

Abstract
Background
Both the trauma of endometrium and hysteroscopic adhesiolysis can lead to a high rate of placenta accreta spectrum (PAS) in women with intrauterine adhesion (IUA). This study analysed the impact of time interval from adhesiolysis to pregnancy on PAS in IUA women.
Methods
Patients diagnosed with IUA who underwent adhesiolysis in Anhui Women and Children’s Medical Centre between January 2016 and December 2020 were included in this case-series study. Clinical data were obtained from electronic medical records and telephone interviews.
Results
Among a total of 102 IUA women with successful pregnancies, 8 (7.8%) suffered from miscarriages with PAS, and 94 (92.2%), 47 with PAS and 47 without PAS, had successful delivery. The total prevalence of PAS in pregnant women with IUA was 53.9% (55/102). The average time from adhesiolysis to pregnancy in the PAS group was significantly longer than in the non-PAS group (14.2 ± 5.7 vs. 10.3 ± 4.4 months, p = 0.000). Regression analysis showed that AFS grade (OR = 7.40, 95% CI 1.38–39.73, p = 0.020) and adhesiolysis to pregnancy interval time between 12 and 24 months (OR = 12.09, 95% CI 3.76–38.83, p = 0.000) were closely related to PAS. A Kaplan–Meier analysis showed the median interval time to PAS was 16.00 months (95% CI 15.11–16.89).
Conclusions
We assume that prolonged adhesiolysis to pregnancy interval may be considered a significant risk factor for PAS in IUA women.
PLAIN LANGUAGE SUMMARY
Both the trauma of endometrium and hysteroscopic adhesiolysis can result in a high rate of placenta accreta spectrum in women with intrauterine adhesion. This study analysed the impact of time interval from adhesiolysis to pregnancy on placenta accreta spectrum in intrauterine adhesion women. This case-series study included patients diagnosed with intrauterine adhesion who underwent adhesiolysis in Anhui Women and Children’s Medical Centre between January 2016 and December 2020. Clinical data were obtained from electronic medical records and telephone interviews. We assume that prolonged adhesiolysis to pregnancy interval may be considered a significant risk factor for placenta accreta spectrum in intrauterine adhesion women.
Introduction
Placenta accreta spectrum (PAS) includes placenta accreta (a direct apposition of villous tissue into the myometrium without intervening decidua), increta (the villous tissue invading into the myometrium), and percreta (invasion of the placental villi into uterine serosa). The presence of PAS often leads to more postpartum haemorrhage volume and has been associated with major morbidity and mortality in pregnant women (Oyelese and Smulian Citation2006, Baldwin et al. Citation2017). PAS is caused by an abnormal decidualization triggered by endometrial damage, for which the most common reasons are prior gynaecologic procedures, including surgical abortion and hysteroscopic surgery (Baldwin et al. Citation2018). Many prospective studies have also confirmed other risk factors, including a prior history of caesarean section (CS), advanced maternal age, pregnancies achieved by in vitro fertilisation (IVF), a current placenta previa, multiparity and others (Thurn et al. Citation2016, Kyozuka et al. Citation2019).
Trauma to the basal layer of the endometrium is the most important reason for intrauterine adhesion (IUA) (Hooker et al. Citation2014). Hysteroscopy has been widely used in diagnosing and treating IUA, which can help gynaecologists accurately evaluate uterine cavity and release adhesions (Pabuçcu et al. Citation1997). Therefore, both the trauma of endometrium itself and hysteroscopic interference can lead to a high rate of PAS in IUA women, which has also been widely confirmed in previous studies (Deans et al. Citation2018, Sonan et al. Citation2018, Zhang et al. Citation2020).
It is supposed that defective wound healing of endometrium, existing in the short interval pregnancy, defined as interpregnancy interval < 18 months, will result in PAS and predispose PAS patients to greater degrees of placental invasion (Einerson et al. Citation2020, Munoz et al. Citation2021). Even though previous studies have addressed this issue, it remains unclear whether the time interval to pregnancy after hysteroscopic adhesiolysis makes a difference in the prevalence of PAS in IUA women. Some research has described the time to pregnancy after adhesiolysis; however, they failed to focus more on its influence on PAS (Chen et al. Citation2017, Deans et al. Citation2018). Only one limited report showed it did not influence the incidence of PAS during postoperative pregnancy (Zhang et al. Citation2022). Therefore, this study was designed to thoroughly explore the influence of time intervals from adhesiolysis to pregnancy on PAS in IUA women.
Methods
Study design and population
Patients treated in Anhui Women and Children’s Medical Centre between January 2016 and December 2020 were included in this case-series study. The retrospective data were accessed from October 1, 2022, to November 30, 2022. Inclusion criteria were the following: 1) symptomatic women with either amenorrhoea or a decrease in menstrual volume; 2) age between 20 and 40; 3) diagnosed with IUA by hysteroscopy; 4) underwent adhesiolysis and resumed normal uterine cavity after surgery and wished further fertility simultaneously. Exclusion criteria were: 1) other pre-existing infertility factors, including endometriosis, adenomyosis, polycystic ovarian syndrome, uterine anomalies, pathological problems of the uterus (including fibroids, endometrial hyperplasia, polyps, etc.); 2) abnormal semen examination detected in their partners; 3) any major diseases, including severe liver and renal dysfunction, cardiovascular, respiratory disorders, pre-gestational diabetes mellitus, thrombophilia, thyroid disease and other chronic diseases.
The degree and extent of IUA were evaluated by hysteroscopy according to the American Fertility Society (AFS) classification system (Anon Citation1988). A 30° hysteroscopy with an outer sheath diameter of 5 mm (KARL Storz, Germany) was undertaken in the outpatient operation room without anaesthesia. Once the patients were diagnosed with IUA, the surgeon cut the adhesions, usually using micro-scissors to restore the normal anatomy of the uterine cavity. The bipolar loop or needle electrode, using a 12° hysteroscopy with an outer sheath diameter of 8 mm (KARL Storz, Germany), was applied under general anaesthesia in the inpatient operating room only when meeting dense muscular adhesions. Normal saline was used as the uterine distension medium at a pressure between 80 and 120 mmHg. Experienced endoscopic surgeons conducted the procedures. Adhesiolysis was under surveillance by ultrasound when it was difficult to enter or distinguish the uterine cavity. Following surgery, the patients received 4 mg/day of oestradiol valerate (Progynova, Bayer, Germany) for 21 days and 20 mg/day of dydrogesterone (Duphaston, Abbott, Netherlands) in the last ten days of each oestrogen treatment cycle. Next, hormone therapy was initiated from the first day of the menstrual cycle. Generally, all the therapies were repeated for 3 months. The patients were requested to have a hysteroscopic re-examination in the first postoperative month. If the uterus shape and endometrium returned to normal, the patient could prepare for pregnancy after treatment. If there were other IVF indications in the process of pregnancy preparation, such as fallopian tube obstruction, no pregnancy for 1 year without contraception, etc., the clinician would recommend IVF to assist pregnancy.
Parameters including maternal age at surgery, body mass index (BMI), history of gravidity and parity, number of CS and hysteroscopic surgeries, and type of IUA were collected from electronic medical records. According to the AFS guidelines, IUA was classified as mild (AFS 1-4), moderate (AFS 5-8), and severe (AFS 9-12) adhesion (Anon Citation1988). Interpregnancy interval, time to pregnancy after adhesiolysis, and mode of pregnancy were assessed by telephone interviews. When interviewing these patients, we verified the diagnosis of PAS, and only the placentas examined by the pathological department were included. When the patient gave birth or miscarried, if the placenta was difficult to peel, the clinician would do it by hand, clamp the placenta if necessary, and send the removed placenta for pathological testing. As we could not get all pathological reports, diseases of PAS, encompassing placenta accreta, increta, and percreta, were all recorded. The gestational age was calculated by the last period date in case of regular menstrual period. When the menstrual cycle was not accurate, it was calculated by the first-trimester ultrasound based on crown-lump length (CRL) close to 10 mm. Miscarriage was defined as < 28 weeks of gestation. The primary outcome of this study was the impact of time interval from adhesiolysis to pregnancy on PAS.
Statistical analysis
All data were analysed using SPSS statistics (IBM. SPSS Statistics for Windows. Version 26.0. Chicago, IL, USA: IBM; 2019.). The primary outcome measure was divided into PAS group and the non-PAS group. Gravidity was divided into 4 grades and a time interval into 3 grades. Continuous variables are presented with mean ± standard deviation. Categorical variables are presented with frequencies and percentages. T-test was used to compare the differences between continuous variables. Chi-square, Trend Chi-square analysis, and Continuous Corrective Chi-square analysis were used to compare the difference between categorical variables, as appropriate. Binary logistic regression was applied to analyse the association between PAS and all the confounders. Kaplan-Meier analysis was used to describe how the incidence of PAS changed over time from adhesiolysis to pregnancy. P-values were two-tailed, and a p-value of < 0.05 was considered statistically significant. The confidence intervals for odds ratios ranged from 5% to 95%.
Ethics statement
This trial was approved by the institutional review board of Anhui Women and Children’s Medical Centre, Hefei, China, on September 1, 2022 (YYLL2022-14-01-1.0). The patients were contacted by telephone to obtain verbal informed consent.
Results
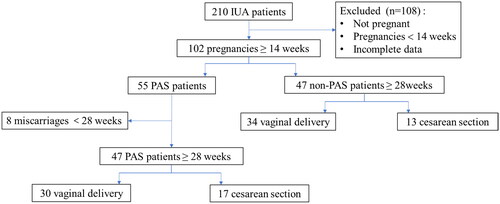
A total of 210 IUA women who underwent adhesiolysis between January 2016 and December 2020 were incuded in the present study. Our study subjects had moderate to severe adhesions, and no women had mild adhesions. Among these women, 102/210 (48.6%) had a successful pregnancy after surgery, defined as gestational age > 14 weeks, and had adequate information for data extraction in the follow-up period. Of the 102 pregnant women, 8 (7.8%) patients with PAS suffered a miscarriage, leaving 94 (92.2%) patients who progressed into the third trimester and delivered 94 infants successfully in the end. The total live birth rate was 44.8% (94/210) in IUA women. Of the 94 women who delivered successfully, 47 were with PAS, and 47 were without PAS. The total prevalence of PAS in pregnant women with IUA was 53.9% (55/102). There was no hysterectomy, maternal morbidity or mortality in this study. The flow diagram of follow-up process is shown in .
Figure 1. A flow diagram of the study population.
Demographic data of patients are presented in . There were no patients with recurrent PAS in our study. Intrauterine adhesion was more severe in the PAS group (36.4% vs. 6.4%, p = 0.000). There was no intrauterine insemination pregnancy in this study. It seemed that the risk of PAS after IVF pregnancy was higher than that of spontaneous pregnancy (21.8% vs. 2.1%, p = 0.003). Concerning the gravidity, the PAS group had more prior pregnancy times, though a statistically significant difference was not reached. There were no significant differences in age, BMI, interpregnancy interval, parity, number of previous CSs, and hysteroscopic surgery.
Table 1. Demographics of study group.
The average time to pregnancy after adhesiolysis in the PAS group was significantly longer than that in the non-PAS group. The interval time was divided into three grades, including ≤ 12 months, ≤ 24 months and > 24 months. showed that, as a categorical variable, time interval was also significantly associated with PAS (14.2 ± 5.7 vs. 10.3 ± 4.4 months, p = 0.000). When we performed a regression analysis of all confounding factors that might influence PAS, we found that only AFS grade (OR = 7.40, 95% CI 1.38–39.73, p = 0.020) and adhesiolysis to pregnancy interval time between 12 and 24 months (OR = 12.09, 95% CI 3.76–38.83, p = 0.000) were statistically significant (). In , a Kaplan–Meier analysis showed that the median interval time to PAS was 16.00 months (95% CI 15.11–16.89).
Figure 2. Kaplan-Meier analysis of time interval from adhesiolysis to pregnancy. Abbreviations: PAS: placenta accreta spectrum.
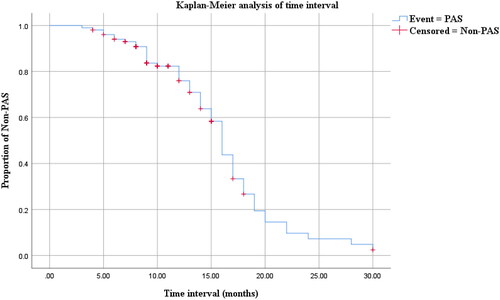
Table 2. Time interval from adhesiolysis to pregnancy assessment.
Table 3. Logistic regression analysis for PAS.
Discussion
To the best of our knowledge, this is the first retrospective study that presented the association between PAS and the time to pregnancy after adhesiolysis in IUA women. Our results showed that the successful pregnancy rate of IUA women was 48.6%, similar to that changing from 48.2–79% in prebious studies (Chen et al. Citation2017, Deans et al. Citation2018, Guo et al. Citation2019). The total live birth rate was 44.8% in this study, and it changed from 42.2–63.7% in other studies (Chen et al. Citation2017, Deans et al. Citation2018). The mid-trimester miscarriage rate in this study was 7.8%, slightly lower than the 11.5% in another study (Guo et al. Citation2019). Compared with the PAS rate (5.6–17.6%) reported in previous studies (Chen et al. Citation2017, Deans et al. Citation2018, Guo et al. Citation2019), it was 53.9% in the present research, significantly higher than before. One important reason may be that only patients with moderate and severe adhesions were included in this study, while a large number of patients with mild adhesions were included in other studies. Furthermore, unlike the previous studies, we included patients who had miscarriages and all patients with placenta accreta, increta, and percreta when calculating the incidence of PAS. Hysterectomy is the first line of management in PAS so far. However, no hysterectomy, maternal morbidity, or mortality occurred. We hypothesised this may be due to the low proportion of placenta increta or percreta in this study.
The classification of IUA and the basic description of the relationship between the extent of adhesions and the rate of pregnancy and live birth have been commonly described (Zhao et al. Citation2017, Hui et al. Citation2018). In this study, the AFS score of IUA in the PAS group was higher, and the miscarriage rate was significantly increased, indicating, among others, that the more severe the AFS grade, the worse the pregnancy outcome. To the best of our knowledge, this is the first study that demonstrated the positive correlation between the AFS grade and the prevalence of PAS. Prior studies considered IVF pregnancy an independent risk factor for PAS (Kyozuka et al. Citation2019, Imafuku et al. Citation2021), whereas our study suggested an association, but regression analysis showed it did not reach a significant difference. Similar to other studies, the occurrence of PAS was independent of age (Imafuku et al. Citation2021), as was the association between PAS and BMI (Kyozuka et al. Citation2019). Previous studies reported that gravidity and parity were significantly higher in PAS patients versus those without (Martimucci et al. Citation2019). Short interval pregnancy (Einerson et al. Citation2020, Munoz et al. Citation2021), prior CS, and invasive gynaecologic procedures (Baldwin et al. Citation2018, Imafuku et al. Citation2021) were independently associated with PAS. However, there were no significant differences between groups in our research. As is well known, recurrent miscarriages and intrauterine surgeries are risk factors for adhesion (Berman Citation2008, Hooker et al. Citation2014). Therefore, the subjects in this study had similar pregnancy histories and invasive gynaecologic procedures.
The most important focus of this study was the impact of time interval from adhesiolysis to pregnancy on PAS in IUA women. Numerous researchers either described IUA without reporting time intervals (Zhang et al. Citation2020) or only displayed time intervals without discussing its influence on obstetric outcomes in depth. The median time to conception was 7 months, and the time to conception leading to a live birth was 15 months in IUA women (Hooker et al. Citation2021). Another study showed that mean time to conception was equivalent in the mild (11.5 months), moderate (12.8 months), and severe (14.2 months) IUA women (Roy et al. Citation2010). A recent report found no correlation between time interval from adhesiolysis to pregnancy and placenta accreta in IUA women (Zhang et al. Citation2022). In contrast, our study found that IUA women who became pregnant in the second year after adhesiolysis had a higher rate of PAS during pregnancy, and the median time to PAS was 16.00 months. Short-interval pregnancy is supposed to be a hazard factor for adverse obstetric outcomes such as preterm delivery, low birth weight (Ihongbe et al. Citation2018), and uterine rupture in the next pregnancies after CS (Stamilio et al. Citation2007). Some investigators supported the positive correlation between short-interval pregnancy and the incidence of PAS (Munoz et al. Citation2021). Those previous findings may be based on the hypothesis that incomplete wound healing without enough time would result in adverse placenta-related diseases (Stamilio et al. Citation2007). It is worth noting that defective wound healing also occurred in postoperative IUA women. On the contrary, the risk of PAS in the second year after adhesiolysis was significantly higher than that in the first year. Compared with the pregnancies achieved in the first year, the risk of PAS after the second year was increased by 2 times, though the difference was not statistically significant, which may be due to the small sample size in this study. One possible way to explain this phenomenon is that the uterus cavity in postsurgical IUA women, with a high rate (3.1% to 27.3%) of reformation of adhesions (Yu et al. Citation2008, Hanstede et al. Citation2015), was fibrous and obliterated gradually as time went on. As researchers (Einerson et al. Citation2020) proposed a new commentary on the mechanism of PAS, arguing that defective decidua and uterine scar dehiscence create an access route for chorionic villi to get deep within the uterine wall, not being a disorder of destructive trophoblast invasion, we assumed that more severe defective decidua and uterine scar affecting the implantation of embryo, caused by uterine cavity fibrosis over time in the postoperative IUA women, lead to a higher risk of PAS ultimately.
The present study has some limitations. Firstly, this is a retrospective study, with some information obtained by telephone interviews. A prospective study, providing overall accurate clinical data, is needed, as it could provide more convincing results. In addition, because we did not get all pathological reports, it was impossible to analyse the risk and outcomes for different types of PAS, though describing the overall incidence of PAS could basically meet the needs of this study. As the previous study reported different obstetric outcomes in the percreta group and increta group (Zhang et al. Citation2019), further studies are needed to elucidate risk factors and outcomes in different types of PAS.
The present study indicates that severe IUA is a high risk for PAS in IUA women. We assume that prolonged adhesiolysis to pregnancy interval may be considered a significant risk factor for PAS in IUA women. Finally, more attention should be paid to prepregnancy, antenatal, and intrapartum surveillance in the IUA women managed by adhesiolysis. Meanwhile, a population-based prospective study investigating the specific mechanism of PAS in pregnancies after a longer interval, and detailing the risk factors and outcomes according to different types of PAS in postoperative IUA women, is recommended to provide more robust support for our conclusion.
Ethics Statement.docx
Download MS Word (585.5 KB)Acknowledgments
We are grateful for the participation of the patients. We thank the clinical personnel who supported this study.
Disclosure statement
The authors have no conflicts of interest relevant to this article.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article or its supplementary materials.
Additional information
Funding
References
- Anon 1988. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, mullerian anomalies and intrauterine adhesions. Fertility and Sterility, 49 (6), 944–955.
- Baldwin, H. J., et al., 2017. Maternal and neonatal outcomes following abnormally invasive placenta: a population-based record linkage study. Acta Obstetricia et Gynecologica Scandinavica, 96 (11), 1373–1381.
- Baldwin, H. J., et al., 2018. Antecedents of abnormally invasive placenta in primiparous women: risk associated with gynecologic procedures. Obstetrics and Gynecology, 131 (2), 227–233.
- Berman, J.M., 2008. Intrauterine adhesions. Seminars in Reproductive Medicine, 26 (4), 349–355.
- Chen, L., et al., 2017. Reproductive outcomes in patients with intrauterine adhesions following hysteroscopic adhesiolysis: experience from the largest women’s hospital in China. Journal of Minimally Invasive Gynecology, 24 (2), 299–304.
- Deans, R., et al., 2018. Live birth rate and obstetric complications following the hysteroscopic management of intrauterine adhesions including Asherman syndrome. Human Reproduction (Oxford, England), 33 (10), 1847–1853.
- Einerson, B.D., et al., 2020. Placenta accreta spectrum disorder: uterine dehiscence, not placental invasion. Obstetrics and Gynecology, 135 (5), 1104–1111.
- Guo, E.J., et al., 2019. Reproductive outcomes after surgical treatment of asherman syndrome: A systematic review. Best Practice & Research. Clinical Obstetrics & Gynaecology, 59, 98–114.
- Hanstede, M.M., et al., 2015. Results of centralized Asherman surgery, 2003-2013. Fertility and Sterility, 104 (6), 1561–1568 e1.
- Hooker, A.B., et al., 2021. Reproductive performance of women with and without intrauterine adhesions following recurrent dilatation and curettage for miscarriage: long-term follow-up of a randomized controlled trial. Human Reproduction (Oxford, England), 36 (1), 70–81.
- Hooker, A. B., et al., 2014. Systematic review and meta-analysis of intrauterine adhesions after miscarriage: prevalence, risk factors and long-term reproductive outcome. Human Reproduction Update, 20 (2), 262–278.
- Hui, C.Y., et al., 2018. Clinical and reproductive outcomes following hysteroscopic adhesiolysis for asherman syndrome in an asian population. Annals of the Academy of Medicine, Singapore, 47 (1), 36–39.
- Ihongbe, T.O., et al., 2018. Short interpregnancy interval and adverse birth outcomes in women of advanced age: a population-based study. Annals of Epidemiology, 28 (9), 605–611.
- Imafuku, H., et al., 2021. Clinical factors associated with a placenta accreta spectrum. Placenta, 112, 180–184.
- Kyozuka, H., et al., 2019. Risk factors for placenta accreta spectrum: findings from the Japan environment and Children’s study. BMC Pregnancy and Childbirth, 19 (1), 447.
- Martimucci, K., et al., 2019. Interpregnancy interval and abnormally invasive placentation. Acta Obstetricia et Gynecologica Scandinavica, 98 (2), 183–187.
- Munoz, J.L., et al., 2021. Short interval pregnancy is associated with pathology severity in placenta accreta spectrum (PAS). The Journal of Maternal-Fetal & Neonatal Medicine, 35(25), 8863–8868.
- Oyelese, Y. and Smulian, J.C., 2006. Placenta previa, placenta accreta, and vasa previa. Obstetrics and Gynecology, 107 (4), 927–941.
- Pabuçcu, R., et al., 1997. Hysteroscopic treatment of intrauterine adhesions is safe and effective in the restoration of normal menstruation and fertility. Fertility and Sterility, 68 (6), 1141–1143.
- Roy, K.K., et al., 2010. Reproductive outcome following hysteroscopic adhesiolysis in patients with infertility due to Asherman’s syndrome. Archives of Gynecology and Obstetrics, 281 (2), 355–361.
- Sonan, Y., et al., 2018. Placenta accreta following hysteroscopic lysis of adhesions caused by asherman’s syndrome: a case report and literature review. Case Reports in Obstetrics and Gynecology, 2018, 6968382.
- Stamilio, D. M., et al., 2007. Short interpregnancy interval: risk of uterine rupture and complications of vaginal birth after cesarean delivery. Obstetrics and Gynecology, 110 (5), 1075–1082.
- Thurn, L., et al., 2016. Abnormally invasive placenta-prevalence, risk factors and antenatal suspicion: results from a large population-based pregnancy cohort study in the Nordic countries. BJOG: An International Journal of Obstetrics and Gynaecology, 123 (8), 1348–1355.
- Yu, D., et al., 2008. Asherman syndrome–one century later. Fertility and Sterility, 89 (4), 759–779.
- Zhang, H., et al., 2019. Maternal and neonatal outcomes of placenta increta and percreta from a multicenter study in China. The Journal of Maternal-Fetal & Neonatal Medicine , 32 (16), 2622–2627.
- Zhang, L.-P., et al., 2020. The incidence of placenta related disease after the hysteroscopic adhesiolysis in patients with intrauterine adhesions. Taiwanese Journal of Obstetrics & Gynecology, 59 (4), 575–579.
- Zhang, Y., et al., 2022. Analysis of risk factors for obstetric outcomes after hysteroscopic adhesiolysis for Asherman syndrome: A retrospective cohort study. International Journal of Gynaecology and Obstetrics: The Official Organ of the International Federation of Gynaecology and Obstetrics, 156 (1), 89–94.
- Zhao, J., et al., 2017. Dominant factors affecting reproductive outcomes of fertility-desiring young women with intrauterine adhesions. Archives of Gynecology and Obstetrics, 295 (4), 923–927.