
ABSTRACT
Uncertain language can be used to express genuine uncertainty but can also be used to manage face (e.g., by softening bad news). These conflicting motivations can create ambiguity in health communication. In this preregistered two-part experiment, participants assumed the position of a health specialist and wrote a letter communicating either a certain or an uncertain medical diagnosis. This was addressed to either a patient (high face threat) or the patient’s family doctor (low face threat). Letters written under high face threat contained more words and more dispreferred markers (e.g., sorry, unfortunately) than those written under low face threat. The number of explicit hedges (e.g., possibly, maybe) did not differ as a function of face threat. Time taken to write the letters was elevated only in the condition where face threat was high and the diagnosis was uncertain, suggesting that the joint pressures of communicating uncertain information in a tactful way increased the task demands. Our data demonstrate that participants spontaneously produced dispreferred markers (but not explicit hedges) to manage face and that face management is more taxing under uncertainty. Ratings from a second set of participants indicate that face management strategies did not affect the perceived meaning or manner of the message. For open materials, data, and code, see https://doi.org/10.17605/OSF.IO/ZU2AN.
Introduction
Much of the information shared in social and professional discourse is uncertain. This uncertainty can be communicated in various ways, with the most direct method being to use explicit hedging terms such as possibly, probably, and likely. Hedging terms like these avoid full commitment to a proposition (Crompton, Citation1997). Consider, for example, a patient who is told by their doctor “you will possibly experience erectile dysfunction as a side effect of your new medication”; the term “possibly” in this example could be interpreted in several different ways. First, the patient may take a literal interpretation, assuming it has been used by the doctor as a genuine marker of uncertainty. However, they may adjust this interpretation if the doctor’s interpersonal motivations are considered. Because of the sensitive interpersonal context, the patient may interpret the doctor as being tactful or cautious, leading to other possible conclusions. It may be inferred, for example, that the doctor is deliberately understating the likelihood of the negative event to tactfully soften the bad news (e.g., saying possible when they believe the outcome is probable or even certain; Bonnefon & Villejoubert, Citation2006) or as a precaution against blame if the prognosis is wrong (Juanchich et al., Citation2012). One or both of these motivations (tact or caution) may lead the doctor to use language that diverges from their genuine level of certainty. For this reason, a patient may not interpret uncertainty terms (e.g., a hedge) at face value. The multiple possible motivations for using uncertainty terms means that they are a major source of ambiguity in linguistic communication (Holtgraves & Perdew, Citation2016).
The reason the patient may make these pragmatic inferences is due to the possibility that the doctor is engaging in face management (Goffman, Citation1967). A person’s “face” refers to their public self-esteem. People project a sense of positive identity that is always at stake during social interactions. This identity is sacred to the individual, and for this reason, people are motivated to manage and protect not just their own face but also to the face of others (Holtgraves, Citation2005). For example, communicating negative or critical information can threaten the face of the recipient, so speakers are motivated to communicate in a way that minimizes this threat. An awareness of this in the moment will cause a speaker to employ a number of linguistic strategies. These are acts of facework (Goffman, Citation1967).
One way a speaker can achieve an act of facework is to engage in politeness (Brown & Levinson, Citation1987). Those required to perform a face-threatening act (e.g., deliver bad news) can select from a variety of options to reduce the harm imposed on the recipient. For instance, a speaker could use “positive politeness” to attend to the recipient’s desire for social appreciation and bolster their self-esteem (e.g., “side effects are rarer in fit and healthy men like yourself”). Similarly, “negative politeness” strategies such as indirectness, hedging, or being apologetic can be used to redress (or “set right”) the recipient’s desire to remain autonomous and unimpeded. In effect, the speaker can minimize harm to face by softening the blow of bad news via the way they communicate (Brown & Levinson, Citation1987).
In our example above (informing a patient that they may have a negative side effect), there is a threat to the patient’s face because as a sexually active male, a diagnosis of erectile dysfunction threatens his public self-image. The use of a hedge (e.g., “possibly”) could be used as a negative face management strategy to manage the face of both speaker and hearer. The patient’s face is spared because the doctor avoids bluntness (rather than being told “this medication will give you erectile dysfunction”). Additionally, the doctor manages their own face by accounting for every eventuality (i.e., if erectile dysfunction doesn’t occur, they have not misinformed the patient).
Uncertainty terms such as “possibly” or “maybe” are inherently ambiguous, as they have no solid referent (Holtgraves, Citation2014). Their meaning must be inferred by considering the multiple possible motivations of the speaker (i.e., are they genuinely uncertain or are they engaging in face management?). Disentangling these motivations is taxing on mental resources, as the hearer attempts to read between the lines (Bonnefon et al., Citation2011).
Most research on uncertain language conducted to date has focused on how uncertainty terms are comprehended in different contexts. One contextual factor that has been shown to affect the comprehension of uncertainty terms is the degree of situational face threat. For example, informing a patient that they will “possibly suffer deafness soon” is more threatening than informing them that they will “possibly suffer insomnia soon,” as the consequences of the former are more severe. When the severity of the communicated information (and thus the face threat to the hearer) changes, so does the interpretation of the hedging term “possibly.” Bonnefon and Villejoubert (Citation2006) found that more severe outcomes were perceived to be more probable. In other words, the likelihood of possibly developing deafness was perceived as higher than the likelihood of possibly developing insomnia (all else being equal). This indicates that recipients of uncertain information adjust their interpretations when they infer that the speaker is motivated by face management.
Several studies have shown that the comprehension of uncertain language is affected by the presumed motivations of the speaker (Bhise et al., Citation2018; Bonnefon et al., Citation2009; Holtgraves, Citation2014; Lee & Pinker, Citation2010; Pinker et al., Citation2008; Stewart et al., Citation2018). In contrast, there has been less focus on the production of uncertain language by speakers or writers (Holtgraves & Perdew, Citation2016). In line with politeness theory, the studies that have been conducted demonstrate that when information is face-threatening, the speaker (or writer) will adjust the wording of their message to manage the recipient’s face (e.g., Burgers et al., Citation2012; Holtgraves & Perdew, Citation2016; Holtgraves & Yang, Citation1992; Juanchich & Sirota, Citation2013; Lee, Citation1993; Sirota & Juanchich, Citation2015). For example, this may be a speaker who is certain choosing uncertain language (e.g., uttering “your drinking may be a problem” rather than “your drinking is a problem”) or an uncertain speaker understating their degree of certainty (e.g., uttering “perhaps you drink too much” rather than “you probably drink too much”).
Of the studies looking into uncertain language production under face threat, most have presented participants with a hypothetical scenario and asked them to choose, from a list, the probability term they would use to communicate an uncertain outcome. For example, Juanchich and Sirota (Citation2013) asked participants which of eight verbal probability terms (e.g., “slightly probable,” “evenly probable,” “rather probable”) they would use to communicate to an investor the likelihood of their investments losing value. Participants were instructed to be informative or to engage in face management (e.g., avoid blame or soften the bad news). This motivational manipulation influenced the probability terms chosen. When participants were motivated to engage in face management (e.g., to avoid blame or upset), they selected significantly less certain probability terms than when they were instructed to be informative. This suggests that when instructed to purposefully engage in face management, people may understate the certainty of a negative event.
A limitation of the research conducted by Juanchich and Sirota (Citation2013) is that participants were explicitly instructed to engage in face management, so it does not tell us whether people spontaneously choose their words to save face. In a later study, Sirota and Juanchich (Citation2015) again asked participants to select the probability term they would use to communicate negative information, but this time without the instruction to manage face. Participants were then retrospectively asked to indicate the motivation for their choice. In this study 41.6% of participants indicated face management as a reason for their choice (by indicating that tact or caution was their motivation). The participants who selected face management concerns as a motive selected more uncertain probability terms than those who indicated their motivation was simply to be informative. This indicates that at least some people do spontaneously engage in face management and that one method of achieving this is to understate the certainty (probability) of negative events.
While previous studies typically asked participants to select from a list of specific probability terms, Holtgraves and Perdew (Citation2016; Experiment 2) used a more naturalistic open-ended approach in which participants were asked to communicate a face-threatening opinion in their own words. This allowed them to measure the spontaneous production of uncertainty terms and to identify other face management strategies. Importantly, their method also allowed them to look at the communicative dyad (i.e., the speaker and hearer together). The first part of their study focused on the type of language participants produced when communicating in a face-threatening context, while the second part examined how these messages were comprehended by a second set of participants.
In the first part of their study, Holtgraves and Perdew (Citation2016; Experiment 2) used hypothetical scenarios to examine how participants communicated opinions that were potentially face-threatening to a fictional recipient. For example, one of the scenarios required participants to explain that the reason a friend was failing at university was (possibly) due to their excessive drinking and partying. Within the scenarios, they manipulated the degree of face threat. This was achieved by keeping the scenario constant while changing the referent. In practical terms, the high face threat condition involved breaking a negative opinion directly to the friend. In contrast, the low face threat (control) condition involved communicating this negative opinion to a third party while the friend was not present. Second, the certainty of the opinion was manipulated. Participants were asked to imagine they were either 20%, 50%, or 80% certain of their opinion (e.g., 20/50/80% certain that excessive drinking is the reason their friend is failing).
While previous research conducted under restrictive forced-choice conditions has shown that people select less certain probability terms under face threat, Holtgraves and Perdew (Citation2016) sought to identify the specific types of uncertain language that people spontaneously produce under face threat. They planned to objectively examine the production of uncertain language by measuring the use of linguistic features such as probability terms (e.g., probably, possibly), hedges (e.g., could, might), and dispreferred markers that signal impending bad news (e.g., unfortunately …, I am afraid to say …, sadly …). It was predicted that when participants were communicating an utterance in the high face threat condition, they would produce more uncertain language. However, contrary to their expectations the use of these uncertainty terms was infrequent. The authors therefore chose to focus on linguistic indirectness as a substitute, which was measured using a five-point scale. The more a message deviated from a direct assertion (e.g., “you’re partying too much”), the more indirect it was judged to be. They found that language production was significantly more indirect in the face-threatening condition. A second set of participants then rated the probability (uncertainty) of the messages (e.g., the probability the friend is failing due to excessive drinking). The more indirect the message was, the more uncertain (lower probability) the messages were perceived to be.
The findings of Holtgraves and Perdew (Citation2016) reveal that face threat causes greater use of indirect language and that this indirect language is perceived as more uncertain (lower probability). However, one of the most surprising findings was the infrequent use of explicitly uncertain language by participants. This meant the authors were unable to reliably examine specific strategies for communicating uncertainty (e.g., the production of hedges and dispreferred markers). They reasoned that the lack of explicitly uncertain language was due to the informal interpersonal nature of their scenarios, which led participants to use indirectness as a more subtle, implicit method of communicating uncertainty. They contrasted their scenarios with more formal situations (e.g., a doctor communicating a diagnosis to a patient or a financial advisor communicating risk to a client) in which they reasoned that explicit methods of communicating uncertainty would be more likely. These formal situations are generally high stakes, where the use of tact and the avoidance of ambiguity are equally critical. In this study we build on the work of Holtgraves and Perdew (Citation2016) by asking participants to produce certain or uncertain messages under high or low face threat but in a much more formal manner. Specifically, participants were asked to put themselves in the position of a medical specialist and to communicate a certain diagnosis or an uncertain diagnosis to either a patient (high face threat) or to a patient’s family doctor (low face threat). We anticipated that asking participants to communicate a consequential negative outcome in a formal manner would encourage the use of explicit uncertainty terms to manage face threat. These formal, emotionally sensitive scenarios provide an ideal testbed for examining specifically how different types of uncertain language are used to manage face threat.
Present research
This preregistered two-part experiment aimed to extend the findings of Holtgraves and Perdew (Citation2016). Our intention was to create vignettes that encouraged greater use of uncertain language, allowing us to examine the various ways in which uncertain language can be used to manage face. To increase the strength of the face threat manipulation, we asked participants to communicate high stakes information in a formal manner to a potentially vulnerable recipient. We achieved this by using a formal context known to have a high degree of face threat: breaking bad medical news to patients (Baile et al., Citation2000; Bonnefon et al., Citation2011; Burgers et al., Citation2012; Rodriguez et al., Citation2007; Shaw et al., Citation2012; Sirota et al., Citation2018).
In Experiment 1a participants were asked to put themselves in the position of a health specialist (i.e., a specialist in a specific condition rather than a general practitioner) and to write a letter communicating diagnostic information. Face threat was manipulated by instructing participants to write a letter addressing the family doctor of a patient (low face threat condition) or the patient themselves (high face threat condition). Communicating with the patient is particularly face-threatening because the consequential negative outcome applies directly to them (Brown & Levinson, Citation1987). While the doctor’s greater power and status in this context could reduce the weight of this threat to some extent, the act of breaking bad news to a patient is generally acknowledged to be face-threatening for medical professionals (e.g., Aronsson & Sätterlund-Larsson, Citation1987). The vignettes were also manipulated so that the diagnosis was either certain or uncertain. This manipulation allowed us to investigate whether face management strategies differ as a function of (un)certainty.
In Experiment 1a we measured the number of hedging terms used, number of dispreferred markers used, time spent writing the letters, and total number of words used to complete the letters. In Experiment 1b, a second set of participants rated the letters that were written by participants in Experiment 1a. The letters were rated for subjective politeness, certainty, directness, and probability (i.e., probability that the patient has the diagnosed condition).
We predicted that the face threat manipulation would affect the number of hedges and dispreferred markers produced by participants who wrote letters in Experiment 1a and also the perception of these letters in Experiment 1b (see Appendix 1 for our detailed definitions of uncertainty terms and dispreferred markers, https://osf.io/p8rc2). Specifically, we predicted that participants would produce more hedges and more dispreferred markers when the letter was written in the high face threat condition than in the low face threat condition, as these are acts of negative politeness that can be used to manage face (Brown & Levinson, Citation1987). Existing production studies illustrate that hedging, in particular, may take many forms in the pursuit of negative politeness, such as the use of a modal (e.g., I feel I must inform you) to alleviate responsibility on the part of the speaker (see Markkanen & Schröder, Citation2010). We also expected that the production of these linguistic devices would result in a greater number of words being produced and a greater amount of time spent writing the letter. These expectations are based on a wealth of data suggesting that breaking bad news takes longer than delivering good news (Dibble & Levine, Citation2013). In Experiment 1b, we expected that letters written under high face threat (relative to low face threat) would be perceived as more polite, less certain, and less direct due to the use of negative politeness strategies.
We predicted that the certainty manipulation would affect the number of hedges and dispreferred markers produced by participants who wrote letters in Experiment 1a and the perception of these letters in Experiment 1b. Specifically, we predicted that participants would produce more hedges and more dispreferred markers when the diagnosis was uncertain. This is because hedges inherently communicate uncertainty (e.g., maybe, possibly, might), while dispreferred markers may indicate regret at the lack of certainty (e.g., I’m sorry I can’t be more certain). We also expected that the production of uncertain language would result in a greater number of words being produced and a greater amount of time spent writing the letter. In Experiment 1b, we expected that uncertain diagnoses would be perceived as more polite (because the uncertain language may be perceived as negative politeness), less certain, and less direct.
In addition to the predicted main effects of face threat and uncertainty, we also predicted that these factors would interact. In Experiment 1a, we predicted that uncertain diagnoses written under high face threat (see lower right cell in ) would result in the greatest number of hedges and dispreferred markers, the greatest number of words, and take the longest to write. In Experiment 1b, we predicted that letters written in this condition would be perceived to be the politest. These interaction effects were predicted as we expected the effects of high face threat and uncertainty to be cumulative (i.e., an uncertain diagnosis may include additional uncertain language when there is also the motivation to manage face).
Table 1. Four Experimental Conditions of Our 2 × 2 Independent Groups Design
Preregistration and data availability
This experiment was preregistered prior to data collection. The preregistration, materials, raw data and analysis scripts can be found on the Open Science Framework (OSF; Clelland & Haigh, Citation2023; osf.io/zu2an/). There are four known differences between our preregistration and the study reported here. These differences (and our reasoning for them) are discussed below and outlined in more detail on the OSF project page.
Experiment 1a Methods
Design
A 2 × 2 independent groups design was used in Experiment 1a. The first independent variable was face threat; participants addressed the letter to either the patient’s family doctor (low threat) or directly to the patient (high threat). The second independent variable was diagnosis certainty; the diagnosis to be communicated was either certain or uncertain. Participants were randomly assigned to one of four independent conditions ().
We measured the number of hedging terms produced by participants (e.g., maybe, might, possibly, potentially). We also measured the number of dispreferred markers (e.g., well, unfortunately, I am afraid, I regret), the amount of time taken to produce the letter, and the total number of words written.
Participants
A prospective power analysis was conducted using GPower 3.1. For 80% power to detect a medium-sized effect (f = 0.25) with an alpha level of .05, we would require a minimum of 128 participants, or 32 per condition (Faul et al., Citation2007). This was our minimum sample size target. The anticipated effect size used in the sample size calculation (f = 0.25) was comparable to effect sizes reported following similar manipulations. For example, Holtgraves and Perdew (Citation2016; Experiment 2, Part 1) examined the effect of face threat and probability on the production of indirect language (using very similar manipulations similar to ours). The effect size of their face threat manipulation was f = 0.32, and the effect size of their probability manipulation was f = 0.34.
Participants were recruited online via opportunity sampling. The study was advertised online through participation websites, social media, and university mailing lists. Undergraduate psychology students could claim course credit for completion. The study was open to those aged 18 or over and fluent in English. A total of 462 participants clicked the link taking them to the study information page. After excluding those who did not complete the study (n = 184), declared a nonserious response (n = 4), or identified themselves as having worked as a health professional (n = 40), a sample of 234 completed responses remained. Following manual inspection of the letters, a further 34 were excluded for the following reasons: the letter did not communicate a diagnosis as instructed (n = 18), the letter contained an incorrect addressee (e.g., letter was addressed to the patient when the task required a letter addressed to the patient’s doctor; n = 14), or the participant did not engage with the task (e.g., making a comment about the study rather than writing a letter; n = 2).
A document identifying these letters and their reasons for exclusion can be found on the OSF. The remaining 200 letters were written by English-speaking adults (140 women, 59 men, 1 selected “other”), aged between 18 and 63 (M age = 27.23, SD = 10.44). Gender makeup did not differ across conditions: χ2 (6, N=200) = 5.75, p = .45.
Materials
Six experimental vignettes were created. Each scenario asked the participant to imagine they were a consultant health professional (i.e., a specialist in a single medical condition). They were given information about a fictional patient, a list of recently reported symptoms, details of recently conducted tests, and the diagnosis to be communicated (which was either certain or uncertain). Participants were asked to communicate the diagnosis in a letter to either the patient’s family doctor or directly to the patient. An example scenario and key information can be found in . All six scenarios can be found on the OSF.
Figure 1. Example scenario. Superscripted digits correspond with variable patient information outlined in the subordinate table. Demographics of the fictional patients were counterbalanced across conditions.
As depicted in , six scenarios were created referring to various life-altering diseases. To aid in operationalizing the certainty of diagnoses, the chosen diseases have no definitive test and so require a level of professional opinion. There were four conditions, resulting in 24 vignettes. Each of our participants was randomly allocated to write a letter relating to 1 of these 24 vignettes. The vignettes were padded out with superficial information about the patient, both as a means of enhancing engagement and to disguise our manipulations. Superficial information was counterbalanced across scenarios to offset any potential assumptions or biases associated with such information (e.g., we counterbalanced characteristics such as patient gender, marital status and exercise levels across the six vignettes) ().
Table 2. Characteristics such as Patient Gender, Marital Status, and Exercise Levels Across the Six Vignettes
Manipulations
Certainty manipulation
To operationalize certainty within our vignettes, both an uncertain version and a certain version were created. For example, “Multiple sclerosis is known to be difficult to diagnose, so you are uncertain” (uncertain condition) or “Multiple sclerosis is known to be difficult to diagnose, but you are certain” (certain condition). Rather than manipulating the numeric certainty of the vignettes as in Holtgraves and Perdew (Citation2016; study 2), we operationalized our scenarios as either wholly certain or wholly uncertain. Our reasoning is as follows. First, patient diagnoses and prognoses can rarely be given exact probabilities on a case-by-case basis (Rodriguez et al., Citation2007). Moreover, there is limited evidence to suggest that people mentally represent probability at such a fine-grained level, as words do not always map neatly onto numeric expressions of uncertainty (Auger & Roy, Citation2008). We therefore manipulated the diagnosis to be either wholly certain or wholly uncertain with no numeric or verbal probability terms used.
Face threat manipulation
To operationalize face threat within our vignettes, both a high face threat version and a low face threat version were created, based on the manipulation used by Holtgraves and Perdew (Citation2016). In the high face threat version, participants were tasked with writing a letter addressed to the patient themselves. In the low face threat version, participants are tasked with writing a letter to the patient’s family doctor (known as a general practitioner in the United Kingdom). Delivering a medical diagnosis is more face-threatening when writing directly to the patient compared to the patient’s general practitioner as the diagnosis directly threatens the patient’s self-image. Doctors have described giving a serious diagnosis as “dropping a bomb” on the patient (Miyaji, Citation1993), and breaking bad news in a manner that saves face for the patient is particularly stressful on those who are unfamiliar with the process (Ptacek & Eberhardt, Citation1996). We therefore expected this manipulation to have a strong effect within our sample who were not health professionals.
Measures
Hedges and dispreferred markers
The preregistered plan was to automatically count hedges and dispreferred markers using word count software. However, it became apparent that this would not be possible to do in an automated fashion. The reason is that producing an exhaustive list of hedges and dispreferred markers to use as criteria for word count software is an unachievable task. Detection of hedges and dispreferred markers is largely context dependent, and these linguistic devices are often not isolated to a single word (e.g., I am afraid to say …). Crompton (Citation1997) outlines that hedging is best understood as a product of social forces, arguing that it cannot be limited to and labeled as a closed set of lexical terms. Moreover, Fraser (Citation2010) states that “an expression is usually only recognized as a hedge when it is used in hedging. Thus, it should not be surprising that there is no grammatical class of hedges, since hedging devices are drawn from every syntactic category” (p. 23). To ensure that linguistic features were considered in their context, we decided to code our letters with the help of independent coders who applied detailed coding criteria.
Our comprehensive instructions for identifying hedges and dispreferred markers were based on the criteria set out by Holtgraves and Perdew (Citation2016). The coding instructions can be found in Appendix 2 (see https://osf.io/5grxz/). These criteria were based on the working definitions of hedges and dispreferred markers described in Appendix 1.
Criteria for coding the letters was modified slightly from Holtgraves and Perdew (Citation2016). Initially, our intention was to measure hedges (e.g., may, might, could), dispreferred markers (e.g., well, unfortunately, I am afraid, sadly), and probability terms (e.g., likely, probably) separately. However, considering our working definition of hedges, we decided that probability terms should be categorized as a hedge. Our instructions defined a hedge as “an item of language which a speaker uses to explicitly qualify his/her lack of commitment to the truth of a proposition” (Crompton, Citation1997, p. 281). Within the context of breaking bad news to patients, probability terms neatly fit this definition, and they were therefore categorized as a hedge rather than measured as their own separate subset. Terms that allow the speaker to signal caution or probability rather than full certainty were categorized as hedges. Total number of hedges were summed for each letter.
Our instructions defined dispreferred markers as items of language that “reduce the face threat to the receiver by sending out a warning that a threat is forthcoming, or acknowledging in a conciliatory manner that a threat has occurred” (Hamilton et al., Citation2014, p. 199). Language was categorized as a dispreferred marker when a word or phrase signaled that some kind of bad news was coming or when language was intended to minimize harm. Total number of dispreferred markers were summed for each letter.
First, the instructions were given to an independent coder, who was blind to the hypotheses. These instructions were supplemented with a collaborative example coding exercise with the first author to ensure consistency and understanding. Initial coding was reviewed by the first author; after this, a meeting was held in which discrepancies between coder and first author were discussed. Discrepancies were resolved following discussion, with final judgment decisions made by the coder as the independent party. The coder identified a total of 683 hedges and 140 dispreferred markers. Following review by the first author, a further 195 hedges and 28 dispreferred markers were identified. Collaborative discussion of the review also resulted in the removal of 5 originally identified hedges and 1 originally identified dispreferred marker. A complete set of coded letters can be found on the OSF. To test the inter-rater reliability of our coding, we recruited a further coder to independently code the letters following the same instructions. Intraclass correlations revealed an excellent level of agreement in the identification of both hedges (intraclass correlation = .852) and dispreferred markers (intraclass correlation = .925; Hallgren, Citation2012).
Writing time
The vignette describing the patient and the text box in which participants wrote their letter appeared on the same web page (see for an example). Time spent writing the letter was measured by calculating the difference in seconds between the first mouse click on that page (when participants are presumed to have clicked on the free text box to begin writing) and the page submit time (when participants clicked to progress to the next page). This is an estimate of writing time as we cannot be sure that the first time a participant clicked their mouse was to activate the text entry box, although this is the most likely reason (i.e., there was no other reason to click). As such, the difference between first click and page submit was as a proxy for writing time. Because this measure has limitations, we also present exploratory analysis based on total time spent on the page (i.e., total time taken to read the vignette and write the letter, which makes no assumption about the onset of writing).
Number of words written
We summed the total number of words used to compose each letter. This was done using the base R function strsplit. A “word” was defined in our analysis as a string of characters followed by a space.
Procedure
This online study was conducted using Qualtrics (Snow & Mann, Citation2013). Participants first answered some basic demographic questions. Before being presented with a scenario, participants were shown a prompt screen asking them to ensure a period of uninterrupted attention. Participants were randomly assigned one scenario only out of a possible 24 (6 scenarios × 4 conditions). The number of participants allocated to each of the 24 scenarios ranged from 5 to 13. While completing the letter-writing task, participants were provided with standardized openings “Dear Mr/Mrs/Dr …” and conclusions “Yours Sincerely, The Specialist Practice.” Letters were restricted to a minimum character length of 50 characters, with no maximum. After writing the letter, participants were asked if they completed the task seriously (Aust et al., Citation2013), took a break or experienced any distractions during the task, about their status as a health professional, and about their experience of giving and receiving bad news. Mean completion time was 10 minutes, 16 seconds. A .qsf file for the Qualtrics survey can be accessed via the OSF.
Treatment of data
Some of the letters written by participants in Experiment 1a contained spelling or grammatical errors. Prior to analysis, some letters were manually edited. This process was necessary to aid the coding of uncertainty terms, improve accuracy of the word count in Experiment 1a, and also to aid the comprehension of the letters when presented to a separate set of participants in Experiment 1b. Reformatting was completed with the goal of making as few changes as reasonably possible. We corrected typos and misspellings and also improved the clarity of utterances that were not initially clear (see OSF for exact changes). For example, participant 232 wrote “I am writing to inform you of the condition of your male patient you referred to our clinic and undergone a brain scan” [sic]; this was corrected to “I am writing to inform you of the condition of your male patient, who you referred to our clinic having undergone a brain scan.” Details of manual cleaning and the exact changes made can be found on the OSF. No hedges or dispreferred markers were added or removed from the original letters during the editing. The mean letter word count prior to editing was 96.09 words. After editing the mean word count was and 95.73 words.
Results
A 2 × 2 (certainty × face threat) independent groups analysis of variance was conducted on each dependent variable (number of hedges contained in each letter, number of dispreferred markers, time spent writing, and number of words written).Footnote1 Cohen’s f is reported as a measure of effect size. All data analysis was conducted using R version 4.0.2 (R Core Team, Citation2020) and RStudio version 1.3.959 (RStudio Team, Citation2020). The raw data and analysis scripts for Experiment 1a are publicly available on the OSF.
Hedges and dispreferred markers
We measured the total number of hedges and dispreferred markers used in each letter (see Methods for details). No further exclusions from the final sample of 200 were made. The mean number of hedges and dispreferred markers in each condition is illustrated in .
Figure 2. Mean number of hedges and mean number of dispreferred markers per letter across four certainty × face threat conditions (high/certain, n = 49; low/certain, n = 44; high/uncertain, n = 53; low/uncertain, n = 54). Black horizontal lines represent condition means. Surrounding bands represent 95% confidence intervals. Black jittered dots represent raw data points, and beans represent smoothed density curves.
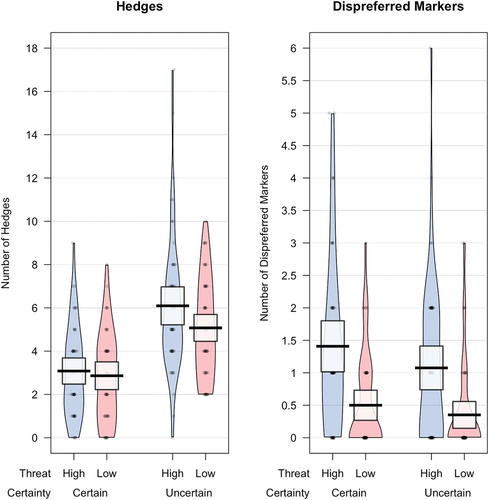
We found a significant and large main effect of certainty on the number of linguistic hedges produced per letter (F(1, 196) = 55.20, p < .001, f = 0.53). Participants who were asked to communicate an uncertain diagnosis (M = 5.58) produced significantly more hedges than those who communicated a certain diagnosis (M = 2.97). There was no significant main effect of face threat (F(1, 196) = 3.10, p = .080, f = 0.10). For this nonsignificant effect, the p value was only marginally above .05. Participants produced slightly more hedges under high face threat, but the effect size was small. There was no significant interaction between face threat and certainty (F(1, 196) = 1.30, p = .255, f = 0.07).
We found a significant and large main effect of face threat on the number of dispreferred markers produced per letter (F(1, 196) = 29.08, p < .001, f = 0.38). Participants asked to communicate a diagnosis directly to the patient (high face threat) produced significantly more dispreferred markers (M = 1.24) than those who communicated a diagnosis to the patient’s family doctor (low face threat; M = 0.43). There was no significant main effect of certainty (F(1, 196) = 2.53, p = .114, f = 0.11) and no significant interaction between face threat and certainty (F(1, 196) = 0.37, p = .543, f = 0.04).
Time spent writing (time from first click to page submit)
For writing time analyses, 14 participants who declared they were distracted during the task were excluded, leaving a sample of 186 responses. Visual inspection of the data identified some possible outliers. We therefore removed any values that were more than 2.5 SDs from the grand mean. This resulted in the removal of 3 additional responses, leaving a final sample of 183. Mean writing time in each condition is plotted in .
Figure 3. Mean number of seconds spent writing the letters (this proxy for writing time is the difference in seconds between first click and page submit) as a function of four certainty × face threat conditions (high/certain, n = 49; low/certain, n = 42; high/uncertain, n = 50; low/uncertain, n = 47). Black horizontal lines represent condition means. Surrounding bands represent 95% confidence intervals. Black jittered dots represent raw data points, and beans represent smoothed density curves.
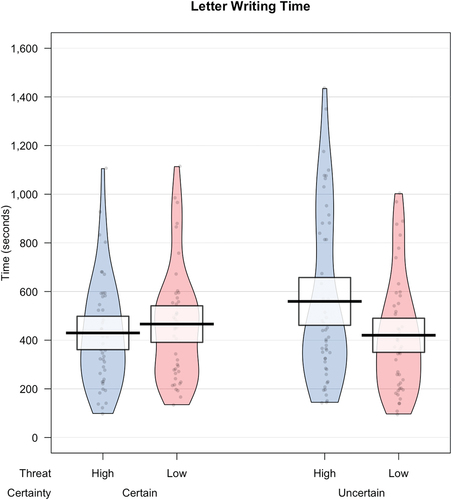
We found no significant main effect of face threat (F(1, 179) = 1.65, p = .201, f = 0.10) and no significant main effect of certainty (F(1, 179) = 1.09, p = .297, f = 0.08) on time taken to write the letter. However, we did find a significant interaction between face threat and certainty (F(1, 179) = 4.83, p = .029, f = 0.16). Bonferroni-corrected post-hoc comparisons (using alpha = .025) revealed that when communicating a diagnosis that was certain, there was no significant effect of face threat on writing time (t(82.97) = −0.72, p = .471). However, when communicating a diagnosis that was uncertain, there was a significant effect of face threat on writing time (t(87.41) = 2.32, p = .023). Those who communicated an uncertain diagnosis under high face threat took significantly longer to write their letter (M = 559.4) than those who communicated an uncertain diagnosis under low face threat (M = 420.2). The pattern of results described above did not differ when the analysis was rerun with outliers included.
Because our measure of writing time only serves as a proxy for writing time, we also conducted exploratory analysis on the “page submit” time (see above for details). This analysis does not make any assumptions about when participants started writing their letters. This analysis produced the same pattern of results as our writing time proxy measure, including a significant interaction between face threat and certainty. Details of this additional analysis can be found on the OSF.
Number of words written
Word count was calculated by totaling the number of words used to complete each letter. As in our writing time analysis, we excluded participants with word counts that were more than 2.5 SDs from the grand mean. Six participants were excluded on this criterion, leaving a final sample of 194. The mean number of words written is illustrated in .
Figure 4. Mean letter word count as a function of four certainty × face threat conditions (high/certain, n = 47; low/certain, n = 44; high/uncertain, n = 49; low/uncertain, n = 54). Black horizontal lines represent condition means. Surrounding bands represent 95% confidence intervals. Black jittered dots represent raw data points, and beans represent smoothed density curves.
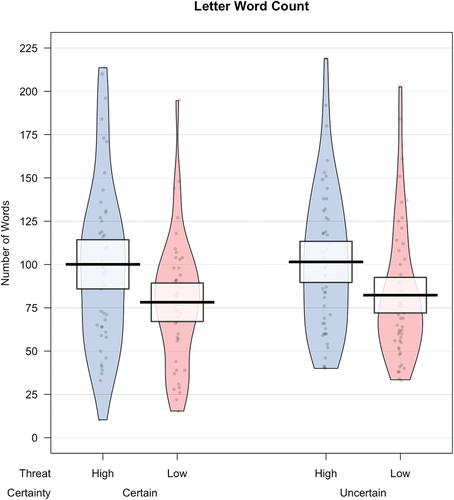
We found a significant main effect of face threat on the number of words used to produce the letter (F(1, 190) = 12.03, p < .001, f = 0.25). Participants who communicated a diagnosis directly to the patient (high face threat, M = 100.8 words) wrote longer letters than those who communicated a diagnosis to the patient’s family doctor (low face threat, M = 80.3 words). There was no significant main effect of certainty (F(1, 190) = 0.22, p = .644, f = 0.03) and no significant interaction between face threat and certainty (F(1, 190) = 0.05, p = .821, f = 0.02). The pattern of results described above did not differ when we reran the analysis with outliers included.
Discussion
As predicted, diagnosing a serious medical condition under high face threat caused participants to produce more dispreferred markers (e.g., I’m sorry, unfortunately, this must be tough for you) compared to diagnosing a serious condition under low face threat. In other words, when communicating threatening information directly to the patient in our scenarios rather than to the patient’s family doctor, participants produced more terms that signaled and acknowledged the sensitivity of the information being communicated.
Also in line with our predictions, higher face threat caused participants to produce more words when composing their letters than those who wrote under low face threat. When delivering threatening information directly to the patient, participants wrote letters that were longer. This likely reflects the elevated use of dispreferred markers when writing to the patient, which are motivated by face management concerns.
Contrary to our expectations, increasing face threat did not affect the number of hedges (e.g., possibly, likely, potentially) produced by participants. Descriptive statistics did indicate that slightly more hedges were produced under high face threat, but the effect size was small and marginally nonsignificant. The only factor to affect the production of hedges was the writer’s degree of certainty. This trivial finding indicates that less certain information was communicated using less certain language. Certainty also had no effect on the production of dispreferred markers or word count. Participants did not routinely use dispreferred markers to indicate regret about their uncertainty (e.g., I’m sorry I can’t be more certain).
Perhaps most interestingly, face threat moderated the effect of certainty on time taken to write the letters. Participants took longer to write their letter of diagnosis under high face threat only when the diagnosis was uncertain. Having to manage both sensitivity and uncertainty while communicating a threatening diagnosis meant that participants required more time to process and engineer their speech in such a way that attends to the sensitivity of the situation, but also accurately depicts their level of commitment to the information being exchanged. This suggests that joint pressures of genuinely communicating uncertain information in a tactful way increased the demands of the task. It is possible that the need to use uncertainty terms to communicate genuine uncertainty required speakers to think of alternative methods to manage face. This interaction effect was observed on our most sensitive measure (writing time) but not observed on our other measures (hedges, dispreferred markers, or word count), suggesting that the joint demands of managing face and communicating uncertainty affect processing time but not the language produced.
Experiment 1b
In Experiment 1b we sought to evaluate the communicative dyad in a way that builds on the findings of Holtgraves and Perdew (Citation2016). We wanted to understand how the language produced under varying levels of face threat would be interpreted from the receiver’s perspective. To measure this, we gave the letters that participants wrote in Experiment 1a, to a new set of participants who rated the letters on four interpretive measures.
First, we measured probability (e.g., “in your opinion, what is the probability that Mr Wilson has Alzheimer’s disease?”). Holtgraves and Perdew (Citation2016) found that probability ratings did not differ between messages produced under high face threat and those produced under low face threat (i.e., participants judged the likelihood of a negative opinion as the same irrespective of whether it was written in a socially threatening situation or not). However, Bonnefon and Villejoubert (Citation2006) reported evidence that hedging terms such as “possibly” were perceived to have higher probability in face threatening contexts. Because our face threat manipulation was more formal than that used by Holtgraves and Perdew (Citation2016) and the information to be communicated was more severe, we expected that the linguistic strategies used to manage face threat in Experiment 1a would be more detectable by participants in Experiment 1b, leading to higher probability estimates.
Second, letters were rated on certainty (i.e., “how certain is the specialist about their diagnosis?”). Because uncertainty terms can be used to manage face, we predicted that letters written under high face threat would be perceived as less certain.
Third, letters were rated on directness (i.e., “how direct is this diagnosis?”). This question was followed by our definition of directness (“direct language can be defined as blunt and straight to the point”). Holtgraves and Perdew reported that when their scenario was face-threatening, participants produced more indirect language, or language that differs from the most efficient way of communicating. We expected therefore that a diagnosis produced under face-threatening conditions would be interpreted as more indirect (i.e., less direct) than a diagnosis produced under less face-threatening circumstances.
Fourth, letters were rated on politeness (i.e., “how polite is this letter?”). Bonnefon and Villejoubert (Citation2006) evidenced that when communicating negative health information to a patient, the use of hedging terms (e.g., “you will possibly suffer from … “) caused participants to interpret the use of this term as a technique for managing face (i.e., masking the seriousness of the information). We expected that letters written under high face threat would be interpreted as more polite than letters produced under low face threat.
Design
There were no further experimental manipulations in Experiment 1b. Letters written in Experiment 1a under low or high face threat and communicating a certain or uncertain diagnosis were subjectively rated on the four measures detailed above.
Participants
We set out to have each individual letter produced in Experiment 1a rated by a single participant in Experiment 1b, resulting in a target sample of 200. The study was open to those who were aged 18 or over, fluent in English, and had not taken part in Experiment 1a. Each participant was randomly assigned to rate one of the letters generated in Experiment 1a. Following the same recruitment strategies, 219 participants consented to take part. Nine respondents were shown a unique letter but did not then go on to rate the letter, meaning that our randomizer presented 9 letters twice. Duplicate ratings were removed, and a further 10 incomplete responses were also excluded. A final sample of 200 English-speaking adults (39 men, 169 women, 1 “prefer not to say”) aged between 18 and 77 (M age = 30.31, SD = 12.75) rated a single letter. Given that our data from Experiment 1a served as the stimuli for Experiment 1b, the number of participants assigned to each condition was the same. Gender makeup did not differ across conditions (χ2 (6, N = 200) = 3.33, p = .77).
Materials
Each of the 200 letters written in Experiment 1a were converted into separate experimental vignettes; see for an example. Formatting examples from all 6 scenarios can be found on the OSF.
Figure 5. Example scenario as it appeared to participants in Experiment 1b.
Measures
The four measures described above (probability, certainty, directness, and politeness) were each rated on a scale ranging from 0 to 100.
Procedure
Participants accessed Experiment 1b via an anonymous link. Volunteers were informed they should not take part if they took part in Experiment 1a. They first answered some basic demographic questions. Afterward, participants were randomly presented with one vignette containing a single letter written from Experiment 1a. Viewing a single letter aids the believability of the hypothetical scenario and avoids revealing the experimental manipulations that were made in Experiment 1a. Once participants had read and considered the scenario, they reported their rating of probability, certainty, directness, and politeness. We again ran seriousness checks before participants submitted their survey. Mean completion time was 2 minutes, 49 seconds. A .qsf file for the Qualtrics survey can be accessed via the OSF.
Results
The raw data and analysis scripts for Experiment 1b are publicly available on the OSF. The data from our four measures are plotted in .
Figure 6. Mean probability, certainty, directness, and politeness ratings across our four experimental conditions (high/certain, n = 49; low/certain, n = 44; high/uncertain, n = 53; low/uncertain, n = 54). Black horizontal lines represent condition means. Surrounding bands represent 95% confidence intervals. Black jittered dots represent raw data points, and beans represent smoothed density curves.
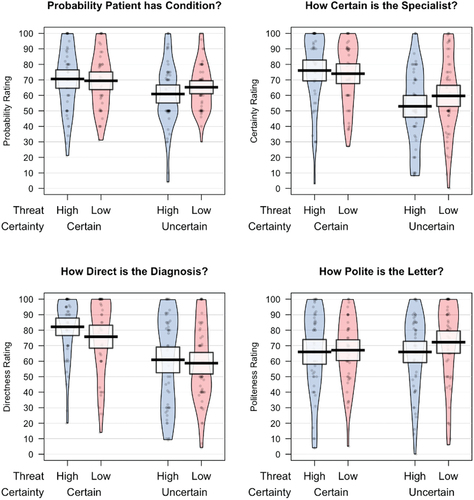
Probability
We found a significant main effect of certainty on judgments of probability (F(1, 196) = 6.51, p = .011, f = 0.18). Participants who read a letter of diagnosis that was uncertain rated the probability that the patient had the condition as significantly less likely (M = 63.1) than when a certain diagnosis was being communicated (M = 70.0). There was no significant main effect of face threat (F(1, 196) = 0.35, p = .553, f = 0.04) and no interaction between face threat and certainty (F(1, 196) = 1.02, p = .314, f = 0.07).
Certainty
We found a significant main effect of our certainty manipulation on judgments of perceived certainty (F(1, 196) = 30.48, p < .001, f = 0.39). Participants who read a letter of diagnosis that was uncertain perceived the specialist to be significantly less certain in their diagnosis (M = 56.3) than when a certain diagnosis was being communicated (M = 75.0). There was no main effect of face threat (F(1, 196) = 0.47, p = .495, f = 0.04) and no interaction between face threat and certainty (F(1, 196) = 1.69, p = .195, f = 0.09).
Directness
There was a significant main effect of certainty on judgments of directness (F(1, 196) = 28.74, p < .001, f = 0.38). Participants who read a letter of diagnosis that was uncertain perceived the specialist to be significantly less direct in their diagnosis (M = 59.8) than when a certain diagnosis was being communicated (M = 79.0). There was no significant main effect of face threat (F(1, 196) = 1.41, p = .236, f = 0.09) and no significant interaction between face threat and certainty (F(1, 196) = 0.35, p = .555, f = 0.04).
Politeness
There was no significant main effect of face threat (F(1, 196) = 1.05, p = .307, f = 0.08) and no significant main effect of certainty (F(1, 196) = 0.52, p = .474, f = 0.05) on judgments of politeness. Additionally, there was no significant interaction between face threat and certainty (F(1, 196) = 0.53, p = .467, f = 0.05).
Exploratory analysis
To determine whether participants in Experiment 1b were sensitive to linguistic variation in the Experiment 1a letters (irrespective of experimental condition), we conducted a series of bivariate correlations (). These revealed that the number of hedges was negatively associated with ratings of probability, certainty, and directness and positively associated with politeness. Word count was also positively associated with politeness.
Table 3. Pearson Correlation Coefficients Representing the Relationship Between Experiment 1a Letter Counts (Number of Hedges, Number of Dispreferred Markers, Total Word Count, Writing Time) and Letter Ratings in Experiment 1b (Judged Probability, Certainty, Directness, and Politeness)
Discussion
Contrary to our predictions, letters that were written under high face threat were not perceived any differently from letters written under low face threat. Our face threat manipulation, whereby we instructed participants to address their letter of diagnosis directly to the patient or to the patient’s family doctor, did not alter judgments of (1) probability that the patient had the condition (which replicates findings reported by Holtgraves & Perdew, Citation2016), (2) how certain the specialist was in their diagnosis, (3) how direct the letters were, or (4) how polite the letters were. In short, our Experiment 1a face threat manipulation did not lead to differences in language production that affected the interpretation of participants in Experiment 1b. Despite the absence of between-group differences, exploratory analysis did indicate that the production of hedges (which can be used to manage negative face) was associated with perceived politeness; letters containing more hedges were perceived as more polite.
In contrast to face threat manipulation, our manipulation of certainty (certain vs. uncertain) did alter participants’ interpretation on three measures during Experiment 1b. Two of these findings reflected the simple fact that uncertain writers produce more uncertain language. First, when letters were written in the uncertain condition, the probability of the patient having the condition was perceived to be lower than letters written in the certain condition. This demonstrates that participants in Experiment 1b could detect this uncertainty via the language of the speaker and lowered their probability estimate as a result. Second, when letters were written in the uncertain condition, the specialist was interpreted as being less certain in their diagnosis. This demonstrates that hearers could detect uncertainty via the language produced by the speaker.
Perhaps most interestingly, however, uncertain letters were rated as less direct than certain letters. In other words, the presence of uncertainty made letters appear more indirect than when letters were certain. This demonstrates that the presence of uncertainty when communicating threatening information causes the speaker to produce language that is more indirect and, importantly, that this indirectness can be detected by the reader.
General discussion
The two-part experiment reported in this article builds on the work of Holtgraves and Perdew (Citation2016). They found that messages communicated when face management was a concern (high face threat) were perceived as more indirect. Here, we support and extend these findings with evidence that writers primarily manage face threat using dispreferred markers (e.g., “Unfortunately,” “I’m sorry to tell you”). These markers alert the reader to the presence or occurrence of threatening news and are an explicit expression of emotional acknowledgment from the writer.
Contrary to our predictions, the face threat manipulation did not affect production of linguistic hedges. While the overall production of uncertainty terms was found to be infrequent (sparing) in the data reported by Holtgraves and Perdew (Citation2016), they used relatively informal interpersonal scenarios in their research. This may have encouraged participants to use subtle indirectness as a face-saving strategy rather than explicitly using uncertainty terms. We hypothesized that increasing the severity of the information to be communicated (i.e., breaking bad news), making the communication more formal (i.e., writing a letter), and increasing relationship distance (i.e., professional rather than personal) would encourage participants to produce hedging terms (e.g., “possibly,” “maybe”) to manage face. Even under these conditions, the number of hedges produced did not differ as a function of face threat. Descriptive statistics indicate that those under high face threat did produce slightly more hedges, but the effect size was small. This small, marginally nonsignificant effect may reflect that our letter-writing paradigm allowed participants to edit their letters with no immediate social pressure. Future research that increases the social pressure further (e.g., communicating face-to-face in role play) may amplify the face threat and result in larger effects.
This study is the second open-ended language production task to show that the explicit production of hedging terms is not the primary strategy for managing face threat. We must therefore consider the possibility that terms like “possibly” and other hedges are primarily used to communicate genuine uncertainty rather than as a politeness strategy. Experiment 1a participants produced many more hedging terms when instructed to deliver an uncertain diagnosis compared to certain. Of course, it makes sense that participants produced uncertainty terms to communicate that they are uncertain. It seems that a writer is more willing to hedge when they believe the diagnosis could be in question compared to when they are convinced of the diagnosis. However, given that our experiment and the experiments reported by Holtgraves and Perdew (Citation2016) did not observe a change in spontaneous production of hedges as a function of face threat, it seems that politeness tactics to manage face in high-stakes situations may manifest themselves in other, more subtle ways.
One of the primary ways writers can use subtle forms of politeness to manage face is to be indirect. On discovering that their participants infrequently produced hedges (e.g., “possibly,” “maybe”) when under face threat, Holtgraves and Perdew (Citation2016) presented evidence that writers may instead manage face by using increased levels of indirectness. For example, they coded phrases like “you’re partying too much” as direct, whereas a phrase like “Well I’d be failing too if I partied that often” was coded as indirect. They found that face threat resulted in the production of more indirect language, suggesting that rather than achieving politeness via the use of hedges, writers can tactfully “tiptoe” around sensitive information by being subtly indirect. The data reported in our experiment also support this claim. First, our participants in Experiment 1a “stretched” the language of their letters with dispreferred markers. By explicitly acknowledging the severity of the situation (i.e., “this must be tough for you”) and expressing remorse (i.e., “I’m sorry to inform you”), participants avoided a direct and efficient diagnosis statement that would threaten the reader’s positive face. Moreover, these markers encourage the reader to infer the onset of bad news ahead of time. A statement like “There’s no easy way to say this …”, for example, indirectly hints toward unfavorable news and causes readers to preempt the prognosis. As such, indirectness is used to achieve politeness under face threat through the use of dispreferred markers. Second, Experiment 1a participants chose to use significantly more words to complete their letter while under face threat (which, among other factors, may reflect the increased use of dispreferred markers). One plausible explanation for this finding is that the expected content of the letter is different when addressed to a patient rather than a doctor, based on presumed responsibilities and expertise. For example, stating the purpose of a particular health assessment (e.g., a brain scan) may be useful when writing to a patient but wholly unnecessary when writing to a fellow doctor (and perhaps even impolite or patronizing). Despite this, the increase in word count could also be explained by the aforementioned “polite indirectness.” It is often the case that the politest phrasing deviates from perfectly efficient communication (e.g., saying “if you could pass the salt that would be great” rather than “pass the salt”; Pinker et al., Citation2008). To choose speech that communicates in this way is to speak indirectly. Based on our word count data, it appears that writers under face threat demonstrated a reluctance to deliver undesirable information. This reluctance has previously been referred to as the “MUM effect” (Rosen & Tesser, Citation1970). It appears that writers in our experiment chose to indirectly attend to the reader’s face by “padding out” their letters with additional (unnecessary) words.
Manual inspection of the letters suggests that stretching occurred in other ways, such as giving a full description of the disease or citing support helplines. It’s possible that these are techniques characteristic of a “forecasting” or “stalling” approach to breaking bad news (Shaw et al., Citation2012). Observed in doctors, Shaw and colleagues detail that a forecasting approach represents a staged delivery of bad news (within the first 2 minutes), whereas a stalling approach represents an outright postponement of the delivery (beyond 2 minutes). The additional (or unnecessary) content used to pad out letters in Experiment 1a may reflect these delivery styles, potentially opening an avenue of further investigation. Researchers may, for example, wish to conduct exploratory analysis using our open access data.
We support the interpretation of Holtgraves and Perdew (Citation2016) that face threat can be subtly managed via indirect language. This is a particularly notable finding. We know that tactful indirectness can be beneficial in everyday social situations that threaten face, such as attempting to get out of a speeding ticket or expressing a negative opinion to a friend (Pinker et al., Citation2008; Sirota & Juanchich, Citation2015). However, this research extends our knowledge, demonstrating that language producers use subtle politeness tactics even in particularly high-stakes situations (i.e., breaking bad news to patients). Even under these extreme circumstances, it seems that face threat is managed through subtle indirectness.
One of the most notable effects in Experiment 1a was the time taken to compose the letters. The effect of face threat (high vs. low) on writing time only occurred when the diagnosis was uncertain. There was no such effect when the diagnosis was certain. This gives a novel insight into how managing both uncertainty and threat plays out in the mind of the writer in real time. We present a potential explanation for this finding. Having to balance both uncertainty and sensitivity at the same time is particularly difficult to achieve. Bonnefon et al. (Citation2011) showed that disentangling politeness is taxing on mental resources, meaning that greater cognitive effort is needed to “read between the lines.” Presumably, placing speakers in situations that require them to use politeness creates somewhat of a barrier to efficient communication. When faced with the balancing act of accurately communicating their level of commitment to the statement while attending to the face of all parties, writers are forced to use greater cognitive resources to overcome these linguistic hurdles put forward by the circumstances. It is entirely plausible therefore that the cumulative challenges posed by uncertainty and threat together account for an increase in time spent writing the letter.
In Experiment 1b, we examined the comprehension of the letters produced in Experiment 1a. This was based on a method by Holtgraves and Perdew (Citation2016) and gives additional insight into the communicative dyad. Beginning with the effect of our certainty manipulation, we found that letters written in our certain condition in Experiment 1a were perceived to be more certain by participants in Experiment 1b. Likewise, letters written in the certain condition were perceived as more direct and to be communicating a higher probability that the patient truly has the diagnosed condition. This suggests that our experimental manipulation of certainty in Experiment 1a produced changes in language production that were detected by participants in Experiment 1b. In general, our manipulation of the writers’ certainty is particularly valuable here in achieving a more complete understanding of uncertainty communication, primarily because it allowed us to observe how uncertainty is handled in particularly threatening circumstances.
Contrary to our predictions, letters written under high and low face threat were not judged differently on any of our interpretive measures (probability, certainty, directness, and politeness). Despite letters written under high face threat in Experiment 1a containing more words and more dispreferred markers than letters written under low face threat, these letters were not actually perceived as any less direct by participants in Experiment 1b. Likewise, the change in language use caused by our Experiment 1a face threat manipulation did not affect how participants in Experiment 1b perceived the certainty of the diagnosis or the probability that the patient truly has the diagnosed condition. From one perspective, these null findings are reassuring, as they suggest that facework strategies do not cloud the core meaning of the message being communicated. This aligns with a wider body of research evidence suggesting that despite the multiple possible motivations for speech, humans are particularly good at mitigating the use of face-management strategies and disentangling ambiguity (Aronsson & Sätterlund-Larsson, Citation1987; Bromme et al., Citation2012; Person et al., Citation1995). For instance, hearers seem to be good at knowing that the hedged polite utterance “I don’t think you’re suffering from measles” in practice means “Your concerns are unwarranted, this isn’t measles” (Brummernhenrich & Jucks, Citation2019). This may mean that facework strategies are perceived by recipients as symbolic (i.e., used by speakers to acknowledge the face threat) and do not necessarily cloud the intended speech act.
Participants in Experiment 1b were also asked to judge the politeness of the letter, and we found that politeness ratings did not differ as a function of certainty or face threat. We believe there may be an elementary explanation for our null finding. Participants in Experiment 1b were not asked to place themselves in the position of the recipient (either the patient or family doctor); rather, they read the exchange from the third person (i.e., from the outside looking in). It is therefore possible that context-dependent expectations of politeness confounded the judged level of politeness between the two scenarios. For example, a relatively terse letter written by a medical specialist to a family doctor may be considered polite in that professional context, even though that same letter might not be considered polite if it were addressed to the patient. This is because changing the addressee of the letter (i.e., from doctor to patient) changes the degree of politeness required to manage the threat of that situation and by extension changes the type of politeness that one would expect in that situation. This could mean that our participants in Experiment 1b judged relative (contextual) politeness rather than absolute (objective) politeness. Because of this, when they were asked “how polite is this letter?,” participants are likely to have judged the letters in their respective context, because they knew the intended recipient of the letter. This means that our letters may not be equally polite in absolute terms, but when judged within their own individual circumstances they are rated as equally polite.
Another consideration with regards to ratings of politeness in Experiment 1b is that in addition to facework, participants may have also been influenced by indicators of deference (e.g., please, thank you). These linguistic markers are not used explicitly to manage face, but when used in discourse they are commonly attributed to a person that is being polite. Indeed, the discrepancy between the academic versus everyday understanding of politeness may have had a nontrivial influence in this sample and should be considered as a potential limitation.
We must also consider other limiting factors and their influence on the effects (or lack of effects) outlined above. First, some of the effect sizes observed in Experiment 1a and Experiment 1b were small, whereas our study was designed to detect only medium-sized effects. Second, we did not perform manipulation checks in Experiment 1b and so cannot verify whether face threat was effectively operationalized within our scenarios. Differences in wording between the conditions were subtle (i.e., nonexplicit), so a potential instance of the letter addressee being overlooked (e.g., a participant assuming that the letter is addressed to the patient rather than the doctor) would not have been detected in the analysis.
The communication of uncertainty is a complex linguistic process, particularly under circumstances that threaten the positive social identity of the parties involved. We tested the production and comprehension of uncertain language within a health context, manipulating how socially delicate (or face threatening) the situation is. Our results indicate that writers manage threat under difficult social circumstances by using dispreferred markers (e.g., “I’m sorry to inform you,” “I understand this must be a difficult time for you”) to acknowledge the damaging effects of the threatening information and to address the sensitivity of the situation. These face-saving strategies used by language producers did not appear to cloud comprehension of the core messages being communicated.
Acknowledgments
We thank Molly Wheeler and Isabel Dunkerley who acted as independent coders in Experiment 1a.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
All data and code are available via the OSF https://osf.io/zu2an/.
Additional information
Funding
Notes
1. Additional exploratory analysis was also conducted in which scenario (i.e., the six different vignettes) was also included as a factor (i.e., 2 × 2 × 6 certainty × face threat × scenario; see Appendix 3 [https://osf.io/k34tn]). Scenario did not interact with the other variables (i.e., the effects of face threat and certainty did not differ across the six scenarios).
References
- Aronsson, K., & Sätterlund-Larsson, U. (1987). Politeness strategies and doctor-patient communication. On the social choreography of collaborative thinking. Journal of Language and Social Psychology, 6(1), 1–27. https://doi.org/10.1177/0261927X8700600101
- Auger, A., & Roy, J. (2008). Expression of uncertainty in linguistic data. In 2008 11th International Conference on Information Fusion (pp. 1–8). IEEE.
- Aust, F., Diedenhofen, B., Ullrich, S., & Musch, J. (2013). Seriousness checks are useful to improve data validity in online research. Behavior Research Methods, 45(2), 527–535. https://doi.org/10.3758/s13428-012-0265-2
- Baile, W. F., Buckman, R., Lenzi, R., Glober, G., Beale, E. A., & Kudelka, A. P. (2000). SPIKES—A six‐step protocol for delivering bad news: Application to the patient with cancer. The Oncologist, 5(4), 302–311. https://doi.org/10.1634/theoncologist.5-4-302
- Bhise, V., Meyer, A. N., Menon, S., Singhal, G., Street, R. L., Giardina, T. D., & Singh, H. (2018). Patient perspectives on how physicians communicate diagnostic uncertainty: An experimental vignette study. International Journal for Quality in Health Care, 30(1), 2–8. https://doi.org/10.1093/intqhc/mzx170
- Bonnefon, J.-F., Feeney, A., & De Neys, W. (2011). The risk of polite misunderstandings. Current Directions in Psychological Science, 20(5), 321–324. https://doi.org/10.1177/0963721411418472
- Bonnefon, J.-F., Feeney, A., & Villejoubert, G. (2009). When some is actually all: Scalar inferences in face threatening contexts. Cognition, 112(2), 249–258. https://doi.org/10.1111/j.1467-9280.2006.01776.x
- Bonnefon, J.-F., & Villejoubert, G. (2006). Tactful or doubtful? Expectations of politeness explain the severity bias in the interpretation of probability phrases. Psychological Science, 17(9), 747–751. https://doi.org/10.1111/j.1467-9280.2006.01776.x
- Bromme, R., Brummernhenrich, B., Becker, B. M., & Jucks, R. (2012). The effects of politeness-related instruction on medical tutoring. Communication Education, 61(4), 358–379. https://doi.org/10.1080/03634523.2012.691979
- Brown, P., & Levinson, S. C. (1987). Politeness: Some universals in language usage (Vol. 4). Cambridge University Press.
- Brummernhenrich, B., & Jucks, R. (2019). “Get the shot, now!” disentangling content-related and social cues in physician–patient communication. Health Psychology Open, 6(1), 2055102919833057. https://doi.org/10.1177/2055102919833057
- Burgers, C., Beukeboom, C. J., & Sparks, L. (2012). How the doc should (not) talk: When breaking bad news with negations influences patients’ immediate responses and medical adherence intentions. Patient Education and Counseling, 89(2), 267–273. https://doi.org/10.1016/j.pec.2012.08.008
- Clelland, H. T., & Haigh, M. (2023). Materials and data from politeness and the communication of uncertainty when breaking bad news [data set & materials]. Open Science Framework. https://doi.org/10.17605/OSF.IO/ZU2AN
- Crompton, P. (1997). Hedging in academic writing: Some theoretical problems. English for Specific Purposes, 16(4), 271–287. https://doi.org/10.1016/S0889-4906(97)00007-0
- Dibble, J. L., & Levine, T. R. (2013). Sharing good and bad news with friends and strangers: Reasons for and communication behaviors associated with the MUM effect. Communication Studies, 64(4), 431–452. https://doi.org/10.1080/10510974.2013.770407
- Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G* power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191. https://doi.org/10.3758/bf03193146
- Fraser, B. (2010). Pragmatic competence: The case of hedging. In G. Kaltenböck, W. Mihatsch, & S. Schneide (Eds.), New approaches to hedging (pp. 15–34). Brill. https://doi.org/10.1163/9789004253247_003
- Goffman, E. (1967). Interaction ritual: Essays on face-to-face interaction. Aldine.
- Hallgren, K. A. (2012). Computing inter-rater reliability for observational data: An overview and tutorial. Tutorials in Quantitative Methods for Psychology, 8(1), 23–34. https://doi.org/10.20982/tqmp.08.1.p023
- Hamilton, R., Vohs, K. D., & McGill, A. L. (2014). We’ll be honest, this won’t be the best article you’ll ever read: The use of dispreferred markers in word-of-mouth communication. Journal of Consumer Research, 41(1), 197–212. https://doi.org/10.1086/675926
- Holtgraves, T. (2005). Social psychology, cognitive psychology, and linguistic politeness. Journal of Politeness Research. Language, Behaviour, Culture, 1(1), 73–93. https://doi.org/10.1515/jplr.2005.1.1.73
- Holtgraves, T. (2014). Interpreting uncertainty terms. Journal of Personality and Social Psychology, 107(2), 219. https://doi.org/10.1037/a0036930
- Holtgraves, T., & Perdew, A. (2016). Politeness and the communication of uncertainty. Cognition, 154, 1–10. https://doi.org/10.1016/j.cognition.2016.05.005
- Holtgraves, T., & Yang, J. N. (1992). Interpersonal underpinnings of request strategies: General principles and differences due to culture and gender. Journal of Personality and Social Psychology, 62(2), 246–256. https://doi.org/10.1037/0022-3514.62.2.246
- Juanchich, M., & Sirota, M. (2013). Do people really say it is ‘likely’ when they believe it is only ‘possible’? Effect of politeness on risk communication. Quarterly Journal of Experimental Psychology, 66(7), 1268–1275. https://doi.org/10.1080/17470218.2013.804582
- Juanchich, M., Sirota, M., & Butler, C. L. (2012). The perceived functions of linguistic risk quantifiers and their effect on risk, negativity perception and decision making. Organizational Behavior and Human Decision Processes, 118(1), 72–81. https://doi.org/10.1016/j.obhdp.2012.01.002
- Lee, F. (1993). Being polite and keeping MUM: How bad news is communicated in organizational hierarchies. Journal of Applied Social Psychology, 23(14), 1124–1149. https://doi.org/10.1111/j.1559-1816.1993.tb01025.x
- Lee, J. J., & Pinker, S. (2010). Rationales for indirect speech: The theory of the strategic speaker. Psychological Review, 117(3), 785. https://doi.org/10.1037/a0019688
- Markkanen, R., & Schröder, H. (Eds.). (2010). Hedging and discourse: Approaches to the analysis of a pragmatic phenomenon in academic texts (Vol. 24). Walter de Gruyter.
- Miyaji, N. T. (1993). The power of compassion: Truth-telling among American doctors in the care of dying patients. Social Science & Medicine, 36(3), 249–264. https://doi.org/10.1016/0277-9536(93)90008-R
- Person, N. K., Kreuz, R. J., Zwaan, R. A., & Graesser, A. C. (1995). Pragmatics and pedagogy: Conversational rules and politeness strategies may inhibit effective tutoring. Cognition and Instruction, 13(2), 161–188. https://doi.org/10.1207/s1532690xci1302_1
- Pinker, S., Nowak, M. A., & Lee, J. J. (2008). The logic of indirect speech. Proceedings of the National Academy of Sciences, 105(3), 833–838. https://doi.org/10.1073/pnas.0707192105
- Ptacek, J., & Eberhardt, T. L. (1996). Breaking bad news: A review of the literature. JAMA, 276(6), 496–502. https://doi.org/10.1001/jama.1996.03540060072041
- R Core Team. (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing. https://www.R-project.org/
- Rodriguez, K. L., Gambino, F. J., Butow, P., Hagerty, R., & Arnold, R. M. (2007). Pushing up daisies: Implicit and explicit language in oncologist–patient communication about death. Supportive Care in Cancer, 15(2), 153–161. https://doi.org/10.1007/s00520-006-0108-8
- Rosen, S., & Tesser, A. (1970). On reluctance to communicate undesirable information: The MUM effect. Sociometry, 33(3), 253–263. https://doi.org/10.2307/2786156
- RStudio Team. (2020). RStudio: Integrated development environment for R. RStudio, PBC. http://www.rstudio.com/
- Shaw, J., Dunn, S., & Heinrich, P. (2012). Managing the delivery of bad news: An in-depth analysis of doctors’ delivery style. Patient Education and Counseling, 87(2), 186–192. https://doi.org/10.1016/j.pec.2011.08.005
- Sirota, M., & Juanchich, M. (2015). A direct and comprehensive test of two postulates of politeness theory applied to uncertainty communication. Judgment and Decision Making, 10(3), 232–240. https://doi.org/10.1017/S1930297500004642
- Sirota, M., Juanchich, M., & Bonnefon, J.-F. (2018). ‘1-in-X’ bias:’1-in-X’ format causes overestimation of health-related risks. Journal of Experimental Psychology. Applied, 24(4), 431. https://doi.org/10.1037/xap0000190
- Snow, J., & Mann, M. (2013). Qualtrics survey software: Handbook for research professionals. Qualtrics Labs.
- Stewart, A. J., Wood, J. S., Le-luan, E., Yao, B., & Haigh, M. (2018). ‘It’s hard to write a good article’: The online comprehension of excuses as indirect replies. Quarterly Journal of Experimental Psychology, 71(6), 1265–1269. https://doi.org/10.1080/17470218.2017.1327546