
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
The efficient deployment of resources in home-based care is considered crucial for the sustainability of health and social care systems worldwide. The aim of this study was to identify and review operational research approaches to support decision-making in home health care. We identified a set of linked decisions at different planning levels (strategic, tactical, operational) and conducted a systematic review of operational research approaches used to address these decisions. We also sampled OR literature applied to analogous decisions in other settings. The 77 papers selected focused predominantly on solutions for staff-to-patient allocation, visit scheduling and staff routing, few of which were adopted by organisations. Few studies dealt with tactical decisions of team size and composition or strategic decisions of districting, and we found no studies on contract design for commissioning home health care, on staff role definitions or on reassessment of patient need. Integrative work is scarce and the aspects of system performance considered are variable and diverse. For these reasons the literature does not provide guidance for home health care services aspiring to effective and coherent decisions across planning levels. OR approaches from other areas of application provide some insights for future research aimed at addressing this shortfall.
1. Introduction
Home health care (HHC) (the face-to-face delivery of care by a worker in a patient’s or client’s home) is seen as an important component of the health care sector and one that presents a distinct set of decision problems for those designing, funding, providing and working within such services (Hulshof et al., Citation2012). It can be argued that the importance of HHC is increasing due to its potential role in addressing two key policy initiatives within health and social care across many nations: reducing use of and stays within hospitals, and reducing demand for long-term residential care facilities by prolonging the time that people can live in their own home, including at the end of life (NHS England, Citation2014; Monitor, Citation2015).
As noted in Burgess (Citation2012), patients, professionals and the organisations that commission or provide home health care may all have different notions of what improved system performance means to them. For instance, patients may value punctual visits or visits within preferred time windows, staff may value fair distribution of work within or between teams, and provider organisations may want to reduce the amount of unproductive time that staff spend travelling. The complexity of home health care and the relationships and potential trade-offs between such aspects of system performance make HHC amenable to operational research approaches.
The decision problems associated with HHC include logistic problems well studied within the Operational Research (OR) literature, and Cissé et al. (Citation2017) and Fikar and Hirsch (Citation2017) provide technical reviews of the state-of-the-art in routing and scheduling of HHC staff. While conceptually restricted to the delivery of health care services rather than personal social care, the blurred distinctions in different settings, and the scope for integration and coordination of some health and personal social care services delivered in the home mean that some literature is common to both. Other reviews by Gutiérrez and Vidal (Citation2013) and Sahin and Matta (Citation2015) map the extant literature onto a broader framework of decision problems related to the design and delivery of HHC services. These decision frameworks reflect the hierarchical nature of decisions in HHC from a supply chain perspective. Both reviews highlight that there is abundance of work in some operational domains and less work in strategic and tactical decision making. Another finding of both reviews is that there is little explicit recognition of this hierarchy within the papers they reviewed. The authors point out that this undermines the potential benefits of improved operational decision making by not making clear the strategic and tactical decisions required to create a context in which OR approaches to operational decisions can have most impact.
The research questions raised by these previous reviews include:
What combinations and hierarchies of decisions have been addressed in the OR literature on home health care and what aspects system performance have been considered when addressing each decision?
Can a group of research works be identified that, together, provide a comprehensive (in terms of the decisions addressed) and coherent (in terms of the aspects of system performance considered) set of OR solutions to decision problems for Home Health Care?
What decisions relevant to home health care and amenable to OR have been given insufficient attention in the literature?
In this paper we address these research questions by:
counting the numbers of papers that address different combinations and hierarchies of decision;
reviewing how the performance of HHC systems is conceived within the literature and mapping the different aspects of system performance considered within the literature to the different decisions addressed;
clustering papers by the aspects of performance considered and identifying the sets of decisions spanned within each cluster;
comparing the set of decisions addressed in the literature to a hierarchical framework of decisions in HHC compiled with input from discussions with HHC decision makers in North East London.
As a secondary research question, we sought to identify OR approaches used outside HHC that could be adapted to address decision problems neglected by the set of papers identified in this review.
Our review has been undertaken as part of a study in which we are working with a number of home health care organisations. While these organisations face problems of districting, service definition, contract design and capacity planning, their efforts to improve efficiency focus largely on what they term as “workforce innovations”, essentially changes to the work done by clinicians and how this work is organised. As well as including interventions to tackle operational decision problems addressed in the OR literature, these workforce innovations include interventions to increase the use of information technology to cut administration time and reduce the need for staff routes to start and/or end routes at a base, introducing new scoring systems intended to quantify workload more fairly, and considering the creation of new workforce roles. Some of these alter the nature of operational problems addressed in the literature and/or facilitate the implementation of OR solutions, whereas others frame their own decision problems. This motivated us to bring to the fore the explicit and implicit assumptions made in the literature about workforce structure, terms of employment, preferences and agency. We consider how these underpinning assumptions may influence the feasibility, acceptability or potential benefits associated with different OR approaches in the context of the workforce arrangements that prevail in different health care systems.
This work contributes to the body of operational research on home health care by updating previous reviews, providing an analysis of the extent to which the current OR literature provides a basis for improved, coherent decision making across the spectrum of decisions faced in home health care, and identifying priority areas for future research, in terms of decision problems to address and contextual and environmental features of home health care systems that should be reported alongside model formulations and solution approaches.
2. Methods
2.1. Decision problems in home health care
We identified an initial set of decisions at different planning levels relevant to the design and delivery of HHC from Hulshof et al. (Citation2012). We split some of these into multiple decisions, for example Hulshoff’s ‘Visit (re-)scheduling’ was separated into four discrete decisions, ‘allocation of staff’, ‘visit scheduling’, ‘routing of visits’ and ‘short-term fixes’, whilst acknowledging that sometimes these decisions are combined within modelling approaches in the literature.
We then broadened this based on discussions with HHC stakeholders in North East London, which comprised 29 meetings and 3 workshops with people working in the HHC system, including managers and frontline nursing staff from the local home health provider and commissioners of home health services, managers of local voluntary organisations providing support to home care patients and their families and a group of service user representatives. In relation to the set of decisions considered in this paper, our findings from these discussions led us to augment the frameworks of home health care decisions presented elsewhere in the literature in the following ways:
Stakeholders are currently considering the introduction of new workforce roles that blend skills associated with multiple roles, including across different traditional professional disciplines (e.g. hybrid nursing and physio support roles). We therefore felt that defining workforce roles was a decision that needed to be differentiated from that of resource dimensioning or allocation (as used by Hulshof et al., Citation2012), which generally focus on determining the number of staff needed from existing roles.
The development of home health care plans for patients is not explicitly covered by Hulshof et al. (Citation2012) or previous reviews on HHC (e.g. Gutiérrez & Vidal, Citation2013; Sahin & Matta, Citation2015 and Cissé et al., Citation2017), but we found it to be an important decision that stakeholders face, which relates not only to operational decisions about scheduling visits but also to tactical decisions regarding team size and composition. Related to this, the timing and nature of reassessments of patient need, which feed into amendments to care plans, was also considered an important decision by stakeholders (and absent from Hulshof et al., Citation2012) and the frameworks presented in the previous reviews).
Many patients receive multiple home-based health or care services and informal support, and stakeholders felt it was important to consider how these services can coordinate effectively. Although Sahin and Matta (Citation2015) refer to decisions about partnership strategy at a strategic level and the identification of partners at a tactical level, they do not make explicit coordination with other services at an operational level, and this is also absent in Hulshoff’s taxonomy (Hulshof et al., Citation2012) and the other HHC review articles (Gutiérrez & Vidal, Citation2013; Cissé et al., Citation2017).
There are important patient-level service processes that feed into the decisions, such as identifying and specifying a patient’s need(s), and some stakeholders focus primarily on the main patient-level output from the decisions, namely the delivery of a home visit. Therefore, in line with Gutiérrez and Vidal (Citation2013), who include an explicit dimension on service processes in their framework, we added the decision inputs ‘need identified’ and ‘referral’ to our framework along with the decision output ‘home visit’. We also made explicit the distinction between decisions and their inputs and outputs.
In addition to incorporating these findings into our framework, we identified logical links and hierarchical orderings between the decisions to ensure consistency with existing descriptions of HHC from a supply chain perspective (Gutiérrez & Vidal, Citation2013; Sahin & Matta, Citation2015). We then devised a graphical representation of this decision framework (), in which we placed the output of a home visit on the right hand side of the page and then worked back through the decisions (and other inputs) necessary for a specific professional to visit a specific patient at a particular time on a particular day. This led to a group of operational decisions being placed in the centre of the page. Within this left-to-right flow of quasi-precedence relationships, we chose to display organisations’ prior strategic and tactical decisions as feeding into operational decisions from above, with prior patient-specific decisions feeding into operational decisions from below. Both of these strands were considered to be dependent on a decision around the definition of service to be offered and the terms of access for patients, with this placed at the far left of the page.
Figure 1. A graphical representation of the set of decision problems identified as associated with the design and operation of a home health care service. The framework diagram shows a flow of decisions from the definition of the service to delivery of care at a patient’s home, with some key inputs related to the patient shown at the bottom.
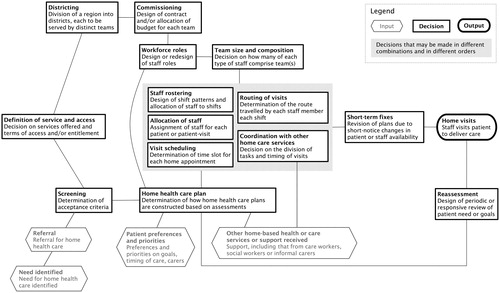
Where possible, our working definition of each decision was made consistent with the nomenclature used in Hulshof et al. (Citation2012).
2.2. Literature search
2.2.1. Operational research applied to home health care
We conducted a systematic review to assess the extent to which the development and adoption of OR approaches address the identified set of HHC decision problems.
We searched the electronic database Web of Science (https://wok.mimas.ac.uk/) using a combination of the search terms listed in Appendix 1 (Tables A1 and A2), and extracting records with:
at least one of the terms related to OR methods set out in Table A1 in the article title, abstract or keywords (informed by Palmer et al. Citation2018);
AND
at least one of the terms related to the setting of HHC set out in Table A1 in the article title, abstract or keywords;
AND
at least one of the decision terms set out in Table A2 in the article title, abstract or keywords.
Note that our choice of search terms respected that the distinction between health care and social/personal care activities can differ among systems, meaning that some of the papers identified relate to the delivery of personal social care by non-health professionals.
We considered all publications in English with no constraints on publication type or year. The search was run on the 28th September 2018. All publications found were then assessed against this sequence of criteria:
Peer-reviewed: The titles and abstracts of only peer-reviewed articles were assessed.
Title/abstract: Review articles were subject to full text reading if the title and/or the abstract suggested that a subset of the papers reviewed focused on tackling decisions in HHC through OR approaches. Other publication types (e.g. research articles, peer-reviewed conference proceedings, book chapters) were subject to full text reading if the title and/or abstract suggested that the work focused on tackling one or more of the decisions of interest in HHC through an OR approach.
Full text: Articles were retained if the above criterion was still satisfied on reading of the full text and, for non-review articles, if the description of the approach was sufficiently detailed to identify modelling assumptions, formulation and outputs.
Additional research papers identified from accepted review articles were then subject to the same sequence of inclusion criteria. We only extracted data from non-review article publication types.
2.2.2. Operational research applied to analogous decision problems
We conducted an additional scoping review of OR approaches to decisions analogous to those in HHC that have been developed for other settings outside HHC. To do this, we used the same search strategy described in 2.2.1 but without the “Settings” terms and with some HHC specific “Decision” terms adapted (for instance “nurse” was replaced with “worker” in searches – see Table A3 in Appendix 1 for full details). Defined this way, analogous decisions included, for example, the scheduling and routing of workers providing maintenance services at a number of client locations or the size and composition of teams in other industries. Because of this broad definition and the anticipated volume of papers related to some decisions, we restricted this scoping review to review articles. From the search results associated with each analogous decision, we studied the two most recent review articles describing decision problems where we considered the structure of the problem and the nature of objectives/requirements to be similar to those we found in HHC settings.
2.3. Data extraction
The study team agreed on an initial data extraction table for the systematic review. Data extracted included the aim of the study, the HHC decisions addressed, the planning horizon considered, the modelling and solution approaches taken, the aspects of performance considered (and associated metrics) and the level of engagement with practice. One reviewer (LG) carried out the article search and selection, reading and data extraction, making an initial assessment as to the decision(s) in HHC addressed. In cases where the same aspect of performance was labelled differently in different publications (e.g. “caregiver utilisation”, “worker utilisation”, “resource utilisation”), we chose a label (e.g. “staff utilisation”) for our analyses. For papers in which the aspects of HHC system performance being promoted were not explicit, a judgement was made based on the objective functions and constraints of models and on the presentation of results.
To identify and to try to minimise the impact of subjective assessments in extracting data, a second reviewer (MU) read 20% of the selected papers sampled at random but with at least one paper per decision where possible. Data extracted by the second reader was compared with that obtained from first reading. Any systematic difference in extraction or interpretation of data was resolved through discussion with the senior author (SC). This process led to the iterative refinements of the data extraction table allowing us to capture important distinctions between papers relevant to our research questions. For instance, we refined our mapping of papers to HHC decisions to specify whether papers focused on and proposed a quantitative model for a given decision, considered that decision as a secondary outcome, made explicit assumptions about that decision as a model input, or simply made reference to that decision. Finally, the first reviewer revisited the completed data extraction table to ensure a consistent presentation and level of detail across all entries.
2.4. Analysis
For each paper, we identified the partial hierarchy of decisions in HHC considered. We then counted the number of papers that considered each unique hierarchy and produced a graphical summary of these data based on the graphical representation of the decision framework devised at section 2.1. For each decision, we then tabulated the OR approaches and accompanying solution methods used in the literature and, separately, the aspects of system performance considered.
2.4.1. Paper clustering
One of our aims was to identify whether there are groups of papers that, between them, provide a comprehensive and coherent basis for decision making across strategic, tactical and operational decisions. To do this, we adapted a clustering algorithm to find groups of papers that were coherent in terms of how system performance was conceived and then looked at how comprehensive the set of decisions addressed in each cluster was. To explore the coherence of papers in terms of the aspects of system performance considered, we computed a similarity score between all possible pairs of papers
and
:
with
denoting the set of aspects of system performance considered in paper
(the higher the overlap between papers
and
the closer
to 1). We then built an undirected, weighted graph with each node denoting a paper and an arc with weight
existing between node
and node
if
We identified each connected component (i.e. set of nodes in the graph that are linked to each other by paths) in the obtained graph as a cluster of papers dealing with similar sets of aspects of system performance. Note that the lower the cut-off, the higher the average size of the connected components in the graph. We chose the cut-off (0.6) as the minimum real number such that at least two of the obtained clusters were formed of more than four papers.
3. Results
3.1. Decision framework
shows the set of decisions identified as important to the design and delivery of HHC services, spanning the strategic, tactical and operational planning levels. There is an implied hierarchy, or logical precedence relationship between some decisions, whereas others may be made in combination or in different sequences.
3.2. Literature search output
3.2.1. Summary of articles retrieved and data extracted
Our search identified 222 articles, with 4 review articles and 62 non-review articles meeting our inclusion criteria (). Fifteen additional non-review articles identified in the 4 review articles were accepted. shows the data extracted from the 77 non-review articles.
Figure 2. Literature search flow diagram, showing the number (N) of articles identified, meeting the inclusion criteria of peer-review, and retained for analysis after title/abstract assessment and after full-text reading. The left-hand side of the diagram shows the flow for non-review articles, whilst the right-hand side shows our process for identifying additional research papers from accepted review articles (which were then subject to the same sequence of inclusion criteria). We only extracted data from non-review article publication types.
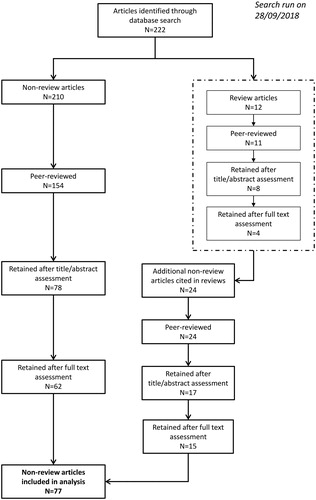
Table 1. Data extracted from the non-review article publications that met the selection criteria.
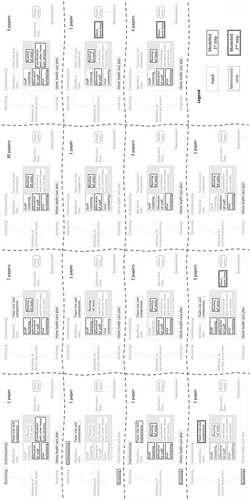
3.2.2. Decision hierarchies
Among the 59 of the 77 papers that addressed more than one decision, we identified 15 distinct partial hierarchies of decision (see ). The most commonly considered partial hierarchy (30 papers) was where staff rosters and home health care plans are taken as input and the allocation of staff to patients, appointment schedules and the routing of staff are decided in combination.
Figure 3. The set of partial decision hierarchies of decision among the 59 of 77 reviewed papers that considered more than one of the identified decision problems in home health care. Each tile shows a different subset of decisions, with the number of papers considering precisely that combination of decisions given at the top right of the tile. The line-style used for the boxes denotes whether, within those papers, the respective decisions are: merely mentioned as relevant; viewed as a necessary prior step but not modelled; modelled at the first (or only) step of analysis; or modelled at a second step of analysis.
3.2.3. Or approaches in HHC
shows the OR approaches and solution methods adopted to address each of the decision problems in HHC. We summarise our findings below.
Table 2. OR approaches by decision.
All studies of districting use mixed-integer programming. Two aspects of system performance are addressed either using different models, each with one aspect as the objective and the other as a hard constraint (Benzarti et al., Citation2013), or by minimising a weighted sum of two components (Blais et al., Citation2003). Lin et al. (Citation2017) develop a greedy algorithm to rapidly obtain near-optimal solutions, whereas the other studies apply existing algorithms and focus on their applicability in the real world.
Mathematical programming approaches (integer, mixed/integer, stochastic) are also applied in 3 of the 4 studies about team size and composition (Rodriguez et al., Citation2015; Nasir & Dang, Citation2018; Nasir et al., Citation2018). In the other paper, Koeleman et al. (Citation2012) calculate the impact on workforce size of a Markov decision process framed to give optimal patient admission (screening) policies given the demand for service.
In other papers addressing this decision of patient screening, Zhang et al. (Citation2015) and Nasir and Dang (Citation2018) use mixed-integer programming and constraint programming, respectively, proposing meta-heuristic algorithms to deal with the computational complexity of the problem. De Angelis (Citation1998) jointly models the commissioning and screening decisions using a linearly approximated stochastic programming model, with resource needs for different types of patients estimated using an existing stochastic model and resource limits (budget) included as constraints. The objective is to maximise the weekly number of AIDS patients admitted to home care, with an implicit assumption that this would lead to the best allocation of resources.
The vast majority of the studies addressing staff rostering, visit scheduling, allocation of staff and routing visits propose mixed-integer programming formulations based on the vehicle routing problem and incorporating one or more additional features (e.g. time windows, activity interdependencies, workload balance). The high computational cost associated with such formulations is usually tackled by developing heuristic algorithms able to produce good solutions in a reasonable amount of time. Less common approaches include robust optimisation (Carello & Lanzarone, Citation2014), stochastic programming (Yuan et al., Citation2015; Lanzarone & Matta, Citation2012; Lanzarone et al., Citation2012; Errarhout et al., Citation2016), multi-objective optimisation (Maya Duque et al., Citation2015; En-Nahli et al., Citation2015), constraint programming (Nickel et al., Citation2012; Cattafi et al., Citation2015), and clustering techniques (Quintana et al., Citation2017). Short-term fixes to such solutions are also addressed in several of these publications. For instance, Lin et al. (Citation2018) use mixed-integer programming and Nickel et al. (Citation2012) use constraint programming, both proposing two-step approaches: the first step determining a rostering/scheduling/allocation/routing solution, the second step minimising deviations from that solution in case of disruptions. Focused on practice, Begur et al. (Citation1997), Eveborn et al. (Citation2006) and Eveborn et al. (Citation2009) also use (mixed-)integer programming as a core component of interactive decision support tools producing solutions for a scheduling/allocation/routing problem and enabling the user to introduce real-time barriers downstream, with solutions automatically adapted.
Coordination of care between different professionals or different services is modelled using (mixed)-integer programming approaches and solved using bespoke heuristic algorithms (Mankowska et al., Citation2014; Decerle et al., Citation2016; Decerle et al., Citation2018).
3.2.4. Approaches from the non-HHC literature
In this section, we summarise our findings on OR approaches to analogous decisions in settings other than HHC. In particular, we focus on decisions that are not currently covered by the HHC literature or that are covered but might benefit from OR approaches adopted in other fields.
The problem of service definition and access has similarities to investment portfolio selection: choosing the set of home health care services to offer and identifying the corresponding target patients can be seen as a form of investment selection (with return expressed as a combination of monetary and utility terms) over a given planning period. Masmoudi et al. (2018) review multiple objective deterministic and stochastic programming models for this problem. The aim is to select the least risky set of investments (services in HHC settings) for a given level of return, which need not be monetary. As discussed in deLlano-Paz et al. (Citation2017), the recent use of portfolio theory in energy planning challenges least-cost approaches that favour fossil fuels and can incorporate multiple stakeholder perspectives.
While potentially unpalatable to many working in HHC, time-of-use pricing could have useful insights for patient screening. For instance, Chrysopoulos and Mitkas (Citation2018) discuss the use of multi-objective particle swarm optimisation to customise time-of-use pricing to deter some customers from requesting service at peak times.
Related to team size and composition, Boucher et al. (Citation2007) survey how competence-related concepts are modelled and formalised in the literature on industrial performance improvement. This literature focuses on interaction and complementarity between team members, distinct from the HHC literature focus on just the team configurations that best meet demand. Aspects analysed include team building and competence allocation. Specifically, studies are cited that start from “Belbin’s self-perception inventory” to develop formal models and/or decision support systems to assist managers in team composition (e.g. Sommerville & Dalziel, Citation1998; Chen & Lin, Citation2004).
Decisions on the home health care plans made for patients can be seen as analogous to the elicitation of and response to “customer requirements”. A potentially relevant stream of research is that dealing with intelligent design for customised products, defined by Zhang et al. (Citation2017) as products “designed to satisfy the customer’s individual and diversified requirements as quickly and at as low a cost as possible”. They cite Quality Function Deployment (Akao, Citation2004) as one approach to map product features to customer requirements that has been used in service design (see for instance Yan et al., Citation2016).
For the decision of staff rostering, the HHC literature found in our systematic review does not address shift design, whereas in other contexts this problem is addressed using queueing theory (Green et al., Citation2006) and integer programming (Ingolfsson et al., Citation2010).
Approaches analysing the benefits of information flow within and between organisations seem relevant to the coordination of home care between services. Durugbo et al. (Citation2013) review quantitative flow analysis methods for improving organisational performance. Among the cited references, Barua et al. (Citation1997) develop a game theory model of information exchange to analyse the exchange of usable intra- and inter-organisational information between decision units and use the idea of “cheap talk” as a mechanism for coordinating inter-organisational activities.
In our search we did not identify decisions directly analogous to the design of processes for reassessment of patient need. However, we consider that there are similarities to optimal control problems, consisting of designing and dimensioning interventions on a system over time (and possibly accounting for measurement uncertainties) in order to optimise the behaviour of that system. In HHC settings, such interventions would consist of updating patients’ home health care plans based on changes to their health status. For instance, Büyüktahtakın and Haight (Citation2018) reviewed such an approach in the markedly different context of invasive species management.
Finally, our search did not identify OR literature related to decisions analogous to commissioning or workforce role definition, nor work outside HHC to augment approaches to the decisions of allocation, scheduling, routing or short-term fixes.
3.2.5. Aspects of system performance in home health care
As part of the data extraction, we identified from the stated aims of each paper, or from the objective functions and constraints within the models proposed, the different aspects of the HHC system’s performance considered to contribute to service quality in that paper (for instance workload balance or continuity of care).
We identified 21 different aspects of system performance and 55 different related metrics (see Appendix 2) across the 77 accepted articles. reports the number of papers that consider each aspect for each decision problem (see for a definition of the decisions).
Table 3. Aspects of system performance.
We briefly discuss below the aspects of system performance that authors use to define the quality of solutions to different decision problems and their alignment with the perspectives of different stakeholders in HHC. First, it is worth noting that over 30 of the papers reviewed explicitly consider the productivity of the staff responsible for making these decisions. This acknowledgement of the (often considerable) planning time that staff currently devote to these tasks and the extent to which this could be reduced by the adoption of OR solutions brings a focus in the literature on the process of decision support and on heuristic approaches that reduce the high computational times associated with existing solution methods (e.g. An et al., Citation2012; Eveborn et al., Citation2006).
Due to the dominance in the literature of scheduling, allocation and routing problems (usually modelled as a vehicle routing problem), staff travelling is the most represented aspect of system performance. In particular, a common objective is to minimise travelling costs (or distance, or time) incurred by the provider for daily home visits. While this reflects a provider perspective (cost minimisation), some authors augment their formulation to penalise or preclude solutions that do not take the presumed or elicited interests of patients and/or staff into account.
Patient perspectives are manifest in preferred time slots for visits (“time windows”) in the model formulation, either as hard constraints (Du et al., Citation2017; Akjiratikarl et al., Citation2007), or penalties in the objective function (Braekers et al., Citation2016; Mankowska et al., Citation2014), or both (Bertels & Fahle, Citation2006). Overall tardiness is also used as a measure of patient experience and modelled as a component of the objective function to be minimised (Mankowska et al., Citation2014; Rest & Hirsch Citation2016). Some papers consider patients’ preference for specific staff to carry out the visit (usually through penalties in the objective function) (Bowers et al., Citation2015; Braekers et al., Citation2016).
Continuity of care is another aspect of system performance important from a patient perspective. Ensuring that the same staff visit a given patient during the whole period of care can be in conflict with workload balance (staff perspective) and cost containment (provider perspective), however it has been shown that OR approaches can achieve a good level of continuity of care and a fair workload balance with limited cost increase (Carello et al., Citation2018). The most common measure for continuity of care is the number of staff per patient (Cattafi et al., Citation2015; Hewitt et al., Citation2016), though other metrics are also used such as number of staff deployed on tours of similar characteristics (Wirnitzer et al., Citation2016) or number of changes in the allocation of staff to a patient (Wirnitzer et al., Citation2016; Carello et al., Citation2018).
A related aspect of system performance that reflects a staff perspective is workload balance, with this measured in several publications through metrics such as the deviation of each member of staff’s workload from average workload (e.g. Benzarti et al., Citation2013). Some models account directly for a staff perspective by incorporating preferences for certain patients (Hiermann et al., Citation2015) or penalisation of staff waiting time (Trautsamwieser et al., Citation2011). Also, we note that approaches that minimise staff travel time or overtime (Braekers et al., Citation2016) may also reflect the perspectives of some staff.
We found few papers on the commissioning of HHC and the commissioner’s perspective is largely absent, although many models penalise or preclude solutions that fail to meet demand and one paper seeks to maximise the number of new patients accepted per week (De Angelis, Citation1998).
As with most complex systems, the models developed in HHC reflect intrinsic tensions and trade-offs between different aspects of system performance. For instance, Benzarti et al. (Citation2013) built two complementary models to solve the districting problem: i) one minimising the maximum size of districts (seen as desirable), with constraints on the imbalance of workload between districts; ii) one minimising the maximum deviation of district workload from the average workload, with maximum district size constrained. Their results show a clear tension between the two aspects. The more common approach of combining contrasting aspects of system performance in a single objective function is exemplified in Nasir and Dang (Citation2018), who tackle the decision of team size and composition by minimising a weighted sum of: staff travelling (measured through total distance travelled), staff costs (measured through wage costs), workload balance (measured through workload variability across staff), and demand satisfaction (measured through a cost of delaying patients).
While only a handful of papers study decisions that span different levels of planning, some aspects of system performance are considered in strategic, tactical and operational models. Specifically, staff travelling is considered in decisions of districting (Blais et al., Citation2003), team size and composition (Nasir & Dang, Citation2018), screening (Nasir & Dang, Citation2018) and in the vast majority of papers on rostering/scheduling/allocation/routing. In all these studies, the total distance travelled by staff is used consistently as a metric.
The level of demand satisfied is considered in models addressing decisions of screening and team size and composition (Nasir & Dang, Citation2018) and joint decisions of rostering, scheduling, allocation and routing (Nickel et al., Citation2012), using penalty costs for patient delays and unassigned visits respectively.
Workload balance among teams or individuals also features at different planning levels, with Benzarti et al. (Citation2013) minimising the maximum deviation of district workload from the average in strategic districting decisions and Cappanera et al. (2015) maximising the minimum staff utilisation rate within a district in operational decisions of scheduling, allocation and routing.
While these single aspects of system performance appear in papers across planning levels, clustering papers by the sets of performance measures considered tended to group papers addressing similar decision problems. Of the 10 (non-singleton) clusters of papers identified (see Appendix 3), two spanned planning levels, perhaps the most useful being a cluster of 9 papers that use a similar set of performance measures in dealing with decisions on districting and (in different combinations) rostering, scheduling, allocation and routing decisions.
3.2.6. Treatment of workforce
Part of our motivation for this review was to inform our research on workforce innovations relevant to the delivery of HHC, and so we had a particular interest in how the home care workforce was conceived within the papers reviewed. There is a range of such perspectives, reflecting differences in the nature and operations of the HHC organisations that authors were working with or studying.
Differentiation of staff by profession, seniority, qualification or mode of transport (e.g. Braekers et al., Citation2016) is a realistic feature of many models whereas, either because of the strategic purpose of the model or for the sake of simplicity, staff are viewed as a homogenous discrete resource (e.g. Lanzarone et al., Citation2010) or a homogeneous continuous (e.g. Koeleman et al., Citation2012) resource in others.
A key division in the literature is whether HHC staff (typically nurses) are treated as salaried employees or as a casual resource in the modelled systems. For instance, in Bard, Shao and Jarrah (Citation2014) the nurses that deliver care are paid hourly (with differential rates per activity), with optimal route construction offering cash-releasing savings to the organisation by providing solutions in which fewer nurse shifts are used and/or nurses working shorter shifts. In such systems, nurses state their availability to work as an input and then get allotted work as an output. As an aside, forcing hierarchical binary decisions on nurses regarding their availability to work (rather than eliciting preferences for periods to work, say) could arguably lead to suboptimal solutions for nurses and their hiring organisation.
Given the scope of the research presented in these articles, there is no consideration given to the equity of work allocation across different nurses or to the consistency of work allocated to individual nurses over time. In a context where nurses are an abundant resource, this may have no implications for the organisation, whereas if nurses are not abundant, unstable nurse incomes might make the organisation unattractive to nurses and pose a threat to services in the longer term.
In contrast, the work of Rodriguez et al. (Citation2015) to inform the dimensioning of a salaried workforce is explicitly motivated by a wish to have a stable team of nurses, with job security implicit to this, reflecting a view in the organisation studied that this would benefit all parties.
For systems where nurses are considered permanent salaried staff, while there is some prospect of cost reduction through reduced overtime or optimal dimensioning of the workforce, the objectives of allocation, scheduling and routing models (e.g. Carello et al., Citation2018; Decerle et al., Citation2018; López-Santana et al., Citation2016) focus more on the opportunity costs of travel times and unutilised staff time.
Workload balance within or across teams also features in some papers (for instance Cattafi et al., Citation2015; Bowers et al., Citation2015). In the main, this is considered simply in terms of the number of visits allocated to staff, but Hertz and Lahrichi (Citation2009) assess instead the burden that different types of case present for different grades of staff.
Another feature of modelled systems is the degree of autonomy or agency that staff have. A number of modelled systems have scope for staff to express preferences over when they work (Maya Duque et al., Citation2015; Bertels & Fahle, Citation2006). In the setting studied by Hertz and Lahrichi (Citation2009), nurses have full autonomy over how they arrange their working day, with this precluding the development and use of centralised routing and scheduling algorithms. In other works, the modelled systems operate such that optimisation could work to the detriment of staff, for instance where staff travel costs and the time to their first appointment and home from their last appointment are not included in the objective function (e.g. Bennett & Erera, Citation2011) or where solutions are in line with the letter but perhaps not the spirit of working regulations (the 7-hour shifts in Cattafi et al., Citation2015 are partly driven by regulation that workers should have a half-hour break every 7 h).
3.2.7. Methods vs practice
Most of the papers reviewed focus on the development of new formulations and/or fast solution algorithms to better deal with model complexity. Few studies address the challenges of implementing the proposed approach in practice and the implications that these challenges have for the development of models and solution methods. We highlight some exceptions in what follows.
Although using randomly generated instances, Benzarti et al. (Citation2013) present their work on districting as a decision support system for managers in HHC, envisaging that staff would interact with the tool (by modifying relevant parameters) and adapt the suggested solutions. The districting solution obtained by Blais et al. (Citation2003) was actually adopted by their client who had provided the authors with real-world instances to validate the model.
Both works by Hindle et al. (Citation2000; Citation2009) were conceived to provide health care organisations with inputs for decisions on fund allocation (commissioning) at national level. The former study informed yearly allocation of funds for HHC to four areas in Northern Ireland, improving existing criteria already based on OR modelling by incorporating a “rurality” feature in the model. The latter, aimed to support HHC funding allocation across districts in England, was less successful due to the low survey response rate by local authorities in providing key input data to the researchers.
Begur et al. (Citation1997), Eveborn et al. (Citation2006) and Eveborn et al. (Citation2009) discuss the use of (mixed-)integer programming as a core component of interactive decision support tools producing solutions for the scheduling/allocation/routing problem and enabling the user to introduce real-time barriers downstream, with solutions automatically adapted (short-term fixes). In another scheduling/allocation/routing example, a HHC organisation implemented and tested the approach proposed by Maya Duque et al. (Citation2015), in collaboration with an external software company. The authors assisted the organisation during the early stage of implementation by developing and testing a prototype of the tool. They also worked with a district manager to compare solutions from the tool with manually-generated ones and to understand the level of acceptability of the former. The organisation also provided advice during the modelling process that helped to shape the approach taken. For instance, the authors present a two-stage solution strategy not relying on Pareto-optimality criteria because the organisation considered preferences to be more important than total distance travelled. Finally, software implementing the staff allocation models developed by Lanzarone et al. (Citation2012) was adopted by a HHC provider.
More often, algorithms in the literature were tested on simulated instances or instances generated from data provided by partner organisations. Among the latter, the model presented by Trautsamwieser et al. (Citation2011) for rostering, scheduling, allocation and routing decisions was developed in close connection with a health care organisation with plans to include it in their decision support systems; Wirnitzer et al. (Citation2016) mention a partnership with a home care organisation who provided a test instance and contributed to the assessment of different objective functions, one of which was used (manually) by the organisation; close collaboration with health care organisations who actively contributed to the modelling work is also mentioned in Cattafi et al. (Citation2015), although no details were given on any implementation. Among the papers related to patient screening, only Zhang et al. (Citation2015) mention a collaboration with an HHC organisation, which in their case provided advice on current admission policies.
4. Discussion
The strengths and weaknesses of a systematic approach to reviewing the literature are well rehearsed; while a reproducible and transparent approach to identifying papers for review, we acknowledge that search and selection of papers driven by keywords and prospective criteria can fail to identify relevant papers that could be found through other approaches. Although this has been mitigated by considering the reference lists of previous (non-systematic) review articles, we do not claim that our review contains all relevant papers. Additionally, we note that our decision framework is not exhaustive and that individuals, teams and organisations may face other decision problems specific to home health care that are amenable to Operational Research approaches. The other limitation intrinsic to our study design is that there is an inevitable degree of subjectivity in some of our interpretation of the intent and context of papers in the literature. That said, this systematic review and analysis of the OR literature on decision problems in home health care has yielded some valuable findingsFootnote1.
Previous reviews indicated that individual papers did not span the strategic, tactical and operational decisions faced in home health care. By studying the combinations and hierarchies of decision addressed in individual papers and by clustering papers that have a coherent view on system performance, one contribution of this work is to establish that there are no groups of papers that, between them, provide a comprehensive and coherent set of tools for strategic, tactical and operational decision-making in home health care. So while a home health care organisation could find approaches in the literature to problems at different planning levels, there would be no guarantee that tools chosen for operational decisions would not undermine the value of tools chosen for tactical or strategic decisions, due to the disparate aspects of system performance considered in different papers. Despite the negative results in this instance, as far as we are aware this use of clustering is novel in the context of systematic reviewing and has potential to enhance analyses of other literatures.
Other contributions of our work are that it has identified decisions in home health care amenable to operational research where there has been little or no research activity, and that is has highlighted contextual and environmental factors that should perhaps be included to enhance OR papers on home health care problems. These are presented below.
We found that the OR literature concerning HHC remains dominated by papers proposing models and solution methods for combinations of operational decisions concerning the rostering of staff, the allocation of staff to patient visits, the scheduling of visits and the routing of staff. Previous reviews (Cissé et al., Citation2017 and Fikar & Hirsch, Citation2017) have suggested a need for more stochastic formulations in such models and our review found that recent work has indeed incorporated stochastic patient demand, staff travel times and service times (for instance Shi et al., Citation2017a, Citation2017b, Citation2018; Yuan et al., Citation2018; Cappanera et al., Citation2018). Other advances since previous reviews include moves to explore alternative approaches to the multiple aspects of system performance acknowledged to be important in HHC, with for instance Liu et al. (Citation2018) and Carello et al. (Citation2018) using multi-objective optimisation, as suggested by Cissé et al. (Citation2017). This ambition to address more of the complexity inherent in HHC systems motivates the continued focus within the literature on the development of computationally efficient solution methods.
Our analysis shows some recognition of the hierarchy of decisions in home health care with many partial hierarchies addressed, but as stated above it remains the case that papers addressing strategic, tactical and operational decisions are missing from this literature. One defence of the research community on this point would be that Operational Researchers often take the pragmatic view of wanting to build models for the problem in front of them, which typically means models that serve the explicit decisions made by the organisation or team within an organisation that they are working with and, to a greater or lesser extent, adopting the perspective of that organisation or team. Another pragmatic consideration would be that strategic decision making often has a periodicity of many years with organisations rarely receptive to solutions that involve structural change unless they arrive at the right point in this cycle, whatever the promised benefits.
This sets up a tension between the potential value of “whole supply-chain” approaches and pragmatic considerations of implementation. This would be a stronger defence if there was a greater focus on implementation in this literature, yet few papers report successful implementation in the organisations they worked with or that supplied data. Indeed, there is arguably little value to home health care in further improvement of models and solution methods without greater attention given to challenges to implementation, and we repeat the call of Fikar and Hirsch (Citation2017) for more study of the organisational and social factors that inhibit and promote the adoption of innovations rooted in OR to decision processes in HHC.
Our review also highlights strategic and tactical decisions where there is insufficient literature. Specifically, we found little on the coordination of care across professions and organisations (although Nasir et al., Citation2018 make a valuable start on this), the design of contracts to support effective commissioning in HHC, the construction of home health care plans and role definitions within the workforce.
The lack of research on role definition is indicative of researchers accepting some of the choices made in HHC as fixed, or rather as not being choices. This fits a general pattern in the literature of HHC systems being presented as characterising “the HHC problem” rather than one instance of a HHC problem specific to the system or organisation that informed model development. For instance, models were, naturally, strongly influenced by the employment practices of the organisations studied and labour protections in place in that setting.
Other aspects of organisational context are apparent from, though not always made explicit in, descriptions of the organisational problems faced and in the models developed to address these problems. These include features of the environment in which an organisation is operating, such as whether it can choose what home care services it offers, the profiles of patient groups it accommodates or the individual patients it takes on within these groups, and what it is paid to do and on what terms. In some settings, these aspects constitute a choice of business model, in other settings they reflect the entitlements of citizens and the organisation of state provision or state funded provision. Similarly, the overarching organisational objective may be profitability, sustainability, meeting an explicit or implicit social contract, improving population health, or preventing or delaying the use of more expensive health services.
Other features often excluded from problem descriptions include the proportion of the organisation’s business that is represented by HHC, or specifically whether HHC is organised independently from its other services. This is relevant when considering the value of a whole supply-chain approach because, if strategic decisions are made for a wider set of services, then good strategy may not necessarily be conducive to good operational performance in HHC services.
While the omission of these features of organisational context does not necessarily undermine the potential value of the work done for the organisations studied, it can be argued that it makes the models less generalisable (Sahin & Matta, Citation2015), or rather it makes it harder to understand what configurations of HHC service and in what societal settings a model could be applied or adapted.
Based on this review, we make a number of recommendations for future research. We consider that work addressing problems of role definition, home health care plan construction and contract design for commissioning would be valuable additions to the literature, as would models to support the coordination and integration of different home based health and care services. In conducting and reporting such work, we suggest that it would be beneficial for authors to align, where possible, the aspects of system performance used in objectives and constraints with those used in existing literature. This would enhance the prospects of decision makers identifying a suite of OR models that address decisions at different planning levels but that promote consistent goals. Also, as discussed above, we consider that it would be useful for authors to clarify the context of the home health care organisations that they work with such that the applicability of models to different societal settings can be more readily assessed.
Supplemental Material
Download Zip (56.7 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 Given the elapsed time between running our literature search and publication of this article, we re-ran our search during the peer-review process (on the 20th January 2020) and obtained 63 additional articles, of which 34 were retained based on title/abstract. Based on information gathered from the abstracts and full-text, we found that all of the identified papers reported formulations and/or algorithms for some combination of allocation, scheduling and routing problems, except one paper presenting a formulation and an algorithm for the districting problem. We did not identify any relevant discrepancies between such additional results and the findings reported in this review.
References
- Akao, Y. (2004). Quality function deployment: Integrating customer requirments into product design. Productivity Press.
- Akjiratikarl, C., Yenradee, P., & Drake, P. R. (2007). PSO-based algorithm for home care worker scheduling in the UK. Computers & Industrial Engineering, 53(4), 559–583. doi:https://doi.org/10.1016/j.cie.2007.06.002
- An, Y.-J., Kim, Y.-D., Jeong, B. J., & Kim, S.-D. (2012). Scheduling healthcare services in a home healthcare system. Journal of the Operational Research Society, 63(11), 1589–1599. https://doi.org/10.1057/jors.2011.153
- Argiento, R., Guglielmi, A., Lanzarone, E., & Nawajah, I. (2016). A Bayesian framework for describing and predicting the stochastic demand of home care patients. Flexible Services and Manufacturing Journal, 28(1-2), 254–279. https://doi.org/10.1007/s10696-014-9200-4
- Bachouch, R. B., Guinet, A., & Hajri-Gabouj, S. (2011). A decision-making tool for home health care nurses’ planning. Supply Chain Forum: An International Journal, 12(1), 14–20. https://doi.org/10.1080/16258312.2011.11517250
- Bard, J. F., Shao, Y., & Jarrah, A. I. (2014). A sequential GRASP for the therapist routing and scheduling problem. Journal of Scheduling, 17(2), 109–133. https://doi.org/10.1007/s10951-013-0345-x
- Bard, J. F., Shao, Y., Qi, X., & Jarrah, A. I. (2014). The traveling therapist scheduling problem. IIE Transactions, 46(7), 683–706. https://doi.org/10.1080/0740817X.2013.851434
- Bard, J. F., Shao, Y., & Wang, H. (2013). Weekly scheduling models for traveling therapists. Socio-Economic Planning Sciences, 47(3), 191–204. https://doi.org/10.1016/j.seps.2012.07.001
- Barua, A., Ravindran, S., & Whinston, A. B. (1997). Coordination in information exchange between organizational decision units. IEEE Transactions on Systems, Man, and Cybernetics - Part A: Systems and Humans, 27(5), 690–698. https://doi.org/10.1109/3468.618268
- Begur, S. V., Miller, D. M., & Weaver, J. R. (1997). An integrated spatial DSS for scheduling and routing home-health-care nurses. Interfaces, 27(4), 35–48. https://doi.org/10.1287/inte.27.4.35
- Bennett, A. R., & Erera, A. L. (2011). Dynamic periodic fixed appointment scheduling for home health. IIE Transactions on Healthcare Systems Engineering, 1(1), 6–19. https://doi.org/10.1080/19488300.2010.549818
- Benzarti, E., Sahin, E., & Dallery, Y. (2013). Operations management applied to home care services: Analysis of the districting problem. Decision Support Systems, 55(2), 587–598. https://doi.org/10.1016/j.dss.2012.10.015
- Bertels, S., & Fahle, T. (2006). A hybrid setup for a hybrid scenario: Combining heuristics for the home health care problem. Computers & Operations Research, 33(10), 2866–2890. https://doi.org/10.1016/j.cor.2005.01.015
- Blais, M., Lapierre, S. D., & Laporte, G. (2003). Solving a home-care districting problem in an urban setting. Journal of the Operational Research Society, 54(11), 1141–1147. https://doi.org/10.1057/palgrave.jors.2601625
- Boucher, X., Bonjour, E., & Grabot, B. (2007). Formalisation and use of competencies for industrial performance optimisation: A survey. Computers in Industry, 58(2), 98–117. https://doi.org/10.1016/j.compind.2006.09.004
- Bowers, J., Cheyne, H., Mould, G., & Page, M. (2015). Continuity of care in community midwifery. Health Care Management Science, 18(2), 195–204. https://doi.org/10.1007/s10729-014-9285-z
- Braekers, K., Hartl, R. F., Parragh, S. N., & Tricoire, F. (2016). A bi-objective home care scheduling problem: Analyzing the trade-off between costs and client inconvenience. European Journal of Operational Research, 248(2), 428–443. https://doi.org/10.1016/j.ejor.2015.07.028
- Burgess, J. F. (2012). Innovation and efficiency in health care: Does anyone really know what they mean? Health Systems, 1(1), 7–12. https://doi.org/10.1057/hs.2012.6
- Büyüktahtakın, I. E., & Haight, R. G. (2018). A review of operations research models in invasive species management: State of the art, challenges, and future directions. Annals of Operations Research, 271(2), 357–403. https://doi.org/10.1007/s10479-017-2670-5
- Cappanera, P., & Scutellà, M. G. (2015). Joint assignment, scheduling, and routing models to home care optimization: A pattern-based approach. Transportation Science, 49(4), 830–852. https://doi.org/10.1287/trsc.2014.0548
- Cappanera, P., Scutellà, M. G., Nervi, F., & Galli, L. (2018). Demand uncertainty in robust Home Care optimization. Omega, 80, 95–110. https://doi.org/10.1016/j.omega.2017.08.012
- Carello, G., & Lanzarone, E. (2014). A cardinality-constrained robust model for the assignment problem in home care services. European Journal of Operational Research, 236(2), 748–762. https://doi.org/10.1016/j.ejor.2014.01.009
- Carello, G., Lanzarone, E., & Mattia, S. (2018). Trade-off between stakeholders’ goals in the home care nurse-to-patient assignment problem. Operations Research for Health Care, 16, 29–40. https://doi.org/10.1016/j.orhc.2017.12.002
- Cattafi, M., Herrero, R., Gavanelli, M., Nonato, M., & Malucelli, F. (2015). An application of constraint solving for home health care. AI Communications, 28(2), 215–237. https://doi.org/10.3233/AIC-140632
- Chen, S.-J., & Lin, L. (2004). Modeling team member characteristics for the formation of a multifunctional team in concurrent engineering. IEEE Transactions on Engineering Management, 51(2), 111–124. https://doi.org/10.1109/TEM.2004.826011
- Chrysopoulos, A., & Mitkas, P. A. (2018). Customized time-of-use pricing for small-scale consumers using multi-objective particle swarm optimization. Advances in Building Energy Research, 12(1), 25–47. https://doi.org/10.1080/17512549.2017.1325397
- Cissé, M., Yalçındağ, S., Kergosien, Y., Şahin, E., Lenté, C., & Matta, A. (2017). OR problems related to home health care: A review of relevant routing and scheduling problems. Operations Research for Health Care, 13-14, 1–22. https://doi.org/10.1016/j.orhc.2017.06.001
- De Angelis, V. (1998). Planning home assistance for AIDS patients in the City of Rome. Interfaces, 28(3), 75–83. https://doi.org/10.1287/inte.28.3.75
- Decerle, J., Grunder, O., El Hassani, A. H., & Barakat, O. (2016). A two-phases matheuristic for the home care routing and scheduling problem. IFAC-PapersOnLine, 49(12), 1484–1489. https://doi.org/10.1016/j.ifacol.2016.07.781
- Decerle, J., Grunder, O., El Hassani, A. H., & Barakat, O. (2018). A memetic algorithm for a home health care routing and scheduling problem. Operations Research for Health Care, 16, 59–71. https://doi.org/10.1016/j.orhc.2018.01.004
- deLlano-Paz, F., Calvo-Silvosa, A., Antelo, S. I., & Soares, I. (2017). Energy planning and modern portfolio theory: A review. Renewable and Sustainable Energy Reviews, 77, 636–651. https://doi.org/10.1016/j.rser.2017.04.045
- Du, G., Liang, X., & Sun, C. (2017). Scheduling optimization of home health care service considering patients’ priorities and time windows. Sustainability, 9(2), 253. https://doi.org/10.3390/su9020253
- Durugbo, C., Tiwari, A., & Alcock, J. R. (2013). Modelling information flow for organisations: A review of approaches and future challenges. International Journal of Information Management, 33(3), 597–610. https://doi.org/10.1016/j.ijinfomgt.2013.01.009
- En-Nahli, L., Allaoui, H., & Nouaouri, I. (2015). A multi-objective modelling to human resource assignment and routing problem for home health care services. IFAC-PapersOnLine, 48(3), 698–703. https://doi.org/10.1016/j.ifacol.2015.06.164
- Erdem, M., & Bulkan, S. (2017). A two-stage solution approach for the large-scale home healthcare routeing and scheduling problem. South African Journal of Industrial Engineering, 28(4), 133–149. https://doi.org/10.7166/28-4-1754
- Errarhout, A., Kharraja, S., & Corbier, C. (2016). Two-stage stochastic assignment problem in the home health care. IFAC-PapersOnLine, 49(12), 1152–1157. https://doi.org/10.1016/j.ifacol.2016.07.659
- Eveborn, P., Flisberg, P., & Rönnqvist, M. (2006). Laps care—an operational system for staff planning of home care. European Journal of Operational Research, 171(3), 962–976. https://doi.org/10.1016/j.ejor.2005.01.011
- Eveborn, P., Rönnqvist, M., Einarsdóttir, H., Eklund, M., Lidén, K., & Almroth, M. (2009). Operations research improves quality and efficiency in home care. Interfaces, 39(1), 18–34. https://doi.org/10.1287/inte.1080.0411
- Fikar, C., & Hirsch, P. (2015). A matheuristic for routing real-world home service transport systems facilitating walking. Journal of Cleaner Production, 105, 300–310. https://doi.org/10.1016/j.jclepro.2014.07.013
- Fikar, C., & Hirsch, P. (2017). Home health care routing and scheduling: A review. Computers & Operations Research, 77, 86–95. https://doi.org/10.1016/j.cor.2016.07.019
- Fikar, C., Juan, A. A., Martinez, E., & Hirsch, P. (2016). A discrete-event driven metaheuristic for dynamic home service routing with synchronised trip sharing. European J. of Industrial Engineering, 10(3), 323. https://doi.org/10.1504/EJIE.2016.076382
- Green, L. V., Soares, J., Giglio, J. F., & Green, R. A. (2006). Using queueing theory to increase the effectiveness of emergency department provider staffing. Academic Emergency Medicine, 13(1), 61–68. https://doi.org/10.1197/j.aem.2005.07.034
- Guericke, D., & Suhl, L. (2017). The home health care problem with working regulations. Or Spectrum, 39(4), 977–1010. https://doi.org/10.1007/s00291-017-0481-3
- Gutiérrez, E. V., & Vidal, C. J. (2013). Home health care logistics management problems: A critical review of models and methods. Revista Facultad de Ingeniería Universidad de Antioquia, 68, 160–175.
- Hertz, A., & Lahrichi, N. (2009). A patient assignment algorithm for home care services. Journal of the Operational Research Society, 60(4), 481–495. https://doi.org/10.1057/palgrave.jors.2602574
- Hewitt, M., Nowak, M., & Nataraj, N. (2016). Planning strategies for home health care delivery. Asia-Pacific Journal of Operational Research, 33(05), 1650041. https://doi.org/10.1142/S021759591650041X
- Hiermann, G., Prandtstetter, M., Rendl, A., Puchinger, J., & Raidl, G. R. (2015). Metaheuristics for solving a multimodal home-healthcare scheduling problem. Central European Journal of Operations Research, 23(1), 89–113. https://doi.org/10.1007/s10100-013-0305-8
- Hindle, T., Hindle, A., & Spollen, M. (2000). Resource allocation modelling for home-based health and social care services in areas having differential population density levels: A case study in Northern Ireland. Health Services Management Research, 13(3), 164–169. https://doi.org/10.1177/095148480001300304
- Hindle, T., Hindle, G., & Spollen, M. (2009). Travel-related costs of population dispersion in the provision of domiciliary care to the elderly: A case study in English Local Authorities. Health Services Management Research, 22(1), 27–32. https://doi.org/10.1258/hsmr.2008.008012
- Hulshof, P. J. H., Kortbeek, N., Boucherie, R. J., Hans, E. W., & Bakker, P. J. M. (2012). Taxonomic classification of planning decisions in health care: A structured review of the state of the art in OR/MS. Health Systems, 1(2), 129–175. https://doi.org/10.1057/hs.2012.18
- Ingolfsson, A., Campello, F., Wu, X., & Cabral, E. (2010). Combining integer programming and the randomization method to schedule employees. European Journal of Operational Research, 202(1), 153–163. https://doi.org/10.1016/j.ejor.2009.04.026
- Koeleman, P. M., Bhulai, S., & van Meersbergen, M. (2012). Optimal patient and personnel scheduling policies for care-at-home service facilities. European Journal of Operational Research, 219(3), 557–563. https://doi.org/10.1016/j.ejor.2011.10.046
- Lanzarone, E., & Matta, A. (2012). A cost assignment policy for home care patients. Flexible Services and Manufacturing Journal, 24(4), 465–495. https://doi.org/10.1007/s10696-011-9121-4
- Lanzarone, E., Matta, A., & Sahin, E. (2012). Operations management applied to home care services: The problem of assigning human resources to patients. IEEE Transactions on Systems, Man, and Cybernetics - Part A: Systems and Humans, 42(6), 1346–1363. https://doi.org/10.1109/TSMCA.2012.2210207
- Lanzarone, E., Matta, A., & Scaccabarozzi, G. (2010). A patient stochastic model to support human resource planning in home care. Production Planning & Control, 21(1), 3–25. https://doi.org/10.1080/09537280903232362
- Lin, C.-C., Hung, L.-P., Liu, W.-Y., & Tsai, M.-C. (2018). Jointly rostering, routing, and rerostering for home health care services: A harmony search approach with genetic, saturation, inheritance, and immigrant schemes. Computers & Industrial Engineering, 115, 151–166. https://doi.org/10.1016/j.cie.2017.11.004
- Lin, M., Chin, K. S., Wang, X., & Tsui, K. L. (2016). The therapist assignment problem in home healthcare structures. Expert Systems with Applications, 62, 44–62. https://doi.org/10.1016/j.eswa.2016.06.010
- Lin, M., Chin, K.-S., Fu, C., & Tsui, K.-L. (2017). An effective greedy method for the meals-on-wheels service districting problem. Computers & Industrial Engineering, 106, 1–19. https://doi.org/10.1016/j.cie.2017.01.022
- Liu, M., Yang, D., Su, Q., & Xu, L. (2018). Bi-objective approaches for home healthcare medical team planning and scheduling problem. Computational and Applied Mathematics, 37(4), 4443–4474. https://doi.org/10.1007/s40314-018-0584-8
- Liu, R., Xie, X., Augusto, V., & Rodriguez, C. (2013). Heuristic algorithms for a vehicle routing problem with simultaneous delivery and pickup and time windows in home health care. European Journal of Operational Research, 230(3), 475–486. https://doi.org/10.1016/j.ejor.2013.04.044
- Liu, R., Xie, X., & Garaix, T. (2014). Hybridization of tabu search with feasible and infeasible local searches for periodic home health care logistics. Omega, 47, 17–32. https://doi.org/10.1016/j.omega.2014.03.003
- Liu, R., Yuan, B., & Jiang, Z. (2017). Mathematical model and exact algorithm for the home care worker scheduling and routing problem with lunch break requirements. International Journal of Production Research, 55(2), 558–575. https://doi.org/10.1080/00207543.2016.1213917
- López-Santana, E. R., Espejo-Díaz, J. A., & Méndez-Giraldo, G. A. (2016). Multi-agent approach for solving the dynamic home health care routing problem. In J. C. Figueroa-García, E. R. López-Santana, & R. Ferro-Escobar (Eds.), Applied computer sciences in engineering. (Vol. 657, pp. 188–200). Cham: Springer. https://doi.org/10.1007/978-3-319-50880-1_17
- Manerba, D., & Mansini, R. (2016). The nurse routing problem with workload constraints and incompatible services. IFAC-PapersOnLine, 49(12), 1192–1197. https://doi.org/10.1016/j.ifacol.2016.07.670
- Mankowska, D. S., Meisel, F., & Bierwirth, C. (2014). The home health care routing and scheduling problem with interdependent services. Health Care Management Science, 17(1), 15–30. https://doi.org/10.1007/s10729-013-9243-1
- Marcon, E., Chaabane, S., Sallez, Y., Bonte, T., & Trentesaux, D. (2017). A multi-agent system based on reactive decision rules for solving the caregiver routing problem in home health care. Simulation Modelling Practice and Theory, 74, 134–151. https://doi.org/10.1016/j.simpat.2017.03.006
- Masmoudi, M., & Abdelaziz, F. B. (2018). Portfolio selection problem: A review of deterministic and stochastic multiple objective programming models. Annals of Operations Research, 267(1-2), 335–352. https://doi.org/10.1007/s10479-017-2466-7
- Maya Duque, P. A., Castro, M., Sörensen, K., & Goos, P. (2015). Home care service planning. The case of Landelijke Thuiszorg. European Journal of Operational Research, 243(1), 292–301. https://doi.org/10.1016/j.ejor.2014.11.008
- Monitor. (2015). Moving healthcare closer to home. https://www.gov.uk/guidance/moving-healthcare-closer-to-home
- Mutingi, M., Mbohwa, C. (2013). Home healthcare worker scheduling: A group genetic algorithm approach [Poster presentation]. Proceedings of the World Congress on Engineering 2013, I, 721–725. http://www.iaeng.org/publication/WCE2013/WCE2013_pp721-725.pdf
- Mutingi, M., & Mbohwa, C. (2014). A fuzzy-based particle swarm optimisation approach for task assignment in home healthcare. South African Journal of Industrial Engineering, 25(3), 84–95. https://doi.org/10.7166/25-3-777
- Nasir, J. A., & Dang, C. (2016). Identifying quantitative thresholds for the home health care problem [Paper presentation]. 2016 IEEE Symposium on Computers and Communication (ISCC), 220–225. https://doi.org/10.1109/ISCC.2016.7543743
- Nasir, J. A., & Dang, C. (2018). Solving a more flexible home health care scheduling and routing problem with joint patient and nursing staff selection. Sustainability, 10(2), 148. https://doi.org/10.3390/su10010148
- Nasir, J. A., Hussain, S., & Dang, C. (2018). An integrated planning approach towards home health care, telehealth and patients group based care. Journal of Network and Computer Applications, 117, 30–41. https://doi.org/10.1016/j.jnca.2018.05.009
- NHS England. (2014). The NHS five year forward view. https://www.england.nhs.uk/publication/nhs-five-year-forward-view/
- Nickel, S., Schröder, M., & Steeg, J. (2012). Mid-term and short-term planning support for home health care services. European Journal of Operational Research, 219(3), 574–587. https://doi.org/10.1016/j.ejor.2011.10.042
- Palmer, R., Fulop, N. J., & Utley, M. (2018). A systematic literature review of operational research methods for modelling patient flow and outcomes within community healthcare and other settings. Health Systems, 7(1), 29–50. https://doi.org/10.1057/s41306-017-0024-9
- Quintana, D., Cervantes, A., Saez, Y., & Isasi, P. (2017). Clustering technique for large-scale home care crew scheduling problems. Applied Intelligence, 47(2), 443–455. https://doi.org/10.1007/s10489-017-0908-1
- Rasmussen, M. S., Justesen, T., Dohn, A., & Larsen, J. (2012). The home care crew scheduling problem: Preference-based visit clustering and temporal dependencies. European Journal of Operational Research, 219(3), 598–610. https://doi.org/10.1016/j.ejor.2011.10.048
- Redjem, R., & Marcon, E. (2016). Operations management in the home care services: A heuristic for the caregivers’ routing problem. Flexible Services and Manufacturing Journal, 28(1-2), 280–303. https://doi.org/10.1007/s10696-015-9220-8
- Rest, K.-D., & Hirsch, P. (2015). Supporting urban home health care in daily business and times of disasters. IFAC-PapersOnLine, 48(3), 686–691. https://doi.org/10.1016/j.ifacol.2015.06.162
- Rest, K.-D., & Hirsch, P. (2016). Daily scheduling of home health care services using time-dependent public transport. Flexible Services and Manufacturing Journal, 28(3), 495–525. https://doi.org/10.1007/s10696-015-9227-1
- Rodriguez, C., Garaix, T., Xie, X., & Augusto, V. (2015). Staff dimensioning in homecare services with uncertain demands. International Journal of Production Research, 53(24), 7396–7410. https://doi.org/10.1080/00207543.2015.1081427
- Sahin, E., & Matta, A. (2015). A contribution to operations management-related issues and models for home care structures. International Journal of Logistics Research and Applications, 18(4), 355–385. https://doi.org/10.1080/13675567.2014.946560
- Shao, Y., Bard, J. F., & Jarrah, A. I. (2012). The therapist routing and scheduling problem. IIE Transactions, 44(10), 868–893. https://doi.org/10.1080/0740817X.2012.665202
- Shi, Y., Boudouh, T., & Grunder, O. (2017a). A hybrid genetic algorithm for a home health care routing problem with time window and fuzzy demand. Expert Systems with Applications, 72, 160–176. https://doi.org/10.1016/j.eswa.2016.12.013
- Shi, Y., Boudouh, T., & Grunder, O. (2017b). A home health care routing problem with stochastic travel and service time. IFAC-PapersOnLine, 50(1), 13987–13992. https://doi.org/10.1016/j.ifacol.2017.08.2419
- Shi, Y., Boudouh, T., Grunder, O., & Wang, D. (2018). Modeling and solving simultaneous delivery and pick-up problem with stochastic travel and service times in home health care. Expert Systems with Applications, 102, 218–233. https://doi.org/10.1016/j.eswa.2018.02.025
- Sommerville, J., & Dalziel, S. (1998). Project teambuilding—the applicability of Belbin’s team-role self-perception inventory. International Journal of Project Management, 16(3), 165–171. https://doi.org/10.1016/S0263-7863(97)00054-9
- Trautsamwieser, A., Gronalt, M., & Hirsch, P. (2011). Securing home health care in times of natural disasters. Or Spectrum, 33(3), 787–813. https://doi.org/10.1007/s00291-011-0253-4
- Trautsamwieser, A., & Hirsch, P. (2011). Optimization of daily scheduling for home healthcare services. Journal of Applied Operational Research, 3(3), 124–136.
- Trautsamwieser, A., & Hirsch, P. (2014). A branch-price-and-cut approach for solving the medium-term home health care planning problem. Networks, 64(3), 143–159. https://doi.org/10.1002/net.21566
- Wirnitzer, J., Heckmann, I., Meyer, A., & Nickel, S. (2016). Patient-based nurse rostering in home care. Operations Research for Health Care, 8, 91–102. https://doi.org/10.1016/j.orhc.2015.08.005
- Yalçındağ, S., Cappanera, P., Grazia Scutellà, M., Şahin, E., & Matta, A. (2016). Pattern-based decompositions for human resource planning in home health care services. Computers & Operations Research, 73, 12–26. https://doi.org/10.1016/j.cor.2016.02.011
- Yan, H.-B., Cai, S., & Li, M. (2016). A two-stage fuzzy quality function deployment model for service design. In V.-N. Huynh, M. Inuiguchi, B. Le, B. N. Le, & T. Denoeux (Eds.), Integrated uncertainty in knowledge modelling and decision making. (Vol. 9978, pp. 110–123). Cham: Springer. https://doi.org/10.1007/978-3-319-49046-5_10
- Yuan, B., & Jiang, Z. (2017). Disruption management for the real-time home caregiver scheduling and routing problem. Sustainability, 9(12), 2178. https://doi.org/10.3390/su9122178.
- Yuan, B., Liu, R., & Jiang, Z. (2015). A branch-and-price algorithm for the home health care scheduling and routing problem with stochastic service times and skill requirements. International Journal of Production Research, 53(24), 7450–7464. https://doi.org/10.1080/00207543.2015.1082041
- Yuan, B., Liu, R., & Jiang, Z. (2018). Daily scheduling of caregivers with stochastic times. International Journal of Production Research, 56(9), 3245–3261. https://doi.org/10.1080/00207543.2018.1445879
- Zhang, R., Fry, M. J., & Krishnan, H. (2015). Efficiency and Equity in Healthcare: An Analysis of Resource Allocation Decisions in a Long-Term Home Care Setting. INFOR: Information Systems and Operational Research, 53(3), 97–112. https://doi.org/10.3138/infor.53.3.97
- Zhang, S., Xu, J., Gou, H., & Tan, J. (2017). A research review on the key technologies of intelligent design for customized products. Engineering, 3(5), 631–640. https://doi.org/10.1016/J.ENG.2017.04.005