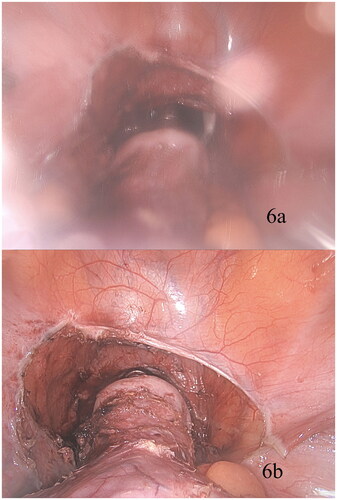
Using both OpClear functions, high-level visual acuity was maintained near-seamlessly throughout the cases in the OpClear group. The continuous flow function prevented condensation. The surgeon-activated wash addressed vision loss due to adherent particulate matter and blood. An example of OpClear’s effect is given in the photographs ( and ) from a TLH in a patient with stage 3 endometriosis, previous LSCS, morbid obesity and omental adhesions. shows the initial view of the pelvis before the commencement of dissection. The image lacks definition due to early condensation. shows the same view after activation of the OpClear. The anatomy is better defined, with the scarring and adhesions from the previous caesarean section visible. There is an enhanced definition of the endometriotic deposits, including vesicular disease, which was not apparent before OpClear activation. illustrates the development of significant fogging at a critical step in the posterior colpotomy. The bladder is reflected, and the vagina opened anteriorly. However, it is unsafe to continue without improving the surgical view. Following activation of OpClear (), there is immediate restoration of clarity, allowing safe completion of the posterior colpotomy and extirpation of the uterus vaginally. In such a case, surgical progress would usually be challenging due to repeated lens contamination and scope removal. However, using OpClear, vision was maintained, and the procedure was completed with minimal interruption to progress.
Figure 5. View of the pelvis prior to commencement of total laparoscopic hysterectomy with (a) initial fogging due to lens condensation and (b) Restoration of clarity following activation OpClear activation.
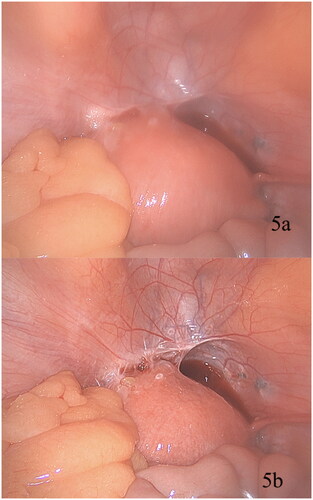
Figure 6. (a) Illustrates the development of significant fogging at a critical step in the posterior colpotomy. Following activation of OpClear (), there is immediate restoration of clarity.
In the series, the mean number of surgeon-activated washes per procedure was 7.9 (range 0–40). Since each wash substituted a four-second cleaning cycle for a scope removal episode of at least 1.5 minutes, some 13 minutes were potentially saved per case. This potential time benefit appears realised, as shown by the differences in the mean duration of cases between the two groups (see below). However, any time benefit was additional to preventing the loss of surgical continuity by avoiding the need for scope removal.
Regarding utility
In the series overall, the mean operating time in the pre-OpClear group was 95 minutes, and in the post-OpClear group, 80 minutes. A subgroup review examined highly comparable cases, with no significant difference in uterine weight, the addition of salpingo-ophorectomy or ovarian conservation, or parity. These cases were confined to one-year pre-OpClear, n = 24) and one-year post-OpClear, n = 19). In this subgroup analysis, the mean operating time in the pre-OpClear group was 98 minutes, and in the post-OpClear group, 81 minutes, a 17-minute reduction in operating time in the OpClear group.
The overall and subgroup time savings are commensurate with the average number of washes per case, as noted above.
In the series overall, there was a trend towards reduction in estimated intra-operative blood loss in the OpClear group. Patients in this group were also more likely to have earlier discharges from hospital, 24 hours vs 48 hours.
Discussion
Safe laparoscopic surgery demands clear, unobstructed vision. Despite the availability of advanced optic systems, laparoscopic surgeons often encounter challenges when the DLL becomes obscured, causing a critical impairment of intraoperative vision. This study aimed to evaluate the efficacy and utility of the OpClear intra-operative laparoscopic lens cleaning system, specifically during TLH.
Contamination of the DLL has three principal causes (Lawrentschuk et al. Citation2010, Yong et al. Citation2016). Firstly, condensation forms on the lens due to the intraperitoneal environment, leading to a near-universal occurrence of visual fogging, most evident early in a case when the relatively cold laparoscope enters the humid abdominal cavity (Flemming et al. Citation1996, Kubo et al. Citation2023). The second source of DLL contamination is smearing caused by fat and other tissue debris. Using high-energy dissection devices increases the likelihood of splattering liquefied or charred fatty tissue onto the DLL. While such contamination can occur at any time during the procedure, this is particularly likely when the DLL is near tissues during dissection. Removing such matter can be difficult, as it tends to adhere firmly.
The third source of lens contamination is blood, which can rapidly obstruct the operative field. Addressing a spurting vessel requires immediate surgical attention, which may be challenging when vision is compromised by blood covering the lens.
Any vision loss during laparoscopic procedures can threaten operative safety, but surgeons may need to continue operating, accepting reduced vision until a point is reached when scope cleaning can occur. This is not unusual, with one study (Yong et al. Citation2016) reporting 37% of the duration of laparoscopic procedures being performed with impaired vision. When vision loss is complete, an immediate pause in operative progress is necessary for lens cleaning.
Various methods have been documented for DLL cleaning (Ohdaira et al. Citation2007, Nezhat and Morozov Citation2008, Lawrentschuk et al. Citation2010, Mohammadhosseini Citation2010, Yong et al. Citation2016, Brown et al. Citation2022). The simplest and most widely used method (Yong et al. Citation2016) is removing contaminants by touching the DLL against organs or other visceral surfaces. While this may avoid scope removal, it carries risks since the laparoscopic light source can reach temperatures sufficient to produce tissue damage (Yavuz et al. Citation2006). The most widely accepted cleaning method involves removing the laparoscope and soaking the distal end in warmed sterile saline to facilitate particle loosening. The lens is then cleaned directly using a surgical swab. A de-fogging agent may then be applied.
The impact of cleaning episodes during laparoscopic procedures is notable. Each scope removal for cleaning necessitates a pause in operative progress, diverting surgical attention from the ongoing task. These episodes create a significant cumulative period of non-productive operating time. Yong et al. (Citation2016) report that approximately 7% of laparoscopic operating time is spent cleaning the DLL.
By contrast, the OpClear system (Cipher Surgical, Coventry, UK) claims to provide an effective method for cleaning the DLL without scope removal. Other devices with the same aim have been reported, although, to date, none appear to have gained widespread clinical acceptance. Early examples include an intra-cavity device with fabric wings against which the DLL is cleaned (Cassera et al. Citation2011). More recently, the FloShield Air System (Bendifallah et al. Citation2018) has been reported, providing a continuous flow of dry CO2 gas over the tip of the scope, with the aim of preventing condensation and smoke settling on the DLL rather than addressing adherent material. Improved vision and fewer scope removals were reported, but there was no reduction in operative duration.
OpClear, through continuous CO2 and surgeon-triggered saline flow across the DLL, not only addresses condensation and smoke but also washes away adherent tissue debris and blood. Consequently, the system maintains visual acuity throughout procedures, minimising non-productive operating time. Its ease of use also reduces the temptation to clean the DLL against visceral structures.
The use of OpClear in general surgical laparoscopic practice has been documented (Ozgur et al. Citation2022, Ozgur and Gorgun Citation2022), with reports describing near-continuous visual acuity. However, until the current audit, no report has been available on using the device in gynaecological practice.
In this review, OpClear was used in 82 TLH cases. Regarding efficacy, the system was easily set up before each case and readily integrated with standard laparoscopic equipment. As depicted in and , the device provided high-quality visual acuity in all cases, accomplished through the two cleaning mechanisms offered by the system. The continuous CO2 flow prevented condensation and cleared smoke, while the surgeon-triggered saline wash quickly removed adherent particulate matter and blood. Together, these functions allowed uninterrupted surgical progress.
As a result, the OpClear group required fewer scope removals, decreasing non-productive operative time. This contributed to an observed reduction in operating time of fifteen minutes per case for the OpClear group. Since the series contained the variations recognised in TLH patients, a subgroup analysis focused on highly comparable TLH patients with no significant differences in uterine weight, parity, or need for additional procedures (e.g. bilateral salpingo-ophorectomy). In this analysis, a mean reduction of seventeen minutes in operating time was observed in the OpClear group, a time-saving commensurate with the number of wash cycles replacing scope removals.
In TLH, as reported in colorectal procedures (Ozgur et al. Citation2022, Ozgur and Gorgun Citation2022), a reduction in the duration of laparoscopic cases was approximately 15%. However, in the only other report of OpClear use (Watanabe et al. Citation2023), also in colorectal surgery, time reduction was not observed. This assessment focussed on surgical workload, concluding that OpClear resulted in less physical demand than cleaning involving scope removal. The number of extra-peritoneal DLL washes required was significantly less, but despite this, it is unclear why a reduction in case duration was also not observed.
In drawing conclusions regarding case duration, it is acknowledged that the current study has limitations, particularly that it is not randomised. Conducting a randomised trial was not considered feasible because OpClear had become an integral part of the unit’s practice due to its enhanced operative vision. Performing procedures without OpClear was, therefore, considered inappropriate. Against this background, the audit is primarily an observational assessment of OpClear’s effectiveness in providing enhanced laparoscopic vision and confirms that this is the case.
Regarding the impact on operative duration, the audit must be considered an initial exploration defining the potential for further studies. Even so, the cases reviewed, with and without OpClear, are comparable. All procedures occurred in the same operating theatre and were performed by the same experienced consultant gynaecologist (AT). No new operative techniques or equipment were introduced during the study, maintaining the comparability of procedures. While the audit was retrospective, data were collected on independent systems at the time of the procedures. Patient demographics and uterine pathology were comparable. This comparability supports the conclusion that the observed reduction in operative duration is a real event, a conclusion also drawn in laparoscopic colorectal surgery (Ozgur et al. Citation2022). The study, therefore, strengthens the case for conducting further trials and health economic studies, particularly in situations where operating costs are based on operative duration. The series also showed a trend, with OpClear, towards reducing estimated blood loss. This is encouraging, suggesting that enhanced vision may improve laparoscopic surgical accuracy. The trend towards earlier hospital discharge in the OpClear group was unexpected, and since the factors influencing discharge times are complex, this must be interpreted with caution.
Despite the potential benefits of improved vision and shorter case times, the acceptance of OpClear will depend on cost-effectiveness. Unfortunately, demonstrating cost-benefit for devices like OpClear is challenging given that acquisition and disposable costs are incurred, expenses that potentially limit use in many departments unless offset by savings. Consequently, while it may seem counterintuitive to withhold continuous vision from surgeons, along with potential improvements in surgical workload and safety, this is a reality for many units unless incremental costs are reasonable. Any enhanced operative time efficiency offered by such new devices, therefore, becomes a crucial consideration. Time efficiency can arise from shortening the duration of individual cases and enhanced operating department throughput. The time savings highlighted in this and other reports of OpClear may benefit operating departments, translating into cost savings per case and improved logistics. In the contemporary clinical landscape, operational efficiency and cost reduction are universal concerns (Boggs et al. Citation2019, Schouten et al. Citation2023), and strategies that may create such service improvements deserve consideration. Even so, such strategies must be multifactorial, with devices like OpClear reviewed as part of broader efficiency reviews rather than in isolation. For instance, studies indicate that using Vectec uterine manipulators in TLH can also reduce operative duration compared to similar devices (Misirlioglu et al. Citation2019). The cumulative impact of practice evolution that includes OpClear alongside instrument selection may improve efficiency and resource utilisation. Such wide-ranging reviews of surgical efficiency are sparse (Schouten et al. Citation2023). Nevertheless, given the reported outcomes for OpClear, it is suggested that its role should be further assessed as part of comprehensive health economic studies in specific surgical specialities, including gynaecology.
This first report on using the OpClear system in gynaecological practice supports its efficacy and utility. The device maintains high-level visual acuity throughout laparoscopic procedures by virtually eliminating the need for scope removal for cleaning. This reduces non-productive operating time, leading to shorter operative procedures. These audit findings support the case for undertaking prospective studies to further define the device’s value in gynaecological and other laparoscopic specialities and align with initiatives to improve quality in operating departments (Getting it right first time (GIRFT) Citation2009). Health economic studies may also provide insights into the device’s potential contribution to improving operating department cost efficiency while supporting operative safety and improving surgical workload.
Contributions to authorship
R Evans and A Taylor contributed equally to this study, the collection of data and the production of the manuscript.
Acknowledgments
We thank Mr A Ready for his help and advice on audit design and proof reading.
Disclosure statement
Mr Alexander Taylor is a member of the Advisory Board for Cipher Surgery.
Data availability statement
Data associated with this paper can made available by request to the corresponding author.
Additional information
Funding
References
- Aarts, J.W., et al., 2015. Surgical approach to hysterectomy for benign gynaecological disease. The Cochrane Database of Systematic Reviews, 2015 (8), CD003677.
- Bendifallah, S., et al., 2018. Prospective, randomized comparison of the use of FloShield Air System((R)) versus the reference technique (water + povidone-iodine solution) during gynecologic endoscopic surgery to evaluate the operative lens vision quality. Surgical Endoscopy, 32 (3), 1593–1599.
- Boggs, S.D., et al., 2019. OR management and metrics: how it all fits together for the healthcare system. Journal of Medical Systems, 43 (6), 147.
- Brown, J.A., et al., 2022. Use of a warming bath to prevent lens fogging during laparoscopy. J Endourol, 2008 (11), 2413–2414.
- Cassera, M.A., et al., 2011. Efficacy of using a novel endoscopic lens cleaning device: a prospective randomized controlled trial. Surgical Innovation, 18 (2), 150–155.
- Flemming, E., et al., 1996. Principles determining optical clarity in endoscopic surgery. Minimally Invasive Therapy & Allied Technologies, 5 (5), 440–444.
- Getting it right first time (GIRFT), 2009. Improving quality and efficiency in the operating theatre, a lifeline for financial leaders. The Productive Operating Theatre Team, The NHS Institute for Innovation and Improvement 2009. NHS England https://www.gettingitrightfirsttime.co.uk/
- Kubo, Y., et al., 2023. Mechanism underlying lens fogging and its countermeasure in laparoscopic surgery. Minimally Invasive Therapy & Allied Technologies: MITAT: Official Journal of the Society for Minimally Invasive Therapy, 32 (2), 56–61.
- Lawrentschuk, N., et al., 2010. Laparoscopic lens fogging: a review of etiology and methods to maintain a clear visual field. Journal of Endourology, 24 (6), 905–913.
- Madhvani, K., et al., 2019. Route of hysterectomy: a retrospective, cohort study in English NHS Hospitals from 2011 to 2017. BJOG: An International Journal of Obstetrics and Gynaecology, 126 (6), 795–802.
- Misirlioglu, S., et al., 2019. Clermont-Ferrand versus Vectec uterine manipulator for total laparoscopic hysterectomy. Minimally Invasive Therapy & Allied Technologies: MITAT: Official Journal of the Society for Minimally Invasive Therapy, 28 (1), 51–56.
- Mohammadhosseini, B., 2010. Povidone-iodine surgical scrub solution prevents fogging of the scope’s lens during laparoscopic surgery. Surgical Endoscopy, 24 (6), 1498–1499; author reply 1500.
- Nabeel, A., et al., 2022. Effective cleaning of endoscopic lenses to achieve visual clarity for minimally invasive abdominopelvic surgery: a systematic review. Surgical Endoscopy, 36 (4), 2382–2392.
- Nezhat, C. and Morozov, V., 2008. A simple solution to lens fogging during robotic and laparoscopic surgery. JSLS, 12 (4), 431.
- NHS Digital. 2018. www.digital.nhs.uk.
- Ohdaira, T., et al., 2007. Antifogging effects of a socket-type device with the super hydrophilic, titanium dioxide-coated glass for the laparoscope. Surgical Endoscopy, 21 (2), 333–338.
- Ozgur, I., et al., 2022. Stop the smudge: a novel solution to loss of vision during laparoscopic colorectal surgery. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques, 32 (5), 534–536.
- Ozgur, I., and Gorgun, E. , 2022. OpClear; a novel solution to loss of vision during laparoscopic colorectal surgery - a video vignette. Colorectal Disease: The Official Journal of the Association of Coloproctology of Great Britain and Ireland, 24 (12), 1632–1633.
- Pitter, M.C., et al., 2014. The impact of different surgical modalities for hysterectomy on satisfaction and patient reported outcomes. Interactive Journal of Medical Research, 3 (3), e11.
- Schouten, A.M., et al., 2023. Operating room performance optimization metrics: a systematic review. Journal of Medical Systems, 47 (1), 19.
- Watanabe, J., et al., 2023. Randomized controlled trial evaluating the effect of the use of a laparoscopic lens-cleaning device during laparoscopic colorectal surgery on the multidimensional workload (YCOG1903). Surgical Endoscopy, 37 (6), 4748–4753.
- Yavuz, Y., et al., 2006. Are cold light sources really cold? Surgical Laparoscopy, Endoscopy & Percutaneous Techniques, 16 (5), 370–376.
- Yong, N., et al., 2016. Impact of laparoscopic lens contamination in operating theaters: a study on the frequency and duration of lens contamination and commonly utilized techniques to maintain clear vision. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques, 26 (4), 286–289.